

Abstract
The purpose of this study was to find the effect of endurance training and thiamine supplementation on anti-fatigue during the exercise. Each nine students from K Women’s University went through three cross-over treatments: placebo treatment, training treatment and thiamine treatment. Training treatment was performed with bicycle ergometer exercise for four weeks (five days per week). Each exercise was performed for an hour with intensity set at 70% (50rpm) of maximal oxygen uptake. Thiamine treatment group was given 10mg of thiamine tetrahydrofurfuryl disulfide per one kilogram for four weeks. The bicycle ergometer exercise was performed at 70% of maximal oxygen uptake in exercise intensity which 60 minutes of exercise was performed at 50rpm . Lactate concentration was significantly decreased during 15 to 30 minutes of exercise for those with training treatment and 15 to 60 minutes of exercise for those with thiamine treatment compared to placebo treatment group. Ammonia concentration was significantly decreased during 15 to 60 minutes of exercise and 15 to 30 minutes of recovery for those with training and thiamine treatment compared to placebo treatment. Resting blood thiamine concentrations of placebo treatment were significantly lower than training treatment. 60 minutes after the exercise, plasma thiamine concentration was significantly increased in all treatment group. To sum up the previous, thiamine intake during exercise positively benefits carbohydrate metabolism in a way that will decrease lactate concentration, ammonia concentration, and anti- fatigue by reducing the RPE. Therefore, we can consider thiamine intake to be utilized as similar benefits as endurance training.
Keywords: thiamine, endurance training, anti-fatigue, energy substrate, 5-HT
INTRODUCTION
Vitamin adjusts the energy metabolism in physical activities and is widely used as a dietary supplements to enhance exercise performance. [1-3]. Among vitamins, thiamine is an coenzyme of the pyruvate dehydrogenase (PDH) which stimulates the conversion from the pyruvate to the acetyl CoA and plays an important role in carbohydrate metabolism. It also plays a role as a coenzyme of the branched-chain decarboxylase which reacts to the physiochemical reaction of the oxoglutarate dehydrogenase and the branched-chain amino acids in the formation of succinyl CoA in the TCA cycle [4]. Decreasing the thiamine in the cell degrades enzyme activation, decreases ATP biosynthesis and causes fatigue [5]. Such a low level of thiamine in the body may degrade the exercise performance. Thiamine tetrahydrofurfuryl disulfide (TTFD), lipid-soluble thiamine, is effectively absorbed from various organs compared to the water-soluble thiamine, thiamine hydrochloride (THCL) which limits the absorption, converted to thiamine in the cytoplasm and to the phosphate ester [6-8]. A daily recommended dose of thiamine is 0.5mg/1000Kcal for a healthy adult. Therefore, thiamine may be sufficiently taken; otherwise, the energy intake would be limited or refined food would be taken too much in daily life [9]. However, it is reported that thiamine request may increase by stimulating the metabolic pathway using thiamine under continuous exercise [4]. Kaiserauer et al. [10] report that the thiamine level is low for an athlete under intensive training. Guilland et al. [11] report that vitamin deficiency in sedentary is restored to the normal range, but it is not effective for athletes after supplementing multivitamin with thiamine. Hasegawa et al. [12] propose that thiamine and riboflavin intake increase for athletes during the season compared to the off-season. Such result suggests that the athletes under continuous training may experience thiamine insufficiency. Also, if a person takes vitamin B (B1, B2, B6), vitamin C and other vitamins less than one third of the recommended daily requirements, it is observed that the maximum oxygen uptake and the lactate threshold significantly decrease within 4 weeks, causing problems in the exercise performance through vitamine deficency [13]. Van der Beek et al. [14] report that the maximum oxygen uptake decreases by about 11.6% and the lactate accumulation increases by 7% as a result of deficiencies in thiamine, riboflavin and vitamin B6 for 24 healthy male adults for more than 11 weeks. Also, Fogelholm et al. [15] announce that the erythrocyte activation coefficient significantly increases as a result of supplementing multivitamin for 42 active university students with low levels of thiamine, riboflavin and vitamin B6 for 5 weeks. However, such result is from the study involving the vitamin B complex, and for this reason it is hard to say that the effect is from thiamine alone, which calls for a study involving single intake of thiamine. Up to now, it is observed that the single supplementation of thiamine decreases fatigue in seniors and manual workers [16,17] and prolongs the duration of swimming time until exhaustion while decreasing the lactate threshold and lactate concentration [18-20]. However, Doyle et al. [21] and Webster [22] propose that the TTFD intake does not affect exercise performance. Studies observing the effect of single administration of thiamine do not reach a clear conclusion and the one week supplementation period is too short requiring investigation on the effect on long-term supplementation. Meanwhile, it is reported that regular exercise increases the PDH activation in the model exposed to diabetes and improves carbohydrate metabolism [23]. It is observed that much supplement of thiamine is effective in improving diabetic complication [24-30]; it is also confirmed that the result is related to the PDH activation, as thiamine supplementation increases the PDH activation [31]. Therefore, the thiamine supplementation suggests that it would activate PDH at the same level of regular exercise, and it is required to verify how thiamine supplementation affects healthy person.
Such results show that thiamine supplementation may prevent fatigue and increase the exercise performance, but there are insufficient studies in Korea on the effect of exercise on fatigue after taking thiamine for a long time . Also, whether the thiamine supplementation is utilized as an effective administration in improving the carbohydrate metabolism similar to endurance training needs to be verified. Therefore, this study was to observe the effect of endurance training and thiamine supplementation on anti-fatigue during exercise.
METHODS AND MATERIALS
Subjects
The subjects of the study are 9 female university students in the department of physical education with a career in athletics or Taekwondo. They had never taken drugs or nutritional supplements for 6 months before the experiment and their health condition is good. The placebo treatment, endurance training treatment and thiamine treatment are administered for the same subjects. Each treatment is applied for 4 weeks and the repetitive measurement experiment was designed to offset the effect of the previous treatment by setting up a week interval among the treatment to observe the changes in dietary supplements and exercise administration, while the treatment order offsets the error from the administration order by applying random assignment method. The physical characteristics in the subjects are shown in Table 1.
Table 1.
