

Abstract
While the International Prognostic Index is commonly used to predict outcomes in immunocompetent patients with aggressive B-cell non-Hodgkin lymphomas, HIV-infection is an important competing risk for death in patients with AIDS-related lymphomas. We investigated whether a newly created prognostic score (AIDS-related lymphoma International Prognostic Index) could better assess risk of death in patients with AIDS-related lymphomas. We randomly divided a dataset of 487 patients newly diagnosed with AIDS-related lymphomas and treated with rituximab-containing chemoimmunotherapy into a training (n=244) and validation (n=243) set. We examined the association of HIV-related and other known risk factors with overall survival in both sets independently. We defined a new score (AIDS-related lymphoma International Prognostic Index) by assigning weights to each significant predictor [age-adjusted International Prognostic Index, extranodal sites, HIV-score (composed of CD4 count, viral load, and prior history of AIDS)] with three risk categories similar to the age-adjusted International Prognostic Index (low, intermediate and high risk). We compared the prognostic value for overall survival between AIDS-related lymphoma International Prognostic Index and age-adjusted International Prognostic Index in the validation set and found that the AIDS-related lymphoma International Prognostic Index performed significantly better in predicting risk of death than the age-adjusted International Prognostic Index (P=0.004) and better discriminated risk of death between each risk category (P=0.015 vs. P=0.13). Twenty-eight percent of patients were defined as low risk by the ARL-IPI and had an estimated 5-year overall survival (OS) of 78% (52% intermediate risk, 5-year OS 60%; 20% high risk, 5-year OS 50%).
Introduction
The International Prognostic Index (IPI) was developed in 1993 by the International Non-Hodgkin Lymphoma (NHL) Prognostic Factors Project to create a prognostic tool for patients with aggressive NHL treated with doxorubicin-containing chemotherapy.1 Among the aggressive lymphomas included, diffuse large B-cell lymphoma (DLBCL) was most common. The IPI categorizes patients into low-, intermediate- and high-risk groups based on the base-line characteristics of age, ECOG performance status (PS), lactate dehydrogenase (LDH) level, Ann Arbor stage, and extranodal involvement. The age-adjusted IPI (aaIPI) stratifies prognosis based on age (< 60 vs. ≥ 60) and relies solely on stage, PS, and LDH. Both prognostic indices are commonly used to provide prognostic information in immunocompetent patients with newly diagnosed aggressive NHL, and have been validated in patients treated with rituximab plus doxorubicin-containing chemotherapy.2 The IPI is also prognostic for lymphomas associated with the acquired immunodeficiency syndrome (AIDS) caused by the human immunodeficiency virus (HIV). This includes patients diagnosed with lymphoma in the era of combination antiretroviral therapy (cART).3–6
Nevertheless, several factors require refinement of the IPI in patients with AIDS-related lymphomas (ARL). First, ARL commonly include more aggressive lymphomas than DLBCL, including Burkitt lymphoma (BL). BL requires more intensive chemotherapy, which, while feasible, may be less well tolerated by HIV-infected patients.7–10 Second, rituximab has been associated with an increased risk of infectious deaths in patients with ARL and low base-line CD4 counts.11 Third, HIV infection is a competing risk that may influence prognosis, and may be dependent not only on the base-line CD4 count, but also on other factors.
We, therefore, sought to develop and independently validate a clinically relevant prognostic index for HIV-positive patients diagnosed with aggressive NHL and treated in the rituximab-era by analyzing data from 487 patients with ARL who were prospectively treated on clinical trials with rituximab plus chemotherapy. In a training set of 236 patients, we identified the influence of HIV-specific factors in addition to a variety of lymphoma-specific factors on overall survival (OS). We then created a new prognostic index called the “ARL-IPI” which integrated these factors, and validated the ARL-IPI in a separate validation set of 251 patients.
Methods
Patients and data collection
We performed a systematic review of the literature to identify prospectively conducted clinical trials that assessed therapeutic interventions for HIV-associated NHL. A detailed description of the search strategy has been previously reported12 and is available in the Online Supplementary Appendix. We limited our dataset to only patients treated with rituximab-containing chemoimmunotherapy.
Clinical variables
We collected individual patient information for the following variables: age, sex, ECOG PS, CD4 count and viral load (VL) at diagnosis, history of any AIDS-defining illness prior to NHL diagnosis (h/o AIDS), type of lymphoma, Ann-Arbor stage, LDH, number of involved extranodal sites (ENS), and type of chemotherapy. Complete response (CR) was defined as per the individual study protocol. Overall survival was defined as time from enrollment to death from any cause; progression-free survival (PFS) was time to progression, relapse or death from any cause. The Albert Einstein College of Medicine institutional review board approved the study.
