

Abstract
Background
Little is known about the effectiveness of strategies to enable people to achieve and maintain recommended levels of physical activity.
Objectives
To assess the effectiveness of interventions designed to promote physical activity in adults aged 16 years and older, not living in an institution.
Search methods
We searched The Cochrane Library (issue 1 2005), MEDLINE, EMBASE, CINAHL, PsycLIT, BIDS ISI, SPORTDISCUS, SIGLE, SCISEARCH (from earliest dates available to December 2004). Reference lists of relevant articles were checked. No language restrictions were applied.
Selection criteria
Randomised controlled trials that compared different interventions to encourage sedentary adults not living in an institution to become physically active. Studies required a minimum of six months follow up from the start of the intervention to the collection of final data and either used an intention‐to‐treat analysis or, failing that, had no more than 20% loss to follow up.
Data collection and analysis
At least two reviewers independently assessed each study quality and extracted data. Study authors were contacted for additional information where necessary. Standardised mean differences and 95% confidence intervals were calculated for continuous measures of self‐reported physical activity and cardio‐respiratory fitness. For studies with dichotomous outcomes, odds ratios and 95% confidence intervals were calculated.
Main results
The effect of interventions on self‐reported physical activity (19 studies; 7598 participants) was positive and moderate (pooled SMD random effects model 0.28 95% CI 0.15 to 0.41) as was the effect of interventions (11 studies; 2195 participants) on cardio‐respiratory fitness (pooled SMD random effects model 0.52 95% CI 0.14 to 0.90). There was significant heterogeneity in the reported effects as well as heterogeneity in characteristics of the interventions. The heterogeneity in reported effects was reduced in higher quality studies, when physical activity was self‐directed with some professional guidance and when there was on‐going professional support.
Authors' conclusions
Our review suggests that physical activity interventions have a moderate effect on self‐reported physical activity, on achieving a predetermined level of physical activity and cardio‐respiratory fitness. Due to the clinical and statistical heterogeneity of the studies, only limited conclusions can be drawn about the effectiveness of individual components of the interventions. Future studies should provide greater detail of the components of interventions.
Keywords: Humans, Exercise, Health Promotion, Health Promotion/methods, Physical Fitness, Randomized Controlled Trials as Topic
Plain language summary
Interventions for promoting physical activity
Not taking enough physical activity leads to an increased risk of a number of chronic diseases including coronary heart disease. Regular physical activity can reduce this risk and also provide other physical and possibly mental health benefits. The majority of adults are not active at recommended levels. The findings of this review indicate that professional advice and guidance with continued support can encourage people to be more physically active in the short to mid‐term. More research is needed to establish which methods of exercise promotion work best in the long‐term to encourage specific groups of people to be more physically active.
Background
Regular physical activity can play an important role both in the prevention and treatment of cardiovascular disease (CVD), hypertension, non‐insulin dependent diabetes, diabetes mellitus, obesity, stroke, some cancers, and osteoporosis, as well as improve the lipid profile (DOH 2004; Folsom 1997; FNB 2002; US Dept. Health 1996; WHO 2004). A meta‐analysis of the relationship between physical activity and coronary heart or cardiovascular disease reported a 30% lower risk for the most physically active versus the least physically activity (Williams 2001). In addition, physical inactivity has been estimated to cause, globally, about 22% of ischaemic heart disease (WHO 2002).
The English Chief Medical Officer (CMO) advises that adults should undertake at least 30 minutes of 'moderate intensity' (5.0‐7.5 kcal/min) physical activity on at least 5 days of the week to benefit their health (DOH 2004). The recommendations are similar to those published in the US and by the World Health Organisation (Pate 1995; US Dept. Health 1996; WHO 2004).
In England the prevalence of physical activity at recommended levels is low. The most recent data show that only 37% of men and 25% of women meet the CMO's physical activity recommendation (DOH 2005a). Local government authorities have been set a target to 'increase the number of adults who engage in at least 30 minutes of moderate intensity level sport three times a week, by 3% by 2008' (DOH 2005b; HM Treasury 2002).
There are randomised controlled trials assessing the effects of physical activity in the management of specific diseases, notably hypertension, hyperlipidaemia, obesity and CVD (DOH 2004). These show the effects of exercise on various physiological and biological outcomes and demonstrate the importance of exercise in the management of disease. However, because the main outcome of these trials is not physical activity, they do not help us understand the effectiveness of physical activity promotion strategies in the general population. A number of Cochrane reviews have assessed the relationship of the effects of exercise upon type 2 diabetes and as part of cardiac rehabilitation (Jolliffe 2001; Thomas 2006).
One recent published review examined the evidence for the effectiveness of 'home based' versus 'centre based' physical activity programs on the health of older adults (Ashworth 2005). Study participants had to have either a recognised cardiovascular risk factor, or existing cardiovascular disease, or chronic obstructive airways disease (COPD) or osteoarthritis. The authors found six trials involving 224 participants who received a 'home based' exercise program and 148 who received a 'centre based' exercise program. They concluded there was insufficient evidence to make any conclusions in support of either home or centre based physical activity programs.
Objectives
To compare the effectiveness of interventions for physical activity promotion in adults aged 16 and above, not living in an institution, with no intervention, minimal intervention or attention control. If sufficient trials existed, the following secondary objectives were to be explored:
a) Are more intense interventions more effective in changing physical activity than less intense interventions (e.g. a greater frequency and duration of professional contact and support v single contact)?
b) Are specific components of interventions associated with changes in physical activity behaviour (e.g. prescribed v self determined physical activity, supervised v unsupervised physical activity)?
c) Are short‐term changes in physical activity or fitness (e.g. less than 3 months from intervention, less than 6 months from intervention) maintained at 12 months?
d) Is the promotion of some types of physical activity more likely to lead to change than other types of physical activity (e.g. walking versus exercise classes)?
e) Are home‐based interventions more successful than facility‐based interventions?
f) Are interventions more successful with particular participant groups (e.g. women, older, minority)?
Methods
Criteria for considering studies for this review
Types of studies
Randomised controlled trials (RCTs) comparing different strategies to encourage sedentary, community dwelling adults to become more physically active, with a minimum of 6 months follow‐up from the start of the intervention to the final results using either an intention to treat analysis or no more than 20% loss to follow up.
Types of participants
Community dwelling adults, age 16 years to any age, free from pre‐existing medical condition or with no more than 10% of subjects with pre‐existing medical conditions that may limit participation in physical activity. Interventions on trained athletes or sports students were excluded.
Types of interventions
One only or a combination of:
One‐to‐one counselling/advice or group counselling/advice;
Self‐directed or prescribed physical activity;
Supervised or unsupervised physical activity;
Home‐based or facility‐based physical activity;
Ongoing face‐to‐face support;
Telephone support;
Written education/motivation support material;
Self monitoring.
The interventions were conducted by one or a combination of practitioners including a physician, nurse, health educator, counsellor, exercise leader or peer. Mass media interventions and multiple risk factor interventions were excluded.
The interventions were compared with a no intervention control, attention control (receiving attention matched to length of intervention, e.g. general health check) and/or minimal intervention control group.
Types of outcome measures
Primary outcome measures
Change in self‐reported physical activity between baseline and follow‐up.
Cardio‐respiratory fitness.
Adverse events.
Physical activity measures were expressed as an estimate of total energy expenditure (kcal/kg/week, kcal/week), total minutes of physical activity, proportion reporting a pre‐determined threshold level of physical activity (e.g., meeting current public health recommendation), frequency of participation in various types of physical activity e.g. walking, moderate intensity physical activity.
Cardio‐respiratory fitness was either estimated from a sub‐maximal fitness test or recorded directly from a maximal fitness test and was expressed as maximal oxygen consumption (VO2 max) either in ml·kg‐1·min‐1 or ml·min‐1. Aspects of cardio‐respiratory fitness were also included as secondary outcome measures.
Adverse events included job‐related injuries any reported musculoskeletal injury or cardiovascular events (and exercise‐related cardiac events and injuries (fractures, sprains)).
Search methods for identification of studies
We searched The Cochrane Library (Issue 1, 2005) , MEDLINE (January 1966 to December 2004), EMBASE (January 1980 to December 2004), CINAHL (January 1982 to December 2004), PsycLIT (1887 to December 2004), BIDS ISI (January 1973 to December 2004), SPORTDISCUS (January 1980 to December 2004), SIGLE (January 1980 to December 2004) and SCISEARCH (January 1980 to December 2004), and reference lists of articles. Hand searching was conducted on one journal Medicine and Science in Sport and Exercise from 1990 to December 2004. Published systematic reviews of physical activity interventions were used as a source of randomised controlled trials. Reference lists of all relevant articles, books and personal contact with authors were also used. All languages were included.
The search strategy below was used to search MEDLINE, with the addition of an RCT filter (Dickersin 1995). This strategy was modified for other databases, using an appropriate RCT filter for EMBASE (Lefebvre 1996). (see Table 1; Table 2;Table 3;Table 4;Table 5; Table 6).
1. Search Strategy for EMBASE.
| Dates 2000 to 2004 |
| 1.((((health‐education) or (health‐education‐research)) or ((patient‐education) or (patient‐education‐and‐counseling)) or ((health‐promotion) or (health‐promotion‐international)) or (primary‐health‐care) or ((workplace) or (workplace‐)) or (promot*) or ((promot*) or ((educat*) or ((program*) and ((((exertion) or (fitness) or (fitness‐) or ((fitness) or (fitness‐)) or (exercise) or ((exercise) or (sport) or (walk*))) 2.((research) or (((((random‐controlled) or (random‐sample) or (randomisation) or (randomised) or (randomised‐controlled) or (randomization) or (randomization‐) or (randomizd) or (randomize) or (randomized) or (randomized‐block) or (randomized‐controlled) or (randomized‐controlled‐trial) or (randomized‐control)) or ((double‐blind) or (double‐blind‐procedure)) or ((single‐blind) or (single‐blind‐procedure))) and (ec=human)) or (clinical) or (clin*) or (trial*) or (((clin* near trial*) in ti) and (ec=human)) or (clin*) or (trial*) or (((clin* near trial*) in ab) and (ec=human)) or (sing*) or (doubl*) or (trebl*) or (tripl*) or (blind*) or (mask*) or (((sing* or doubl* or trebl* or tripl*) near (blind* or mask*)) and (ec=human)) or ((placebos) or (placebo‐controlled)) or ((placebo* in ti) and (ec=human)) or ((placebo* in ab) and (ec=human)) or ((random* in ti) and (ec=human)) or ((random in ab) and (ec=human)) or (research)) ec=human) 3.((((studies) or (prospective‐study) or (follow‐up) or (comparative) or (evaluation)) and (ec=human)) |
2. Search Strategy for CINAHL.
| Dates 2000 to 2004 |
| 1.exact{controlled} 2.exact{randomized} 3.exact{random‐assignment} 4.exact{double‐blind} 5.exact{single‐blind} 6.#1 or #2 or #3 or #4 or #5 7.exact{animal} 8.exact{human} 9.#6 not #7 10.exact{clinical} 11.(clin* near trial*) in ti 12.(clin* near trial*) in ab 13.(singl* or doubl* or trebl* or tripl*) near (blind* or mask*) 14.(#13 in ti) or (#13 in ab) 15.placebos 16.placebo* in ti 17.placebo* in ab 18.random* in ti 19.random* in ab 20.exact{research‐methodology} 21.#10 or #11 or #12 or #13 or #14 or #15 or #16 or #17 22.#18 or #19 or #20 23.#21 or #22 24.animal 25.human 26.#23 not #24 27.#26 or #9 or #8 or #25 28.exact{comparative} 29.study 30.#28 and #29 31.exact{evaluation} 32.studies 33.#31 and #32 34.exact{follow‐up} 35.exact{propsective} 36.#35 and #32 37.control* or prosepctiv* or volunteer* 38.(#37 in ti) or (#37 in ab) 39.#38 or #36 or #33 or #30 40.#39 not #24 41.#39 or #27 or #9 42.explode "exertion/"/ all subheadings 43."physical fitness" 44.explode "physical education and training"/ all subheadings 45.explode "sports"/ all subheadings 46.explode "dancing"/ all subheadings 47.explode "exercise therapy"/ all subheadings 48.(physical$ adj5 (fit$ or train$ or activ$ or endur$)).tw. 49.(exercis$ adj5 (train$ or physical$ or activ$)).tw. 50.sport$.tw. 51.walk$.tw. 52.bicycle$.tw 53.(exercise$ adj aerobic$).tw. 54.(("lifestyle" or life‐style) adj5 activ$).tw. 55.(("lifestyle" or life‐style) adj5 physical$).tw. 56.#42 or #43 or #44 or #45 or #46 or #47 or #48 or #49 or (exercise$) or (aerobic$) or ("lifestyle") or (activ$) or ("lifestyle") or (life‐style) or (physical$) 57.health education 58.patient education 59.primary prevention 60.health promotion 61.behaviour therapy 62.cognitive therapy 63.primary health care 64.workplace 65.promot$.tw. 66.educat$.tw. 67.program$.tw. 68.#57 or #58 or #59 or #60 or #61 or #62 or #63 or #64 or #65 or #66 or #67 69.#68 and #56 70.#69 and #41 |
3. Search Startegy for PsycLIT.
| Dates 2000 to 2004 |
| 1.exertion 2.physical‐fitness 3.exercise 4.explode exercise 5.sport 6.walk* 7.cycle 8.#1 or #2 or #3 or #4 or #5 or #6 or #7 9.health education 10.patient education 11.primary prevention 12.health promotion 13.behaviour therapy 14.cognitive therapy 15.primary health care 16.workplace 17.promot$.tw. 18.educat$.tw. 19.program$.tw. 20.#9 or #10 or #11 or #12 or #13 or #14 or #15 or #16 or #17 or #18 or #19 21.#8 and #20 22.controlle 23.randomized 24.random‐assignment 25.double‐blind 26.single‐blind 27.#22 or #23 or #24 or #25 or #26 28.animal 29.human 30.#27 not #28 31.clinical 32.(clin* near trial*) in ti 33.clin* near trial*) in ab 34.(singl* or doubl* or trebl* or tripl*) near (blind* or mask*) 35.(#34 in ti) or (#34 in ab) 36.placebos 37.placebo* in ti 38.placebo* in ab 39.random* in ti 40.random* in ab 41.research‐methodology} 42.#31 or #32 or #33 or #34 or #35 or #36 or #37 or #38 43.#39 or #40 or #41 44.#42 or #43 45.animal 46.human 47.#44 not #45 48.#47 or #30 or #29 or #46 49.comparative 50.study 51.#49 and #50 52.evaluation 53.studies 54.#52 and #53 55.follow‐up 56.propsective 57.#56 and #53 58.control* or prosepctiv* or volunteer* 59.(#58 in ti) or (#58 in ab) 60.#59 or #57 or #54 or #51 61.#60 not #45 62.#60 or #48 or #30 63.#62 and #21 |
4. Search Startegy SPORTSDISCUS.
| Dates 2000 to 2004 |
| 1.'physical activity' 2.exercise 3.fitness 4.sedentary 5.housebound 6.aerobics or circuits or swimming or aqua or jogging or running or cycling or fitness or yoga or walking or sport 7.patient education 8.primary prevention 9.health promotion 10.behaviour therapy 11.cognitive therapy 12.primary health care 13.workplace 14.controlled 15.randomized 16.random‐assignment 17.double‐blind 18.single‐blind 19.clinical 20.placebos 21.comparative 22.evaluation 23.study |
5. Search Strategy SIGLE.
| Dates 2000 to 2004 |
| 1.explode "Exertion/"/ all subheadings 2."Physical fitness" 3.explode "Physical education and training"/ all subheadings 4.explode "Sports"/ all subheadings 5.explode "Dancing"/ all subheadings 6.explode "Exercise therapy"/ all subheadings 7.(physical$ adj5 (fit$ or train$ or activ$ or endur$)).tw. 8.(exercis$ adj5 (train$ or physical$ or activ$)).tw. 9.sport$.tw. 10.walk$.tw. 11.bicycle$.tw 12.(exercise$ adj aerobic$).tw. 13.(("lifestyle" or life‐style) adj5 activ$).tw. 14.(("lifestyle" or life‐style) adj5 physical$).tw. 15.#1 or #2 or #3 or #4 or #5 or #6 or #7 or #8 or (exercise$) or (aerobic$) or ("lifestyle") or (activ$) or ("lifestyle") or (life‐style) or (physical$) 16.Health Education 17.Patient education 18.Primary prevention 19.Health promotion 20.Behaviour therapy 21.Cognitive therapy 22.Primary health care 23.Workplace 24.promot$.tw. 25.educat$.tw. 26.program$.tw. 27.#16 or #17 or #18 or #19 or #20 or #21 or #22 or #23 or #24 or #25 or #26 28.#15 and #27 |
6. Search Strategy SCISEARCH.
| Dates 2000 to 2004 |
| 1.((promot$ or uptake or encourag$ or increas$ or start) near (physical adj activity)) 2.(promot$ or uptake or encourag$ or increas$ or start) near exercise 3.(promot$ or uptake or encourag$ or increas$ or start) near (aerobics or circuits or swimming or aqua$) 4.(promot$ or uptake or encourag$ or increas$ or start) near (jogging or running or cycling) 5.(promot$ or uptake or encourag$ or increas$ or start) near ((keep adj fit) or (fitness adj class$) or yoga) 6.(promot$ or uptake or encourag$ or increas$ or start) near walking 7.(promot$ or uptake or encourag$ or increas$ or start) near sport$ |
1 exp Exertion/ 2 Physical fitness/ 3 exp "Physical education and training"/ 4 exp Sports/ 5 exp Dancing/ 6 exp Exercise therapy/ 7 (physical$ adj5 (fit$ or train$ or activ$ or endur$)).tw. 8 (exercis$ adj5 (train$ or physical$ or activ$)).tw. 9 sport$.tw. 10 walk$.tw. 11 bicycle$.tw. 12 (exercise$ adj aerobic$).tw. 13 (("lifestyle" or life‐style) adj5 activ$).tw. 14 (("lifestyle" or life‐style) adj5 physical$).tw. 15 or/1‐14 16 Health education/ 17 Patient education/ 18 Primary prevention/ 19 Health promotion/ 20 Behaviour therapy 21 Cognitive therapy 22 Primary health care 23 Workplace/ 24 promot$.tw. 25 educat$.tw. 26 program$.tw. 27 or/16‐26 28 15 and 27
Data collection and analysis
All abstracts were reviewed independently by two investigators who applied the following criteria to determine if the full paper was needed for further investigation: a) did the study aim to examine the effectiveness of a physical activity promotion strategy to increase physical activity behaviour? b) did the study have a control group (e.g. a no intervention control, attention control and/or minimal intervention control group)? c) did the study allocate participants into intervention or control groups by a method of randomisation? d) did the study include adults of 16 years or older? e) did the study recruit adults not living in institutions and free of chronic disease? f) was the study's main outcome physical activity or physical fitness? g) were the main outcome(s) measured at least 6 months after the start of the intervention? h) did the study analyse the results by intention‐to‐treat or, failing that was there less than 20% loss to follow up?
Two reviewers examined a hard copy of every paper that met the inclusion criteria on the basis of the abstract alone (or title and keywords if no abstract was available). When a final group of papers was identified all papers were reviewed again by two reviewers independently. Any disagreement at this stage was discussed between the three reviewers and resolved by consensus.
From the final set of studies that met the inclusion criteria, study details were extracted independently by two reviewers onto a standard form. Again any disagreements were discussed between three reviewers and resolved by consensus. Extracted data included date and location of study, study design variables, methodological quality, characteristics of participants (age, gender, ethnicity), intervention strategies, frequency and type of intervention and follow‐up contacts, degree of physical activity supervision, study outcome measure, effectiveness of intervention and adverse events.
We wrote to and received clarification from 11 authors of the studies selected for the review. Our requests focused on data missing or unclear from the published papers and included data on study numbers at final analysis, means and standard deviations for intervention and control arms. For incomplete responses, we wrote again to authors asking for further data.
We found different types of outcome results published in two included papers for the Sendai Silver Centre Trial (SSCT 2000). Tsuji 2000 reported changes in cardiovascular fitness and Fujita 2003 reported increases in self‐reported physical activity.
Outcomes were analysed both as continuous outcomes and as dichotomous outcomes (active/sedentary) wherever possible. Standard statistical approaches were adopted:
(a) For each study with continuous outcomes; a standardised mean difference (SMD) and 95% confidence intervals (95% CI) were calculated. If the study had more than two arms then the overall effects of the intervention versus control (means and standard deviations) were examined by pooling the individual effect of each intervention arm (means and standard deviations). These pooled groups means and standard deviations were weighted for overall numbers within each arm (Higgins 2005). Pooled effect sizes were calculated as standardised mean differences with 95% CI using a random‐effects model.
(b) For each study with dichotomous outcomes; an odds ratio (OR) and 95% CI were calculated. Pooled effect sizes were calculated as ORs and with 95% CI using a random‐effects model.
We examined five thematic characteristics of each intervention to try to assess if they modified the main effects of the interventions. These five characteristics were the nature of direction at first contact, degree of programme supervision, frequency of intervention occasions, frequency of follow‐up contacts and type of follow‐up contacts.
We described the nature of the initial contact between the participant and professional/researcher as "the nature of direction". We found three types of intervention: (i) self‐directed only ‐ where the participant is not directed in their choices and thinking about which physical activities to start by the professional; (ii) self‐directed plus professional guidance ‐ where the participant can make a decision about their physical activity using a mixture of both self direction and professional advice and guidance; and (iii) prescribed by professional only ‐ the participant receives the advice and prescription of physical activity from the professional.
We wanted to evaluate the type and supervision of physical activity adopted within studies. We developed three categories of programme supervision: (i) structured and supervised ‐ the physical activity programme was structured and supervised by professional; (ii) unsupervised and independent ‐ the physical activity programme was unstructured and performed independently by the participant; and (iii) mixed ‐ the physical activity programme was both structured and supervised and unstructured and independent.
Results
Description of studies
From 35,524 hits, 287 papers were retrieved for examination against the inclusion criteria (Figure 1). Thirty three papers describing 35 studies met the inclusion criteria. We were unable to secure the requested information from five studies. Halbert 2000 was not contactable and so this study is not presented in the final results. Four studies sent data but the data was incomplete or inappropriate for meta‐analysis (Castro 2001; Lowther 2002a; Lowther 2002b; Mutrie 2002; Nies 2003). After excluding these studies with incomplete data, 29 studies remained (Calfas 2000; Cunningham 1987; Dubbert 2002; Elley 2003; Goldstein 1999; Green 2002; Harland 1999; Hillsdon 2002; Inoue 2003; Juneau 1987; King 1988a; King 1988b; King 1991; Kriska 1986; Lamb 2002; Lombard 1995; Marshall 2003a; Marshall 2004; Norris 2000; Petrella 2003; Pinto 2002; Reid 1979; Resnick 2002a; Simons‐Morton 2001a; Simons‐Morton 2001b; Smith 2000; Stevens 1998; Stewart 2001; SSCT 2000). All 29 studies were randomised controlled trials. Two papers each reported the results of two separate trials (King 1988a; King 1988b; Simons‐Morton 2001a; Simons‐Morton 2001b). Two papers reported different outcomes for one study (SSCT 2000).
1.