Characteristics of subjects
| Variables | mean ±SD (n = 9) |
|---|---|
| Age(yr) | 20.67±0.71 |
| Height(cm) | 163.19±4.67 |
| Body Weight(kg) | 57.34±5.36 |
| VO2max(mL/kg/min) | 38.36±1.92 |
| Career(yr) | 4.89±2.42 |
The endurance training and thiamine treatment method
The endurance training is performed for 4 weeks using the bicycle ergometer. The exercise intensity is configured to 70% of the maximum oxygen uptake achieved from the gradual maximum exercise load test. The exercise is performed 5 times a week with 1 hour and 20 minutes of warm-up and cool-down and 40 minutes of main exercise. All the subjects perform the bicycle exercise at the same time. Thiamine (thiamine tetrahydrofurfuryl disulfide: TTFD, Ecological Concord, Calif., USA) is administered for 4 weeks with 10mg per weight for 3 times 30 minutes after a meal with 150ml of water. During the experiment, the nutritionist trains the dietary and intake method such that they do not be insufficient in protein, vitamin, mineral and iron for every 3 weeks based on the dietary habits of each subject, and the subjects are guided not to skip meals.
Exercise loading test
The subjects keep their fasting for more than 12 hours prior to the experiment and take their regular meal 2 hours before the main exercise starts on the day of the experiment. The exercise is for 60 minutes at 50rpm with 70% of the maximum oxygen uptake using the bicycle ergometer. After the exercise for 60 minutes, the cool-down is performed for 5 minutes at 0.5KP and the subjects take a rest for 30 minutes. The rating of perceived exertion is measured every 5 minutes of exercise with 70% of the maximum oxygen uptake using the Borg's scale [32]. Fig. 1 shows the exercise procedure for the experiment.
Fig. 1.
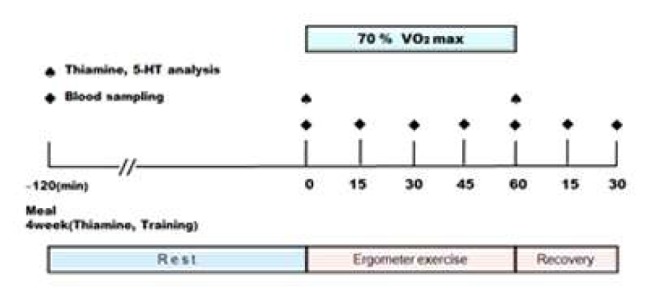
Experimental design
Blood collecting and analysis
Blood collecting is performed 7 times with 10ml each using the catheter installed in the antecubital vein 2 hours before the experiment, right before the exercise, at 15 minute interval during 1 hour of exercise, after 5 minutes of cool-down and 15 and 30 minutes during the recovery periods. To verify the thiamine treatment and the endurance training, glucose, lactate, ammonia, free fatty acid, insulin and glucagon are analyzed. Thiamine and 5-HT are observed from the blood right before and after the exercise. The blood is analyzed by Korea Green Cross Corporation.
Data analysis
The two-way repeated ANOVA is applied to glucose, lactate, ammonia, free fatty acid, insulin, glucagon, thiamine, 5-HT and the rating of perceived exertion to verify the interaction between the exercise initiation timing and the treatment method (endurance training, thiamine treatment, placebo treatment) The one-way repeated ANOVA and the least significant difference (LSD) are applied to verify the difference between dependent factors for each exercise as post-hoc comparison. Also, a dependent t-test is performed to verify the difference between the rest and right after the exercise for the treatment with thiamine and 5-HT. All the data in the study are expressed by the average and the standard deviation and the significant level is below 0.05.
RESULTS
The changes of glucose, lactate, ammonia, free fatty acid, glucacon, insulin during the bicycle ergometer exercise and recovery
The analysis result of applying the two-way repeated ANOVA to analyze the changes in glucose during exercise among 3 treatment methods, as shown in Table 2, shows no significant interaction between the treatment method and the exercise initiation; and significant effects are discovered depending on the treatment method and the exercise initiation. The result of applying the one-way repeated ANOVA to analyze the glocuse difference among 3 treatment methods and the LSD show that the training treatment is significantly lower than the placebo treatment after 15 and 30 minutes of the exercise (p < 0.05) and" the thiamine treatment is significantly lower than the placebo treatment(p,0.05) at 15 and 60 minutes after the exercise and 30 minutes during the recovery"; and in particular, the thiamine treatment at 30 minutes of the recovery is significantly lower than the training treatment (p < 0.05). The analysis result of applying the two-way repeated ANOVA to analyze the changes in the lactate during exercise among 3 treatment methods, as shown in Table 2, shows that significant effects are discovered depending on the treatment method and the exercise initiation. The result of applying the one-way repeated ANOVA to analyze the lactate difference among 3 treatment methods and the LSD show that the training treatment is significantly lower than the placebo treatment after 15, 45 and 60 minutes of the exercise (p < 0.05) and the thiamine treatment is lower than the placebo treatment from 15 minutes to each one of the recovery periods (p < 0.05), and in particular, the thiamine treatment at 60 minutes of the recovery is significantly lower than the training treatment (p < 0.05). The analysis result of applying the two-way repeated ANOVA to analyze the changes in ammonia during the exercise among 3 treatment methods, as shown in Table 2, shows that significant effects are discovered depending on the treatment method and the exercise initiation. The result of applying the one-way repeated ANOVA to analyze the ammonia difference among 3 treatment methods and the LSD show that the training treatment is significantly lower than the placebo treatment from 15 minutes to each one of the recovery points of the exercise (p < 0.05) and the thiamine treatment is significantly lower than the training treatment before 120 minutes to the exercise and at the exercise initiation (p < 0.05); and in particular, the thiamine treatment from 15 minutes to all the recovery points is significantly lower than the training treatment (p < 0.05). In particular, the thiamine treatment at 15 and 30 minutes of the recovery is significantly lower than the training treatment (p < 0.05). The analysis result of applying the two-way repeated ANOVA to analyze the changes in free fatty acid during exercise among 3 treatment methods, as shown in Table 2, shows no significant interaction between the treatment method and the exercise initiation; and significant effect is discovered depending on the exercise time (p < 0.05). The result of applying the one-way repeated ANOVA to analyze the FFA difference among 3 treatment methods and the LSD shows that the training treatment is significantly higher than the placebo treatment at the exercise initiation (p < 0.05) and significantly lower than the placebo treatment (p < 0.05). The thiamine treatment is significantly lower than the training treatment at the exercise initiation, 15 and 60 minutes after the exercise. The analysis result of applying the two-way repeated ANOVA to verify the changes in glucagon during exercise among 3 treatment methods, as shown in Table 2, shows no significant interaction between the treatment method and the exercise initiation; and significant effects are discovered depending on the treatment method and exercise initiation. The result of applying the one-way repeated ANOVA to analyze the glucagon difference among 3 treatment methods and the LSD shows that the training treatment is significantly lower than the placebo treatment 120 minutes before the exercise, exercise initiation, 30 minutes in the exercise and 30 minutes at the recovery of the exercise (p < 0.05) and the thiamine treatment before 120 minutes and the exercise initiation than the placebo treatment (p < 0.05); in particular, the thiamine treatment from the exercise initiation to 30 minutes and 30 minutes of the recovery is significantly lower than the training treatment (p < 0.05). The analysis result of applying the two-way repeated ANOVA to analyze the changes in insulin during exercise among 3 treatment methods, as shown in Table 2, shows that significant effects are discovered depending on the treatment method and the exercise initiation. The result of applying the one-way repeated ANOVA to analyze the insulin difference among 3 treatment methods and the LSD shows that the training treatment is significantly lower than the placebo treatment from the exercise initiation to 30 minutes of the exercise.