Statistical analysis
Patients’ demographic, lymphoma, treatment, and HIV characteristics were summarized. CD4 count at diagnosis was classified as an ordinal variable (<50; 50–199; 200–499; ≥500cells/mL); similarly, the variable VL at diagnosis was examined as an ordinal variable (<400; 400–9,999; ≥10,000 copies/mL). The categorizations for ordinal variables were based on clinically and biologically relevant cut-off points following discussion with HIV experts and review of the IDSA guidelines.13 As the lowest limit of detection of the viral load assays varied between the studies, we chose viral load less than 400 copies/mL as the lowest value instead of ‘undetectable’ or less than 50 copies/mL. IPI and age-adjusted IPI were calculated in our dataset for each patient from the available data.
To assess the overall effect of HIV-related immunodeficiency on lymphoma prognosis among HIV-positive patients, we defined an HIV-score as a combination of individual risk factors. The weight of each variable was determined by examining univariate association with OS.
A random sample splitting method was used in which the prognostic indices (HIV score, IPI, and aaIPI) were examined by using half the data (training set). Specifically, the association of the HIV score in addition to patients’ and lymphoma characteristics with OS was examined in the training set using a Cox proportional hazard model. A new index, the ARL-IPI, was developed by assigning appropriate weight to each significant predictor, depending on the estimated strength of association in the Cox model. The performance of these indices was then examined using the remaining half of the data (validation set). Details are described in the Online Supplementary Appendix.
To verify the random splitting of training and validation sets, the two sets were compared descriptively for patients’ characteristics.
For all statistical models assumptions were evaluated; none were found violated. P<0.05 was considered statistically significant; all statistical tests were two-sided. We quoted 95% confidence intervals (95% CI) whenever applicable. We used SAS software, v.9.2 (SAS Institute Inc., Cary, NC, USA) for statistical analysis. For continuous variables such as VL and ENS, which had 30– 40% missing data, we imputed the missing data using multiple imputations and P-values were generated with the MIANALYZE procedure in SAS.
Results
Patients’ characteristics
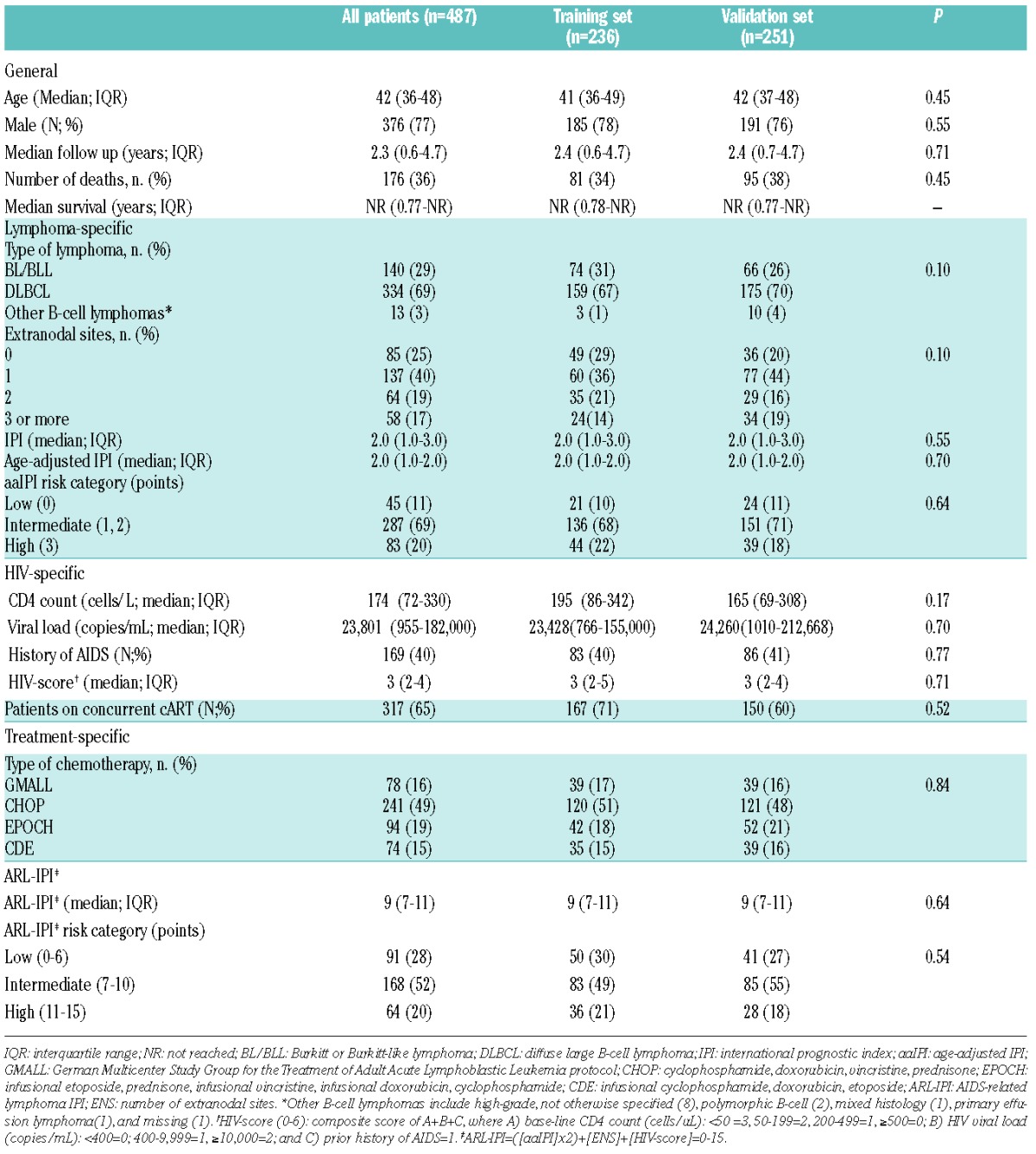
Patient data for 1546 patients from 19 trials were collected. Of the original dataset, 1059 patients were excluded as they had not received rituximab-containing chemoimmunotherapy (Figure 1). Thus, 487 patients from 8 clinical trials (Online Supplementary Table 1S) were available for analysis. These patients were randomly divided into training (n=236) and validation (n=251) sets. Base-line patients’ characteristics between both sets were well balanced (Table 1). Deaths were observed in 176 patients. The most common cause of death was progressive or relapsed disease (n=77), followed by treatment-related deaths (n=48) and complications of HIV (n=23). After a median follow up of 2.3 years, median survival for all patients had not been reached.