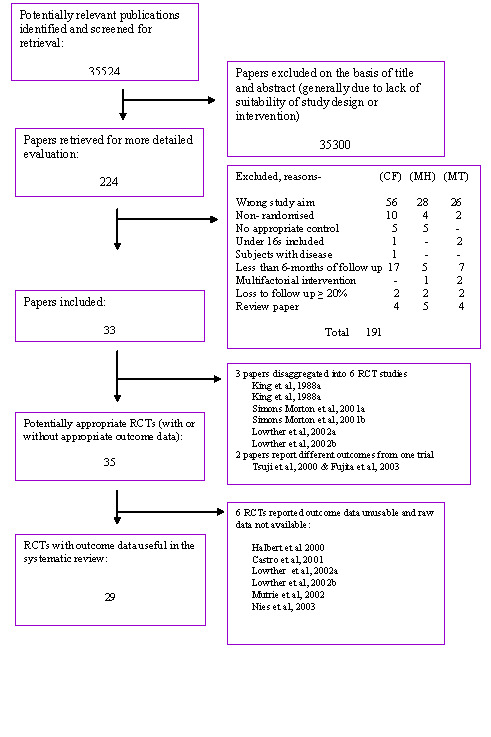
QUOROM statement
Participants of included studies 11,513 apparently healthy adults participated in the 29 included studies. The majority of studies recruited both genders with three studies recruiting men only (Cunningham 1987; Reid 1979; Simons‐Morton 2001a) and four studies recruiting women only (Inoue 2003; Kriska 1986; Resnick 2002a; Simons‐Morton 2001b). The stated age range of participants was from 18 to 95 years. Details on ethnic group of participants were reported in 13 studies, with proportions of participants in ethnic minorities ranging from 3% to 55%. Participants were recruited from four settings; primary healthcare, workplaces, university and the community (see Table 7).
7. Descriptive data for review studies.
| Author | Publication year | Setting | No. randomised | % Male | Age range | Authors' description |
| Reid 1979 | 1979 | Workplace | 124 | 100 | 24 to 56 | Endurance activities |
| Kriska 1986 | 1986 | Community | 229 | 0 | 50 to 65 | Walking |
| Cunningham 1987 | 1987 | Workplace / community | 224 | 100 | 54 to 68 | Walking, jogging or running |
| Juneau 1987 | 1987 | Workplace | 120 | 50 | 40 to 60 | Walking or slow jogging |
| King 1988a | 1988 | Workplace | 52 | 50 | 40 to 60 | Walking and jogging |
| King 1988b | 1988 | Workplace | 51 | 51 | 40 to 60 | Walking and jogging |
| King 1991 | 1991 | Community | 357 | 55 | 50 to 65 | Group or home based walking/jogging activities |
| Lombard 1995 | 1995 | University | 135 | 2.2 | 21 to 63 | Walking |
| Stevens1998 | 1998 | Primary Health Care | 714 | 42 | 45 to 74 | Build on present physical activities |
| Goldstein 1999 | 1999 | Primary Health Care | 355 | 35 | 50+ | Choice of moderate or vigorous physical activity |
| Harland 1999 | 1999 | Primary Health Care | 520 | 41.5 | 40 to 64 | Choice of safe and effective physical activity |
| Calfas 2000 | 2000 | University | 338 | 45.8 | 18 to 29 | Moderate or vigorous physical activity plus strength and flexibility activities |
| Norris 2000 | 2000 | Primary Health Care | 847 | 47.9 | 30+ | Moderate physical activity |
| Smith 2000 | 2000 | Primary Health Care | 1142 | 39.5 | 25 to 65 | Physical activity prescribed by medical practitioner |
| Simons‐Morton 2001a | 2001 | Primary Health Care | 479 | 100 | 35 to 75 | Choice of moderate or vigorous physical activity |
| Simons‐Morton2001b | 2001 | Primary Health Care | 395 | 0 | 35 to 75 | Choice of moderate or vigorous physical activity |
| Stewart 2001 | 2001 | Primary Health Care | 173 | 34 | 65 to 95 | Moderate physical activity |
| SSCT 2000* | 2000/2003 | Community | 65 | 46.1 | 60 to 81 | Group based endurance and resistance training |
| Dubbert 2002 | 2002 | Primary Health Care | 212 | 99 | 60 to 80 | Walking |
| Green 2002 | 2002 | Primary Health Care | 316 | 47.5 | 20 to 64 | Moderate physical activity |
| Hillsdon 2002 | 2002 | Primary Health Care | 1658 | 48.9 | 45 to 64 | Choice of physical activity or walking |
| Lamb 2002 | 2002 | Primary Health Care | 260 | 48.8 | 40 to 70 | Moderate intensity physical activity and walking |
| Pinto 2002 | 2002 | Primary Health Care | 298 | 28 | 25+ | Moderate physical activity |
| Resnick 2002 | 2002 | Community | 20 | 0 | 84 to 92 | Group based or home based walking |
| Elley 2003 | 2003 | Primary Health Care | 878 | 33.5 | 40 to 79 | Moderate physical activity or walking |
| Inoue 2003 | 2003 | Community | 86 | 0 | 47 to 68 | Moderate physical activity after group programme |
| Marshall 2003 | 2003 | Community | 462 | 42.5 | 40 to 60 | Moderate physical activity |
| Petrella 2003 | 2003 | Primary Health Care | 284 | 52 | 65+ | Moderate physical activity |
| Marshall 2004 | 2004 | Community | 719 | 36 | Mean 43 | Moderate physical activity |
| *Same study with different outcome data (Tsuji ‐ VO2: Fujita ‐ self reported physical activity) |
Interventions in included studies We found a marked heterogeneity in the interventions used in each study. Studies used one, or combination of, one‐to‐one counselling/advice or group counselling/advice; self‐directed or prescribed physical activity; supervised or unsupervised physical activity; home‐based or facility‐based physical activity; ongoing face‐to‐face support; telephone support; written education/motivation material; self monitoring. The intervention was delivered by one or a number of practitioners with various professional backgrounds including physicians, nurses, health educators, counsellors, exercise leaders and peers.
Only one study (SSCT 2000) adopted a structured and supervised approach to their intervention, encouraging participants to cycle on a static bike for 10 to 25 minutes at a pre‐determined intensity, as part of a 2‐hour exercise session. The majority of studies adopted an unstructured and independently performed physical activity regime.
We found the majority of studies contacted participants on at least three or more occasions in the first 4 weeks of the intervention to support and encourage any adoption of physical activity. Studies offered a range of support and follow up to participants between week 5 and final outcome measure (a minimum of 6 months post baseline intervention). The types of follow‐up offered to participants at any point ranged from postal only, telephone only, face‐to‐face meetings, or a mixture of postal, telephone or face‐to‐face.
We found an even distribution of studies using all three approaches as described in our explanation of 'nature of direction' with the more recently published studies preferring self direction or self direction with professional guidance.
Design of included studies Nine studies had a no‐contact control group. Five studies had attention control groups with control participants receiving non‐exercise related health advice. The remaining studies had comparison control groups, where participants received advice or written information about physical activity. In Petrella 2003 the control participants received exercise counselling and advice and were asked to keep a diary.
Eight studies had more than one intervention arm (Dubbert 2002; Harland 1999; Hillsdon 2002; King 1991; Norris 2000; Simons‐Morton 2001a; Simons‐Morton 2001b; Smith 2000). Four studies conducted an analysis of any intervention vs control by combining intervention arms (Harland 1999; Hillsdon 2002; Norris 2000; Smith 2000). We calculated pooled results for intervention arms for three further studies (King 1991; Simons‐Morton 2001a; Simons‐Morton 2001b). Our analysis of effectiveness when combining intervention arms, differed from the original results presented by two studies (King 1991; Simons‐Morton 2001b). We also combined the results of two studies as the final results for control and intervention groups were reported separately by gender and there was no a priori hypothesis that the effect of the intervention would be different for men and women (Calfas 2000; Juneau 1987).
Outcome measures A number of secondary outcome measures, which were not the focus of this review, were also measured and included body mass index (King 1991; Kriska 1986; Petrella 2003; Stewart 2001), health status, smoking status (King 1991; Kriska 1986; Norris 2000), socio‐behavioural constructs (e.g. self efficacy, reduction in barriers to physical activity), social support and 'stage of change' (Calfas 2000; Goldstein 1999; Norris 2000), time spent in flexibility and strength training (Calfas 2000), weight, height, lean body mass, body fat, plasma lipids (Cunningham 1987; Juneau 1987; Kriska 1986), minute ventilation, maximal heart rate, respiratory exchange ratio, blood cholesterol, flexibility, grip strength, health conditions, systolic and diastolic blood pressure (Cunningham 1987; King 1991; Kriska 1986; Petrella 2003), and alcohol consumption (Kriska 1986).
Risk of bias in included studies
Two of the three reviewers independently assessed the quality of each study that met the inclusion criteria. We did not rate studies on whether participants were blind to their allocation to intervention or control groups. This would not be appropriate for studies of this type, as it would be impossible to blind participants to a physical activity intervention. Generation of a formal quality score for each study was completed on a four point scale assigning a value of 0 or 1 to each of the factors described below.
a) Was the randomisation method described? All studies reported using randomisation to allocate participants to intervention and control groups, but only 16 described the method of randomisation. Of these, four studies used cluster‐randomisation, where the unit of randomisation was participating practices (Norris 2000; Elley 2003), matched pairs of participating practices (Goldstein 1999), or workplace shifts (Reid 1979). One study used quasi‐randomisation ‐ days of the week (Smith 2000). All other studies randomised individuals.
b) Was the outcome assessment independent and blind? Twelve studies reported independent and blind outcome assessments (Dubbert 2002; Goldstein 1999; Green 2002; Harland 1999; Hillsdon 2002; King 1991; Marshall 2004; Petrella 2003; Pinto 2002; Simons‐Morton 2001a; Simons‐Morton 2001b; Smith 2000).
c) Was the final outcome measure controlled for baseline physical activity? Sixteen studies reported adjusting their final results for baseline values of physical activity (Calfas 2000; Green 2002; Hillsdon 2002; Inoue 2003; King 1988a; King 1988b; King 1991; Lamb 2002; Marshall 2003a; Norris 2000; Petrella 2003; Pinto 2002; Simons‐Morton 2001a; Simons‐Morton 2001b; Smith 2000; Stewart 2001).
d) Was the analysis an intention‐to‐treat analysis? Fourteen studies reported using an intention‐to‐treat analysis (Elley 2003; Hillsdon 2002; Kriska 1986; Lamb 2002; Lombard 1995; Marshall 2003a; Marshall 2004; Pinto 2002; Reid 1979; Simons‐Morton 2001a; Simons‐Morton 2001bSmith 2000; Stewart 2001; Stevens 1998). The remaining nine studies did not use an intention‐to‐treat analysis but had less than 20% loss to follow up. The proportion of participants in studies that did not perform an intention‐to‐treat analysis who were lost to follow up ranged from 0% to 18.9% (see Table 8).
8. Participation numbers in study recruitment, randomisation and follow up.
| Study ID | Potentially eligible | Eligible (b) | Randomised (c) | Complete (d) | % complete/eligible | % lost to follow up |
| Reid 1979 | Not stated | 146 | 124 | 34 | 23.2 | 72.5 |
| Kriska 1986 | Not stated | 229 | 229 | 229 | 100 | 8.7 |
| Cunningham 1987 | Not stated | 224 | 224 | 200 | 89.2 | 10.7 |
| Juneau 1987 | Not stated | 126 | 120 | 113 | 89.6 | 5.8 |
| King 1988a | Not stated | Not stated | 52 | 47 | Not available | 9.6 |
| King 1988b | Not stated | Not stated | 51 | 48 | Not available | 5.8 |
| King 1991 | 3117 | 1755 | 357 | 300 | 17.1 | 15.9 |
| Lombard 1995 | Approximately 5000 | 135 | 135 | 135 | 100 | 0 |
| Stevens 1998 | 2253 | 827 | 714 | 415 | 50.1 | 41.8 |
| Goldstein 1999 | 2145 | 444 | 355 | 312 | 70.2 | 12.1 |
| Harland 1999 | 2974 | 734 | 520 | 442 | 60.2 | 15.0 |
| Calfas 2000 | Not stated | Not stated | 338 | 315 (data provided by study authors) | Not available | 6.8 |
| Norris 2000 | 1920 | 985 | 847 | 812 | 82.4 | 4.1 |
| Smith 2000 | 2097 | 1214 | 1142 | 1101 | 90.6 | 17.1 |
| Simons‐Morton 2001a | 3910 | NS | 479 | 451 ‐ Self‐reported physical activity, 396 ‐ Cardio‐vascular fitness (data provided by study authors) | Not available | 5.8 ‐ Self‐reported physical activity, 17.3 ‐ Cardio‐vascular fitness |
| Simons‐Morton2001b | 3910 | NS | 395 | 349 ‐ Self‐reported physical activity, 302 ‐ Cardio‐vascular fitness (data provided by study authors) | Not available | 11.6 ‐ Self‐reported physical activity, 23.5 ‐ Cardio‐vascular fitness |
| Stewart 2001 | 1381 | 1053 | 173 | 164 | 15.5 | 5.0 |
| SSCT 2000 | 322 | 209 | 65 | 64 | 30.6 | 1.5 |
| Dubbert 2002 | 576 | 475 | 212 | 181 | 38.1 | 14.6 |
| Green 2002 | 1330 | 361 | 316 | 256 | 70.9 | 18.9 |
| Hillsdon 2002 | 5797 | 1658 | 1658 | 674 | 40.6 | 0.1 |
| Lamb 2002 | ˜2000 | 438 | 260 | 260 | 59.3 | 0 |
| Pinto 2002 | 1738 | 609 | 298 | 238 | 39.0 | 18.4 |
| Resnick 2002 | 120 | Not stated | 20 | 17 | Not stated | 15 |
| Elley 2003 | 2984 | 1364 | 878 | 878 | 64.3 | 0 |
| Inoue 2003 | 376 | 156 | 86 | 84 | 53.8 | 2.3 |
| Marshall 2003 | 927 | 738 | 462 | 462 | 62.6 | 0 |
| Petrella 2003 | 320 | 284 | 284 | 284 | 100 | 0 |
| Marshall 2004 | 1185 | 719 | 719 | 622 | 86.5 | 0 |
| (a) Number of people contacted to determine potential eligibility | (b) Number identified as eligible for study ‐ the number of participants who were assessed as eligible for randomisation into study | (c) Number of people randomised ‐ Number eligible minus refusals, excluded on medical grounds or failed to attend for randomisation | (d) Number with complete data set at final outcome measure | (e) % Number of participants with final outcome measure / Numbers identified as eligible for study |
Twenty‐three studies reported data for the number of those participants who completed their study and the number of participants eligible for the study before randomisation. We calculated the proportion of the eligible participants who completed the study and this percentage ranged from 15.5% to 100%. Table 8 presents the numbers of participants at different stages of each study. This data included the number of participants contacted to determine potential eligibility, number identified as eligible for study, number randomised, number with complete data at final outcome measure, number of participants with complete data at final outcome measure as a proportion of number identified as eligible for study and proportion of participants who were lost to follow‐up.
Details of the intensity of the interventions studied, control interventions used and length of follow‐up are in Table 9 and Table 10.
9. Characteristics of study type and intensity of intervention and follow up.
| Study ID & Author | Programme direction | Supervision | Rate of intervention | Rate of Follow Up | Contact at Follow up |
| Reid 1979 | P ‐ prescribed by professional only | US ‐ physical activity programme was unstructured and performed independently by the participant | High ‐ 3+ occasions | High 3+ occasions between week five and outcome measure. | Mixture of postal, telephone or face‐to‐face |
| Kriska 1986 | P ‐ prescribed by professional only | Mixed ‐ physical activity programme was structured (S) and unstructured (US) | High ‐ 3+ occasions | High 3+ occasions between week five and outcome measure. | Mixture of postal, telephone or face‐to‐face |
| Cunningham 1987 | P ‐ prescribed by professional only | Mixed ‐ physical activity programme was structured (S) and unstructured (US) | High ‐ 3+ occasions | High 3+ occasions between week five and outcome measure. | Face‐to‐face |
| Juneau 1987 | P ‐ prescribed by professional only | US ‐ physical activity programme was unstructured and performed independently by the participant | Low ‐ 0‐1 occasions | Low ‐ 0‐1 occasions between week five and outcome measure. | None |
| King 1988 a | SD self directed only | US ‐ physical activity programme was unstructured and performed independently by the participant | Med ‐ 2 occasions | Low ‐ 0‐1 occasions between week five and outcome measure. | None |
| King 1988 b | SD self directed only | US ‐ physical activity programme was unstructured and performed independently by the participant | High ‐ 3+ occasions | High 3+ occasions between week five and outcome measure. | Telephone only |
| King 1991 | P ‐ prescribed by professional only | Mixed ‐ physical activity programme was structured (S) and unstructured (US) | High ‐ 3+ occasions | High 3+ occasions between week five and outcome measure. | Mixture of postal, telephone or face‐to‐face |
| Lombard 1995 | P ‐ prescribed by professional only | US ‐ physical activity programme was unstructured and performed independently by the participant | Low ‐ 0‐1 occasions | High 3+ occasions between week five and outcome measure. | Telephone only |
| Stevens 1998 | SD self directed only | US ‐ physical activity programme was unstructured and performed independently by the participant | Low ‐ 0‐1 occasions | Low ‐ 0‐1 occasions between week five and outcome measure. | Face‐to‐face |
| Goldstein 1999 | SD+ self directed plus professional guidance | US ‐ physical activity programme was unstructured and performed independently by the participant | Med ‐ 2 occasions | High 3+ occasions between week five and outcome measure. | Mixture of postal, telephone or face‐to‐face |
| Harland 1999 | SD+ self directed plus professional guidance | US ‐ physical activity programme was unstructured and performed independently by the participant | High ‐ 3+ occasions | High 3+ occasions between week five and outcome measure. | Face‐to‐face |
| Calfas 2000 | SD+ self directed plus professional guidance | US ‐ physical activity programme was unstructured and performed independently by the participant | High ‐ 3+ occasions | High 3+ occasions between week five and outcome measure. | Mixture of postal, telephone or face‐to‐face |
| Norris 2000 | SD+ self directed plus professional guidance | US ‐ physical activity programme was unstructured and performed independently by the participant | High ‐ 3+ occasions | High 3+ occasions between week five and outcome measure. | Mixture of postal, telephone or face‐to‐face |
| Smith 2000 | P ‐ prescribed by professional only | US ‐ physical activity programme was unstructured and performed independently by the participant | Med ‐ 2 occasions | Low ‐ 0‐1 occasions between week five and outcome measure. | Mixture of postal, telephone or face‐to‐face |
| Simons‐Morton 2001a | SD+ self directed plus professional guidance | US ‐ physical activity programme was unstructured and performed independently by the participant | High ‐ 3+ occasions | High 3+ occasions between week five and outcome measure. | Mixture of postal, telephone or face‐to‐face |
| Simons‐Morton 2001b | SD+ self directed plus professional guidance | US ‐ physical activity programme was unstructured and performed independently by the participant | High ‐ 3+ occasions | High 3+ occasions between week five and outcome measure. | Mixture of postal, telephone or face‐to‐face |
| Stewart 2001 | SD+ self directed plus professional guidance | US ‐ physical activity programme was unstructured and performed independently by the participant | High ‐ 3+ occasions | High 3+ occasions between week five and outcome measure. | Mixture of postal, telephone or face‐to‐face |
| SSCT 2000 | P ‐ prescribed by professional only | S ‐ physical activity programme was structured and supervised by professional | High ‐ 3+ occasions | High 3+ occasions between week five and outcome measure. | Mixture of postal, telephone or face‐to‐face |
| Dubbert 2002 | SD ‐ self directed only | US ‐ physical activity programme was unstructured and performed independently by the participant | High ‐ 3+ occasions | High 3+ occasions between week five and outcome measure. | Mixture of postal, telephone or face‐to‐face |
| Green 2002 | SD ‐ self directed only | US ‐ physical activity programme was unstructured and performed independently by the participant | High ‐ 3+ occasions | High 3+ occasions between week five and outcome measure. | Telephone only |
| Hillsdon 2002 | SD ‐ self directed only | US ‐ physical activity programme was unstructured and performed independently by the participant | Low ‐ 0‐1 occasions | High 3+ occasions between week five and outcome measure. | Telephone only |
| Lamb 2002 | SD+ self directed plus professional guidance | Mixed ‐ physical activity programme was structured (S) and unstructured (US) | Low ‐ 0‐1 occasions | Low ‐ 0‐1 occasions between week five and outcome measure. | Mixture of postal, telephone or face‐to‐face |
| Pinto 2002 | SD ‐ self directed only | US ‐ physical activity programme was unstructured and performed independently by the participant | High ‐ 3+ occasions | High 3+ occasions between week five and outcome measure. | Mixture of postal, telephone or face‐to‐face |
| Resnick 2002 | P ‐ prescribed by professional only | Mixed ‐ physical activity programme was structured (S) and unstructured (US) | High ‐ 3+ occasions | High 3+ occasions between week five and outcome measure. | Mixture of postal, telephone or face‐to‐face |
| Elley 2003 | SD+ self directed plus professional guidance | US ‐ physical activity programme was unstructured and performed independently by the participant | Low ‐ 0‐1 occasions | Low ‐ 0‐1 occasions between week five and outcome measure. | Mixture of postal, telephone or face‐to‐face |
| Inoue 2003 | SD+ self directed plus professional guidance | Mixed ‐ physical activity programme was structured (S) and unstructured (US) | High ‐ 3+ occasions | Low ‐ 0‐1 occasions between week five and outcome measure. | Postal only |
| Marshall 2003 | SD ‐ self directed only | US ‐ physical activity programme was unstructured and performed independently by the participant | Low ‐ 0‐1 occasions | Low ‐ 0‐1 occasions between week five and outcome measure. | None |
| Petrella 2003 | SD ‐ self directed only | US ‐ physical activity programme was unstructured and performed independently by the participant | Low ‐ 0‐1 occasions | Low ‐ 0‐1 occasions between week five and outcome measure. | Face‐to‐face |
| Marshall 2004 | SD ‐ self directed only | US ‐ physical activity programme was unstructured and performed independently by the participant | Low ‐ 0‐1 occasions | Low ‐ 0‐1 occasions between week five and outcome measure. | None |
| (a) Nature of direction of the intervention | (b) Degree of programme supervision ‐ S ‐ physical activity programme was structured and supervised by professional, US ‐ physical activity programme was unstructured and performed independently by the participant | (c) Frequency of intervention occasions in first four weeks post baseline. | (d) Frequency of follow up contacts. | (e) Type of follow up contacts |
10. Characteristics of study control groups and number of study arms.
| Study ID | No. study arms (a) | Description (b) | Type of control (c) |
| Reid 1979 | 2 | Written advice | Comparison control |
| Kriska 1986 | 2 | Baseline assessment only | No contact |
| Cunningham 1987 | 2 | Continue usual physical activity | No contact |
| Juneau 1987 | 2 | Daily physical activity logs | Comparison control |
| King 1988a | 2 | Weekly exercise monitoring | Comparison control |
| King 1988b | 2 | Self monitoring materials and pulse monitor | Comparison control |
| King 1991 | 4 | Asked not to change physical activity | No contact |
| Lombard 1995 | 2 | Written information | Comparison control |
| Stevens 1998 | 2 | Written information | Comparison control |
| Goldstein 1999 | 2 | Usual care | Attention control |
| Harland 1999 | 5 | Health check | Attention control |
| Calfas 2000 | 2 | General health lectures | Attention control |
| Norris 2000 | 3 | Usual care | No contact |
| Smith 2000 | 3 | Usual care | No contact |
| Simons‐Morton 2001a | 3 | Advice to exercise from physician & health educator | Comparison control |
| Simons‐Morton 2001b | 3 | Advice to exercise from physician & health educator | Comparison control |
| Stewart 2001 | 2 | Wait list | No contact |
| SSCT 2000 | 2 | Attend weekly lecture and indoor games | Attention control |
| Dubbert 2002 | 3 | Wait list | Comparison control |
| Green 2002 | 2 | Self help materials only | Comparison control |
| Hillsdon 2002 | 3 | Wait list | Attention control |
| Lamb 2002 | 2 | Group seminar and advice to exercise | Comparison control |
| Pinto 2002 | 2 | Computer‐based phone calls | Attention control |
| Resnick 2002 | 2 | Routine care | Attention control |
| Elley 2003 | 2 | Usual care and wait list | Attention control |
| Inoue 2003 | 2 | Baseline assessments only | No contact |
| Marshall 2003 | 2 | Assessments only | Attention control |
| Petrella 2003 | 2 | Exercise counselling, advice and record their exercise weekly in a diary | Comparison control |
| Marshall 2004 | 2 | Assessments only | Attention control |
| (a) Number of study arms ‐ This figure is a sum of the number of intervention arms plus control | (b) Description of control group | (c) Type of control group ‐ No contact ‐ Wait list, baseline assessment only, Attention control ‐ Usual care, health check, health advice not physical activity specific, Comparison control ‐ Written information, advice about physical activity, self monitoring materials |
Effects of interventions
Self‐reported physical activity
Reported as a continuous measure Nineteen studies (7,598 participants) reported their main outcome as one of several continuous measures of physical activity (Calfas 2000; Cunningham 1987; Elley 2003; Goldstein 1999; Green 2002; Hillsdon 2002; Inoue 2003; King 1988a; King 1988b; Kriska 1986; Marshall 2003a; Pinto 2002; Resnick 2002a; Simons‐Morton 2001a; Simons‐Morton 2001b; Smith 2000; SSCT 2000; Stevens 1998; Stewart 2001). Measures included estimated energy expenditure (kcals/day, kcals/week of moderate physical activity), total time of physical activity (mean mins/week of moderate physical activity) and mean number of occasions of physical activity in past four weeks. The pooled effect of these studies was positive but moderate (SMD 0.28, 95% CI 0.15 to 0.41) with significant heterogeneity in observed effects (I2 = 83.5%). Seven studies reported positive effects (Cunningham 1987; Elley 2003; King 1988a; Kriska 1986; Stevens 1998; SSCT 2000; Stewart 2001) (see Table 11).