Table 2.
The changes of glucose, lactate, ammonia, free fatty acid, glucagon, insulin during the bicycle ergometer exercise and recovery
| Variables | treatment | -120 | 0 | 15 | 30 | 45 | 60 | rec.15 | rec.30 | F-value |
|---|---|---|---|---|---|---|---|---|---|---|
| Glucose (mg/dL) | placebo | 77.20±7.24 | 74.99±11.21 | 71.90±5.26 | 74.10±7.61 | 78.19±9.25 | 83.29±13.84 | 83.96±9.11 | 79.18±8.90 | treat 11.812* |
| training | 73.38±8.46 | 70.70±11.65 | 66.70±5.44a | 66.76±8.19a | 73.96±8.20 | 76.06±7.81 | 79.61±15.87 | 79.41±11.24 | time 5.030* | |
| thiamine | 77.61±5.01 | 74.24±13.22 | 67.36±3.51a | 69.08±7.88a | 73.12i9.56a | 76.26±13.51a | 77.83±12.05 | 75.02±8.99ab | treat×time 0.846 | |
| Lactate (mmoL/L) | placebo | 0.67±.40 | 1.03±.20 | 3.54±.91 | 4.04±1.20 | 4.09±1.34 | 4.05±1.66 | 2.39±1.14 | 1.78±.89 | treat 17.096* |
| training | 0.56±.17 | 1.01±.31 | 2.89±.85a | 3.48±.73 | 3.12±1.11a | 3.17±1.13a | 1.55±.56a | 1.38±.70 | time 59.042* | |
| thiamine | 0.56±.14 | 0.97±.14 | 2.87±.89a | 2.89i1.26a | 2.53i1.10a | 2.25±.95ab | 1.25±.56a | 1.10±.45a | treat×time 6.620* | |
| Ammonia (μg/dL) | placebo | 45.44±27.12 | 51.33±18.99 | 107.33±18.87 | 128.33±21.94 | 140.67±22.87 | 139.36±20.35 | 75.33±7.28 | 66.78±15.22 | treat 18.594* |
| training | 59.56±17.07 | 61.56±15.57 | 92.22±15.67a | 107.11i20.29a | 111.78i21.22a | 118.44±19.43a | 61.56±15.50a | 54.56±16.17a | time 97.796* | |
| thiamine | 44.33±20.89b | 42.78±18.48b | 83.44±28.76a | 101.89i26.75a | 107.44i26.95a | 113.67i 26.06a | 46.75±10.85ab | 37.90±8.82ab | treat×time 2.990* | |
| FFA (μEq/L) | placebo | 395.00±138.26 | 115.44±37.49 | 134.44±53.69 | 353.44±140.91 | 444.78±155.31 | 555.89±181.60 | 737.56±183.23 | 584.33±197.32 | treat 0.329 |
| training | 462.22±163.39 | 152.56±34.96a | 166.60±26.64 | 288.78±100.65 | 324.44±82.54 | 390.78± 122.99a | 758.33±273.36 | 557.33±231.42 | time 80.481* | |
| thiamine | 428.29±136.83 | 121.56±22.65b | 132.44±35.70b | 295.11±164.22 | 391.44±156.66 | 530.67±185.92b | 792.89±231.98 | 675.78±261.02 | treat×time 1.585 | |
| Glucagon (pg/mL) | placebo | 59.82±6.99 | 69.14±9.95 | 79.78±6.96 | 85.13±6.49 | 85.99±8.53 | 89.23±19.73 | 80.95±7.68 | 74.62±10.18 | treat 28.023* |
| training | 50.30±11.89a | 51.89±11.36a | 71.28±10.19 | 71.81i8.13a | 75.20±14.72 | 76.87±10.65 | 72.62±16.77 | 63.16±10.14a | time 27.497* | |
| thiamine | 62.16±12.13b | 82.08±8.83ab | 89.70±5.74ab | 95.74 i9.15ab | 94.96±14.36b | 101.02±15.82b | 85.48±10.24b | 88.18± 14.29ab | treat×time 1.453 | |
| Insulin (μIU/mL) | placebo | 8.44±2.26 | 38.48±15.31 | 18.60±14.15 | 9.72±6.10 | 6.25±3.66 | 5.63±3.73 | 19.76±11.96 | 13.32±6.49 | treat 0.958 |
| training | 7.43±1.97 | 24.83±11.77 | 9.73±4.24 | 6.48±1.78 | 5.65±1.82 | 4.60±2.10 | 18.39±12.25 | 18.76±15.08 | time 32.288* | |
| thiamine | 8.77±3.29 | 33.96±15.24 | 14.74±8.41 | 8.94±4.31 | 5.87±1.63 | 5.15±1.85 | 15.01±8.21 | 11.50±6.63 | treat×time 2.938* |
: indicates significant interaction or main effect(p < .05)
: indicates difference from treatment of placebo(p < .05)
: indicates difference from treatment of thiamine(p < .05)
treat : treatment
The changes of thiamine, 5-TH in pre and post the bicycle ergometer exercise
The analysis result of applying the two-way repeated ANOVA to verify the changes in thiamine during exercise among 3 treatment methods, as shown in Table 3, shows no significant interaction between the treatment method and the exercise initiation, and significant effects are discovered depending on the treatment method, before and after the exercise (p < 0.05). The dependent T-test is applied to verify the difference in thiamine before and after the exercise for each treatment shows that all 3 methods significantly increase both before and after the exercise (p < 0.05); and one-way repeated ANOVA and LSD application applied to verify the difference in thiamine for each treatment method before and after the exercise shows that the training treatment is significantly low before and after the training treatment compared to the placebo treatment (p < 0.05), and the thiamine treatment is significantly higher than the placebo and the training treatments before and after the exercise (Fig. 2).