Figure 1.
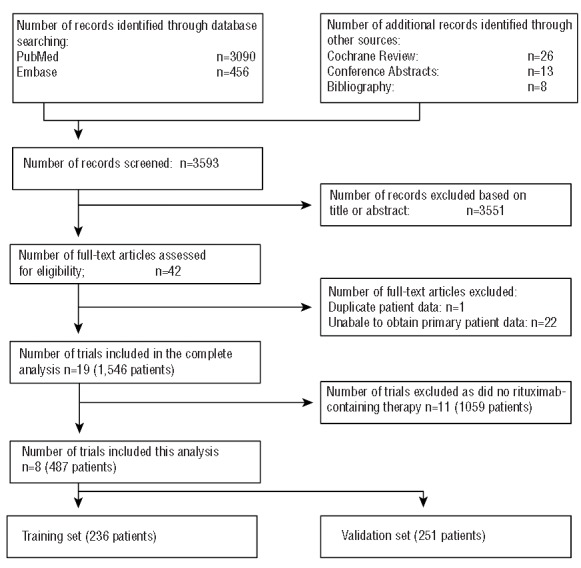
CONSORT diagram documenting the flow of information through the different phases of the systematic review as per the PRISMA statement.
Table 1.
Patients’ characteristics.
Definition of HIV score
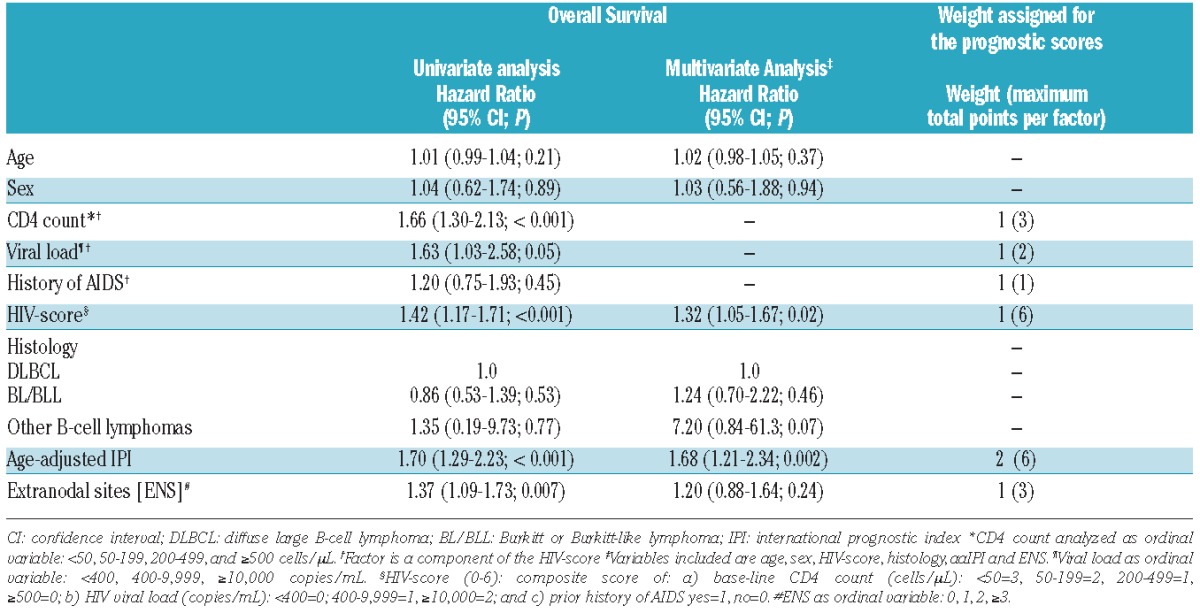
CD4 count, HIV VL and AIDS history were each individually correlated with OS. Their estimated log of the hazard ratio (HR) did not differ from each other by more than 150% (Table 2). For ease of clinical use, equal weight was assigned to each individual variable, i.e. the points from each variable were simply added together to achieve an HIV-score, resulting in a possible maximum score of 6. Each level increase in this HIV-score resulted in a HR of 1.42 (95%CI: 1.17–1.71) in univariate analysis, where one level increase in HIV score can be a result of one level decrease in CD4, one level increase in VL, or with prior history of AIDS.