11. Outcome measure, SMD, 95% CI for studies with continuous self‐reported PA.
| Study ID | Outcome measure | SMD | 95% CI | Outcome direction | Study quality score |
| Kriska 1986 | Kcal/week | 0.54 | 0.28 to 0.80 | + favours intervention | 1 |
| Cunningham 1987 | Mins/day vigorous physical activity (>4.9 METS) | 0.40 | 0.13 to 0.67 | + favours intervention | 0 |
| King 1998a | Exercise occasions per month (30 Mins. per session) | 0.64 | 0.05 to 1.23 | + favours intervention | 2 |
| King 1988b | Exercise occasions per month (30 Mins. per session) | 0.37 | ‐0.21 to 0.94 | 0 no effect | 2 |
| Stevens 1998 | Exercise occasions per month (greater than 20 Mins per session) | 0.84 | 0.68 to 0.99 | + favours intervention | 2 |
| Goldstein 1999 | Physical Activity Scale for Elderly (PASE Scale) | 0.02 | ‐0.20 to 0.24 | 0 no effect | 0 |
| Calfas 2000 | Kcal/kg/week | 0.12 | ‐0.10 to 0.34 | 0 no effect | 1 |
| Smith 2000 | Mins/week | 0.08 | ‐0.04 to 0.21 | 0 no effect | 3 |
| Simons‐Morton 2001a | Kcal/kg/day | 0.18 | ‐0.02 to 0.38 | 0 no effect | 4 |
| Simons‐Morton 2001a | Kcal/kg/day | 0.08 | ‐0.14 to 0.30 | 0 no effect | 4 |
| Stewart 2001 | Kcal/day | 0.32 | 0.02 to 0.63 | + favours intervention | 3 |
| SSCT 2000 | Total daily energy expenditure (kcal/kg/day) | 1.18 | 0.64 to 1.72 | + favours intervention | 1 |
| Green 2002 | Self reported physical activity PACE score | 0.24 | 0.00 to 0.49 | 0 no effect | 3 |
| Hillsdon 2002 | Energy expenditure (kcal/kg/week) | 0.06 | ‐0.04 to 0.16 | 0 no effect | 3 |
| Pinto 2002 | Moderate intensity physical activity (kcal/week) | 0.06 | ‐0.19 to 0.32 | 0 no effect | 2 |
| Resnick 2002 | Energy expenditure | 0.72 | ‐0.29 to 1.72 | 0 no effect | 0 |
| Elley 2003 | Energy expenditure (kcal/kg/week) | 0.19 | 0.06 to 0.32 | + favours intervention | 1 |
| Inoue 2003 | Moderate intensity physical activity (kcal/week) | 0.24 | ‐0.19 to 0.67 | 0 no effect | 1 |
| Marshall 2003 | Total physical activity (hrs/week) | 0.06 | ‐0.12 to 0.24 | 0 no effect | 2 |
| METS = Energy cost of physical activity measured at cost of basal metabolic rate. |
Studies with positive SMDs used a range of different intervention approaches with varying effect sizes. Kriska 1986 found that encouraging walking via an 8‐week training programme, followed by a choice of group or independent walking, plus follow‐up phone calls and incentives resulted in a mean increase of 479 kcal/week (95% CI 249 to 708) of physical activity of all intensities. Cunningham 1987 found that encouragement to attend three group exercise sessions per week and perform an additional weekly exercise session at home resulted in an additional mean 53.7 minutes of vigorous physical activity per day (95% CI 18.09 to 89.31).
King 1988a found a mean increase of 3.90 exercise sessions per month (95% CI 0.43 to 7.37), at 6 months, following 30 minutes of baseline instruction (15 minutes of advice and a 15 minute video about exercise training), and daily self monitoring of physical activity using exercise logs returned to staff every month. These additional sessions were approximately equivalent to 101 minutes of moderate intensity physical activity per week. Stevens 1998 saw a net difference between intervention and control groups of 2.31 'sessions' (one session was at least 20 minutes of continuous physical activity) of moderate or vigorous exercise per month (95% CI 1.91 to 2.71). At an initial meeting with a community exercise development officer intervention participants were encouraged to extend a physical activity that they already did rather than start a new activity. A further meeting was offered ten weeks later to support and encourage any changes. Stewart 2001 reported a significant net difference of 82 kcal per day between the intervention and control arms (95% CI 73.9 to 90.1). The intervention group received face‐to‐face counselling based on social cognitive theory (Bandura 1986). In addition they were offered further individual follow up appointments, educational materials, phone calls and monthly workshops about physical activity.
Elley 2003 reported a between group mean difference of 2.67 kcal/kg/wk (95% CI 0.48 to 4.86). The authors estimate this was equivalent to a net difference of 247 kcals/week between groups. The intervention group received motivational counselling from their general practitioner, followed by three follow up phone calls from a local exercise specialist, plus written materials. Participants were asked to choose their own physical activity.
SSCT 2000 reported a large increase in mean self‐reported physical activity in their intervention group. However the physical activity regime was very prescriptive. Participants were encouraged to attend at least two from three 2‐hour exercise classes per week, held at a local community centre. The class contained endurance and resistance training typically involving 10‐25 minutes of static cycling at prescribed heart rate reserve, with intensity monitored by heart monitors. In addition to attending classes participants were asked to monitor their walking behaviour using pedometers.
No statistically significant effects were observed for the other 12 studies (Calfas 2000; Goldstein 1999; Green 2002; Hillsdon 2002; Inoue 2003; King 1988b; Marshall 2003a; Pinto 2002; Resnick 2002a; Simons‐Morton 2001a; Simons‐Morton 2001b; Smith 2000). No studies had effects that favoured controls. Reported as a dichotomous measure Ten studies (3595 participants) reported physical activity as a dichotomous measure which represented achievement or not of a predetermined level of physical activity (Dubbert 2002; Harland 1999; Lamb 2002; Lombard 1995; Marshall 2004; Norris 2000; Pinto 2002; Reid 1979; Simons‐Morton 2001a; Simons‐Morton 2001b). The pooled odds ratio of these studies was positive but modest (OR 1.33, 95% CI 1.03 to 1.72) with significant heterogeneity in observed effects (I2 = 53.4%). Only two studies reported a significantly positive effect (Dubbert 2002; Lombard 1995). Lombard 1995 found that participants who received a high frequency of follow up telephone calls (10 calls over 12 weeks) were more successful at changing their walking behaviour than participants who did not receive telephone calls (OR 10.95, 95% CI 1.42 to 84.15). Dubbert 2002 found that adult participants who received a video, walking plan, weekly walking diary, financial incentive for completing diary, plus follow up phone calls were more successful at adhering to a 3 walks per week programme that participants who did not receive any phone calls (OR 2.31, 95% CI 1.15 to 4.66) (see Table 12).
12. Outcome measure, OR, 95% CI for studies with dichotomous physical activity.
| Study ID | Outcome measure | OR | 95% CI | Outcome direction | Study quality score |
| Reid 1979 | Improving physical activity compliance and fitness increase (OR for a participant achieving "prescribed compliance" if they reported exercising at least twice a week and increased their VO2 by +9.5% over baseline level) | 1.68 | 0.72 to 3.92 | 0 no effect | 1 |
| Lombard 1995 | Achieving at least 3 occasions of walking for at least 20 minutes per week (OR for a participant walking on least 3 occasions per week for at least 20 minutes per occasion) | 10.95 | 1.42 to 84.15 | + favours treatment | 1 |
| Harland 1999 | Improving physical activity index score by at least one level (OR for a participant increasing their number of sessions of moderate and vigorous physical activity lasting a minimum of 20 minutes in the previous four weeks, used in a physical activity index score) | 1.18 | 0.69 to 2.04 | 0 no effect | 2 |
| Norris 2000 | Increasing physical activity by at least 30 minutes per week (OR for a participant increasing their level of any type of physical activity by at least 30 minutes per week compared to their baseline level) | 0.79 | 0.60 to 1.04 | 0 no effect | 2 |
| Simons‐Morton 2001a | Meeting CDC recommendation for physical activity (Odds ratio for a participant meeting 30 minutes of moderate to vigorous intensity physical activity (at least 3 METS) at least 5 days a week, 30 minutes of vigorous physical activity (at least 5 METS) at least 3 days a week, or at least 2 kcal·kg‐1·day‐1 in moderate to vigorous physical activity) | 1.63 | 0.98 to 2.71 | 0 no effect | 4 |
| Simons‐Morton 2001b | Meeting CDC recommendation for physical activity (Odds ratio for a participant meeting 30 minutes of moderate to vigorous intensity physical activity (at least 3 METS) at least 5 days a week, 30 minutes of vigorous physical activity (at least 5 METS) at least 3 days a week, or at least 2 kcal·kg‐1·day‐1 in moderate to vigorous physical activity) | 1.26 | 0.68 to 2.34 | 0 no effect | 4 |
| Dubbert 2002 | Achieving exercise adherence goal of walking 20 min 3 days/week | 2.31 | 1.15 to 4.66 | + favours treatment | 1 |
| Lamb 2002 | Achieving more than 120 minutes per week moderate physical activity | 1.51 | 0.84 to 2.74 | 0 no effect | 3 |
| Pinto 2002 | Meeting CDC/ACSM recommendation for moderate physical activity | 1.24 | 0.64 to 2.38 | 0 no effect | 2 |
| Marshall 2004 | Achieving a sufficient level of physical activity | 1.22 | 0.89 to 1.69 | 0 no effect | 1 |
| CDC = Centre for disease control |
No effect was found in eight studies (Harland 1999; Lamb 2002; Marshall 2004; Norris 2000; Pinto 2002; Reid 1979; Simons‐Morton 2001a; Simons‐Morton 2001b). No studies had effects that favoured controls. Cardio‐respiratory fitness In addition to self‐reported physical activity, 11 studies (2195 participants) examined the effect of their intervention on cardio‐respiratory fitness (Cunningham 1987; Dubbert 2002; Juneau 1987; King 1988a; King 1988b; King 1991; Lamb 2002; Petrella 2003; Simons‐Morton 2001a; Simons‐Morton 2001b; SSCT 2000) (see Table 13). The pooled effect was again positive and moderate with significant heterogeneity in the observed effects (SMD 0.52 95% CI 0.14 to 0.90). Five studies (1359 participants) had significant positive effects that favoured treatment (Cunningham 1987; Juneau 1987; Petrella 2003; Simons‐Morton 2001b; SSCT 2000). Cunningham 1987 reported that recently retired men who were offered supervised exercise sessions increased their fitness by a greater amount than controls who continued with their usual physical activity programmes (SMD 0.44 95% CI 0.16 to 0.72). Juneau 1987 found a mean increase in fitness (SMD 1.49 95% CI 1.07 to 1.91) for participants who received a combination of a 30‐minute consultation, an educational video, information on using a heart rate monitor and a daily physical activity log, compared to controls. Simons‐Morton 2001b found that women who received an intensive mixture of behavioural counselling, support materials and telephone calls (assistance + counselling arms) were more likely to increase their fitness (SMD 0.47, 95% CI 0.23 to 0.71) than women who received a less intensive intervention (advice arm only). Petrella 2003 evaluated the effects of a fitness assessment using a step test and counselling from physician, plus a simple target heart rate goal and recording their physical activity in a diary on cardio‐respiratory fitness. Controls received the same intervention without the heart rate goal setting. The standardised mean difference was 1.87 (95% CI 1.59 to 2.15).
13. Outcome measure, SMD, 95% CI for studies with continuous cardio‐respir fitness.
| Study ID | Outcome measure | SMD | 95% CI | Outcome direction | Study quality score |
| Cunningham 1987 | VO2 | 0.44 | 0.16 to 0.72 | + favours treatment | 0 |
| Juneau 1987 | VO2 | 1.49 | 1.07 to 1.91 | + favours treatment | 0 |
| King 1988a | VO2 | ‐0.16 | ‐0.74 to 0.42 | 0 no effect | 2 |
| King 1988b | VO2 | 0.15 | ‐0.42 to 0.72 | 0 no effect | 2 |
| King 1991 | VO2 | 0.17 | ‐0.09 to 0.43 | 0 no effect | 3 |
| Simons‐Morton 2001a | VO2 | 0.14 | ‐0.07 to 0.35 | 0 no effect | 4 |
| Simons‐Morton 2001b | VO2 | 0.47 | 0.23 to 0.71 | + favours treatment | 4 |
| SSCT 2000 | VO2 | 1.14 | 0.61 to 1.68 | + favours treatment | 1 |
| Dubbert 2002 | VO2 | ‐0.06 | ‐0.37 to 0.25 | 0 no effect | 1 |
| Lamb 2002 | VO2 | 0.05 | ‐0.20 to 0.29 | 0 no effect | 3 |
| Petrella 2003 | VO2 | 1.87 | 1.59 to 2.15 | + favours treatment | 3 |
Although King 1991 reported a significant difference in VO2 max between intervention and control group at 12‐months follow‐up this difference did not remain when based on the standardised mean difference of the pooled intervention arms (SMD 0.17, 95% CI ‐0.09 to 0.43). In one other study (King 1988b), the author reported a significant difference in the change in fitness between groups, which did not remain significant when based on standardised mean differences at 12 month follow up using their published data. This may be an effect of pooling study arms.
Adverse events Eight studies reported data on adverse events. Only one study found a difference in the rate of adverse events between the intervention and control groups. Reid 1979 reported the rate of job‐related injuries was four times higher in the control group compared to the intervention group. The other seven studies reported no significant difference in rates of musculoskeletal injury (fractures and sprains), falls, illness and potential cardiovascular events between groups (Dubbert 2002; Elley 2003; King 1991; Resnick 2002a; Simons‐Morton 2001a; Simons‐Morton 2001b; SSCT 2000).
Sensitivity analysis by study quality We examined the pooled effects for the three types of outcome data (self‐reported physical activity, dichotomous and cardio‐respiratory fitness outcomes) by an assessment of study quality. High quality studies scored more than 2 on the quality scale. A score of 2 or less was categorised as low quality. For the 19 studies that reported continuous outcomes for physical activity six were classified as high quality (comparison 02 01). The pooled effect of these interventions was again positive with no significant heterogeneity in the observed effects; the standardised mean difference was 0.11 (95% CI 0.04 to 0.17). Lower quality studies also had a positive pooled effect but with significant heterogeneity in the observed effects; the standardised mean difference was 0.36 (95% CI 0.17 to 0.56).
We found three high quality scoring studies from the 10 studies that reported dichotomous outcome data for self‐reported physical activity (comparison 02 02). The pooled odds ratio of these three studies was positive but modest (OR 1.48, 95% CI 1.07 to 2.06) with no significant heterogeneity in observed effects.
We found five high quality studies from the 11 studies that reported continuous outcome data for cardio‐respiratory fitness (comparison 02 03). The pooled effects of these studies was not significant and there was significant heterogeneity (SMD 0.54, 95% CI ‐0.07 to 1.14). We noted two studies had a string effect on the pooled analysis (Juneau 1987; Petrella 2003).
Secondary objectives
a) Are more intense interventions more effective in changing physical activity than less intense interventions? Two studies attempted to investigate the effect of increasing intervention intensity. In Simons‐Morton 2001a and Simons‐Morton 2001b the three groups received different levels of intervention. The control group (advice) received physician advice to achieve the recommended level for exercise, then referral to an on‐site health educator. At this appointment the health educator provided educational materials and repeated the physician advice to exercise with further follow‐up appointments repeating this advice. No other follow‐up activities were offered. The assistance group received the same advice from a physician and also received a 30‐40 minute counselling session the health educator conducted, including a videotape and action planning. Participants then received follow‐up phone calls, interactive mail, an electronic step counter, and monthly monitoring cards, which were returned to the health educator. Follow‐up mail and incentives were sent to all participants. The counselling group received all of the components of the advice and assistance group with additional bi‐weekly telephone calls for 6 weeks and then monthly telephone calls up to 12 months. Frequency of telephone calls for the final 12 months of the study was negotiated between the participant and their health educator. Weekly behavioural classes on skills for adopting and maintaining physical activity were also offered to this group. In women, the addition of behavioural counselling, follow up support and materials produced a significant difference in fitness compared to the control groups. In men addition of these components did not lead to greater change (Simons‐Morton 2001a and Simons‐Morton 2001b).
b) Are specific components of interventions associated with changes in physical activity behaviour? We stratified the behavioural components of the interventions, according to a number of characteristics. These characteristics were the degree of nature of direction (the extent to which physical activity was prescribed or self‐directed) and the level of on‐going professional support (frequency of follow up after week five of the study). Although there were insufficient studies to statistically test the difference in observed effects between these various study characteristics, the significant heterogeneity in reported effects was reduced when physical activity was self‐directed with some professional guidance and when there was on‐going professional support (in studies with continuous outcome measures for self‐reported physical activity).
c) Are short term changes in physical activity or fitness maintained at 12 months? Six studies reported outcomes more than 6 months after the initial intervention (e.g. at least a measure of the primary outcome at 6 months and 12 months post intervention). In King 1991 improvements in physical activity and cardio‐respiratory fitness at 6 months were maintained at 12 months for cardio‐respiratory fitness only. Simons‐Morton 2001a and Simons‐Morton 2001b presented data for cardio‐respiratory fitness and self‐reported physical activity at 6 and 24 months. All three study arms increased their cardio respiratory fitness and self reported levels of physical activity between baseline and 6 months. However there were no significant differences between groups. At 24 months there was a significant difference in VO2 max between participants who received assistance and counselling compared to the advice group for women only (Simons‐Morton 2001b). Calfas 2000 reported outcomes at 12 and 24 months with no significant effect observed at either time points. Lamb 2002 reported no significant effect in the likelihood of increasing walking at 6 and 12 months. Petrella 2003 reported a significant increase in cardio‐respiratory fitness at 6 months and this effect was further increased at 12 months.
d) Is the promotion of some types of physical activity more likely to lead to change than other types of physical activity? We were unable to determine if any type of physical activity is more likely to be adopted than any other type of physical activity, (e.g. walking, jogging or running) as the studies were not designed to examine this question and as such generally did not report exactly what type of physical activity was performed. e) Are home‐based interventions more successful than facility‐based interventions? No study specifically examined this question. However King 1991 compared the difference in adherence to prescribed physical activity sessions between participants who were prescribed home‐based versus facility‐based exercise. A greater number of participants completed at least 75% of prescribed exercise sessions in both home‐based arms compared to the facility‐based arms (P < 0.05). This improved adherence to the home‐based exercise sessions was not reflected in greater improvements in fitness. f) Are interventions more successful with particular participant groups? Nine studies examined the differential effects of the interventions within various sub‐groups.
Eight studies looked at the effect of gender (Calfas 2000; Elley 2003; Juneau 1987; King 1991; Petrella 2003; Simons‐Morton 2001a; Simons‐Morton 2001b; Stewart 2001). Greater effects were seen for improvements in cardio‐respiratory fitness for women as compared to men in King 1991 and Simons‐Morton 2001a and Simons‐Morton 2001b, while Juneau 1987 reported a greater increase in VO2 max in men than women. Elley 2003 reported greater increases in men compared to women in the intervention group in reported physical activity.
Two studies found no differential effects between high and low levels of baseline self‐reported physical activity (Petrella 2003; Stewart 2001). No effects were seen for age (above or below 75 years) in Stewart 2001. The same study found a greater increase in physical activity for overweight participants (BMI more than 27.0), compared with participants who were not overweight (Stewart 2001). Petrella 2003 examined differential effects of their intervention in four sub groups (i) gender, (ii) age (above versus below 70 years), (iii) chronic health conditions (less than two reported health conditions versus more two or more health conditions) and (iv) BMI (<27, 27‐31, >32 BMI). The intervention group showed a greater improvement in cardio‐respiratory fitness compared to the control group, in a between group analysis regardless of gender, age, having more than 2 chronic health conditions and BMI >32.
Discussion
Our updated review suggests that physical activity interventions have a positive moderate sized effect on increasing self‐reported physical activity and measured cardio‐respiratory fitness, at least in the short to mid‐term. Any conclusions drawn from this review require some caution given the significant heterogeneity in the observed effects. Despite the heterogeneity between the studies, there is some indication that a mixture of professional guidance and self direction plus on‐going professional support leads to more consistent effect estimates. The long‐term effectiveness of these interventions is not established as the majority of studies stopped after 12 months.
These conclusions differ from the findings of previous systematic reviews (Hillsdon 1996; Hillsdon 1999). Earlier reviews concluded that interventions that encouraged home‐based activity were more effective than facility‐based activity interventions. This review used more rigid inclusion criteria (for example outcome measures with at least 6 months follow‐up) and subsequently excluded some studies included in these previous reviews. We were also able to collect unpublished data from study authors and this allowed us to perform a quantitative analysis using standardised mean differences for effects as opposed to just descriptions alone. The conclusions are similar to another published review (Hillsdon 2004). However this review was not a synthesis of primary studies but rather a synthesis of high‐quality systematic reviews and meta‐analyses of studies to increase physical activity among adults. It assessed studies in particular settings and found strong evidence of effectiveness of interventions within healthcare and community settings, particularly brief advice from a health professional, supported by written materials, which is likely to be effective in producing a modest, short‐term (6‐12 weeks) effect on physical activity (Hillsdon 2004).
The findings of this review are in contrast to the conclusions of a review produced by the Center for Disease Control (Kahn 2002). Kahn 2002 examined the effectiveness of individual‐based behavioural interventions for the promotion of physical activity. The review calculated effects as the net percent change from baseline ‐ the median change scores. In 10 studies (using continuous outcome measures of self‐reported physical activity), the authors found a median net increase of 35.4% (interquartile range, 16.7% to 83.3%). Ten studies measured change in the time spent in physical activity, with a net median increase of 64.3% (interquartile range, 1.2% to 85.5%). Four studies measured change in VO2max with a median increase of 6.3% (interquartile range, 5.1% to 9.8%). Overall the authors concluded that there was "good" evidence to suggest that this type of intervention was effective in increasing physical activity. However the authors included studies with shorter periods of follow up, non randomised studies (including uncontrolled before and after studies), and did not take account of loss to follow up. Only one study, King 1991, was shared by both reviews.