Table 3.
The changes of thiamine, 5-HT in pre and post the bicycle ergometer exercise
| Variables | treatment | Pre | Post | F-value |
|---|---|---|---|---|
| Thiamine (nmol/L) | placebo | 130.99±13.69 | 158.89±32.43# | treat 1314.569* |
| training | 95.21±16.48a | 110.29±15.89a# | time 63.681* | |
| thiamine | 420.76±35.74ab | 458.88±20.68ab# | treat×time 1.575 | |
| 5-HT (ng/mL) | placebo | 107.38±24.50 | 114.11±21.57 | treat 17.203* |
| training | 156.72±51.93a | 169.34±33.81a# | time 32.178* | |
| thiamine | 151.61±56.24a | 217.57±76.67ab# | treat×time 10.551* |
: indicates significant interaction or main effect(p < .05)
: indicates difference from treatment of placebo(p < .05)
: indicates difference from treatment of thiamine(p < .05)
: indicates difference from pre test(p < .05)
treat : treatment
Fig. 2.
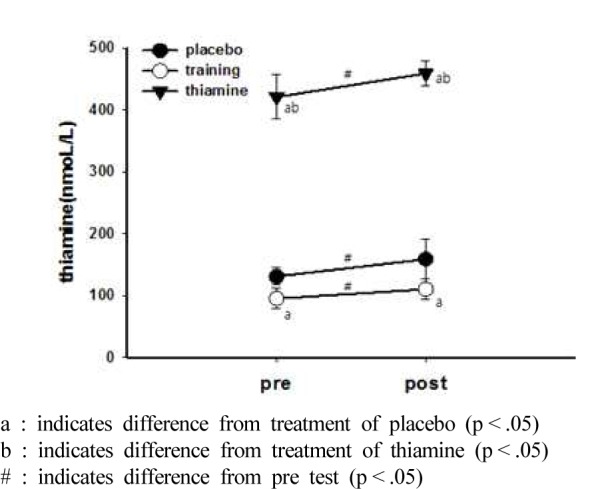
The change of thiamine
The analysis result of applying the two-way repeated ANOVA to analyze the changes in 5-HT during exercise among 3 treatment methods, as shown in Table 3, shows that significant effects are discovered depending on the treatment method and the exercise initiation (p < 0.05). A dependent T-test applied to verify the difference in 5-HT before and after the exercise for each treatment shows that significant increase (p < 0.05) is discovered in the training treatment and the thiamine treatment after the exercise, and the one-way repeated ANOVA and the LSD application applied to verify the difference in 5-HT for each treatment method before and after the exercise shows that the training treatment is significantly high before and after the training treatment compared to the placebo treatment (p < 0.05), and the thiamine treatment is significantly higher than the placebo and training treatments before and after the exercise. In particular, the thiamine treatment is significantly higher than the training treatment (p < 0.05) (Fig. 3).
Fig. 3.
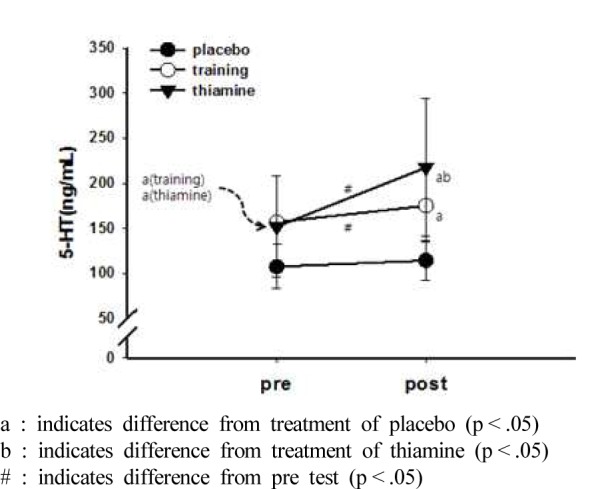
The change of 5-HT
The changes of RPE during the bicycle ergometer exercise
The analysis result of applying the two-way repeated ANOVA to analyze the changes in RPE during exercise among 3 treatment methods, as shown in Table 4, shows no significant interaction between the treatment method and the exercise initiation; and significant effects are discovered depending on the treatment method and the exercise initiation. The one-way repeated ANOVA and the LSD applied to verify the difference in RPE among 3 treatment methods for each exercise shows that the training treatment is significantly lower than the placebo treatment from 10 to 60 minutes after the exercise (p < 0.05) and the thiamine treatment is significantly lower than the placebo treatment for all the exercise periods (p < 0.05).
Table 4.