Table 2.
Association of prognostic factors with overall survival in the training set (n=236).
Development of the ARL-IPI
In the multivariate model, the estimated HR for OS associated with the HIV score was 1.32 (95%CI: 1.05–1.67), 1.20 (95%CI: 0.88–1.64) for ENS, and 1.68 (95%CI: 1.21–2.34) for aaIPI (Table 2). The magnitude of the estimated log of HR was used as the base for assigning weights for each variable (details available in Online Supplementary Methods). We, therefore, assigned weight=1 for both the HIV score and ENS, and weight=2 for the aaIPI in defining the ARL-IPI. In particular, the ARL-IPI score is composed as follows: points assigned to the aaIPI (LDH abnormal, stage >2, ECOG PS>1 each 1 point) multiplied by two, plus the number of ENS (ENS=0, 1 ENS=1, 2 ENS=2, 3 or more ENS=3) and the HIV score (Online Supplementary Table 2S).
Assessment of contribution from each individual component of ARL-IPI
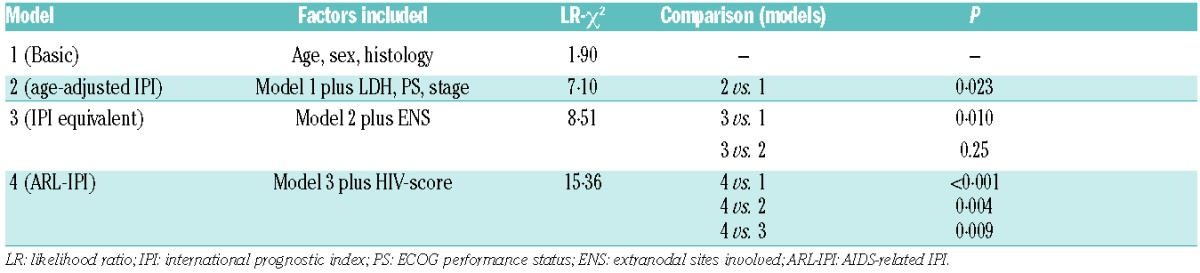
First, we created a basic model (model 1) consisting only of the known biologically relevant factors of age, sex and histology in order to adjust for confounding variables in the subsequent models. We then added the age-adjusted IPI (model 2; “aaIPI model”), followed by number of extranodal sites (ENS) mimicking the actual IPI [model 3, “IPI model” (age already included in model 1)], and lastly the HIV-score (model 4, ARL-IPI). We assessed the models in the validation set and found that the aaIPI was significantly better at predicting OS than the basic model alone (LR-χ2 7.10; P=0.023), while further adding ENS did not improve the model’s fit (Table 3). However, OS was most accurately predicted by adding the HIV-score to the aaIPI and ENS resulting in the ARL-IPI model, (LR-χ2 15.36; P<0.001). Although the ARL-IPI as a continuous variable predicted PFS and CR, and was associated with a significantly higher risk of progression and lack of CR in the high risk group (score >10), we failed to demonstrate that the HIV score provided additional prognostic value on CR rate or PFS after adjusting for the aaIPI (data not shown). Thus we could not conclude that the ARL-IPI predicted CR rate or PFS better than the aaIPI.
Table 3.
Comparison of the prognostic models.