Quality of the evidence The quality of the studies in this current review was limited by a lack of intention‐to‐treat analysis and failure to examine the interaction between baseline levels of physical activity and exposure to the intervention. Only six studies (Green 2002; Hillsdon 2002; Lamb 2002; Petrella 2003; Simons‐Morton 2001a; Simons‐Morton 2001b) achieved all of the quality criteria. The observed effects were smaller but more consistent in studies with higher quality scores.
Internal validity We found three main weaknesses to the studies in terms of their internal validity. First, none of the studies were able to blind participants to their allocation to intervention at baseline. However this criterion is not appropriate to such studies. It is very difficult to blind a participant to their study group if exercise is the intervention. This element of quality is more appropriate to pharmaceutical interventions where blinding for both researchers and participants reduces the risk of selection bias. Second, studies failed to state their randomisation methods. And third, the studies did not use personnel to collect main outcome measures that were independent and blinded to group allocation.
Misclassification of physical activity also threatens internal validity of studies. The insensitivity of self‐reported physical activity measures leads to less precision in its measurement and increases the variance in measures of behaviour. As intervention and control group participants completed the same self‐report measure, any misclassification is likely to be non‐differential leading to an attenuation of the effect of the intervention. This problem would not apply to measures of cardio‐respiratory fitness. External validity Limitations in the external validity of the studies relate to recruitment and screening of participants and the generalisability of the interventions into everyday practice.
The majority of the studies in the review recruited volunteers, for example people replying to newspaper advertisements and the interventions may be less effective in non‐volunteer populations recruited, for example, from primary care settings. Often participants had to agree to extensive screening prior to randomisation and, as a consequence, the people who finally participated in the study were likely to be highly motivated. Participants who were randomised in Project ACT (Simons‐Morton 2001a; Simons‐Morton 2001b) had already undergone three screening visits. Participants in other studies attended pre‐study promotional events plus a baseline assessment (Stewart 2001) or attended two screening interviews (Inoue 2003). By contrast, only three studies, Stevens 1998, Hillsdon 2002 and Elley 2003, randomised all participants at the point of invitation to the study prior to them agreeing to participate. This method is called Zelen randomisation and is adopted to reduce non‐consent rates (Zelen 1990).
The physicians in the studies based in a primary healthcare setting may have been more motivated to deliver the interventions than might be observed in a non‐trial setting. We noted that studies described 'recruiting' participating practices and physicians and reported using financial incentives to physicians and practice staff during the time of the study.
We noted a large drop out of participants between the recruitment, eligibility screening and randomisation phases of studies (data presented in Table 8). This drop out would limit the possible effects of such interventions and the generalisability of the studies.
Many interventions provided components which would be difficult to deliver in usual practice as they would demand large resources. For example studies offered a choice of physical activities plus offered initial support in supervised programmes of physical activity, as well as letting participants choose to exercise independently of professional support.
Only four studies reported data at 2 years, with one study demonstrating maintenance of improvement in cardio‐respiratory fitness (Simons‐Morton 2001b). Evidence for the long‐term effectiveness of interventions is urgently required.
The participants in the studies reviewed were generally white, well educated and middle aged and it is possible that the observed effects may be different in the wider population. There were no studies in this review that examined the effectiveness of interventions in minority groups of any kind.
Authors' conclusions
Implications for practice.
There is some evidence to suggest that interventions designed to increase physical activity can lead to moderate short and mid‐term increases in physical activity, at least in middle age. Due to the clinical and statistical heterogeneity of the studies, only limited conclusions can be drawn about the effectiveness of individual components of the interventions. Nevertheless interventions which provide people with professional guidance about starting an exercise programme and then provide on going support may be more effective in encouraging the uptake of physical activity. There is no evidence that such interventions will reduce physical activity or cause other harm. There is only very limited evidence of the long‐term effectiveness of interventions.
Implications for research.
Existing evidence about the effectiveness of physical activity interventions for sedentary adults in the general population is limited by the recruitment of motivated volunteers, and the problems of measuring of physical activity using self report. No studies examined the effect of interventions on participants from varying socioeconomic or ethnic groups. There is also an urgent need for studies with cost‐effectiveness data. In order to better understand the independent effect of individual programme components, longer studies with greater power are required. High quality studies are required with larger numbers, with a greater variety of participants, and with longer follow‐up periods. In this review we have been able to describe the quantity of the interventions but were unable to describe the quality of the components of the interventions. Future reports of studies should provide greater detail on the nature of the professional who delivered the interventions, the theoretical basis of the intervention and how the theory was translated into practice.
What's new
| Date | Event | Description |
|---|---|---|
| 20 November 2012 | Review declared as stable | This review is being split into three new reviews: Face to face interventions for promoting physical activity; Face to face versus remote and web 2.0 interventions for promoting physical activity; Remote and web 2.0 interventions for promoting physical activity. |
History
Protocol first published: Issue 3, 2001 Review first published: Issue 1, 2005
| Date | Event | Description |
|---|---|---|
| 14 March 2012 | Amended | Additional tables linked to text |
| 9 September 2008 | Amended | Converted to new review format. |
| 26 April 2005 | New citation required and conclusions have changed | Substantive amendment |
Acknowledgements
Stewart 2001 provided clarification regarding the means and standard deviations for the weekly caloric expenditure in all and moderate intensity physical activity at 12 months follow up.
Smith 2000 provided the mean change and standard deviation of the total minutes of activity for the three arms of the study at 7‐8 months follow‐up.
Norris 2000 was unable to provide the standard deviations for various physical activity outcomes.
Calfas 2000 confirmed the final numbers of participants at the 24‐month follow‐up.
Simons‐Morton 2001a and Simons‐Morton 2001b provided the standard errors for the physical activity and VO2max values for men and women in all three study arms at 6‐, 12‐ and 24‐ months follow‐up.
Dubbert 2002 confirmed the numbers of participants in each study arm at baseline, 6 months and 12 months.
Marshall 2003a confirmed the details of the means and standard deviations of total average physical activity time (hrs/wk) for both study arms at 6 months follow‐up.
Data and analyses
Comparison 1. Pooled effects.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Studies with continuous data for self‐reported physical activity | 19 | 7598 | Std. Mean Difference (IV, Random, 95% CI) | 0.28 [0.15, 0.41] |
| 2 Studies with dichotomous data for self‐reported physical activity | 10 | 3595 | Odds Ratio (M‐H, Random, 95% CI) | 1.33 [1.03, 1.72] |
| 3 Studies with continuous data for cardio‐respiratory fitness | 11 | 2195 | Std. Mean Difference (IV, Random, 95% CI) | 0.52 [0.14, 0.90] |
1.1. Analysis.
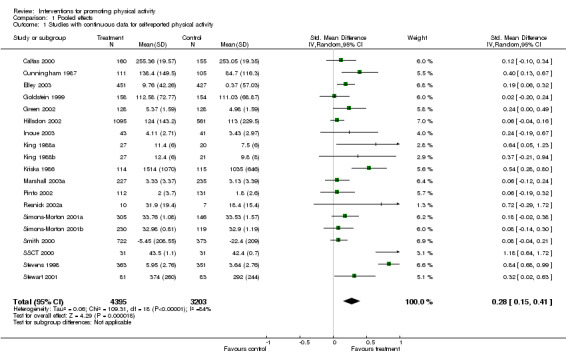
Comparison 1 Pooled effects, Outcome 1 Studies with continuous data for self‐reported physical activity.
1.2. Analysis.
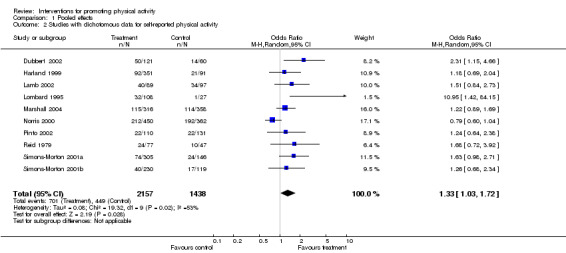
Comparison 1 Pooled effects, Outcome 2 Studies with dichotomous data for self‐reported physical activity.
1.3. Analysis.
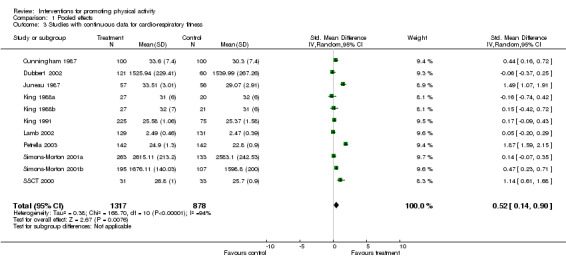
Comparison 1 Pooled effects, Outcome 3 Studies with continuous data for cardio‐respiratory fitness.
Comparison 2. Sensitivity anaylsis.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Study quality ‐ continuous data for self‐reported physical activity | 19 | 7598 | Std. Mean Difference (IV, Random, 95% CI) | 0.28 [0.15, 0.41] |
| 1.1 Higher quality | 6 | 3971 | Std. Mean Difference (IV, Random, 95% CI) | 0.11 [0.04, 0.17] |
| 1.2 Lower quality | 13 | 3627 | Std. Mean Difference (IV, Random, 95% CI) | 0.36 [0.17, 0.56] |
| 2 Study quality ‐ dichotomous data for self‐reported physcial activity | 10 | 3595 | Odds Ratio (M‐H, Random, 95% CI) | 1.33 [1.03, 1.72] |
| 2.1 Higher quality | 3 | 986 | Odds Ratio (M‐H, Random, 95% CI) | 1.48 [1.07, 2.06] |
| 2.2 Lower quality | 7 | 2609 | Odds Ratio (M‐H, Random, 95% CI) | 1.31 [0.93, 1.85] |
| 3 Study quality ‐ continuous data for cardio‐respiratory fitness | 11 | 2195 | Std. Mean Difference (IV, Random, 95% CI) | 0.52 [0.14, 0.90] |
| 3.1 Higher quality | 5 | 1542 | Std. Mean Difference (IV, Random, 95% CI) | 0.54 [‐0.07, 1.14] |
| 3.2 Lower quality | 6 | 653 | Std. Mean Difference (IV, Random, 95% CI) | 0.50 [‐0.01, 1.02] |
2.1. Analysis.
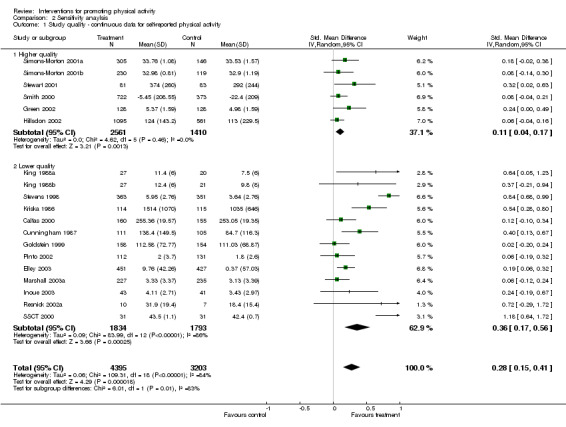
Comparison 2 Sensitivity anaylsis, Outcome 1 Study quality ‐ continuous data for self‐reported physical activity.
2.2. Analysis.
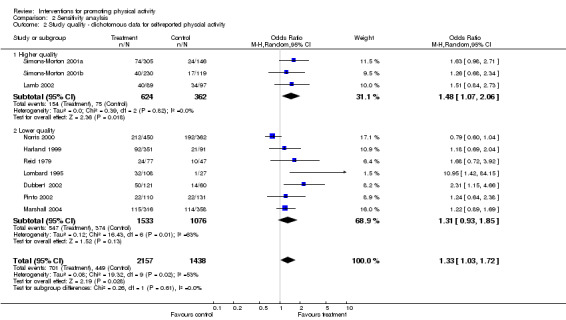
Comparison 2 Sensitivity anaylsis, Outcome 2 Study quality ‐ dichotomous data for self‐reported physcial activity.
2.3. Analysis.
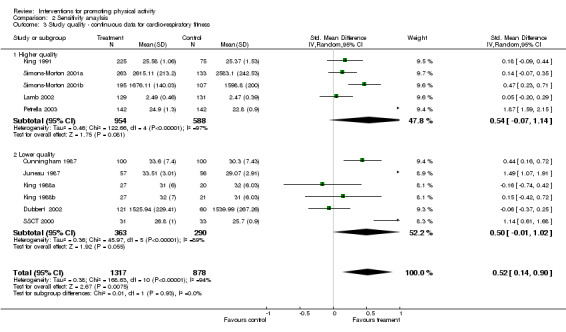
Comparison 2 Sensitivity anaylsis, Outcome 3 Study quality ‐ continuous data for cardio‐respiratory fitness.
Comparison 3. Sub group analysis.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Nature of direction ‐ self‐reported physical activity | 19 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 1.1 Self directed only | 8 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.2 Self directed plus professional guidance | 6 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.3 Prescribed by professional only | 5 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2 Nature of direction ‐ cardio‐respiratory fitness | 11 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 2.1 Self directed only | 4 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.2 Self directed plus professional guidance | 3 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.3 Prescribed by professional only | 4 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3 Frequency of intervention occasions ‐ self‐reported physical activity | 19 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 3.1 Low ‐ 0‐3 occasions | 10 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.2 High ‐ 4+ occasions | 9 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4 Frequency of intervention occasions ‐ dichotomous data | 10 | Odds Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 4.1 Low ‐ 0‐3 occasions | 3 | Odds Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.2 High ‐ 4+ occasions | 7 | Odds Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5 Frequency of intervention occasions ‐ cardio‐respiratory fitness | 11 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 5.1 Low ‐ 0‐3 occasions | 5 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.2 High ‐ 4+ occasions | 6 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 6 Frequency of follow‐up ‐ self‐reported physical activity | 19 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 6.1 Low ‐ 0‐4 occasions | 7 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 6.2 High ‐ 5+ occasions | 12 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 7 Frequency of follow‐up ‐ cardio‐respiratory fitness | 11 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 7.1 Low ‐ 0‐4 occasions | 4 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 7.2 High ‐ 5+ occasions | 7 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 8 Frequency of follow‐up ‐ dichotomous data | 10 | Odds Ratio (M‐H, Random, 95% CI) | Totals not selected | |
| 8.1 Low ‐ 0‐4 occasions | 4 | Odds Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 8.2 High ‐ 5+ occasions | 6 | Odds Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 9 Degree of supervision ‐ self‐reported physical activity | 19 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 9.1 Unsupervised | 8 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 9.2 Supervised + | 11 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 10 Degree of supervison ‐ cardio‐respiratory fitness | 11 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 10.1 Unsupervised | 7 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 10.2 Supervised + | 3 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 10.3 Supervised only | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] |
3.1. Analysis.
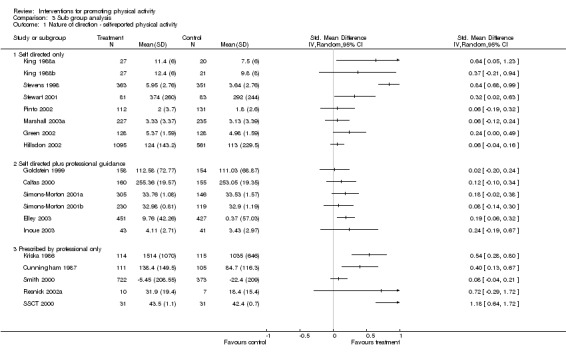
Comparison 3 Sub group analysis, Outcome 1 Nature of direction ‐ self‐reported physical activity.
3.2. Analysis.
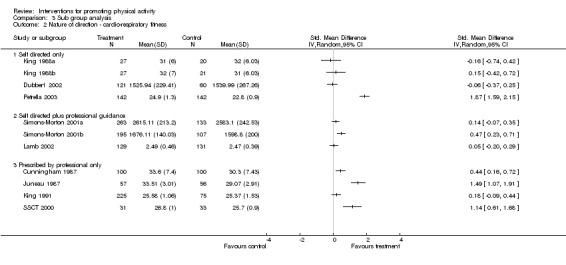
Comparison 3 Sub group analysis, Outcome 2 Nature of direction ‐ cardio‐respiratory fitness.
3.3. Analysis.
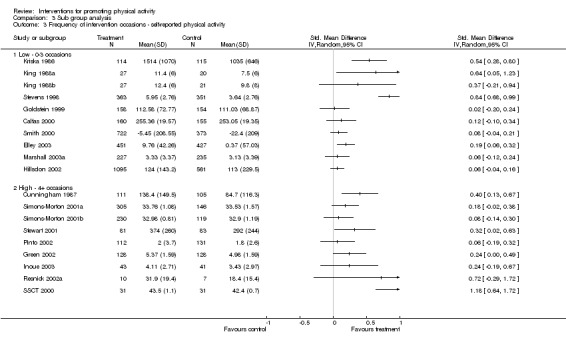
Comparison 3 Sub group analysis, Outcome 3 Frequency of intervention occasions ‐ self‐reported physical activity.
3.4. Analysis.
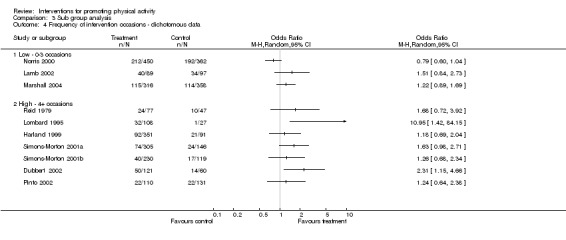
Comparison 3 Sub group analysis, Outcome 4 Frequency of intervention occasions ‐ dichotomous data.
3.5. Analysis.
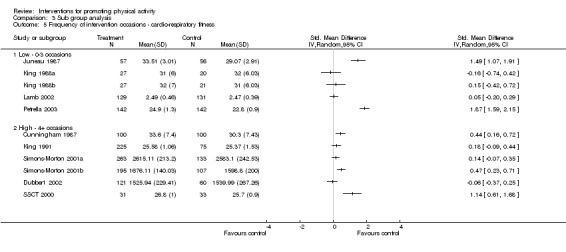
Comparison 3 Sub group analysis, Outcome 5 Frequency of intervention occasions ‐ cardio‐respiratory fitness.
3.6. Analysis.
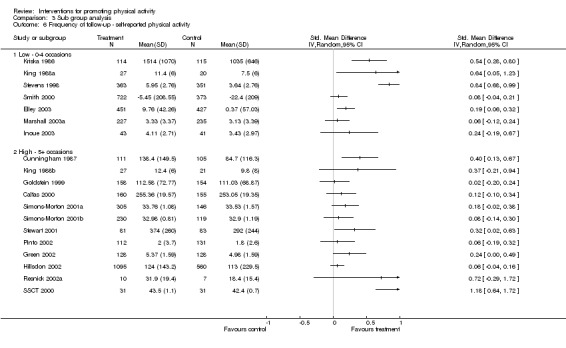
Comparison 3 Sub group analysis, Outcome 6 Frequency of follow‐up ‐ self‐reported physical activity.
3.7. Analysis.
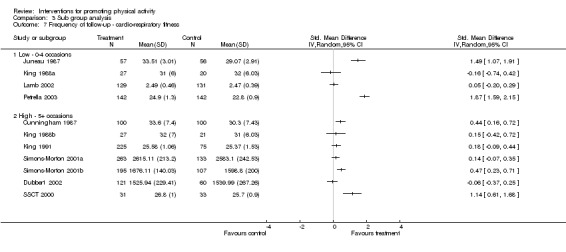
Comparison 3 Sub group analysis, Outcome 7 Frequency of follow‐up ‐ cardio‐respiratory fitness.
3.8. Analysis.
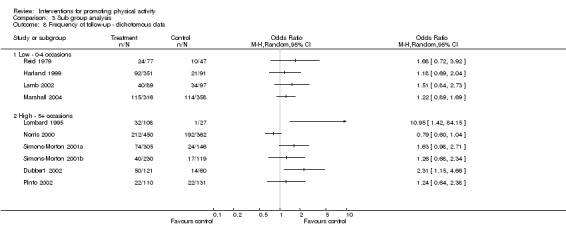
Comparison 3 Sub group analysis, Outcome 8 Frequency of follow‐up ‐ dichotomous data.
3.9. Analysis.
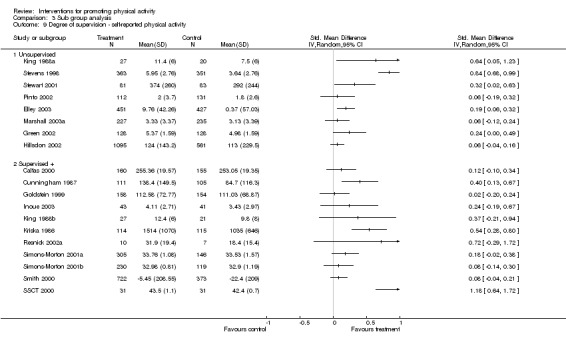
Comparison 3 Sub group analysis, Outcome 9 Degree of supervision ‐ self‐reported physical activity.
3.10. Analysis.
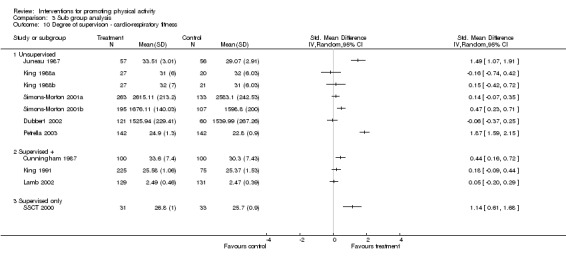
Comparison 3 Sub group analysis, Outcome 10 Degree of supervison ‐ cardio‐respiratory fitness.