The changes of RPE during the bicycle ergometer exercise
| exercise time (min.) | treatment |
F-value | ||
|---|---|---|---|---|
| placebo | training | thiamine | ||
| 5 | 10.74±0.43 | 9.33±2.00 | 9.11±1.96a | |
| 10 | 11.67±1.12 | 10.22±2.11a | 10.11±2.03a | |
| 15 | 12.44±0.88 | 11.00±2.40a | 11.00±2.06a | |
| 20 | 12.78±1.20 | 11.11±2.20a | 11.11±2.09a | |
| 25 | 13.22±1.20 | ll.ll±1.96a | 11.33±1.80a | treat 18.160* |
| 30 | 13.56±1.42 | 11.56±1.94a | 11.67±1.73a | time 22.148* |
| 35 | 13.56±1.24 | 11.78±2.11a | 12.00±1.50a | |
| 40 | 13.67±1.58 | 12.00±1.32a | 12.33±1.94a | treat×time 1.000 |
| 45 | 14.56±2.13 | 12.44±1.51a | 12.44±2.01a | |
| 50 | 14.67±1.94 | 12.48±1.23a | 12.67±1.80a | |
| 55 | 15.45±1.33 | 13.11±2.42a | 12.67±2.00a | |
| 60 | 15.11±2.57 | 13.56±2.51a | 12.56±1.94a | |
: indicates significant interaction or main effect(p < .05)
: indicates difference from treatment of placebo(p < .05)
: indicates difference from treatment of thiamine(p < .05)
treat : treatment
DISCUSSION
The research result shows that the glucose concentration in the blood is significantly lower in the training treatment than in the placebo treatment at 15 and 30 minutes of the training; the thiamine treatment is significantly low from 15 to 60 minutes after the exercise. It is reported that free fatty acid concentration decreases with the increase in fat-oxidation during exercise with the same exercise intensity after regular training, resulting in the decrease of the carbohydrate-oxidation and saving the muscle glycogen [33-35]. The training treatment shows decrease in free fatty acid concentration from 30 minutes to 45 minutes after the exercise; it significantly decreases 60 minutes after the exercise. Therefore, it is considered that regular training decreases carbohydrate-oxidation and glucose in the training treatment. Also, thiamine supplementation activates PDH for the thiamine treatment [36,37], catalyzing pyruvate to acetyl CoA, increasing the movement to the skeletal muscles while decreasing glucose in the blood. Such result is the same as that of Choi [38] who report a significant decrease in glucose in the blood compared to the placebo treatment during exercise when thiamine is supplemented for a week to female university students majoring in physical education. It is considered that the lactate and ammonia accumulation during exercise increases hydrogen ions and acidosis in the muscles and is known as a major cause of muscular fatigue [39,40]. The lactate concentration in blood significantly decreases during exercise in the training treatment and the thiamine treatment in the present study. Such result is the same with the research by Philips et al. [41] who report decrease in lactate concentration during cycling exercise for a month with 60% of the maximum oxygen uptake for untrained man. Meanwhile, Park and Gubbler [42] observe that the lactate production decreases after taking thiamine, and Van der Beek et al. [14] report that the maximum oxygen uptake decreases and the lactate accumulation increases by 7% as a result of vitamin deficiency including thiamine for 11 weeks among healthy men. Also, the study by Knippel et al. [18] proposes that the lactate concentration decreases during exercise with the thiamine supplementation for cyclists, which is the same with the result of the present study. Such result is in accordance with a study which states that the PDH activation decreases the lactate accumulation [43,44] and the thiamine supplementation activates PDH [31,45]. Also, it is thought that the fatigue materials decrease by effective engagement of the training treatment and the thiamine treatment in the energy metabolism process of the ammonia concentration for the same result of the lactate concentration. Increasing the glucose use in the skeletal muscles during exercise causes the liver to supply the glucose required during exercise through glycogenolysis and gluconegenesis [46]. Increasing glucagon in the blood increases the glucose excretion from the liver and the glucose use in the muscles as a result [47]. It is reported that the endurance training increases the glucagon sensitivity in the liver [48,49] but the study shows that the training treatment shows no large changes compared to the placebo treatment. However, it is found that the glucagon concentration is significantly high compared to the treatments at 15 and 30 minutes of the exercise for the thiamine treatment. Such result is the same with the report by Choi [38] which observes the glucagon concentration increase during exercise after single supplementation of thiamine. Therefore, it is considered that glucagon increases to maintain the required demand for metabolism by effectively using the glucagon in the blood through the thiamine supplementation. The insulin decreases with the increase in the period of the endurance training [50] and the repetitive endurance training is reported to decrease the insulin concentration under the same exercise intensity [51]. The study shows that the insulin concentration gradually decreases regardless of the administered material at 60 minutes after the exercise but no difference among the treatment groups. The thiamine is absorbed by the small intestine, observed in the skeletal muscles, liver, heart, kidneys and brain with a high concentration, and a continuous supply is required with the limited storage in the tissues with half life of 10 to 20 days [52]. The plasma thiamine level for a healthy person is reported between 0.018 and 0.855μmol·mg-1 [53-55] and the thiamine level is within the normal range in the resting state of the subjects. Also, it is found that the thiamine level significantly increases for all treatment groups after 60 minutes of the exercise, metabolic requirement for glucose in the later part of the exercise and the thiamine concentration. The training treatment for 4 weeks significantly decreases the thiamine concentration in rest compared to the placebo treatment. Such result is the same with the study by Sato et al. [56] which observes the thiamine concentration decrease for the training of swimming athletes and by Kaiserauer et al. [10] who report that the thiamine concentration decreases for the training of athletes. Such result suggests that exogenous thiamine is required for continuous training. Soares [57] reports that the trained group shows higher serotonin concentration than the non-trained group during rest for the general public. It is proposed that the serotonin concentration increases in rest after the pilates treatment for 12 weeks [58]. The study also shows a significantly high concentration of serotonin during rest after 4 weeks of the bicycle ergometer training in the training treatment compared to the placebo treatment. It is reported that increasing serotonin in the brain after intensive exercise for a long time causes central fatigue [59] and the serotonin concentration increase in the brain is inhibited by continuous training [60]. However, Pitsiladis et al. [61] propose that the serotonin in the brain is not a predictor of the serotonin level in the central fatigue and brain; and it is established that the interpretation of serotonin in the blood has not reached a clear result. The present study shows significant increase in the serotonin concentration in the training and thiamine treatments compared to the placebo treatment after 60 minutes of the exercise. It is said that the serotonin increase in the brain during endurance exercise is caused by the tryptophan increase in the condition of high free fatty acid concentration in the blood [62]. The study shows low lactate and ammonia concentrations in the blood and the rating of perceived exertion in the training and thiamine treatment compared to the placebo treatment after 60 minutes of the exercise, and free fatty acid does not increase. Therefore, it is expected that the serotonin concentration in the blood is not the same with the brain, and more specific studies are required in the future. The training and thiamine treatments shows significant decrease in the rating of perceived exertion than the placebo treatment. Boyle et al. [63] observe that the decrease of the glucose concentration in the brain affects the rating of perceived exertion. Therefore, the reason why the rating of perceived exertion is low is that sufficient amount of glucose is supplied to the central nerve system by effectively using the glucose from the thiamine supplementation for the thiamine treatment.
The combination of such results confirms that the thiamine supplementation for more than 4 weeks brings significant effect on the energy metabolism during exercise, decreases the lactate and ammonia concentration and the rating of perceived exertion; it also positively affects anti-fatigue and may be used as an effective treatment similar to the endurance training. The endurance training with the thiamine supplementation or the complex treatment of glucose or fructose with different glycemic index may be provided as the basic data for the future studies which may verify the effect of biological activity.