Comparison between ARL-IPI and aaIPI
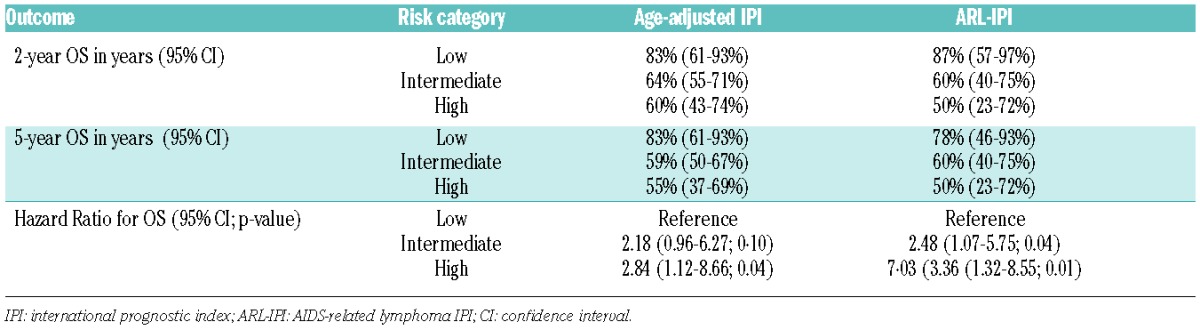
The newly composed ARL-IPI was applied to the validation set. We created three risk groups similarly to the aaIPI: low (LR; score 0–6), intermediate (IR; score 7–10) and high risk (HR; score 11–15). Distribution of these groups is described in Online Supplementary Table 3S. The IR group was not further subdivided into low-intermediate and high-intermediate risk because of low numbers. We then examined the difference in OS for the three risk groups. When we compared the prognostic value of the ARL-IPI with that of the aaIPI (LR=0; IR=1 or 2; HR=3) by predicting OS across the three risk groups, we found that the ARL-IPI was significantly more accurate in differentiating risk of death (Table 3 and Figure 2). OS rates differed significantly between the risk groups with an estimated 5-year OS of 78% for the LR group, 60% for the IR group, and 50% for the HR group (Table 4). In addition, the ARL-IPI identified more patients (28%) as LR (IR 52%; HR 20%), while the aaIPI identified most patients as IR (69%) and only 11% as LR (HR 20%). Moreover, the Dxy between ARL-IPI and OS was 0.40 (95%CI: 0.26–0.54) while only 0.24 (95%CI: 0.16–0.34) for the age-adjusted IPI. The Dxy is a concordance coefficient varying between −1 and +1, with 0 representing no predictive power and 1 perfect concordance of ascribed risk and survival.14
Figure 2.
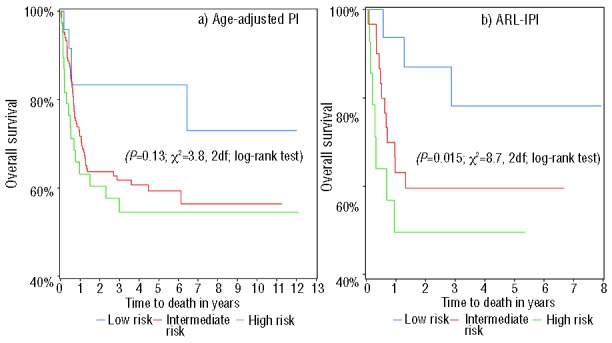
Kaplan-Meier overall survival curves for validation sample according to the prognostic indices a) aaIPI and b) ARL-IPI. IPI: international prognostic index; ARL-IPI: AIDS-related lymphoma IPI.
Table 4.
Overall survival as per risk category for the age-adjusted IPI and the ARL-IPI in the validation set (n=251).
Discussion
Not only patient- and lymphoma-related characteristics, but also HIV-associated factors have been demonstrated to have prognostic significance in patients with ARL.3,4,15,16 Composite scores that involve HIV-specific factors in addition to the commonly used prognostic indices for immunocompetent patients with NHL (IPI or aaIPI) have been developed to predict outcomes in HIV-positive patients with ARL.4,17 However, these prognostic indices: i) were developed for patients treated exclusively with non-rituximab containing chemotherapeutic regimens in the early era of cART; ii) can be cumbersome to calculate; and iii) have not been adopted in clinical practice. The aim of this study was to develop a user-friendly score that incorporates readily available information to better discriminate survival for patients with ARL treated in the current era. We found that the newly developed ARL-IPI was able to more accurately predict OS and better discriminate risk groups compared to the aaIPI, especially for low-risk patients.
The ARL-IPI consists of three components: aaIPI, number of involved extranodal sites, and an HIV score that incorporates base-line CD4 count, VL and prior history of AIDS. We incorporated the aaIPI rather than the IPI in the ARL-IPI as the median age for patients with ARL ranges between 37–42 years11,17 and age was not significantly associated with OS in our dataset. In addition, we included the actual number of involved extranodal sites (ENS) rather than extranodal involvement per the IPI (extranodal sites ≤1 vs. >1) as the association with OS was stronger for ENS compared to ENS ≤1 versus >1.
Although in our data set each of the three examined HIV-specific factors were not individually associated with OS, the composite HIV score was associated with an increased risk of death (HR 1.32; 95%CI: 1.05–1.67; P=0.02). Other studies also describe conflicting results with regards to the prognostic importance of HIV-associated factors on outcomes in the cART era. The Collaboration of Observational HIV Epidemiological Research Europe (COHERE) study group found that for patients with ARL diagnosed between 1998 and 2006, a low CD4 count at diagnosis was an independent risk factors for death.16 Similarly, Bower et al.4 observed that low base-line CD4 count was prognostic for survival in both the pre-cART and cART era, while a prior history of AIDS was associated with worse survival only in the pre-cART era. On the other hand, Lim and colleagues,3,18 as well as a review of the Spanish Grupo de Estudio del SIDA (GESIDA) registry,5 noted that only patient- and lymphoma-related, but not HIV-related factors remained predictive of poor outcome in the cART era. Levels of measurable HIV-RNA viral load and its impact on outcomes in ARL have not been studied systematically. While some studies are indicative of worse outcomes with high HIV-viral levels,19,20 others found no such associations.21,22 Because of differences in the lowest detection limit of HIV viral load assays between studies, we most likely grouped patients with truly undetectable HIV viral load levels with patients who had persistent very low-level viremia (<400 copies/mL). The ability to separate patients with absent viral replication from patients with ongoing HIV replication might have allowed us to even more accurately define prognosis. Nevertheless, our findings suggest that a single measure, such as CD4 count, VL or prior AIDS alone, might not be sufficient to adequately describe the immune deficit caused by the HIV in patients with lymphoma. A more comprehensive assessment such as the HIV score might be better able to capture the HIV-related impact on the immune system.