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Calfas 2000.
| Methods | Randomised controlled trial | |
| Participants | University students | |
| Interventions | Intervention group received a 15 week cognitive behavioural education course, 15x50 minutes lectures followed by 15x110 minutes lab experience, led by peer health facilitators, plus homework including practice of behavioural management strategies. Participants received 2 course credits and could attend supervised x2 per week exercise sessions. All participants received 15 monthly follow up phone calls and monthly written materials. | |
| Outcomes | + Self reported physical activity | |
| Notes | No significant differences in physical activity between groups Participants volunteered to participate in a health course and attend a baseline assessment Participants in both study arms had very high baseline levels of physical activity ‐ mean 2+ hours of vigorous physical activity per week. Students also received academic credits for attending intervention sessions. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
Cunningham 1987.
| Methods | Randomised controlled trial | |
| Participants | Retirees from community centre | |
| Interventions | Participants received 3 group exercise sessions per week and were encouraged to do one additional home based session. | |
| Outcomes | + Self reported physical activity Cardio‐respiratory fitness | |
| Notes | Intervention group improved their fitness and vigorous physical activity levels versus control group. All exercise sessions were conducted on an indoor or outdoor running track | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
Dubbert 2002.
| Methods | Randomised controlled trial | |
| Participants | Primary care patients | |
| Interventions | All participants received a video, walking plan, weekly walking diary, (financial incentive for completing diary), plus (1) 20 counselling, goal setting phone calls from nurse, or (2) 10 nurse calls and 10 automated phone calls | |
| Outcomes | + Self reported physical activity 0 Cardio‐respiratory fitness | |
| Notes | No effect found for fitness changes but effect seen for dichotomous outcome | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
Elley 2003.
| Methods | Randomised controlled trial | |
| Participants | Primary care patients | |
| Interventions | Participants received motivation counselling from their general practitioner. This included discussion on increasing physical activity and goal setting. The participants received a green prescription card stating their recommended physical activity. After this meeting a local exercise specialist called all participants at least 3 times to encourage physical activity using motivational interviewing techniques. Written materials were also sent to participants every 3 months. These materials included information about local physical activity opportunities and motivational material. | |
| Outcomes | + Self reported physical activity | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
Goldstein 1999.
| Methods | Randomised controlled trial | |
| Participants | Primary care patients | |
| Interventions | Participants received 5 minutes of stage of change matched counselling, plus a written prescription, materials plus the chance of a follow up appointment. Participants also received 5 monthly mailed written materials. | |
| Outcomes | 0 Self reported physical activity | |
| Notes | No difference in stage of change or in physical activity in elderly score Active adults were excluded from the study | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
Green 2002.
| Methods | Randomised controlled trial | |
| Participants | Health maintenance organisation members | |
| Interventions | Participants received self help materials via mail, plus 3 x 20 minute phone calls per month for 3 months (up to 9 calls). | |
| Outcomes | 0 Self reported physical activity | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
Harland 1999.
| Methods | Randomised controlled trial | |
| Participants | Primary care patients | |
| Interventions | All participants completed a baseline assessment of self reported physical activity, physical measures and cycle ergometer fitness test. They received feedback of their results, brief advice about their present level of physical activity and comparison to recommended levels, plus written health information, 19 leaflets about local physical activity facilities and activities. In addition there were four intervention group, (i) one motivational interview, (ii) one motivational interview plus vouchers for free use of local facilities, (iii) 6 motivational interviews over 12 weeks and (iv) 6 motivational interviews over 12 weeks plus vouchers. | |
| Outcomes | 0 Self reported physical activity | |
| Notes | All intervention groups more active than control at 12 weeks, no differences at 12 months. Two approaches to recruitment used opportunistic and all potential participants who attended the health centre Self reported vigorously active excluded from study Moderate take up of motivational interviews amongst participants offered up to six ‐ median 3 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
Hillsdon 2002.
| Methods | Randomised controlled trial | |
| Participants | Primary care patients | |
| Interventions | Participants received brief negotiation plus follow up phone calls, or direct advice plus phone calls. | |
| Outcomes | 0 Self reported physical activity | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
Inoue 2003.
| Methods | Randomised controlled trial | |
| Participants | Older Japanese women | |
| Interventions | Participants received feedback on their baseline assessments of exercise behaviour and fitness in 30 minute group lectures. Three exercise goals were recommended to participants. Participants were allowed to use the local research centre exercise facilities during the study. Participants received an 8‐week intensive programme that provided each week one two hour session made up of one hour of group work and one hour of exercise practice. The group work included behavioural management skills based on stages of change. After 8 week all participants received newsletters every two months. | |
| Outcomes | 0 Self reported physical activity | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
Juneau 1987.
| Methods | Randomised controlled trial | |
| Participants | Workplace employees | |
| Interventions | Participants received a 30 minute consultation including watching a video, information on using a heart rate monitor and daily physical activity log. Participants were given a portable heart monitor, which warned the user if heart rate not in prescribed range. Participants were instructed to exercise at 65‐77% peak baseline treadmill heart rate. | |
| Outcomes | + Cardio‐respiratory fitness | |
| Notes | Increase in VO2 in intervention group improved over control group (approx 14% in males, 10% in female) Participants attended a screening session and a VO2 max test prior to randomisation | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
King 1988a.
| Methods | Randomised controlled trial | |
| Participants | Workplace employees | |
| Interventions | Maintenance study participants received 30 minutes of baseline instruction (15 mins advice + 15 mins video), daily self monitoring of physical activity using exercise logs returned to staff every month. | |
| Outcomes | + Self reported physical activity | |
| Notes | Significant difference in number of exercise sessions/month between groups Participants had previously taken part in an exercise RCT | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
King 1988b.
| Methods | Randomised controlled trial | |
| Participants | Workplace employees | |
| Interventions | Adoption study participants received 30 minutes of baseline instruction (15 mins advice + 15 mins video) plus 10 staff initiated phone calls and self‐monitoring materials including pulse monitor. | |
| Outcomes | 0 Self reported physical activity | |
| Notes | No significant difference in number of exercise sessions/month between groups but both groups increased physical activity over baseline. Participants had previously taken part in an exercise RCT | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
King 1991.
| Methods | Randomised controlled trial | |
| Participants | Community older volunteers | |
| Interventions | Participants received baseline physiological assessments and then were prescribed either home or group based training at high or low intensity plus written information, physical activity logs and phone calls. | |
| Outcomes | + Cardio‐respiratory fitness | |
| Notes | Increase in VO2 max (approx 5%) and treadmill duration (approx 14%). Adherence greater in home based arms Participants agreed to attend an extensive medical and physical assessment if they wished to participate in study | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
Kriska 1986.
| Methods | Randomised controlled trial | |
| Participants | Older women | |
| Interventions | Participants received a baseline physical assessment, 8 week walking training programme with organised walks, then choice of group or independent walking. Participants monitored their walking with monthly logs and also were offered social meetings. Participants also received follow up phone calls, cards, and incentives to maintain compliance. | |
| Outcomes | + Self reported physical activity | |
| Notes | Significant different between intervention and control groups on walking blocks per day. Frequency of follow up measures, meetings, mall walks and incentives not stated. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
Lamb 2002.
| Methods | Randomised controlled trial | |
| Participants | Primary care patients | |
| Interventions | Participants received a 30 minute group seminar, advice to exercise plus opportunity to attend health walks programme and verbal and written information about groups. This group also received three phone calls to encourage attendance and bring friends and family. | |
| Outcomes | 0 Self reported physical activity 0 Cardio‐respiratory fitness | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
Lombard 1995.
| Methods | Randomised controlled trial | |
| Participants | University staff & students | |
| Interventions | Participants were encouraged to walk in groups or with a friend and also received different frequencies and intensities of follow up telephone calls plus written materials including walking maps | |
| Outcomes | + Self reported physical activity | |
| Notes | Survival analysis showed that participants who received a high frequency of phone calls rather than a highly structured call were more successful in sustaining walking over control and other groups. Only 3 men in study (2.2%) | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
Marshall 2003a.
| Methods | Randomised controlled trial | |
| Participants | Adult participants of an evaluation cohort | |
| Interventions | Participants received one of 4 stages of change matched booklets, plus a motivational letter plus next stage of change booklet. | |
| Outcomes | 0 Self reported physical activity | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
Marshall 2004.
| Methods | Randomised controlled trial | |
| Participants | Community living adults | |
| Interventions | Participants received a booklet that matched their stage of change plus the booklet for the following stage (same materials as Marshall et al 2003). Participants also received a motivational letter. | |
| Outcomes | 0 Self reported physical activity | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
Norris 2000.
| Methods | Randomised controlled trial | |
| Participants | Health maintenance organisation members | |
| Interventions | Stage matched strategies and written materials given to patient prior to counselling with physician. Physician delivered behavioural counselling appropriate to stages of change model, with goal setting, identifying barriers, problem solving and contracting techniques, plus a written prescription for exercise. Patients also received single follow up phone call. | |
| Outcomes | 0 Self reported physical activity | |
| Notes | No significant differences between groups at 6 months High baseline physical activity levels ‐ 1500+ kcals/week | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
Petrella 2003.
| Methods | Randomised controlled trial | |
| Participants | Primary health care patients | |
| Interventions | Participants received a fitness assessment using a step test and counselling from physician. Each participant was given examples of exercise and the ACSM prescription of physical activity using heart rate reserve (HRR). Participants were asked to record their weekly exercise in a diary which was collected at 3, 6 and 12 months. Participants also received information about local exercise facilities and activities. | |
| Outcomes | + Cardio‐respiratory fitness | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | D ‐ Not used |
Pinto 2002.
| Methods | Randomised controlled trial | |
| Participants | Health maintenance organisation members | |
| Interventions | Participants received computer‐based telephone calls and wore a pedometer. Participants were asked to call every week for three months and at least twice a month for the next three months. The calls assessed present levels of moderate intensity physical activity, daily pedometer scores, motivation and provided stage matched advice. Monthly written reports were generated from calls and sent to participants. | |
| Outcomes | 0 Self reported physical activity | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
Reid 1979.
| Methods | Randomised controlled trial | |
| Participants | Male fire fighters | |
| Interventions | Pre randomisation fitness assessment, feedback by physician of fitness results compared population levels, prescription for exercise appropriate for age. Group one received additional one hour of health education, film, written & verbal advice. Group two received self‐monitoring materials and a weekly record, which were returned to research staff bi‐weekly. All participants reported monthly on exercise programme. | |
| Outcomes | 0 Compliance index score | |
| Notes | Short term significant improvement in compliance index (VO2+exercise freq.) not maintained at 6 months. Participants agreed to attended a screening session prior to randomisation Active fire fighters were excluded from study | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
Resnick 2002a.
| Methods | Randomised controlled trial | |
| Participants | Adults from retirement community | |
| Interventions | Participants received the WALC intervention. All participants were invited to join a walking group (meeting 6 times a week) or walk on their own 3 times a week. Pain was assessed by nurse once a week for four weeks then once a month for 5 months. Participants received written materials and these were used in a short review with their nurse. Participants received a calendar to remind them about walking goals and record walking frequency. | |
| Outcomes | 0 Self reported physical activity | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
Simons‐Morton 2001a.
| Methods | Randomised controlled trial | |
| Participants | Primary care patients | |
| Interventions | Participants were randomised to one of three groups, advice, assistance or counselling. The assistance group received the same advice as the advice for a physician but the health educator conducted a 30‐40 minute counselling session, including a videotape and action planning. Participants then received follow up phone calls, interactive mail, an electronic step counter, and monthly monitoring cards, which were returned to the health educator. Follow up mail was returned plus incentive to all participants. The counselling group received all of components of the advice and assistance group with in addition telephone‐counselling calls. Weekly behavioural classes were also offered to this group. | |
| Outcomes | 0 Self reported physical activity 0 Cardio‐respiratory fitness | |
| Notes | No differences in physical activity. No differences for either fitness or physical activity in any male group. Participants undertook three sessions of pre‐screening before randomisation. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
Simons‐Morton 2001b.
| Methods | Randomised controlled trial | |
| Participants | Primary care patients | |
| Interventions | Participants were randomised to one of three groups, advice, assistance or counselling. The assistance group received the same advice as the advice for a physician but the health educator conducted a 30‐40 minute counselling session, including a videotape and action planning. Participants then received follow up phone calls, interactive mail, an electronic step counter, and monthly monitoring cards, which were returned to the health educator. Follow up mail was returned plus incentive to all participants. The counselling group received all of components of the advice and assistance group with in addition telephone‐counselling calls. Weekly behavioural classes were also offered to this group. | |
| Outcomes | Self reported physical activity Cardio‐respiratory fitness |
|
| Notes | Women's VO2 increased in assistance group and counselling group compared to the advice group. No differences in physical activity. Participants undertook three sessions of pre‐screening before randomisation. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
Smith 2000.
| Methods | Randomised controlled trial | |
| Participants | Primary care patients | |
| Interventions | Participants received GP advice, or GP advice plus stage matched booklets via post | |
| Outcomes | 0 Self reported physical activity | |
| Notes | Short‐term (6‐10 weeks) increase in physical activity for advice plus booklet group versus controls only for participants inactive at baseline . Potential participants with poor English were excluded. Active subjects included in study but final results adjusted for baseline physical activity status | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | D ‐ Not used |
SSCT 2000.
| Methods | Randomised controlled trial | |
| Participants | Older Japanese adults | |
| Interventions | Participants were encouraged to attend at least 2 from 3 2‐hour exercise classes per week, held at a local community centre. The class contained endurance and resistance training. | |
| Outcomes | + Self reported physical activity (Fujita 2003) + Cardio‐respiratory fitness (Tsuji 2000) | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
Stevens 1998.
| Methods | Randomised controlled trial | |
| Participants | Primary care patients | |
| Interventions | Participants were invited by their GP to attend a consultation with an exercise development officer. At this meeting they discussed their present physical activity and were encouraged to increase on their current physical activity choices rather than start anything new. A follow up appointment was made ten weeks later. | |
| Outcomes | + Self reported physical activity | |
| Notes | Significant increase in occasions of exercise in past 4 weeks in intervention v control groups Active participants at baseline were not randomised MH & MT were study authors | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
Stewart 2001.
| Methods | Randomised controlled trial | |
| Participants | Community dwelling older adults | |
| Interventions | SCT based face to face counseling, behavioural, cognitive techniques to use local exercise opportunities or develop own programs. Participants also attended informational meetings, individual planning sessions, monthly group workshops, received physical activity diaries, telephone calls, newsletters, and functional fitness assessments. Participants were strongly encouraged to attend first two of ten workshops where a walking clinic was offered. | |
| Outcomes | + Self reported physical activity | |
| Notes | Greater increase in moderate physical activity in intervention group versus control at 12 months High baseline levels of physical activity ‐ 1052 kcals/week moderate LTPA, 1935 kcals/week for all physical activities | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Andersen 1999 | Study aim irrelevant |
| Andersen 2002 | Study aim irrelevant |
| Aoun 2002 | Study aim irrelevant |
| Asikainen 2002 | Review paper |
| Asikainen 2003 | Study aim irrelevant |
| Atienza 2001 | Review paper |
| Atlantis 2004 | Study aim irrelevant |
| Ballantyne 1978 | Study aim irrelevant |
| Baranowski 1990 | Less than 6 months follow up |
| Baranowski 2003 | Study aim irrelevant |
| Barnett 2003 | Study aim irrelevant |
| Bauman 2001 | Study aim irrelevant |
| Bell 2001 | Study aim irrelevant |
| Blair 1986 | Non‐randomised study |
| Blumenthal 2000 | Study aim irrelevant |
| Bonet 2003 | Study aim irrelevant |
| Brownson 2004 | Non‐randomised study |
| Buijis 2003 | Study aim irrelevant |
| Bull 1998 | Loss to follow up > 20% |
| Burke 2003 | Study aim irrelevant |
| Calfas 2002 | Study aim irrelevant |
| Campbell 1985 | Non‐randomised study |
| Cardinal 1996 | Less than 6 months follow up |
| Carels 2004 | Study aim irrelevant |
| Castro 2002 | Review paper |
| Chang 2003 | Non‐randomised study |
| Clark 2003 | Non‐randomised study |
| Coleman 1999 | No appropriate control group |
| Collins 2004 | Study aim irrelevant |
| Conn 2002 | Study aim irrelevant |
| Conn 2003 | Less than 6 months follow up |
| Dallow 2003 | No appropriate control group |
| De Jong 2004 | Study aim irrelevant |
| Donnelly 2000 | Study aim irrelevant |
| Dunn 1997 | No appropriate control group |
| Dunn 1998 | No appropriate control group |
| DuVall 2004 | Less than 6 months follow up |
| Eakin 2000 | Review paper |
| Eaton 1998 | Review paper |
| Ebrahim 1997 | Study aim irrelevant |
| Ebrahim 1998 | Review paper |
| Elberson 2001 | Study aim irrelevant |
| Elliot 2004 | Study aim irrelevant |
| Emmons 1999 | Multiple risk factor intervention |
| Eriksen 2002 | Study aim irrelevant |
| Fahrenwald 2002 | Study aim irrelevant |
| Fiatarone 1994 | Study aim irrelevant |
| Focht 2004 | Study aim irrelevant |
| Fody‐Urias 2001 | Study aim irrelevant |
| Fritz 2001 | Study aim irrelevant |
| Froehlich‐Grobe 2004 | Study aim irrelevant |
| Furukawa 2003 | Study aim irrelevant |
| Godin 1987 | Less than 6 months follow up |
| Goldwater 1985 | Less than 6 months follow up |
| Gossard 1986 | Less than 6 months follow up |
| Graham‐Clarke 1994 | Multiple risk factor intervention |
| Granner 2001 | Study aim irrelevant |
| Halbert 1999 | Study aim irrelevant |
| Halbert 2000 | Insufficient data, author uncontactable |
| Halbert 2001 | Study aim irrelevant |
| Hamdorf 1999 | Loss to follow up > 20% |
| Hamdorf 2002 | Study aim irrelevant |
| Harrell 1996 | No appropriate control group |
| Heinonen 1999 | Study aim irrelevant |
| Hellenius 1995 | Study aim irrelevant |
| Hellenius 1997 | Study aim irrelevant |
| Hirvensalo 2003 | Study aim irrelevant |
| Hopman‐Rock 2002 | Study aim irrelevant |
| Huang 2002 | Study aim irrelevant |
| Humpel 2004 | Less than 6 months follow up |
| Jakicic 1995 | No appropriate control group |
| Jakicic 1999 | No appropriate control group |
| Jette 1996 | Less than 6 months follow up |
| Jobe 2001 | Study aim irrelevant |
| Kaukiainen 2002 | Study aim irrelevant |
| Keele‐Smith 2003 | Less than 6 months follow up |
| Kelley 2004 | Study aim irrelevant |
| Kennedy 2003 | Study aim irrelevant |
| Kerr 2000 | No appropriate control group |
| Kim 2004 | Study aim irrelevant |
| King 1984 | Less than 6 months follow up |
| King 1995 | Study aim irrelevant |
| King 1997 | Study aim irrelevant |
| King 2000 | Study aim irrelevant |
| King 2001 | |
| Kinion 1993 | Study aim irrelevant |
| Kirk 2001 | Study aim irrelevant |
| Kirk 2004 | Study aim irrelevant |
| Kirk‐Gardner 2003 | Study aim irrelevant |
| Koffman 2001 | Non‐randomised study |
| Kohno 2002 | Non‐randomised study |
| Kontulainen 2004 | Study aim irrelevant |
| Kukkonen‐H 1998 | Study aim irrelevant |
| Lansdown 2002 | Less than 6 months follow up |
| Lawlor 2001 | Review paper |
| Leon 1996 | Study aim irrelevant |
| Lewis 1993a | Under 16s included |
| Lewis 1993b | Less than 6 months follow up |
| Li 2001 | Study aim irrelevant |
| Lindstrom 2003 | Study aim irrelevant |
| Little 2004 | Less than 6 months follow up |
| Lord 1995 | Non‐randomised study |
| Lupton 2002 | Study aim irrelevant |
| MacKeen 1985 | Loss to follow up > 20% |
| Manson 1999 | Study aim irrelevant |
| Marcus 1992 | Non‐randomised study |
| Marcus 1993 | Less than 6 months follow up |
| Marcus 1995 | Study aim irrelevant |
| Marcus 1998a | Less than 6 months follow up |
| Marcus 1998b | Loss to follow up > 20% |
| Marshall 2003b | Less than 6 months follow up |
| Martin 2004 | Study aim irrelevant |
| Mattila 2003 | Study aim irrelevant |
| McAuley 1994 | Less than 6 months follow up |
| McMahon 2002 | Study aim irrelevant |
| McMurdo 1992 | Study aim irrelevant |
| McMurdo 1995 | Study aim irrelevant |
| Messier 2000 | Study aim irrelevant |
| Miller 2002 | Loss to follow up > 20% |
| Mills 1996 | Study aim irrelevant |
| Milne 2002 | Less than 6 months follow up |
| Mulder 1981 | Study aim irrelevant |
| Munsch 2003 | Study aim irrelevant |
| Napolitano 2003 | Less than 6 months follow up |
| Naylor 1999 | Non‐randomised study |
| Newman 2002 | Review paper |
| Nisbeth 2000 | Study aim irrelevant |
| Noland 1989 | Less than 6 months follow up |
| Nurminen 2002 | Study aim irrelevant |
| Oexmann 2001 | Study aim irrelevant |
| Oida 2003 | Study aim irrelevant |
| Oman 2000 | Study aim irrelevant |
| Ortega‐Sanchez 2004 | Under 16s included |
| Ostwald 1989 | Study aim irrelevant |
| Parks 1997 | Non‐randomised study |
| Partonen 1998 | Study aim irrelevant |
| Paschal 2004 | Study aim irrelevant |
| Pereira 1998 | Study aim irrelevant |
| Peterson 1999 | Less than 6 months follow up |
| Peterson 2002 | Study aim irrelevant |
| Petrella 2000 | Study aim irrelevant |
| Petrella 2001 | Study aim irrelevant |
| Pfeiffer 2001 | Less than 6 months follow up |
| Philips 2004 | Study aim irrelevant |
| Pinto 2001 | Study aim irrelevant |
| Plotnikoff 2001 | Study aim irrelevant |
| Pohjonen 2001 | Non‐randomised study |
| Poole 2001 | Study aim irrelevant |
| Poston 2001 | Loss to follow up > 20% |
| Proper 2003a | Study aim irrelevant |
| Proper 2003b | Review paper |
| Purath 2004 | Less than 6 months follow up |
| Reijneveld 2003 | Study aim irrelevant |
| Renger 2002 | Non‐randomised study |
| Resnick 2002b | Study aim irrelevant |
| Reynolds 2001 | Review paper |
| Robison 1992 | Under 16s included |
| Ruby 1993 | Less than 6 months follow up |
| Samaras 1997 | Subjects with chronic disease |
| Schoenfelder 2000 | Study aim irrelevant |
| Schuler 2002 | Study aim irrelevant |
| Sciamanna 2002 | Study aim irrelevant |
| Sevick 2000 | No appropriate control group |
| Simmons 2003 | Study aim irrelevant |
| Sims 2004 | Study aim irrelevant |
| Singh 1997 | Study aim irrelevant |
| Singh 1997a | Less than 6 months follow up |
| Smith 2003 | Non‐randomised study |
| Smolander 2000 | No appropriate control group |
| Sorensen 1999 | Study aim irrelevant |
| Steptoe 1999 | Multiple risk factor intervention |
| Steptoe 2000 | Study aim irrelevant |
| Steptoe 2001 | Study aim irrelevant |
| Stevens 1999 | Non‐randomised study |
| Stevens 2003 | Non‐randomised study |
| Stiggelbout 2004 | Less than 6 months follow up |
| Swinburn 2003 | Review paper |
| Taylor 1998 | Loss to follow up > 20% |
| Twisk 2004 | Study aim irrelevant |
| van der Bij 2002 | Review paper |
| Veverka 2003 | Study aim irrelevant |
| Votruba 1968 | Review paper |
| Vuori 1994 | Less than 6 months follow up |
| Wankel 1985 | Less than 6 months follow up |
| Weinehall 2001 | Study aim irrelevant |
| Wen 2002 | Non‐randomised study |
| Wilbur 2001 | Study aim irrelevant |
| Wood 1983 | Study aim irrelevant |
| Woods 2002 | Study aim irrelevant |
| Yalden 2001 | Study aim irrelevant |
| Yanek 2001 | Study aim irrelevant |
| Young 1999 | Study aim irrelevant |
| Zask 2001 | Study aim irrelevant |
Contributions of authors
Dr Foster was involved in: Conceiving the review Designing the review Coordinating the review Screening search results Screening retrieved papers against inclusion criteria Appraising quality of papers Abstracting data from papers Data management for the review Entering data into RevMan Analysis of data Interpretation of data Providing a methodological perspective Providing a clinical perspective Providing a policy perspective Writing the review Providing general advice on the review Securing funding for the review Performing previous work that was the foundation of current study.
Dr Hillsdon was involved in: Conceiving the review Designing the review Coordinating the review Data collection for the review Developing search strategy Undertaking searches Screening search results Organising retrieval of papers Screening retrieved papers against inclusion criteria Appraising quality of papers Abstracting data from papers Writing to authors of papers for additional information Providing additional data about papers Obtaining and screening data on unpublished studies Data management for the review Entering data into RevMan Analysis of data Interpretation of data Providing a methodological perspective Providing a clinical perspective Providing a policy perspective Writing the review Providing general advice on the review Securing funding for the review Performing previous work that was the foundation of current study
Professor Thorogood was involved with: Conceiving the review Designing the review Coordinating the review Screening search results Screening retrieved papers against inclusion criteria Appraising quality of papers Abstracting data from papers Data management for the review Entering data into RevMan Analysis of data Interpretation of data Providing a methodological perspective Providing a clinical perspective Providing a policy perspective Writing the review Providing general advice on the review Securing funding for the review Performing previous work that was the foundation of current study
Sources of support
Internal sources
No sources of support supplied
External sources
CF funded by British Heart Foundation Core Grant ‐ 2006‐2011, UK.