Acknowledgments
This work was supported by the National Research Foundation of Korea Grant funded by the Korean Government (NRF-2012S1A5A2A01016180)
REFERENCES
- 1.Singh A, Moses FM, Deuster PA. Vitamin and mineral status in physically active men: effects of a high-potency supplement. Am J Clin Nutr. 1992;55:1–7. doi: 10.1093/ajcn/55.1.1. [DOI] [PubMed] [Google Scholar]
- 2.Jacobson B, Sobonya C, Ransone J. Nutrition practices and knowledge of college varsity athletes: A follow-up. J Strength Cond Res. 2001;15:63–8. [PubMed] [Google Scholar]
- 3.Soares MJ, Satyanarayana K, Bamji MS, Jacob CM, Ramana YV, Rao SS. The effect of exercise on the riboflavin status of adult men. Br J Nutr. 1993;69:541–51. doi: 10.1079/bjn19930054. [DOI] [PubMed] [Google Scholar]
- 4.Manore MM. Effect of physical activity on thiamine, riboflavin, and vitamin B-6 requirements. Am J Clin Nutr. 2000;72:598S–606. doi: 10.1093/ajcn/72.2.598S. [DOI] [PubMed] [Google Scholar]
- 5.Parker WD, Haas R, Stumpf DA, Parks J, Eguren LA, Jackson C. Brain mitochondrial metabolism in experimental thiamine deficiency. Neurology. 1984;34:1477–81. doi: 10.1212/wnl.34.11.1477. [DOI] [PubMed] [Google Scholar]
- 6.Itokawa Y, Nishino K, Igarashi S. Evaluation of thiamin derivatives: human bioavailability, uptake by human blood cells, and conversion to thiamin by rat liver homegenate. Vitamins. 1992;66:35–42. [Google Scholar]
- 7.Kitamori N, Itokawa Y. Pharmacokinetics of thiamin after oral administration of thiamin tetrahydrofuryl disulfide to humans. J Nut Sc Vitaminol. 1993;39:465–72. doi: 10.3177/jnsv.39.465. [DOI] [PubMed] [Google Scholar]
- 8.Sen I, Cooper JR. The turnover of thiamine and its phosphate esters in rat organs. Neurochem Res. 1976;1:65–71. doi: 10.1007/BF00965632. [DOI] [PubMed] [Google Scholar]
- 9.Lonsdale D. A review of the biochemistry, metabolism and clinical benefits of thiamin(e) and its derivatives. ℯ CAM. 2006;3:49–59. doi: 10.1093/ecam/nek009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Kaiserauer S, Snyder AC, Sleeper M, Zierath J. Nutritional, physiological, and menstrual status of distance runners. Med Sci Sports Exerc. 1989;21:120–5. [PubMed] [Google Scholar]
- 11.Guilland JC, Penaranda T, Gallet C, Boggio V, Fuchs F, Klepping J. Vitamin status of young athletes including the effects of supplementation. Med Sci Sports Med. 1989;21:441–9. [PubMed] [Google Scholar]
- 12.Hasegawa I, Inoue K, Ishii K, Higuchi M. Nutritional status of vitamin B1 and B2 in male high school speed skaters [in Japanese] Japan J Nutr Dietetics. 2000;58:59–66. [Google Scholar]
- 13.van der Beek EJ. Vitamin supplementation and physical exercise performance. J Sports Sci. 1991;9:77–89. doi: 10.1080/02640419108729868. [DOI] [PubMed] [Google Scholar]
- 14.van der Beek EJ, van Dokkum W, Wedel M, Schrijver J, van den Berg H. Thiamin, riboflavin and vitamin B6: Impact of restricted intake on physical performance in man. J Am Coll Nutr. 1994;13:629–40. doi: 10.1080/07315724.1994.10718459. [DOI] [PubMed] [Google Scholar]
- 15.Fogelholm M, Ruokonen I, Laakso JT, Vuorimaa T, Himberg JJ. Lack of association between indices of vitamin B-1, B-2 and B-6status and exercise-induced blood lactate in young adults. Int J Sport Nutr. 1993;3:165–76. doi: 10.1123/ijsn.3.2.165. [DOI] [PubMed] [Google Scholar]
- 16.Nakamura M. The effect of thiamine tetrahydrofurfury1 disulfide on fatigue of workers in and iron works(in japanese) Jpn J Industrial Health. 1971;13:17–36. [Google Scholar]
- 17.Smidt LJ, Cremin FM, Grivetti LE, Clifford AJ. Influence of thiamin supplementation on the health and general well-being of an elderly Irish population with marginal thiamin deficiency. J Gerontol. 1991;46:M16–22. doi: 10.1093/geronj/46.1.m16. [DOI] [PubMed] [Google Scholar]
- 18.Knippel M, Mauri L, Belluschi R, Bana G, Galli C, Pusterla GL, Spreafico M, Troina E. Azione della tiamina sulla produzione di acido lattico nei ciclisti. Med Sport. 1986;39:11–6. [Google Scholar]
- 19.McNeill AW, Mooney TJ. Relationship among carbohydrate loading, elevated thiamine intake and the cardiovascular endurance of conditioned mice. J Sports Med Phys Fitness. 1983;23:257–62. [PubMed] [Google Scholar]
- 20.Nozaki S, Mizuma H, Tanaka M, Jin G, Tahara T, Mizuno K, Yamato M, Okuyama K, Eguchi A, Akimoto K, Kitayoshi T, Mochizuki-Oda N, Karaoka Y, Watanabe Y. Thiamine tetrahydrofurfury1 disulfide improves energy metabolism and physical performance during physical-fatigue loading in rats. Nutr Res. 2009;29:867–72. doi: 10.1016/j.nutres.2009.10.007. [DOI] [PubMed] [Google Scholar]
- 21.Doyle MR, Webster MJ, Erdmann LD. Allithiamine ingestion does not enhance isokinetic parameters of muscle performance. Int J Sport Nutr. 1997;7:39–47. doi: 10.1123/ijsn.7.1.39. [DOI] [PubMed] [Google Scholar]
- 22.Webster MJ. Physiological and performance responses to supplementation with thiamin and pantothenic acid derivatives. Eur J Appl Physiol. 1998;77:486–91. doi: 10.1007/s004210050364. [DOI] [PubMed] [Google Scholar]