The IPI categorizes patients treated in the rituximab era into four prognostic groups based on risk factors present: low (0–1 risk factors; 3-year OS 91%), low-intermediate (2; 3-year OS 81%), high-intermediate (3; 3-year OS 65%) and high risk (4–5; 3-year OS 59%). In our dataset, we collapsed the low-intermediate and high-intermediate risk groups into one category because of low numbers. The 2-year OS for each risk group as defined by the ARL-IPI in our dataset are comparable to the outcomes for immunocompetent patients with aggressive B-cell NHL treated with R-CHOP. This confirms the observation of other studies that outcomes for patients with ARL in the cART era are approaching those for HIV-negative patients.23 Although the ARL-IPI did not perform better than the aaIPI in predicting CR rate and PFS, it more accurately predicted OS. This inability to better discriminate response and progression might be routed in inadequate statistical power secondary to the relatively small sample size. Alternatively, survival in HIV-positive patients is not only determined by adequate lymphoma control, but also by HIV-related risk factors for death. Therefore, survival might be more impacted by HIV factors than the lymphoma-related outcomes.
While we acknowledge that at the moment, the ARL-IPI by itself has limited utility in informing treatment decisions, the same can be said for the aaIPI. Nevertheless, high HIV scores as defined in our study might give an enhanced measure of immune function in HIV-positive patients. This could allow a choice to be made between potentially equivalent more or less intensive treatment options in some patients (e.g. dose-adjusted EPOCH vs. CODOX/M-IVAC in BL); this approach must be explored prospectively.
There are several strengths in our analysis, including the large sample size, inclusion of patients receiving state-of-the art lymphoma and HIV care, and the use of independent training and validation sets. A limitation of our analysis is the heterogeneity of the patients who had different histologies and were treated with different regimens. Additionally there might have been differences in definitions of extranodal involvement and prior history of AIDS between the included studies. The lack of centralized histological review is another weakness. Also, we used imputations for heavily missing data, which in turn might have impacted the precision of our estimates. While the IPI was originally developed in patients with aggressive NHL, its application has been primarily studied in patients with DLBCL. In our analysis, we found that there was no difference in outcomes for patients with DLBCL and BL/BLL, the two most common forms of ARL, which compromised 97% of all patients in our analysis. Stebbing et al. found also no impact of histological subtype on outcomes for patients with ARL in the cART era,24 while Lim and colleagues observed worse outcomes for patients with BL than DLBCL if treated with the CHOP-like regimens.18 Outcomes for patients with BL treated with CHOP are poor.25 In our dataset, the majority of patients with Burkitt histology were treated either with intensive multi-agent regimens (n=73, 58%)7,26,27 or infusional EPOCH (n=22, 18%),28,29 both of which are considered highly active for BL. Therefore, it appears appropriate to apply the ARL-IPI to any subtype of ARL as long as the lymphoma is being treated with an adequate regimen. It has to be noted that many patients included in this analysis have been treated between 1998 and 2003 and cART has changed dramatically since this period. This might have impacted our results and the score deserves further validation in the current era.
In conclusion, we propose a new prognostic index for patients with ARL, who are treated in the current era with rituximab-containing chemoimmunotherapy. The score uses readily available clinical information and can be easily applied to any patient with newly diagnosed ARL irrespective of histological subtype to prognosticate OS. Furthermore, the HIV score could become a promising tool to assess HIV-related immunodeficiency in patients undergoing cancer treatment and can be used to stratify patients for clinical trials in the future. It is worthy of note and encouraging that survival for patients with ARL in the current era is approximately that of HIV-negative patients.
Footnotes
Funding
The authors would like to thank the AIDS Malignancy Consortium (AMC; grant UO1CA121947), the Paul Calabresi Career Development Award for Clinical Oncology (K12CA132783-03 Grant), The ASCO Cancer Foundation 2010 Young Investigator Award, grant RD12/0036/0029 from RTICC, Instituto de Salud Carlos III, Spain, and by the CTSA Grants UL1 RR025750 and KL2 RR025749 and TL1 RR025748 from the National Center for Research Resources (NCRR), a component of the National Institutes of Health (NIH), and NIH roadmap for Medical Research, for their support.
Authorship and Disclosures
Information on authorship, contributions, and financial & other disclosures was provided by the authors and is available with the online version of this article at www.haematologica.org.