First Cochrane Review was funded by British Heart Foundation Project Grant ‐ PG/2001089, UK.
Declarations of interest
The authors of this review are also authors of one of the included studies (Hillsdon 2002).
Stable (no update expected for reasons given in 'What's new')
References
References to studies included in this review
Calfas 2000 {published data only}
- Calfas KJ, Sallis JF, Nichols JF, Sarkin JA, Johnson MF, Caparosa S, et al. Project GRAD: two‐year outcomes of a randomized controlled physical activity intervention among young adults. Graduate Ready for Activity Daily. American Journal of Preventive Medicine 2000;18(1):28‐37. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Cunningham 1987 {published data only}
- Cunningham DA, Rechnitzer PA, Howard JH, Donner AP. Exercise training of men at retirement: a clinical trial. Journal of Gerontology 1987;42(1):17‐23. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Dubbert 2002 {published and unpublished data}
- Dubbert PM, Cooper KM, Kirchner KA, Meydrech EF, Bilbrew D. Effects of nurse counseling on walking for exercise in elderly primary care patients. Journals of Gerontology Series A‐Biological Sciences & Medical Sciences 2002;57(11):M733‐40. [DOI] [PubMed] [Google Scholar]
Elley 2003 {published data only}
- Elley CR, Kerse N, Arroll B, Robinson E. Effectiveness of counselling patients on physical activity in general practice: cluster randomised controlled trial. BMJ 2003;326(7393):793‐800. [DOI] [PMC free article] [PubMed] [Google Scholar]
Goldstein 1999 {published data only}
- Goldstein MG, Pinto BM, Marcus BH. Physician based physical activity counselling for middle aged and older adults: a randomised trial. Annals of Behavioral Medicine 1999;21:40‐7. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Green 2002 {published data only}
- Green B, McAffee T, Hindmarsh M, Madsen L, Caplow M, Buist D. Effectiveness of telephone support in increasing physical activity levels in primary care patients. American Journal of Preventive Medicine 2002;22(3):177‐83. [DOI] [PubMed] [Google Scholar]
Harland 1999 {published data only}
- Harland J, White M, Drinkwater C, Chinn D, Farr L, Howel D. The Newcastle exercise project: a randomised controlled trial of methods to promote physical activity in primary care. BMJ 1999;319(7213):828‐32. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Hillsdon 2002 {published data only}
- Hillsdon M, Thorogood M, White IR, Foster C. Advising people to take more exercise is ineffective: a randomised controlled trial of physical activity promotion in primary care. International Journal of Epidemiology 2002;31(4):808‐15. [DOI] [PubMed] [Google Scholar]
Inoue 2003 {published data only}
- Inoue S, Odagiri Y, Wakui S, Katoh R, Moriguchi T, Ohya Y, et al. Randomized controlled trial to evaluate the effect of a physical activity intervention program based on behavioural medicine. Journal of Tokyo Medical University 2003;61:154‐65. [Google Scholar]
Juneau 1987 {published data only}
- Juneau M, Rogers F, Santos V, Yee M, Evans A, Bohn A, et al. Effectiveness of self‐monitored, home‐based, moderate‐intensity exercise training in middle‐aged men and women. American Journal of Cardiology 1987;60(1):66‐70. [DOI] [PubMed] [Google Scholar]
King 1988a {published data only}
- King AC, Taylor CB, Haskell WL, DeBusk RF. Strategies for increasing early adherence to and long‐term maintenance of home‐based exercise training in healthy middle‐aged men and women. American Journal of Cardiology 1988;61(8):628‐32. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
King 1988b {published data only}
- King AC, Taylor CB, Haskell WL, DeBusk RF. Strategies for increasing early adherence to and long‐term maintenance of home‐based exercise training in healthy middle‐aged men and women. American Journal of Cardiology 1988;61(8):628‐32. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
King 1991 {published data only}
- King AC, Haskell WL, Taylor CB, Kraemer HC, DeBusk RF. Group‐ vs home‐based exercise training in healthy older men and women. A community‐based clinical trial. JAMA 1991;266(11):1535‐42. [MEDLINE: ] [PubMed] [Google Scholar]
Kriska 1986 {published data only}
- Kriska AM, Bayles C, Cauley JA, LaPorte RE, Sandler RB, Pambianco G. A randomized exercise trial in older women: increased activity over two years and the factors associated with compliance. Medicine & Science in Sports & Exercise 1986;18(5):557‐62. [MEDLINE: ] [PubMed] [Google Scholar]
Lamb 2002 {published data only}
- Lamb SE, Bartlett HP, Ashley A, Bird W. Can lay‐led walking programmes increase physical activity in middle aged adults? A randomised controlled trial. Journal of Epidemiology & Community Health 2002;56:246‐52. [DOI] [PMC free article] [PubMed] [Google Scholar]
Lombard 1995 {published data only}
- Lombard DN, Lombard TN, Winett RA. Walking to meet health guidelines: the effect of prompting frequency and prompt structure. Health Psychology 1995;14(2):164‐70. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Marshall 2003a {published and unpublished data}
- Marshall AL, Bauman AE, Owen N, Booth ML, Crawford D, Marcus BH. Population‐based randomized controlled trial of a stage‐targeted physical activity intervention. Annals of Behavioral Medicine 2003;25(3):194‐202. [DOI] [PubMed] [Google Scholar]
Marshall 2004 {published data only}
- Marshall AL, Bauman AE, Owen N, Booth ML, Crawford D, Marcus BH. Reaching out to promote physical activity in Australia: a statewide randomized controlled trial of a stage‐targeted intervention. American Journal of Health Promotion 2004;18:283‐7. [DOI] [PubMed] [Google Scholar]
Norris 2000 {published data only}
- Norris SL, Grothaus LC, Buchner DM, Pratt M. Effectiveness of physician‐based assessment and counseling for exercise in a staff model HMO. Preventive Medicine 2000;30(6):513‐23. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Petrella 2003 {published data only}
- Petrella RJ, Koval JJ, Cunningham DA, Paterson DH. Can primary care doctors prescribe exercise to improve fitness? The step test exercise prescription (STEP) project. American Journal of Preventive Medicine 2003;24(4):316‐22. [DOI] [PubMed] [Google Scholar]
Pinto 2002 {published data only}
- Pinto BM, Friedman R, Marcus BH, Kelley H, Tennstedt S, Gillman MW. Effects of a computer‐based, telephone counseling system on physical activity. American Journal of Preventive Medicine 2002;23(2):113‐20. [DOI] [PubMed] [Google Scholar]
Reid 1979 {published data only}
- Reid EL, Morgan RW. Exercise prescription: a clinical trial. American Journal of Public Health 1979;69(6):591‐5. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Resnick 2002a {published data only}
- Resnick B. Testing the effect of the WALC intervention on exercise adherence in older adults. Journal of Gerontological Nursing 2002;28(6):40‐9. [DOI] [PubMed] [Google Scholar]
Simons‐Morton 2001a {published data only}
- Simons‐Morton DG, Blair SN, King AC, Morgan TM, Applegate WB, O' Toole M, et al. Effects of physical activity counseling in primary care: The Activity Counseling Trial: A randomized controlled trial. JAMA 2001;286(6):677‐87. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Simons‐Morton 2001b {published data only}
- Simons‐Morton DG, Blair SN, King AC, Morgan TM, Applegate WB, O' Toole M, et al. Effects of physical activity counseling in primary care: The Activity Counseling Trial: A randomized controlled trial. JAMA 2001;286(6):677‐87. [DOI] [PubMed] [Google Scholar]
Smith 2000 {published data only}
- Smith BJ, Bauman AE, Bull FC, Booth ML, Harris MF. Promoting physical activity in general practice: a controlled trial of written advice and information materials. British Journal of Sports Medicine 2000;34(4):262‐7. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
SSCT 2000 {published data only}
- Fujita K, Nagatomi R, Hozawa A, Ohkubo T, Sato K, Anzai Y, et al. Effects of exercise training on physical activity in older people: a randomized controlled trial. Journal of Epidemiology 2003;13(2):120‐6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tsuji I, Tamagawa A, Nagatomi R, Irie N, Ohkubo T, Saito M, et al. Randomized controlled trial of exercise training for older people (Sendai Silver Center Trial; SSCT): study design and primary outcome. Journal of Epidemiology 2000;10(1):55‐64. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Stevens 1998 {published data only}
- Stevens W, Hillsdon M, Thorogood M, McArdle D. Cost‐effectiveness of a primary care based physical activity intervention in 45‐74 year old men and women: a randomised controlled trial. British Journal of Sports Medicine 1998;32(3):236‐41. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Stewart 2001 {published data only}
- Stewart AL, Verboncoeur CJ, McLellan BY, Gillis DE, Rush S, Mills KM, et al. Physical activity outcomes of CHAMPS II: a physical activity promotion program for older adults. Journals of Gerontology Series A‐Biological Sciences & Medical Sciences 2001;56(8):M465‐70. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
References to studies excluded from this review
Andersen 1999 {published data only}
- Andersen RE, Wadden TA, Bartlett SJ, Zemel B, Verde TJ, Franckowiak SC. Effects of lifestyle activity vs structured aerobic exercise in obese women. JAMA 1999;281(4):335‐40. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Andersen 2002 {published data only}
- Andersen LB, Klausen K, Nisbeth O. One‐year effect of health counseling on life style and risk factors of heart disease [Et ars effekt af sundhedsvejledning pa livsstil og risikofaktorer for hjertesygdom]. Ugeskrift for Laeger 2002;164(13):1814‐8. [PubMed] [Google Scholar]
Aoun 2002 {published data only}
- Aoun S, Johnson L. Men's health promotion by general practitioners in a workplace setting. Australian Journal of Rural Health 2002;10(6):268‐72. [DOI] [PubMed] [Google Scholar]
Asikainen 2002 {published data only}
- Asikainen TM, Miilunpalo S, Oja P, Rinne M, Pasanen M, Uusi‐Rasi R, et al. Randomised, controlled walking trials in postmenopausal women: the minimum dose to improve aerobic fitness?. British Journal of Sports Medicine 2002;36(3):189‐94. [DOI] [PMC free article] [PubMed] [Google Scholar]
Asikainen 2003 {published data only}
- Asikainen TM, Miilunpalo S, Kukkonen‐Harjula K, Nenonen A, Pasanen M, Rinne M, et al. Walking trials in postmenopausal women: effect of low doses of exercise and exercise fractionization on coronary risk factors. Scandinavian Journal of Medicine & Science in Sports 2003;13(5):284‐92. [DOI] [PubMed] [Google Scholar]
Atienza 2001 {published data only}
- Atienza AA. Home‐based physical activity programs for middle‐aged and older adults: Summary of empirical research. Journal of Aging and Physical Activity 2001;9(Suppl):S38‐58. [Google Scholar]
Atlantis 2004 {published data only}
- Atlantis E, Chow CM, Kirby A, Singh MF. An effective exercise‐based intervention for improving mental health and quality of life measures: a randomized controlled trial. Preventive Medicine 2004;39(2):424‐34. [DOI] [PubMed] [Google Scholar]
Ballantyne 1978 {published data only}
- Ballantyne D, Clark A, Dyker GS, Gillis CR, Hawthorne VM, Henry DA, et al. Prescribing exercise for the healthy assessment of compliance and effects on plasma lipids and lipoproteins. Health Bulletin 1978;36(4):169‐76. [MEDLINE: ] [PubMed] [Google Scholar]
Baranowski 1990 {published data only}
- Baranowski T, Simons‐Morton B, Hooks P, Henske J, Tiernan K, Dunn JK, et al. A center‐based program for exercise change among black‐American families. Health Educucation Quarterly 1990;17(2):179‐96. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Baranowski 2003 {published data only}
- Baranowski T, Baranowski JC, Cullen KW, Thompson DI, Nicklas T, Zakeri IE, et al. The Fun, Food, and Fitness Project (FFFP): the Baylor GEMS pilot study. Ethnicity & Disease 2003;13(1 Suppl 1):S30‐9. [PubMed] [Google Scholar]
Barnett 2003 {published data only}
- Barnett A, Smith B, Lord SR, Williams M, Baumand A. Community‐based group exercise improves balance and reduces falls in at‐risk older people: a randomised controlled trial. Age and Ageing 2003;32(4):407‐14. [DOI] [PubMed] [Google Scholar]
Bauman 2001 {published data only}
- Bauman AE, Bellew B, Owen N, Vita P. Impact of an Australian mass media campaign targeting physical activity in 1998. American Journal of Preventive Medicine 2001;21(1):41‐7. [DOI] [PubMed] [Google Scholar]
Bell 2001 {published data only}
- Bell AC, Swinburn BA, Amosa H, Scragg RK. A nutrition and exercise intervention program for controlling weight in Samoan communities in New Zealand. International Journal of Obesity 2001;25(6):920‐27. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Blair 1986 {published data only}
- Blair SN, Piserchia PV, Wilbur CS, Crowder JH. A public health intervention model for work‐site health promotion. Impact on exercise and physical fitness in a health promotion plan after 24 months. JAMA 1986;255(7):921‐26. [MEDLINE: ] [PubMed] [Google Scholar]
Blumenthal 2000 {published data only}
- Blumenthal JA, Sherwood A, Gullette ECD, Babyak M, Waugh R, Georgiades A, et al. Exercise and weight loss reduce blood pressure in men and women with mild hypertension: Effects on cardiovascular, metabolic, and hemodynamic functioning. Archives of Internal Medicine 2000;160(13):1947‐58. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Bonet 2003 {published data only}
- Bonet J, Coll R, Rocha E, Romero R. Supervised versus recommended physical exercise in hypertensive women. Is its recommendation enough?. Blood Pressure 2003;12(3):139‐44. [DOI] [PubMed] [Google Scholar]
Brownson 2004 {published data only}
- Brownson RC, Baker EA, Boyd RL, Caito NM, Duggan K, Housemann RA, et al. A community‐based approach to promoting walking in rural areas. American Journal of Preventive Medicine 2004;27(1):1‐34. [DOI] [PubMed] [Google Scholar]
Buijis 2003 {published data only}
- Buijs R, Ross‐Kerr J, Cousins SO, Wilson D. Promoting participation: evaluation of a health promotion program for low income seniors. Journal of Community Health Nursing 2003;20(2):93‐107. [DOI] [PubMed] [Google Scholar]
Bull 1998 {published data only}
- Bull FC, Jamrozik K. Advice on exercise from a family physician can help sedentary patients to become active. American Journal of Preventive Medicine 1998;15(2):85‐94. [DOI] [PubMed] [Google Scholar]
Burke 2003 {published data only}
- Burke V, Giangiulio N, Gillam HF, Beilin LJ, Houghton S. Physical activity and nutrition programs for couples: a randomized controlled trial. Journal of Clinical Epidemiology 2003;56(5):421‐32. [DOI] [PubMed] [Google Scholar]
Calfas 2002 {published data only}
- Calfas KJ, Sallis JF, Zabinski MF, Wilfley DE, Rupp J, Prochaska J‐J, et al. Preliminary evaluation of a multicomponent program for nutrition and physical activity change in primary care: PACE+ for adults. Preventive Medicine 2002;34(2):153‐61. [DOI] [PubMed] [Google Scholar]
Campbell 1985 {published data only}
- Campbell MJ, Browne D, Waters WE. Can general practitioners influence exercise habits? Controlled trial. British Medical Journal Clinical Research Ed 1985;290(6474):1044‐6. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Cardinal 1996 {published data only}
- Cardinal BJ, Sachs ML. Effects of mail‐mediated, stage‐matched exercise behavior change strategies on female adults' leisure‐time exercise behavior. Journal of Sports Medicine & Physical Fitness 1996;36(2):100‐7. [MEDLINE: ] [PubMed] [Google Scholar]
Carels 2004 {published data only}
- Carels RA, Darby LA, Cacciapaglia HM, Douglass OM. Reducing cardiovascular risk factors in postmenopausal women through a lifestyle change intervention. Journal of Women's Health 2004;13(4):412‐26. [DOI] [PubMed] [Google Scholar]
Castro 2002 {published data only}
- Castro C, King A. Telephone‐assisted counseling for physical activity. Exercise & Sport Sciences Reviews 2002;30(2):64‐8. [DOI] [PubMed] [Google Scholar]
Chang 2003 {published data only}
- Chang SF. Worksite health promotion ‐ on the effects of an employee fitness program.. Journal of Nursing Research 2003;11(3):412‐26. [DOI] [PubMed] [Google Scholar]
Clark 2003 {published data only}
- Clark DO, Stump TE, Damush TM. Outcomes of an exercise program for older women recruited through primary care. Journal of Aging and Health 2003;15(3):567‐85. [DOI] [PubMed] [Google Scholar]
Coleman 1999 {published data only}
- Coleman KJ, Raynor HR, Mueller DM, Cerny FJ, Dorn JM, et al. Providing sedentary adults with choices for meeting their walking goals. Preventive Medicine 1999;28(5):510‐9. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Collins 2004 {published data only}
- Collins R, Lee RE, Albright CL, King AC. The effects of a course preparing low‐income multiethnic women to be more physically active. Health Education & Behavior 2004;31(1):47‐64. [DOI] [PubMed] [Google Scholar]
Conn 2002 {published data only}
- Conn VS, Valentine JC, Cooper HM. Interventions to increase physical activity among aging adults: A meta‐analysis. Annals of Behavioral Medicine 2002;24(3):190‐200. [DOI] [PubMed] [Google Scholar]
Conn 2003 {published data only}
- Conn VS, Burks KJ, Minor MA, Mehr DR. Randomized trial of 2 interventions to increase older women's exercise. American Journal of Health Behavior 2003;27(4):380‐8. [DOI] [PubMed] [Google Scholar]
Dallow 2003 {published data only}
- Dallow CB, Anderson J. Using self‐efficacy and a transtheoretical model to develop a physical activity intervention for obese women. American Journal of Health Promotion 2003;17(6):373‐81. [DOI] [PubMed] [Google Scholar]
De Jong 2004 {published data only}
- Jong ORW, Hopman RM, Tak ECMP, Klazinga NS. An implementation study of two evidence‐based exercise and health education programmes for older adults with osteoarthritis of the knee and hip. Health Education Research 2004;19(3):316‐25. [DOI] [PubMed] [Google Scholar]
Donnelly 2000 {published data only}
- Donnelly JE, Jacobsen DJ, Heelan KS, Seip R, Smith S. The effects of 18 months of intermittent vs continuous exercise on aerobic capacity, body weight and composition, and metabolic fitness in previously sedentary, moderately obese females. International Journal of Obesity & Related Metabolic Disorders 2000;24(5):566‐72. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Dunn 1997 {published data only}
- Dunn AL, Marcus BH, Kampert JB, Garcia ME, Kohl HW, Blair SN. Reduction in cardiovascular disease risk factors: 6‐month results from Project Active. Preventive Medicine 1997;26(6):883‐92. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Dunn 1998 {published data only}
- Dunn AL, Garcia ME, Marcus BH, Kampert JB, Kohl‐HW III, Blair SN. Six‐month physical activity and fitness changes in Project Active, a randomized trial. Medicine & Science in Sports & Exercise 1998;30(7):1076‐83. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
DuVall 2004 {published data only}
- DuVall C, Dinger MK, Taylor EL, Bemben D. Minimal‐contact physical activity interventions in women: a pilot study. American Journal of Health Behavior 2004;28(3):280‐6. [DOI] [PubMed] [Google Scholar]
Eakin 2000 {published data only}
- Eakin EG, Glasgow RE, Riley KM. Review of primary care‐based physical activity intervention studies: effectiveness and implications for practice and future research. Journal of Family Practice 2000;49(2):158‐68. [MEDLINE: ] [PubMed] [Google Scholar]
Eaton 1998 {published data only}
- Eaton CB, Menard LM. A systematic review of physical activity promotion in primary care office settings. Britich Journal of Sports Medicine 1998;32(1):11‐16. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Ebrahim 1997 {published data only}
- Ebrahim S, Thompson PW, Baskaran V, Evans K. Randomized placebo‐controlled trial of brisk walking in the prevention of postmenopausal osteoporosis. Age & Ageing 1997;26(4):253‐60. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Ebrahim 1998 {published data only}
- Ebrahim S, Smith GD. Lowering blood pressure: a systematic review of sustained effects of non‐pharmacological interventions. Journal of Public Health Medicine 1998;20(4):441‐8. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Elberson 2001 {published data only}
- Elberson KL, Daniels KK, Miller PM. Structured and nonstructured exercise in a corporate wellness program. A comparison of physiological outcomes. Outcomes Management for Nursing Practice 2001;5(2):82‐6. [PubMed] [Google Scholar]
Elliot 2004 {published data only}
- Elliot DL, Goldberg L, Duncan TE, Kuehl KS, Moe EL, Breger RK, et al. The PHLAME firefighters' study: feasibility and findings. American Journal of Health Behavior 2004;28(1):13‐23. [DOI] [PubMed] [Google Scholar]
Emmons 1999 {published data only}
- Emmons KM, Linnan LA, Shadel WG, Marcus B, Abrams DB. The Working Healthy Project: a worksite health‐promotion trial targeting physical activity, diet, and smoking. Journal of Occupational and Environmental Medicine 1999;41(7):545‐55. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Eriksen 2002 {published data only}
- Eriksen HR, Ihlebaek C, Mikkelsen A, Gronningsaeter H, Sandal GM, Ursin H. Improving subjective health at the worksite: a randomized controlled trial of stress management training, physical exercise and an integrated health programme. Occupational Medicine 2002;52(7):383‐91. [DOI] [PubMed] [Google Scholar]
Fahrenwald 2002 {published data only}
- Fahrenwald NL, Sharma M. Development and expert evaluation of "Moms on the Move," a physical activity intervention for WIC mothers. Public Health Nursing 2002;19(6):423‐39. [DOI] [PubMed] [Google Scholar]
Fiatarone 1994 {published data only}
- Fiatarone MA, O'Neill EF, Ryan ND, Clements KM, Solares GR, Nelson ME, et al. Exercise training and nutritional supplementation for physical frailty in very elderly people. New England Journal of Medicine 1994;330(25):1769‐75. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Focht 2004 {published data only}
- Focht BC, Brawley LR, Rejeski WJ, Ambrosius WT. Group‐mediated activity counseling and traditional exercise therapy programs: Effects on health‐related quality of life among older adults in cardiac rehabilitation. Annals of Behavioral Medicine 2004;28(1):52‐61. [DOI] [PubMed] [Google Scholar]
Fody‐Urias 2001 {published data only}
- Fody‐Urias BM, Fillit H, Hill J. The effect of a fitness program on health status and health care consumption in Medicare MCOs. Managed Care Interface 2001;14(9):58‐64. [MEDLINE: ] [PubMed] [Google Scholar]
Fritz 2001 {published data only}
- Fritz T, Rosenqvist U. Walking for exercise ‐ immediate effect on blood glucose levels in type 2 diabetes. Scandian Journal of Primary Health Care 2001;19(1):31‐3. [PubMed] [Google Scholar]
Froehlich‐Grobe 2004 {published data only}
- Froehlich‐Grobe K, White GW. Promoting physical activity among women with mobility impairments: A Randomized controlled trial to assess a home‐ and community‐based intervention. Archives of Physical Medicine & Rehabilitation 2004;85(4):640‐8. [DOI] [PubMed] [Google Scholar]
Furukawa 2003 {published data only}
- Furukawa F, Kazuma K, Kawa M, Miyashita M, Niiro K, Kusukawa R, et al. Effects of an off‐site walking program on energy expenditure, serum lipids, and glucose metabolism in middle‐aged women. Biological Research for Nursing 2003;4(3):181‐92. [DOI] [PubMed] [Google Scholar]
Godin 1987 {published data only}