- 23.Nakai N, Miyazaki Y, Sato Y, Oshida Y, Nagasaki M, Tanaka M, Nakashima K, Shimomura Y. Exercise training increases the activity of pyruvate dehydrogenase complex in skeletal muscle of diabetic rats. Endocr J. 2002;49:547–54. doi: 10.1507/endocrj.49.547. [DOI] [PubMed] [Google Scholar]
- 24.Babei-Jadidi R, Karachalias N, Kupich C, Ahmed N, Thornalley PJ. High-dose thiamine therapy counters dysilpidaemia in steptozotocin-induced diabetic rats. Diabetologia. 2004;47:2235–46. doi: 10.1007/s00125-004-1582-5. [DOI] [PubMed] [Google Scholar]
- 25.Beltramo E, Berrone E, Tarallo S, Porta M. Effects of thiamine and benfotiamine on intracellular glucose metabolism and relevance in the prevention of diabetic complications. Acta Diabetol. 2008;45:131–41. doi: 10.1007/s00592-008-0042-y. [DOI] [PubMed] [Google Scholar]
- 26.Berrone E, Beltramo E, Solimine C, Ape AU, Porta M. Regulation of intracellular glucose and polyol pathway by thiamine and benfotiamine in vascular cells cultured in high glucose. J Biol Chem. 2006;281:9307–13. doi: 10.1074/jbc.M600418200. [DOI] [PubMed] [Google Scholar]
- 27.Hammes HP, Du X, Edelstein D, Taguchi T, Matsumura T, Ju Q, LIn J, Bierhaus A, Nawroth P, Hannak D, Neumaier M, Berqfeld R, Giardino I, Brownlee M. Benfotiamine blocks three major pathways of hyperglycemic damage and prevents experimental diabetic retinopathy. Nat Med. 2003;9:294–9. doi: 10.1038/nm834. [DOI] [PubMed] [Google Scholar]
- 28.Kohda Y, Shirakawa H, Yamane K, Otsuka K, Kono T, Terasaki F, Tanaka T. Prevention of incipient diabetic cardiomyopathy by high-does thiamine. J Toxicol Sci. 2008;33:459–72. doi: 10.2131/jts.33.459. [DOI] [PubMed] [Google Scholar]
- 29.Thornalley PJ. The potential role of thiamine(vitamin B1) in diabetic complications. Curr Diabetes Rev. 2005;1:287–98. doi: 10.2174/157339905774574383. [DOI] [PubMed] [Google Scholar]
- 30.Schmid U, Stopper H, Heidland A, Schupp N. Benfotiamine exhibits direct antioxidative capacity and prevents induction of DNA damage in vitro. Diabetes Metab Res Rev. 2008;24:371–7. doi: 10.1002/dmrr.860. [DOI] [PubMed] [Google Scholar]
- 31.Scholte HR, Busch HF, Luty-Houwen IE. Vitamin-responsive pyruvate dehydrogenase deficiency in a young girl with external ophthalmoplegia, myopathy and lactic acidosis. J Inherite Metab Dis. 1992;15:331–4. doi: 10.1007/BF02435969. [DOI] [PubMed] [Google Scholar]
- 32.Borg G. Perceived exertion as an indicator of somatic stress. Scand J Rehab Med. 1970;2:92–8. [PubMed] [Google Scholar]
- 33.Friedlander AL, Casazza GA, Horning MA, Buddinger TF, Brooks GA. Effects of exercise intensity and training on lipid metabolism in young women. Am J Physiol. 1998;275:E853–63. doi: 10.1152/ajpendo.1998.275.5.E853. [DOI] [PubMed] [Google Scholar]
- 34.McKenzie S, Phillips SM, Carter SL, Lowther S, Gibala MJ, Tarnopolsky MA. Endurance exercise training attenuates leucine oxidation and BCOAD activation during exercise in humans. Am J Physiol Endocrinol Metab. 2000;278:E580–7. doi: 10.1152/ajpendo.2000.278.4.E580. [DOI] [PubMed] [Google Scholar]
- 35.Phillips SM, Green HJ, Tarnopolsky MA, Grant SM. Decreased glucose turnover after short-term training is unaccompanied by changes in muscle oxidative potential. Am J Physiol. 1995;269:E222–30. doi: 10.1152/ajpendo.1995.269.2.E222. [DOI] [PubMed] [Google Scholar]
- 36.Parolin ML, Chesley A, Matsos MP, Spriet LL, Jones NL, Heigenhauser GJ. Regulation of skeletal muscle glycogen phosphorylase and PDH during maximal intermittent exercise. Am J Physiol. 1999;277:E890–900. doi: 10.1152/ajpendo.1999.277.5.E890. [DOI] [PubMed] [Google Scholar]
- 37.Strumilo S, Czerniecki J, Dobrzyn P. Regulatory effect of thiamin pyrophosphate on pig heart pyruvate dehydrogenase complex. Biochem Biophys Res Commun. 1999;256:341–5. doi: 10.1006/bbrc.1999.0321. [DOI] [PubMed] [Google Scholar]
- 38.Choi SK. The effects of thiamine on anti-fatigue during exercise. J Exerc Nutr Biochem. 2012;16:193–202. doi: 10.5717/jenb.2013.17.4.189. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Guezennec CY, Abdelmalki A, Serrurier B, Merino D, Bigard X, Berthelot M, Pierard C, Peres M. Effects of prolonged exercise on brain ammonia and amino acids. Int J Sports Med. 1998;19:323–7. doi: 10.1055/s-2007-971925. [DOI] [PubMed] [Google Scholar]
- 40.Banister EW, Cameron BJ. Exercise-induced hyperammonemia: peripheral and central effects. Int J Sports Med. 1990;11:S129–42. doi: 10.1055/s-2007-1024864. [DOI] [PubMed] [Google Scholar]
- 41.Phillips SM, Green HJ, Tarnopolsky MA, Heigenhauser GF, Hill RE, Grant SM. Effects of training duration on substrate turnover and oxidation during exercise. J Appl Physiol. 1996;81:2182–91. doi: 10.1152/jappl.1996.81.5.2182. [DOI] [PubMed] [Google Scholar]
- 42.Park DH, Gubler CJ. Studies on the physiological functions of thiamine. V. Effects of thiamine deprivation and thiamine antagonists on blood pyruvate and lactate levels and activity of lactate dehydrogenase and its isozymes in blood and tissues. Biochim Biophys Acta. 1969;177:537–43. [PubMed] [Google Scholar]