References
- 1.A Predictive Model for Aggressive Non-Hodgkin’s Lymphoma. N Engl J Med. 1993;329(14):987–94. [DOI] [PubMed] [Google Scholar]
- 2.Ziepert M, Hasenclever D, Kuhnt E, Glass B, Schmitz N, Pfreundschuh M, et al. Standard International Prognostic Index Remains a Valid Predictor of Outcome for Patients With Aggressive CD20+ B-Cell Lymphoma in the Rituximab Era. J Clin Oncol. 2010;28(14):2373–80. [DOI] [PubMed] [Google Scholar]
- 3.Lim ST, Karim R, Tulpule A, Nathwani BN, Levine AM. Prognostic factors in HIV-related diffuse large-cell lymphoma: before versus after highly active antiretroviral therapy. J Clin Oncol. 2005;23(33):8477–82. [DOI] [PubMed] [Google Scholar]
- 4.Bower M, Gazzard B, Mandalia S, Newsom-Davis T, Thirlwell C, Dhillon T, et al. A Prognostic Index for Systemic AIDS-Related Non-Hodgkin Lymphoma Treated in the Era of Highly Active Antiretroviral Therapy. Ann Intern Med. 2005;143(4):265–73. [DOI] [PubMed] [Google Scholar]
- 5.Miralles P, Berenguer J, Ribera JM, Rubio R, Mahillo B, Tellez MJ, et al. Prognosis of AIDS-Related Systemic Non-Hodgkin Lymphoma Treated With Chemotherapy and Highly Active Antiretroviral Therapy Depends Exclusively on Tumor-Related Factors. J Acquir Immune Defic Syndr. 2007;44(2):167–73 [DOI] [PubMed] [Google Scholar]
- 6.Navarro JT, Ribera JM, Oriol A, Vaquero M, Romeu J, Batlle M, et al. International prognostic index is the best prognostic factor for survival in patients with AIDS-related non-Hodgkin’s lymphoma treated with CHOP. A multivariate study of 46 patients. Haematologica. 1998;83(6):508–13. [PubMed] [Google Scholar]
- 7.Oriol A, Ribera J, Brunet S, del Potro E, Abella E, Esteve J. Highly active antiretroviral therapy and outcome of AIDS-related Burkitt’s lymphoma or leukemia. Results of the PETHEMA-LAL3/97 study. Haematologica. 2005;90(7):990–2. [PubMed] [Google Scholar]
- 8.Montoto S, Wilson J, Shaw K, Heath M, Wilson A, McNamara C, et al. Excellent immunological recovery following CODOX-M/IVAC, an effective intensive chemotherapy for HIV-associated Burkitt’s lymphoma. AIDS. 2010;24(6):851–6. [DOI] [PubMed] [Google Scholar]
- 9.Dunleavy K, Pittaluga S, Shovlin M, Steinberg SM, Cole D, Grant C, et al. Low-Intensity Therapy in Adults with Burkitt’s Lymphoma. N Engl J Med. 2013;369(20):1915–25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Noy A, Kaplan L, Lee JY. A Modified Dose Intensive R- CODOX-M/IVAC For HIV-Associated Burkitt and Atypical Burkitt Lymphoma(BL) Demonstrates High Cure Rates and Low Toxicity: Prospective Multicenter Phase II Trial Of The AIDS Malignancy Consortium (AMC 048). Blood. 2013;122(21):639. [Google Scholar]
- 11.Kaplan LD, Lee JY, Ambinder RF, Sparano JA, Cesarman E, Chadburn A, et al. Rituximab does not improve clinical outcome in a randomized phase 3 trial of CHOP with or without rituximab in patients with HIV-associated non-Hodgkin lymphoma: AIDS-Malignancies Consortium Trial 010. Blood. 2005; 106(5):1538–43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Barta SK, Xue X, Wang D, Tamari R, Lee JY, Mounier N, et al. Treatment factors affecting outcomes in HIV-associated non-Hodgkin lymphomas: a pooled analysis of 1546 patients. Blood. 2013;122(19):3251–62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Aberg JA, Kaplan JE, Libman H, Emmanuel P, Anderson JR, Stone VE, et al. Primary Care Guidelines for the Management of Persons Infected with Human Immunodeficiency Virus: 2009 Update by the HIV Medicine Association of the Infectious Diseases Society of America. Clin Infec Dis. 2009;49(5):651–81. [DOI] [PubMed] [Google Scholar]
- 14.Harrell FE, Jr, Lee KL, Mark DB. Multivariable prognostic models: issues in developing models, evaluating assumptions and adequacy, and measuring and reducing errors. Stat Med. 1996;15(4):361–87. [DOI] [PubMed] [Google Scholar]
- 15.Simcock M, Blasko M, Karrer U, Bertisch B, Pless M, Blumer L, et al. Treatment and prognosis of AIDS-related lymphoma in the era of highly active antiretroviral therapy: findings from the Swiss HIV Cohort Study. Antivir Ther. 2007;12(6):931–9. [PubMed] [Google Scholar]