- Godin G, Desharnais R, Jobin J, Cook J. The impact of physical fitness and health‐age appraisal upon exercise intentions and behavior. Journal of Behavioral Medicine 1987;10(3):241‐50. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Goldwater 1985 {published data only}
- Goldwater BC, Collis ML. Psychologic effects of cardiovascular conditioning: a controlled experiment. Psychosomatic Medicine 1985;47(2):174‐81. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Gossard 1986 {published data only}
- Gossard D, Haskell WL, Taylor CB, Mueller JK, Rogers F, Chandler M, et al. Effects of low‐ and high‐intensity home‐based exercise training on functional capacity in healthy middle‐aged men. American Journal of Cardiology 1986;57(6):446‐9. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Graham‐Clarke 1994 {published data only}
- Graham‐Clarke P, Oldenburg B. The effectiveness of a general‐practice‐based physical activity intervention on patient physical activity status. Behaviour Change 1994;11(3):132‐44. [MEDLINE: ] [Google Scholar]
Granner 2001 {published data only}
- Granner ML, Liguori G, Kirkner GJ, Ainsworth BE. Health care provider counseling for physical activity among black and white South Carolinians. Journal of the South Carolina Medical Association 2001;97(8):338‐41. [PubMed] [Google Scholar]
Halbert 1999 {published data only}
- Halbert JA, Silagy CA, Finucane P, Withers RT, Hamdorf PA. Recruitment of older adults for a randomized, controlled trial of exercise advice in a general practice setting. Journal of the American Geriatrics Society 1999;47(4):477‐81. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Halbert 2000 {published data only}
- Halbert JA, Silagy CA, Finucane PM, Withers RT, Hamdorf PA. Physical activity and cardiovascular risk factors: effect of advice from an exercise specialist in Australian general practice. Medical Journal of Australia 2000;173(2):84‐7. [DOI] [PubMed] [Google Scholar]
Halbert 2001 {published data only}
- Halbert J, Crotty M, Weller D, Ahern M, Silagy C. Primary care‐based physical activity programs: Effectiveness in sedentary older patients with osteoarthritis symptoms. Arthritis & Rheumism 2001;45(3):228‐34. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Hamdorf 1999 {published data only}
- Hamdorf PA, Penhall RK. Walking with its training effects on the fitness and activity patterns of 79‐91 year old females. Australian & New Zealand Journal of Medicine 1999;29(1):22‐8. [DOI] [PubMed] [Google Scholar]
Hamdorf 2002 {published data only}
- Hamdorf P, Starr G, Williams M. California Active Aging Project. Journal of Aging and Physical Activity 2002;10(3):354‐9. [Google Scholar]
Harrell 1996 {published data only}
- Harrell JS, Johnston LF, Griggs TR, Schaefer P, Carr‐EG J, McMurray RG, et al. An occupation based physical activity intervention program: improving fitness and decreasing obesity. AAOHN J 1996;44(8):377‐84. [MEDLINE: ] [PubMed] [Google Scholar]
Heinonen 1999 {published data only}
- Heinonen A, Kannus P, Sievanen H, Pasanen M, Oja P, Vuori I. Good maintenance of high‐impact activity‐induced bone gain by voluntary, unsupervised exercises: An 8‐month follow‐up of a randomized controlled trial. Journal of Bone & Mineral Research 1999;14(1):125‐8. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Hellenius 1995 {published data only}
- Hellenius ML, Brismar KE, Berglund BH, Faire UH. Effects on glucose tolerance, insulin secretion, insulin‐like growth factor 1 and its binding protein, IGFBP‐1, in a randomized controlled diet and exercise study in healthy, middle‐aged men. Journal of Internal Medicine 1995;238(2):121‐30. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Hellenius 1997 {published data only}
- Hellenius ML, Krakau I, Faire UD. Favourable long‐term effects from advice on diet and exercise given to healthy men with raised cardiovascular risk factors. Nutrition Metabolism & Cardiovascular Diseases 1997;7:294‐300. [MEDLINE: ] [Google Scholar]
Hirvensalo 2003 {published data only}
- Hirvensalo M, Heikkinen E, Lintunen T, Rantanen T. The effect of advice by health care professionals on increasing physical activity of older people. Scandinavian Journal of Medicine Science & Sports 2003;13(4):231‐6. [DOI] [PubMed] [Google Scholar]
Hopman‐Rock 2002 {published data only}
- Hopman‐Rock M, Westhoff MH. Health education and exercise stimulation for older people: development and evaluation of the program "Healthy and Vital" [Gezondheidsvoorlichting en bewegingsstimulering voor ouderen: ontwikkeling en evaluatie van het programma "Gezond & Vitaal"]. Tijdschrift voor Gerontologie en Geriatrie 2002;33(2):56‐63. [PubMed] [Google Scholar]
Huang 2002 {published data only}
- Huang LH, Chen SW, Yu YP, Chen PR, Lin YC. The effectiveness of health promotion education programs for community elderly. Journal of Nursing Research 2002;10(4):261‐70. [DOI] [PubMed] [Google Scholar]
Humpel 2004 {published data only}
- Humpel N, Marshall AL, Iverson D, Leslie E, Owen N. Trial of print and telephone delivered interventions to influence walking. Preventive Medicine 2004;39(3):635‐41. [DOI] [PubMed] [Google Scholar]
Jakicic 1995 {published data only}
- Jakicic JM, Wing RR, Butler BA, Robertson RJ. Prescribing exercise in multiple short bouts versus one continuous bout: effects on adherence, cardiorespiratory fitness, and weight loss in overweight women. International Journal of Obesity & Related Metabolic Disorders 1995;19(12):893‐901. [MEDLINE: ] [PubMed] [Google Scholar]
Jakicic 1999 {published data only}
- Jakicic JM, Winters C, Lang W, Wing RR. Effects of intermittent exercise and use of home exercise equipment on adherence, weight loss, and fitness in overweight women: a randomized trial. JAMA 1999;282(16):1554‐60. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Jette 1996 {published data only}
- Jette AM, Harris BA, Sleeper L, Lachman ME, Heislein D, Giorgetti M, et al. A home‐based exercise program for nondisabled older adults. Journal of the American Geriatrics Society 1996;44(6):644‐9. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Jobe 2001 {published data only}
- Jobe JB, Smith DM, Ball K, Tennstedt SL, Marsiske M, Willis SL. ACTIVE: a cognitive intervention trial to promote independence in older adults. Controlled Clinical Trials 2001;22(4):453‐79. [DOI] [PMC free article] [PubMed] [Google Scholar]
Kaukiainen 2002 {published data only}
- Kaukiainen A, Nygard CH, Virtanen P, Saloniemi A. Physical activity intervention among unemployed male construction workers. Advances in Physiotherapy 2002;4(1):1‐15. [Google Scholar]
Keele‐Smith 2003 {published data only}
- Keele‐Smith R, Leon T. Evaluation of individually tailored interventions on exercise adherence. Western Journal of Nursing Research 2003;25(6):623‐40. [DOI] [PubMed] [Google Scholar]
Kelley 2004 {published data only}
- Kelley K, Abraham C. RCT of a theory‐based intervention promoting healthy eating and physical activity amongst out‐patients older than 65 years. Social Science & Medicine 2004;59(4):787‐97. [DOI] [PubMed] [Google Scholar]
Kennedy 2003 {published data only}
- Kennedy MF, Meeuwisse WH. Exercise counselling by family physicians in Canada. Preventive Medicine 2003;37(3):226‐32. [DOI] [PubMed] [Google Scholar]
Kerr 2000 {published data only}
- Kerr J, McKenna J. A randomized control trial of new tailored walking campaigns in an employee sample. Journal of Health Communication 2000;5(3):265‐79. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Kim 2004 {published data only}
- Kim S, Koniak‐Griffin D, Flaskerud JH, Guarnero PA. The impact of lay health advisors on cardiovascular health promotion: using a community‐based participatory approach. Journal of Cardiovascular Nursing 2004;19(3):192‐9. [DOI] [PubMed] [Google Scholar]
King 1984 {published data only}
- King AC, Frederiksen LW. Low‐cost strategies for increasing exercise behaviour. Behavior Modification 1984;8(1):3‐21. [MEDLINE: ] [Google Scholar]
King 1995 {published data only}
- King AC, Haskell WL, Young DR, Oka RK, Stefanick ML. Long‐term effects of varying intensities and formats of physical activity on participation rates, fitness, and lipoproteins in men and women aged 50 to 65 years. Circulation 1995;91(10):2596‐604. [DOI] [PubMed] [Google Scholar]
King 1997 {published data only}
- King AC, Oman RF, Brassington GS, Bliwise DL, Haskell WL. Moderate‐intensity exercise and self‐rated quality of sleep in older adults. A randomized controlled trial. JAMA 1997;277(1):32‐7. [MEDLINE: ] [PubMed] [Google Scholar]
King 2000 {published data only}
- King AC, Pruitt LA, Phillips W, Oka R, Rodenburg A, Haskell WL. Comparative effects of two physical activity programs on measured and perceived physical functioning and other health‐related quality of life outcomes in older adults. Journals of Gerontology Series A‐Biological Sciences & Medical Sciences 2000;55(2):M74‐83. [DOI] [PubMed] [Google Scholar]
King 2001 {published data only}
- King AC. Interventions to promote physical activity by older adults. J Gerontol A Biol Sci Med Sci 2001;56:36‐46. [DOI] [PubMed] [Google Scholar]
Kinion 1993 {published data only}
- Kinion ES, Christie N, Villella AM. Promoting activity in the elderly through interdisciplinary linkages. NursingConnections 1993;6(3):19‐26. [MEDLINE: ] [PubMed] [Google Scholar]
Kirk 2001 {published data only}
- Kirk AF, Higgins LA, Hughes AR, Fisher BM, Mutrie N, Hillis S, et al. A randomized, controlled trial to study the effect of exercise consultation on the promotion of physical activity in people with Type 2 diabetes: a pilot study. Diabetic Medicine 2001;18(11):877‐82. [DOI] [PubMed] [Google Scholar]
Kirk 2004 {published data only}
- Kirk AF, Mutrie N, MacIntyre PD, Fisher MB. Promoting and maintaining physical activity in people with type 2 diabetes. American Journal of Preventive Medicine 2004;27(4):289‐96. [DOI] [PubMed] [Google Scholar]
Kirk‐Gardner 2003 {published data only}
- Kirk‐Gardner R, Steven D. Hearts for Life: a community program on heart health promotion. Canadian Journal of Cardiovascular Nursing 2003;13(1):5‐10. [PubMed] [Google Scholar]
Koffman 2001 {published data only}
- Koffman DM, Bazzarre T, Mosca L, Redberg R, Schmid T, Wattigney WA. An evaluation of Choose to Move 1999: an American Heart Association physical activity program for women. Archives of Internal Medicine 2001;161(18):2193‐9. [DOI] [PubMed] [Google Scholar]
Kohno 2002 {published data only}
- Kohno H, Egawa K, Oida Y, Nagamatsu T, Kitabatake Y, Maie H. Effect of functional fitness promotion program for community‐dwelling elderly person using the transtheoretical model. Bulletin of the Physical Fitness Research Institute 2001;100:11‐20. [Google Scholar]
Kontulainen 2004 {published data only}
- Kontulainen S, Heinonen A, Kannus P, Pasanen M, Sievanen H, Vuori I. Former exercisers of an 18‐month intervention display residual aBMD benefits compared with control women 3.5 years post‐intervention: a follow ‐up of a randomized controlled high‐impact trial. Osteoporosis International 2004;15(3):248‐51. [DOI] [PubMed] [Google Scholar]
Kukkonen‐H 1998 {published data only}
- Kukkonen‐Harjula K, Laukkanen R, Vuori I, Oja P, Pasanen M, Nenonen A, et al. Effects of walking training on health‐related fitness in healthy middle‐aged adults‐‐a randomized controlled study. Scandinavian Journal of Medicine & Science in Sports 1998;8(4):236‐42. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Lansdown 2002 {published data only}
- Lansdown R, Ledward A, Hall A, Issae W, Yona E, Matulu J. Physical activity intervention: A Transtheoretical Model‐based intervention designed to help sedentary young adults become active. Health Educucation Research 2002;17(4):451‐60. [DOI] [PubMed] [Google Scholar]
Lawlor 2001 {published data only}
- Lawlor DA, Hopker SW. The effectiveness of exercise as an intervention in the management of depression: systematic review and meta‐regression analysis of randomised controlled trials. BMJ 2001;322(7289):763‐7. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Leon 1996 {published data only}
- Leon AS, Casal D, Jacobs D, Jr. Effects of 2,000 kcal per week of walking and stair climbing on physical fitness and risk factors for coronary heart disease. Journal of Cardiopulmonary Rehabilitation 1996;16(3):183‐92. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Lewis 1993a {published data only}
- Lewis CE, Raczynski JM, Heath GW, Levinson R, Hilyer JC, Cutter GR. Promoting physical activity in low‐income African‐American communities: the PARR project. Ethnicity & Disease 1993;3(2):106‐18. [MEDLINE: ] [PubMed] [Google Scholar]
Lewis 1993b {published data only}
- Lewis BS, Lynch WD. The effect of physician advice on exercise behavior. Preventive Medicine 1993;22(1):110‐21. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Li 2001 {published data only}
- Li F, Harmer P, McAuley E, Duncan TE, Duncan SC, Chaumeton N, et al. An evaluation of the effects of Tai Chi exercise on physical function among older persons: a randomized contolled trial. Annals of Behavioral Medicine 2001;23(2):139‐46. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Lindstrom 2003 {published data only}
- Lindstrom J, Louheranta A, Mannelin M, Rastas M, Salminen V, Eriksson J. The Finnish Diabetes Prevention Study (DPS): Lifestyle intervention and 3 ‐year results on diet and physical activity. Diabetes Care 2003;26(12):3230‐6. [DOI] [PubMed] [Google Scholar]
Little 2004 {published data only}
- Little P, Dorward M, Gralton S, Hammerton L, Pillinger J, White P, et al. A randomised controlled trial of three pragmatic approaches to initiate increased physical activity in sedentary patients with risk factors for cardiovascular disease. British Journal of General Practice 2004;54(500):189‐95. [PMC free article] [PubMed] [Google Scholar]
Lord 1995 {published data only}
- Lord JC, Green F. Exercise on prescription: does it work?. Health Educucation Journal 1995;54(4):453‐64. [MEDLINE: ] [Google Scholar]
Lupton 2002 {published data only}
- Lupton BS, Fonnebo V, Sogaard AJ, Langfeldt E. The Finnmark Intervention Study. Better health for the fishery population in an Arctic village in North Norway. Scandinavian Journal of Primary Health Care 2002;20(4):213‐8. [DOI] [PubMed] [Google Scholar]
MacKeen 1985 {published data only}
- MacKeen PC, Rosenberger G, Slater JS, Nicholas WC, Buskirk ER. A 13‐year follow‐up of a coronary heart disease risk factor screening and exercise program for 40‐ to 59‐year‐old men: exercise habit maintenance and physiologic status. Journal of Cardiopulmonary Rehabilitation 1985;5(11):510‐23. [Google Scholar]
Manson 1999 {published data only}
- Manson JE, Hu FB, Rich‐Edwards JW, Colditz GA, Stampfer MJ, Willett WC, et al. A prospective study of walking as compared with vigorous exercise in the prevention of coronary heart disease in women. New England Journal of Medicine 1999;341(9):650‐8. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Marcus 1992 {published data only}
- Marcus BH, Banspach SW, Lefebvre RC, Rossi JS, Carleton RA, et al. Using the stages of change model to increase the adoption of physical activity among community participants. American Journal of Health Promotion 1992;6(6):424‐9. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Marcus 1993 {published data only}
- Marcus BH, Stanton AL. Evaluation of relapse prevention and reinforcement interventions to promote exercise adherence in sedentary females. Research Quarterly for Exercise & Sport 1993;64(4):447‐52. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Marcus 1995 {published data only}
- Marcus BH, Albrecht AE, Niaura RS, Taylor ER, Simkin LR, Feder SI, et al. Exercise enhances the maintenance of smoking cessation in women. Addictive Behaviors 1995;20(1):87‐92. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Marcus 1998a {published data only}
- Marcus BH, Emmons KM, Simkin‐Silverman LR, Linnan LA, Taylor ER, Bock BC, et al. Evaluation of motivationally tailored vs. standard self‐help physical activity interventions at the workplace. American Journal of Health Promotion 1998;12(4):246‐53. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Marcus 1998b {published data only}
- Marcus BH, Bock BC, Pinto BM, Forsyth LH, Roberts MB, Traficante RM. Efficacy of an individualized, motivationally‐tailored physical activity intervention. Annals of Behavioral Medicine 1998;20:174‐80. [DOI] [PubMed] [Google Scholar]
Marshall 2003b {published data only}
- Marshall AL, Leslie ER, Bauman AE, Marcus BH, Owen N. Print versus website physical activity programs: a randomized trial. American Journal of Preventive Medicine 2003;25(2):88‐94. [DOI] [PubMed] [Google Scholar]
Martin 2004 {published data only}
- Martin DE, Thuring N, Melges T, Martin BW. The Stages of Change in three stage concepts and two modes of physical activity: A comparison of stage distributions and practical implications. Health Education Research 2004;19(4):400‐17. [DOI] [PubMed] [Google Scholar]
Mattila 2003 {published data only}
- Mattila R, Malmivaara A, Kastarinen M, Kivela SL, Nissinen A. Effectiveness of multidisciplinary lifestyle intervention for hypertension: a randomised controlled trial. Journal of Human Hypertension 2003;17(3):199‐205. [DOI] [PubMed] [Google Scholar]
McAuley 1994 {published data only}
- McAuley E, Courneya KS, Rudolph DL, Lox CL. Enhancing exercise adherence in middle‐aged males and females. Preventive Medicine 1994;23:498‐506. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
McMahon 2002 {published data only}
- McMahon A, Kelleher CC, Helly G, Duffy E. Evaluation of a workplace cardiovascular health promotion programme in the Republic of Ireland. Health Promotion International. 2002;17(4):297‐308. [DOI] [PubMed] [Google Scholar]
McMurdo 1992 {published data only}
- McMurdo ME, Burnett L. Randomised controlled trial of exercise in the elderly. Gerontology 1992;38(5):292‐8. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
McMurdo 1995 {published data only}
- McMurdo ME, Johnstone R. A randomized controlled trial of a home exercise programme for elderly people with poor mobility. Age & Ageing 1995;24(5):425‐8. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Messier 2000 {published data only}
- Messier SP, Royer TD, Craven TE, O'Toole ML, Burns R, Ettinger WH. Long‐term exercise and its effect on balance in older, osteoarthritic adults: results from the Fitness, Arthritis, and Seniors Trial (FAST). Journal of the American Geriatrics Society 2000;48(2):131‐8. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Miller 2002 {published and unpublished data}
- Miller YD, Trost SG, Brown WJ. Mediators of physical activity behavior change among women with young children. American Journal of Preventive Medicine 2002;23(2 Suppl):98‐103. [DOI] [PubMed] [Google Scholar]
Mills 1996 {published data only}
- Mills KM, Stewart AL, King AC, Roitz K, Sepsis PG, Ritter PL, et al. Factors associated with enrollment of older adults into a physical activity promotion program. Journal of Aging & Health 1996;8(1):96‐113. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Milne 2002 {published data only}
- Milne S, Orbell S, Sheeran P. Combining motivational and volitional interventions to promote exercise participation: Protection motivation theory and implementation intentions. British Journal of Health Psychology 2002;7(2):163‐84. [DOI] [PubMed] [Google Scholar]
Mulder 1981 {published data only}
- Mulder JA, Griffin R. Prescription of home exercise therapy for cardiovascular fitness. Journal of Family Practice 1981;13(3):345‐8. [MEDLINE: ] [PubMed] [Google Scholar]
Munsch 2003 {published data only}
- Munsch S, Biedert E, Keller U. Evaluation of a lifestyle change programme for the treatment of obesity in general practice. Swiss Medical Weekly 2003;133(9‐10):148‐54. [DOI] [PubMed] [Google Scholar]
Napolitano 2003 {published data only}
- Napolitano MA, Fotheringham M, Tate D, Sciamanna C, Leslie E, Owen N, et al. Evaluation of an internet‐based physical activity intervention: a preliminary investigation. Annals of Behavioral Medicine 2003;25(2):92‐9. [DOI] [PubMed] [Google Scholar]
Naylor 1999 {published data only}
- Naylor PJ, Simmonds G, Riddoch C, Velleman G, Turton P. Comparison of stage‐matched and unmatched interventions to promote exercise behaviour in the primary care setting. Health Education Research 1999;14(5):653‐66. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Newman 2002 {published data only}
- Newman CF. Effectiveness of physical activity interventions for older adults. American Journal of Preventive Medicine 2002;22(2):120‐33. [DOI] [PubMed] [Google Scholar]
Nisbeth 2000 {published data only}
- Nisbeth O, Klausen K, Andersen LB. Effectiveness of counselling over 1 year on changes in lifestyle and coronary heart disease risk factors. Patient Education & Counseling 2000;40(2):121‐31. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Noland 1989 {published data only}
- Noland MP. The effects of self‐monitoring and reinforcement on exercise adherence. Research Quarterly for Exercise & Sport 1989;60(3):216‐24. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Nurminen 2002 {published data only}
- Nurminen E, Malmivaara A, Ilmarinen J, Ylostalo P, Mutanen P, Ahonen G, et al. Effectiveness of a worksite exercise program with respect to perceived work ability and sick leaves among women with physical work. Scandinavian Journal of Work, Environment and Health 2002;28(2):85‐93. [DOI] [PubMed] [Google Scholar]
Oexmann 2001 {published data only}
- Oexmann MJ, Ascanio R, Egan BM. Efficacy of a church‐based intervention on cardiovascular risk reduction. Ethnicity & Disease 2001;11(4):817‐22. [PubMed] [Google Scholar]
Oida 2003 {published data only}
- Oida Y, Kitabatake Y, Nishijima Y, Nagamatsu T, Kohno H, Egawa K. Effects of a 5‐year exercise‐centered health‐promoting programme on mortality and ADL impairment in the elderly. Age & Aging 2003;32(6):585‐92. [DOI] [PubMed] [Google Scholar]
Oman 2000 {published data only}
- Oman RF, King AC. The effect of life events and exercise program format on the adoption and maintenance of exercise behavior. Health Psychology 2000;19(6):605‐12. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Ortega‐Sanchez 2004 {published data only}
- Ortega‐Sanchez R, Jimenez‐Mena C, Cordoba‐Garcia R, Munoz‐Lopez J, Garcia‐Machado ML, Vilaseca‐Canals J. The effect of office‐based physician's advice on adolescent exercise behavior. Preventive Medicine 2004;38(2):219‐26. [DOI] [PubMed] [Google Scholar]
Ostwald 1989 {published data only}
- Ostwald SK. Changing employees' dietary and exercise practices: an experimental study in a small company. Journal of Occupational Medicine 1989;31(2):90‐7. [MEDLINE: ] [PubMed] [Google Scholar]
Parks 1997 {published data only}
- Parks PSM, Read MH. Adolescent male athletes: Body image, diet, and exercise. Adolescence 1997;32(127):593‐602. [MEDLINE: ] [PubMed] [Google Scholar]
Partonen 1998 {published data only}
- Partonen T, Leppamaki S, Hurme J, Lonnqvist J. Randomized trial of physical exercise alone or combined with bright light on mood and health‐related quality of life. Psychological Medicine 1998;28(6):1359‐64. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Paschal 2004 {published data only}
- Paschal AM, Lewis RK, Martin A, Dennis‐Shipp D, Simpson DS. Baseline assessment of the health status and health behaviors of African Americans participating in the activities‐for‐life program: a community ‐based health intervention program. Journal of Community Health 2004;29(4):305‐18. [DOI] [PubMed] [Google Scholar]