- 43.Durkot MJ, De Garavilla L, Caretti D, Francesconi R. The effects of dichloroacetate on lactate accumulation and endurance in an exercising rat model. Int J Sports Med. 1995;16:167–71. doi: 10.1055/s-2007-972986. [DOI] [PubMed] [Google Scholar]
- 44.Hatta H, Soma R, Atomi Y. Effect of dichloroacetate on oxidative removal of lactate in mice after supramaximal exercise. Comp Biochem Physiol B. 1991;100:561–4. doi: 10.1016/0305-0491(91)90220-8. [DOI] [PubMed] [Google Scholar]
- 45.Veech RL, Veloso D, Mehlman MA. Thiamin deficiency: liver metabolite levels and redox and phosphorylation states in thiamin-deficient rats. J Nutr. 1973;103:267–72. doi: 10.1093/jn/103.2.267. [DOI] [PubMed] [Google Scholar]
- 46.Drouin R, Lavoie C, Bourque J, Ducros F, Poisson D, Chiasson J. Increased hepatic glucose production response to glucagon in trained subjects. Am J Physiol. 1998;274:E23–8. doi: 10.1152/ajpendo.1998.274.1.E23. [DOI] [PubMed] [Google Scholar]
- 47.Wasserman DH, Spalding JA, Lacy DB, Colburn CA, Goldstein RE, Cherrington AD. Glucagon is a primary controller of hepatic glycogenolysis and gluconeogenesis during muscular work. Am J Physiol. 1989;257:E108–17. doi: 10.1152/ajpendo.1989.257.1.E108. [DOI] [PubMed] [Google Scholar]
- 48.Bonjorn VM, Latour MG, Belanger P, Lavoie J. Influence of prior exercise and liver glycogen content on the sensitivity of the liver to glucagon. J Appl Physiol. 2002;92:188–94. doi: 10.1152/jappl.2002.92.1.188. [DOI] [PubMed] [Google Scholar]
- 49.Brooks GA, Donovan CM. Effect of endurance training on glucose kinetics during exercise. Am J Physiol. 1983;244:E505–12. doi: 10.1152/ajpendo.1983.244.5.E505. [DOI] [PubMed] [Google Scholar]
- 50.Kjaer M. Regulation of hormonal and metabolic responses during exercise in humans. Exerc Sport Sci Rev. 1992;20:161–84. [PubMed] [Google Scholar]
- 51.Mendenhall LA, Swanson SC, Habash DL, Coggan AR. Ten days of exercise training reduces glucose production and utilization during moderate-intensity exercise. Am J Physiol. 1994;266:E136–43. doi: 10.1152/ajpendo.1994.266.1.E136. [DOI] [PubMed] [Google Scholar]
- 52.Byun SW, Choi SH, Park HG, Kim BJ, Kim EY, Lee KH, Yang WS. A case of lactic acidosis caused by thiamine deficiency. Korean J Med. 2007;73:443–7. [Google Scholar]
- 53.Lee DC, Chu J, Satz W, Silbergleit R. Low plasma thiamine levels in elder patients admitted through the emergency department. Acad Emerg Med. 2000;7:1156–9. doi: 10.1111/j.1553-2712.2000.tb01268.x. [DOI] [PubMed] [Google Scholar]
- 54.Mancinelli R, Ceccanti M, Guiducci MS, Sasso GF, Sebastiani G, Attilia ML, Allen JP. Simultaneous liquid chromatographic assessment of thiamine, thiamine monophosphate and thiamine diphosphate in human erythrocytes: a study on alcoholics. J Chromatogr B Analyt Technol Biomed Life Sci. 2003;789:355–63. doi: 10.1016/s1570-0232(03)00139-9. [DOI] [PubMed] [Google Scholar]
- 55.Talwar D, Davidson H, Cooney J, St JO'Reilly D. Vitamin B(1) status assessed by direct measurement of thiamin pyrophosphate in erythrocytes or whole blood by HPLC: comparison with erythrocyte transketolase activation assay. Clin Chem. 2000;46:704–10. [PubMed] [Google Scholar]
- 56.Sato A, Shimoyama Y, Ishikawa T, Murayama N. Dietary thiamin and riboflavin intake and blood thiamin and riboflavin concentrations in college swimmers undergoing intensive training. Int J Sport Nutr Exerc Metab. 2011;21:195–204. doi: 10.1123/ijsnem.21.3.195. [DOI] [PubMed] [Google Scholar]
- 57.Soares J, Naffah-Mazzacoratti MG, Cavalheiro EA. Increased serotonin levels in physically trained men. Braz J Med Biol Res. 1994;27:1635–8. [PubMed] [Google Scholar]
- 58.Hassan EA, Amin MA. Pilates exercises influence on the serotonin hormone, some physical variables and the depression degree in battered women. World J Sport Sci. 2011;5:89–100. [Google Scholar]
- 59.Davis JM, Bailey SP. Possible mechanisms of central nervous system fatigue during exercise. Med Sci Sports Exerc. 1997;29:45–57. doi: 10.1097/00005768-199701000-00008. [DOI] [PubMed] [Google Scholar]
- 60.Romanowski W, Grabiec S. The role of serotonin in the mechanism of central fatigue. Acta Physiol Pol. 1974;25:127–34. [PubMed] [Google Scholar]
- 61.Pitsiladis YP, Strachan AT, Davidson I, Maughan RJ. Hyperprolactinaemia during prolonged exercise in the heat: evidence for a centrally mediated component of fatigue in trained cyclists. Exp Physiol. 2002;87:215–26. doi: 10.1113/eph8702342. [DOI] [PubMed] [Google Scholar]
- 62.Newsholme EA, Blomstrand E. Tryptophan, 5-hydroxy-tryptamine and a possible explanation for central fatigue. Adv Exp Med Biol. 1995;384:315–20. doi: 10.1007/978-1-4899-1016-5_25. [DOI] [PubMed] [Google Scholar]
- 63.Boyle PJ, Nagy RJ, O'Connor AM, Kempers SF, Yeo RA, Qualls C. Adaptations in brain glucose uptake following recurrent hypoglycemia. Proc Natl Acad Sci. 1994;91:9352–6. doi: 10.1073/pnas.91.20.9352. [DOI] [PMC free article] [PubMed] [Google Scholar]