- 16.Bohlius J, Schmidlin K, Costagliola D, Fatkenheuer G, May M, Caro Murillo AM, et al. Prognosis of HIV-associated non-Hodgkin lymphoma in patients starting combination antiretroviral therapy. AIDS. 2009;23(15):2029–37. [DOI] [PubMed] [Google Scholar]
- 17.Mounier N, Spina M, Gabarre J, Raphael M, Rizzardini G, Golfier JB, et al. AIDS-related non-Hodgkin lymphoma: final analysis of 485 patients treated with risk-adapted intensive chemotherapy.[see comment]. Blood. 2006;107(10):3832–40. [DOI] [PubMed] [Google Scholar]
- 18.Lim ST, Karim R, Nathwani BN, Tulpule A, Espina B, Levine AM. AIDS-related Burkitt’s lymphoma versus diffuse large-cell lymphoma in the pre-highly active antiretroviral therapy (HAART) and HAART eras: significant differences in survival with standard chemotherapy. J Clin Oncol. 2005;23(19):4430–8. [DOI] [PubMed] [Google Scholar]
- 19.Bortolin MT, Zanussi S, Talamini R, Simonelli C, Pratesi C, Tedeschi R, et al. Predictive value of HIV type 1 DNA levels on overall survival in HIV-related lymphoma Patients treated with high-dose chemotherapy (HDC) plus autologous stem cell transplantation (ASCT). AIDS Res Hum Retroviruses. 2010;26(2):245–51. [DOI] [PubMed] [Google Scholar]
- 20.Long JL, Engels EA, Moore RD, Gebo KA. Incidence and outcomes of malignancy in the HAART era in an urban cohort of HIV-infected individuals. AIDS. 2008;22(4): 489–96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Tedeschi R, Bortolin MT, Bidoli E, Zanussi S, Pratesi C, Vaccher E, et al. Assessment of immunovirological features in HIV related non-Hodgkin lymphoma patients and their impact on outcome. Journal of Clinical Virology. 2012;53(4):297–301. [DOI] [PubMed] [Google Scholar]
- 22.Levine AM, Noy A, Lee JY, Tam W, Ramos JC, Henry DH, et al. Pegylated Liposomal Doxorubicin, Rituximab, Cyclophosphamide, Vincristine, and Prednisone in AIDS-Related Lymphoma: AIDS Malignancy Consortium Study 047. J Clin Oncol. 2013;31(1):58–64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Oriol A, Ribera J, Esteve J, Sanz M, Brunet S, Garcia-Boyero R, et al. Lack of influence of human immunodeficiency virus infection status in the response to therapy and survival of adult patients with mature B-cell lymphoma or leukemia. Results of the PETHEMA-LAL3/97 study. Haematologica. 2003;88(4):445–53. [PubMed] [Google Scholar]
- 24.Stebbing J, Mandalia S, Palmieri C, Nelson M, Gazzard B, Bower M. Burkitt’s Lymphoma and Previous AIDS-Defining Illnesses Are Not Prognostic Factors in AIDS-Related Non-Hodgkin’s Lymphoma. J Clin Oncol. 2005;23(33):8538–40. [DOI] [PubMed] [Google Scholar]
- 25.Aldoss IT, Weisenburger DD, Fu K, Chan WC, Vose JM, Bierman PJ, et al. Adult Burkitt lymphoma: advances in diagnosis and treatment. Oncology (Williston Park, NY). 2008;22(13):1508–17. [PubMed] [Google Scholar]
- 26.Ribera JM, Garcia O, Grande C, Esteve J, Oriol A, Bergua J, et al. Dose-Intensive Chemotherapy Including Rituximab in Burkitt’s Leukemia or Lymphoma Regardless of Human Immunodeficiency Virus Infection Status Final Results of a Phase 2 Study (Burkimab). Cancer. 2013; 119(9):1660–8. [DOI] [PubMed] [Google Scholar]
- 27.Xicoy B, Ribera JM, Muller M, Garcia O, Hoffmann C, Oriol A, et al. Dose-intensive chemotherapy including rituximab is highly effective but toxic in human immunodeficiency virus-infected patients with Burkitt lymphoma/leukemia: parallel study of 81 patients. Leuk Lymphoma. 2014. February 25 [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 28.Dunleavy K, Little RF, Pittaluga S, Grant N, Wayne AS, Carrasquillo JA, et al. The role of tumor histogenesis, FDG-PET, and short-course EPOCH with dose-dense rituximab (SC-EPOCH-RR) in HIV-associated diffuse large B-cell lymphoma. Blood. 2010; 115(15):3017–24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Sparano JA, Lee JY, Kaplan LD, Levine AM, Ramos JC, Ambinder RF, et al. Rituximab plus concurrent infusional EPOCH chemotherapy is highly effective in HIV-associated B-cell non-Hodgkin lymphoma. Blood. 2010;115(15):3008–16. [DOI] [PMC free article] [PubMed] [Google Scholar]