Pereira 1998 {published data only}
- Pereira MA, Kriska AM, Day RD, Cauley JA, LaPorte RE, Kuller LH. A randomized walking trial in postmenopausal women: effects on physical activity and health 10 years later. Archives of Internal Medicine 1998;158(15):1695‐701. [DOI] [PubMed] [Google Scholar]
Peterson 1999 {published data only}
- Peterson TR, Aldana SG. Improving exercise behavior: An application of the stages of change model in a worksite setting. American Journal of Health Promotion 1999;13(4):29‐32. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Peterson 2002 {published data only}
- Peterson J, Atwood JR, Yates B. Key elements for church‐based health promotion programs: outcome‐based literature review. Public Health Nursing 2002;19(6):401‐11. [DOI] [PubMed] [Google Scholar]
Petrella 2000 {published data only}
- Petrella RJ, Wight D. An office‐based instrument for exercise counseling and prescription in primary care. The Step Test Exercise Prescription (STEP). Archives of Family Medicine 2000;9(4):339‐44. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Petrella 2001 {published data only}
- Petrella RJ, Koval JJ, Cunningham DA, Paterson DH. A self‐paced step test to predict aerobic fitness in older adults in the primary care clinic. Journal of the American Geriatrics Society 2001;49(5):632‐8. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Pfeiffer 2001 {published data only}
- Pfeiffer BA, Clay SW, Conatser‐RR J. A green prescription study: does written exercise prescribed by a physician result in increased physical activity among older adults?. Journal of Aging & Health 2001;13(4):527‐38. [DOI] [PubMed] [Google Scholar]
Philips 2004 {published data only}
- Phillips EM, Schneider JC, Mercer GR. Motivating elders to initiate and maintain exercise. Archives of Physical Medicine & Rehabilitation 2004;85(7 Suppl 3):S52‐7. [DOI] [PubMed] [Google Scholar]
Pinto 2001 {published data only}
- Pinto BM, Lynn H, Marcus BH, DePue J, Goldstein MG. Physician‐based activity counseling: intervention effects on mediators of motivational readiness for physical activity. Annals of Behavioral Medicine 2001;23(1):2‐10. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Plotnikoff 2001 {published data only}
- Plotnikoff RC, Hotz SB, Birkett NJ, Courneya KS. Exercise and the transtheoretical model: a longitudinal test of a population sample. Prev Med 2001;33:441‐52. [DOI] [PubMed] [Google Scholar]
Pohjonen 2001 {published data only}
- Pohjonen T, Ranta R. Effects of worksite physical exercise intervention on physical fitness, perceived health status, and work ability among home care workers: Five ‐year follow‐up. Preventive Medicine 2001;32(6):465‐75. [DOI] [PubMed] [Google Scholar]
Poole 2001 {published data only}
- Poole K, Kumpfer K, Pett M. The impact of an incentive‐based worksite health promotion program on modifiable health risk factors. American Journal of Health Promotion 2001;16(1):21‐6. [DOI] [PubMed] [Google Scholar]
Poston 2001 {published data only}
- Poston‐WSC II, Haddock CK, Olvera NE, Suminski RR, Reeves RS, Dunn JK, et al. Evaluation of culturally appropriate intervention to increase physical activity. American Journal of Health Behavior 2001;25(4):396‐406. [DOI] [PubMed] [Google Scholar]
Proper 2003a {published data only}
- Proper KI, Hildebrandt VH, Beek AJ, Twisk JW, Mechelen W. Effect of individual counseling on physical activity fitness and health: a randomized controlled trial in a workplace setting. American Journal of Preventive Medicine 2003;24(3):218‐26. [DOI] [PubMed] [Google Scholar]
Proper 2003b {published data only}
- Proper KI, Koning M, Beek AJ, Hildebrandt VH, Bosscher RJ, Mechelen W. The effectiveness of worksite physical activity programs on physical activity, physical fitness, and health. Clinical Journal of Sport Medicine 2003;13(2):106‐17. [DOI] [PubMed] [Google Scholar]
Purath 2004 {published data only}
- Purath J, Miller AM, McCabe G, Wilbur J. A brief intervention to increase physical activity in sedentary working women. Canadian Journal of Nursing Research 2004;36(1):76‐91. [PubMed] [Google Scholar]
Reijneveld 2003 {published data only}
- Reijneveld SA, Westhoff MH, Hopman‐Rock M. Promotion of health and physical activity improves the mental health of elderly immigrants: results of a group randomised controlled trial among Turkish immigrants in the Netherlands aged 45 and over. Journal of Epidemiology & Community Health 2003;57(6):405‐11. [DOI] [PMC free article] [PubMed] [Google Scholar]
Renger 2002 {published data only}
- Renger R, Steinfelt V, Lazarus S. Assessing the effectiveness of a community‐based media campaign targeting physical inactivity. Family & Community Health 2002;25(3):18‐30. [DOI] [PubMed] [Google Scholar]
Resnick 2002b {published data only}
- Resnick B, Magaziner J, Orwig D, Zimmerman S. Evaluating the components of the Exercise Plus Program: rationale, theory and implementation. Health Education Research 2002;17(5):648‐58. [DOI] [PubMed] [Google Scholar]
Reynolds 2001 {published data only}
- Reynolds F. Strategies for facilitating physical activity and wellbeing: A health promotion perspective. British Journal of Occupational Therapy 2001;64(7):330‐6. [Google Scholar]
Robison 1992 {published data only}
- Robison JI, Rogers MA, Carlson JJ, Mavis BE. Effects of a 6‐month incentive‐based exercise program on adherence and work capacity. Medicine & Science in Sports & Exercise 1992;24(1):85‐93. [MEDLINE: ] [PubMed] [Google Scholar]
Ruby 1993 {published data only}
- Ruby KL, Blainey CA, Haas LB, Patrick M. The knowledge and practices of registered nurse, certified diabetes educators: teaching elderly clients about exercise. Diabetes Educator 1993;19(4):299‐306. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Samaras 1997 {published data only}
- Samaras K, Ashwell S, Mackintosh AM, Fleury AC, Campbell LV, Chisholm DJ. Will older sedentary people with non‐insulin‐dependent diabetes mellitus start exercising? A health promotion model. Diabetes Research & Clinical Practice 1997;37(2):121‐128. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Schoenfelder 2000 {published data only}
- Schoenfelder DP. A fall prevention program for elderly individuals. Exercise in long‐term care settings. Journal of Gerontological Nursing 2000;26(3):43‐51. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Schuler 2002 {published data only}
- Schuler G. Primary and secondary prevention: physical activity [Primare und sekundare Pravention: Korperliche Aktivitat]. Zeitschrift fur Kardiologie 2002;91(Suppl 2):30‐9. [PubMed] [Google Scholar]
Sciamanna 2002 {published data only}
- Sciamanna CN, Lewis B, Tate D, Napolitano MA, Fotheringham M, Marcus BH. User attitudes toward a physical activity promotion website. Preventive Medicine 2002;35(6):612‐5. [DOI] [PubMed] [Google Scholar]
Sevick 2000 {published data only}
- Sevick MA, Dunn AL, Morrow MS, Marcus BH, Chen GJ, Blair SN. Cost‐effectiveness of lifestyle and structured exercise interventions in sedentary adults: Results of Project ACTIVE. American Journal of Preventive Medicine 2000;19(1):1‐8. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Simmons 2003 {published data only}
- Simmons D, Voyle JA. Reaching hard‐to‐reach, high‐risk populations: piloting a health promotion and diabetes disease prevention programme on an urban marae in New Zealand. Health Promotion International 2003;18(1):41‐50. [DOI] [PubMed] [Google Scholar]
Sims 2004 {published data only}
- Sims J, Huang N, Pietsch J, Naccarella L. The Victorian Active Script Programme: promising signs for general practitioners, population health, and the promotion of physical activity. British Journal of Sports Medicine 2004;38(1):19‐25. [DOI] [PMC free article] [PubMed] [Google Scholar]
Singh 1997 {published data only}
- Singh S. Why are GP exercise schemes so successful (for those who attend)? Results from a pilot study. Journal of Management in Medicine 1997;11(4):233‐7. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Singh 1997a {published data only}
- Singh NA, Clements KM, Fiatarone MA. A randomized controlled trial of progressive resistance training in depressed elders. Journals of Gerontology Series A‐Biological Sciences & Medical Sciences 1997;52(1):M27‐35. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Smith 2003 {published data only}
- Smith BJ, Brown BJ, Hermann JR. Impact of a physical activity program emphasizing cardiovascular fitness, muscle strength, and flexibility among middle‐aged women. Journal of Nutrition Education & Behavior 2003;35(4):215‐216. [DOI] [PubMed] [Google Scholar]
Smolander 2000 {published data only}
- Smolander J, Blair SN, Kohl HW. Work ability, physical activity, and cardiorespiratory fitness: 2‐year results from Project Active. Journal of Occupational & Environmental Medicine 2000;42(9):906‐10. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Sorensen 1999 {published data only}
- Sorensen M, Anderssen S, Hjerman I, Holme I, Ursin H. The effect of exercise and diet on mental health and quality of life in middle‐aged individuals with elevated risk factors for cardiovascular disease. Journal of Sports Sciences 1999;5(17):369‐77. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Steptoe 1999 {published data only}
- Steptoe A, Doherty S, Rink E, Kerry S, Kendrick T, Hilton S. Behavioural counselling in general practice for the promotion of healthy behaviour among adults at increased risk of coronary heart disease: randomized trial. BMJ 1999;319(7215):943‐7. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Steptoe 2000 {published data only}
- Steptoe A, Rink E, Kerry S. Psychosocial predictors of changes in physical activity in overweight sedentary adults following counseling in primary care. Preventive Medicine 2000;31(2 Pt 1):183‐94. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Steptoe 2001 {published data only}
- Steptoe A, Kerry S, Rink E, Hilton S. The impact of behavioral counseling on stage of change in fat intake, physical activity, and cigarette smoking in adults at increased risk of coronary heart disease. American Journal of Public Health 2001;91(2):265‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
Stevens 1999 {published data only}
- Stevens M, Bult P, Greef MH, Lemmink KA, Rispens P. Groningen Active Living Model (GALM): stimulating physical activity in sedentary older adults. Preventive Medicine 1999;29(4):267‐76. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Stevens 2003 {published data only}
- Stevens M, Lemmink KA, Heuvelen MJ, Jong J, Rispens P. Groningen Active Living Model (GALM): stimulating physical activity in sedentary older adults; validation of the behavioral change model. Preventive Medicine 2003;37(6 Pt 1):561‐70. [DOI] [PubMed] [Google Scholar]
Stiggelbout 2004 {published data only}
- Stiggelbout M, Popkema DY, Hopman‐Rock M, Greef M, Mechelen W. Once a week is not enough: effects of a widely implemented group based exercise programme for older adults; a randomised controlled trial. Journal of Epidemiology & Community Health 2004;58(2):83‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Swinburn 2003 {published data only}
- Swinburn B, Sager R. Promotion of exercise prescriptions in general practice for older populations. Geriatrics and Aging 2003;6(7):20‐23. [Google Scholar]
Taylor 1998 {published data only}
- Taylor AH, Doust J, Webborn N. Randomised controlled trial to examine the effects of a GP exercise referral programme in Hailsham, East Sussex, on modifiable coronary heart disease risk factors. Journal of Epidemiology & Community Health 1998;52(9):595‐601. [DOI] [PMC free article] [PubMed] [Google Scholar]
Twisk 2004 {published data only}
- Twisk J, Proper K. Evaluation of the results of a randomized controlled trial: how to define changes between baseline and follow‐up. Journal of Clinical Epidemiology 2004;57(3):223‐8. [DOI] [PubMed] [Google Scholar]
van der Bij 2002 {published data only}
- Bij AK, Laurant M, Wensing M. Effectiveness of physical activity interventions for older adults: a review. American Journal of Preventive Medicine 2002;22(2):120‐33. [DOI] [PubMed] [Google Scholar]
Veverka 2003 {published data only}
- Veverka D, Anderson J, Auld G, Coulter G, Kennedy C, Chapman P, et al. Use of the stages of change model in improving nutrition and exercise habits in enlisted Air Force men. Military Medicine 2003;168(5):373‐9. [PubMed] [Google Scholar]
Votruba 1968 {published data only}
- Votruba SB, Horvitz MA, Schoeller DA. The role of exercise in the treatment of obesity. Nutrition 2000;16(3):179‐88. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Vuori 1994 {published data only}
- Vuori IM, Oja P, Paronen O. Physically active commuting to work‐‐testing its potential for exercise promotion. Medicine & Science in Sports & Exercise 1994;26(7):844‐50. [MEDLINE: ] [PubMed] [Google Scholar]
Wankel 1985 {published data only}
- Wankel LM, Yardley JK, Graham J. The effects of motivational interventions upon the exercise adherence of high and low self‐motivated adults. Canadian Journal of Applied Sport Sciences 1985;10(3):147‐56. [MEDLINE: ] [PubMed] [Google Scholar]
Weinehall 2001 {published data only}
- Weinehall L, Hellsten G, Boman K, Hallmans G. Prevention of cardiovascular disease in Sweden: the Norsjo community intervention programme‐‐motives, methods and intervention components. Scandinavian Journal of Public Health. Supplement 2001;56:13‐20. [PubMed] [Google Scholar]
Wen 2002 {published data only}
- Wen LM, Thomas M, Jones H, Orr N, Moreton R, King L, et al. Promoting physical activity in women: evaluation of a 2‐year community ‐based intervention in Sydney, Australia. Health Promotion International 2002;17(2):127‐37. [DOI] [PubMed] [Google Scholar]
Wilbur 2001 {published data only}
- Wilbur J, Chandler P, Miller AM. Measuring adherence to a women's walking program. Western Journal of Nursing Research 2001;23(1):8‐24. [DOI] [PubMed] [Google Scholar]
Wood 1983 {published data only}
- Wood PD, Haskell WL, Blair SN, Williams PT, Krauss RM, Lindgren FT, et al. Increased exercise level and plasma lipoprotein concentrations: a one‐year, randomized, controlled study in sedentary, middle‐aged men. Metabolism: Clinical & Experimental 1983;32(1):31‐9. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Woods 2002 {published data only}
- Woods C, Mutrie N, Scott M. Physical activity intervention: a transtheoretical model‐based intervention designed to help sedentary young adults become active. Health Education Research 2002;17(4):451‐60. [DOI] [PubMed] [Google Scholar]
Yalden 2001 {published data only}
- Yalden J, Chung L. Tai Chi: towards an exercise program for the older person. Australian Journal of Holistic Nursing 2001;8(1):4‐13. [PubMed] [Google Scholar]
Yanek 2001 {published data only}
- Yanek LR, Becker DM, Moy TF, Gittelsohn J, Koffman DM. Project Joy: faith based cardiovascular health promotion for African American women. Public Health Reports 2001;116(Suppl 1):68‐81. [DOI] [PMC free article] [PubMed] [Google Scholar]
Young 1999 {published data only}
- Young DR, Appel LJ, Jee S, Miller ER 3rd. The effects of aerobic exercise and T'ai Chi on blood pressure in older people: results of a randomized trial. Journal of the American Geriatrics Society 1999;47(3):277‐284. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Zask 2001 {published data only}
- Zask A, Beurden E, Barnett L, Brooks LO, Dietrich UC. Active school playgrounds‐myth or reality? Results of the "move it groove it" project. Preventive Medicine 2001;33(5):403‐8. [DOI] [PubMed] [Google Scholar]
References to studies awaiting assessment
Castro 2001 {published data only}
- Castro CM, King AC, Brassington GS. Telephone versus mail interventions for maintenance of physical activity in older adults. Health Psychology 2001;20(6):438‐44. [PubMed] [Google Scholar]
Lowther 2002a {published data only}
- Lowther M, Mutrie N, Scott EM. Promoting physical activity in a socially and economically deprived community: a 12 month randomized control trial of fitness assessment and exercise consultation. Journal of Sports Sciences 2002;20(7):577‐88. [DOI] [PubMed] [Google Scholar]
Lowther 2002b {published data only}
- Lowther M, Mutrie N, Scott EM. Promoting physical activity in a socially and economically deprived community: a 12 month randomized control trial of fitness assessment and exercise consultation. Journal of Sports Sciences 2002;20(7):577‐88. [DOI] [PubMed] [Google Scholar]
Mutrie 2002 {published data only}
- Mutrie N, Carney C, Blamey A, Crawford F, Aitchison T, Whitelaw A. "Walk in to Work Out": a randomised controlled trial of a self help intervention to promote active commuting. Journal of Epidemiology & Community Health 2002;56:407‐12. [DOI] [PMC free article] [PubMed] [Google Scholar]
Nies 2003 {published data only}
- Nies MA, Chruscial HL, Hepworth JT. An intervention to promote walking in sedentary women in the community. American Journal of Health Behavior 2003;27(5):524‐35. [DOI] [PubMed] [Google Scholar]
Zakocs 2003 {published data only}
- Zakocs RC, Earp JA. Population‐based randomized controlled trial of a stage‐targeted physical activity intervention. Annals of Behavioral Medicine 2003;25(3):194‐202. [DOI] [PubMed] [Google Scholar]
References to ongoing studies
Coday 2002 {published data only}
- Coday M, Klesges LM, Garrison RJ, Johnson KC, O'Toole M, Morris GS. Health Opportunities with Physical Exercise (HOPE): social contextual interventions to reduce sedentary behavior in urban settings. Health Education Research 2002;17(5):637‐47. [DOI] [PubMed] [Google Scholar]
Grandes 2003 {published data only}
- Grandes G, Sánchez A, Torcal J, Ortega Sánchez‐Pinilla R, Lizarraga K, Serra J, et al. Protocol for the multi‐centre evaluation of the Experimental Programme Promotion of Physical Activity (PEPAF) [Protocolo para la evaluacion multicentrica del Programa Experimental de Promocion de la Actividad Fisica (PEPAF)]. Atencion Primaria 2003;32(8):475‐80. [DOI] [PMC free article] [PubMed] [Google Scholar]
King 2002 {published data only}
- King AC, Friedman R, Marcus B, Castro C, Forsyth L, Napolitano M, Pinto B. Harnessing motivational forces in the promotion of physical activity: the Community Health Advice by Telephone (CHAT) project. Health Educucation Research 2002;17(5):627‐36. [DOI] [PubMed] [Google Scholar]
Additional references
Ashworth 2005
- Ashworth NL, Chad KE, Harrison EL, Reeder BA, Marshall SC. Home versus center based physical activity programs in older adults. Cochrane Database of Systematic Reviews 2005, Issue 1. [DOI: 10.1002/14651858.CD004017.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Bandura 1986
- Bandura A. Social foundations of thought and action. Englewood Cliffs, NJ: Prentice Hall, 1986. [Google Scholar]
Dickersin 1995
- Dickersin K, Scherer, Lefebvre C. Identifying relevant studies from systematic reviews. In: Chalmers I, Altman DG editor(s). Systematic Reviews. London: BMJ Publishing Group, 1995:64‐74. [Google Scholar]
DOH 2004
- Department of Health. At least five a week: evidence on the impact of physical activity and its relationship to health. A report from the Chief Medical Officer. London: Department of Health, 2004. [Google Scholar]
DOH 2005a
- Department of Health. Health Survey for England 2004. London: The Stationary Office, 2005. [Google Scholar]
DOH 2005b
- Department of Health. Choosing Activity: a physical activity action plan. London: Department of Health, 2005. [Google Scholar]
FNB 2002
- Food, Nutrition Board (FNB). Institute of Medicine (IOM). Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids (Macronutrients). A Report of the Panel on Macronutrients, Subcommittees on Upper Reference Levels of Nutrients and Interpretation and Uses of Dietary Reference Intakes, and the Standing Committee on the Scientific Evaluation of Dietary Reference Intakes. Washington: National Academies Press, 2002:697‐736. [Google Scholar]
Folsom 1997
- Folsom AR, Arnett DK, Hutchinson RG, Liao F, Clegg LX, Cooper LS. Physical activity and incidence of coronary heart disease in middle‐aged women and men. Medicine & Science in Sports & Exercise 1997;29:901‐9. [DOI] [PubMed] [Google Scholar]
Higgins 2005
- Higgins JPT, Green S. Cochrane Handbook for Systematic Reviews of Interventions 4.2.5. John Wiley & Sons, Ltd, 2005. [Google Scholar]
Hillsdon 1996
- Hillsdon M, Thorogood M. A systematic review of physical activty promotion strategies. British Journal of Sports Medicine 1996;30(2):84‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
Hillsdon 1999
- Hillsdon M, Thorogood M, Foster C. A systematic review of physical activity promotion strategies. In: D MacAuley editor(s). Exercise Benefits and Risks. London: BMJ Press, 1999. [Google Scholar]
Hillsdon 2004
- Hillsdon M, Foster C, Naidoo B, Crombie H. The effectiveness of public health interventions for increasing physical activity among adults: a review of reviews. London: Health Development Agency, 2004. [Google Scholar]
Hillsdon 2005
- M Hillsdon, C Foster, M Thorogood. Interventions for promoting physical activity. Cochrane Database of Systematic Reviews 2005, Issue 1. [DOI: 10.1002/14651858.CD003180.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
HM Treasury 2002
- HM Treasury. Public Service Agreements 2003 ‐ 2006. London: HM Treasury, 2002. [Google Scholar]
Jolliffe 2001
- Jolliffe JA, Rees K, Taylor RS, Thompson D, Oldridge N, Ebrahim S. Exercise‐based rehabilitation for coronary heart disease. Cochrane Database of Systematic Reviews 2001, Issue 1. [DOI: 10.1002/14651858.CD001800] [DOI] [PubMed] [Google Scholar]
Kahn 2002
- Kahn E B, Ramsey LT, Brownson RC, Health GW, Howze EH, Powell KE, et al. The effectiveness of interventions to increase physical activity: a systematic review. American Journal of Preventive Medicine 2002;22(4 Suppl):73‐107. [DOI] [PubMed] [Google Scholar]
Lefebvre 1996
- Lefebvre C, McDonald S. Development of a sensitive search strategy for reports of randomised controlled trials in EMBASE. Paper presented at the Fourth International Cochrane Colloquium, 20 ‐24 Oct ; Adelaide, Australia. 1996.
Pate 1995
- Pate RR, Pratt M, Blair SN, Haskell WL, Macera CA, Bouchard C, et al. Physical activity and public health: a recommendation from the Centers for Disease Control and Prevention and the American College of Sports Medicine. JAMA 1995;273:402‐7. [DOI] [PubMed] [Google Scholar]
Thomas 2006
- Thomas DE, Elliott EJ, Naughton GA. Exercise for type 2 diabetes mellitus. Cochrane Database of Systematic Reviews 2006, Issue 3. [DOI: 10.1002/14651858.CD002968.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
US Dept. Health 1996
- US Department of Health and Human Services. Physical activity and health: a report of the surgeon general. Atlanta, GA: US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, 1996. [Google Scholar]
WHO 2002
- World Health Organisation. World Health Report 2002. Geneva: World Health Organisation, 2002. [Google Scholar]
WHO 2004
- World Health Organisation. Global Strategy on diet, nutrition and physical activity. Geneva: World Health Organisation, 2004. [Google Scholar]
Williams 2001
- Williams PT. Physical fitness and activity as separate heart disease risk factors: a meta‐analysis. Medicine and Science in Sports and Exercise 2001;33(5):754‐62. [DOI] [PMC free article] [PubMed] [Google Scholar]
Zelen 1990
- Zelen, M. Randomized consent designs for clinical trials: an update. Statistics in Medicine 1990;9(6):645‐6. [DOI] [PubMed] [Google Scholar]