

Abstract
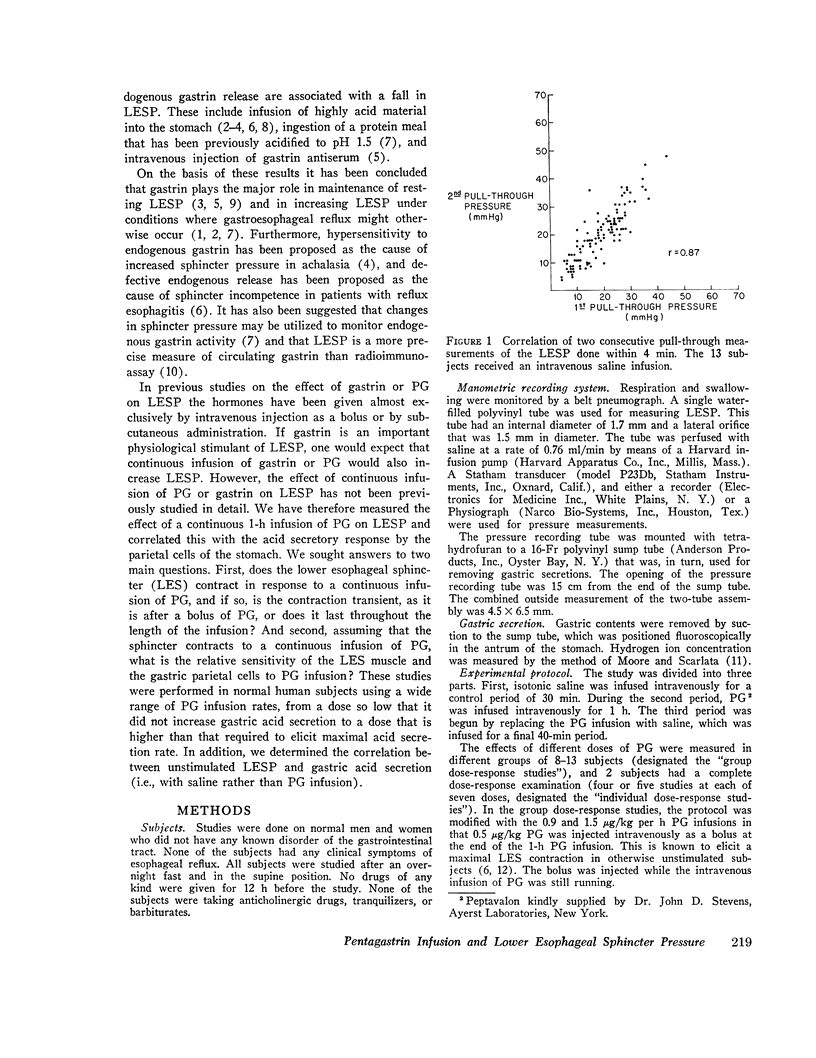
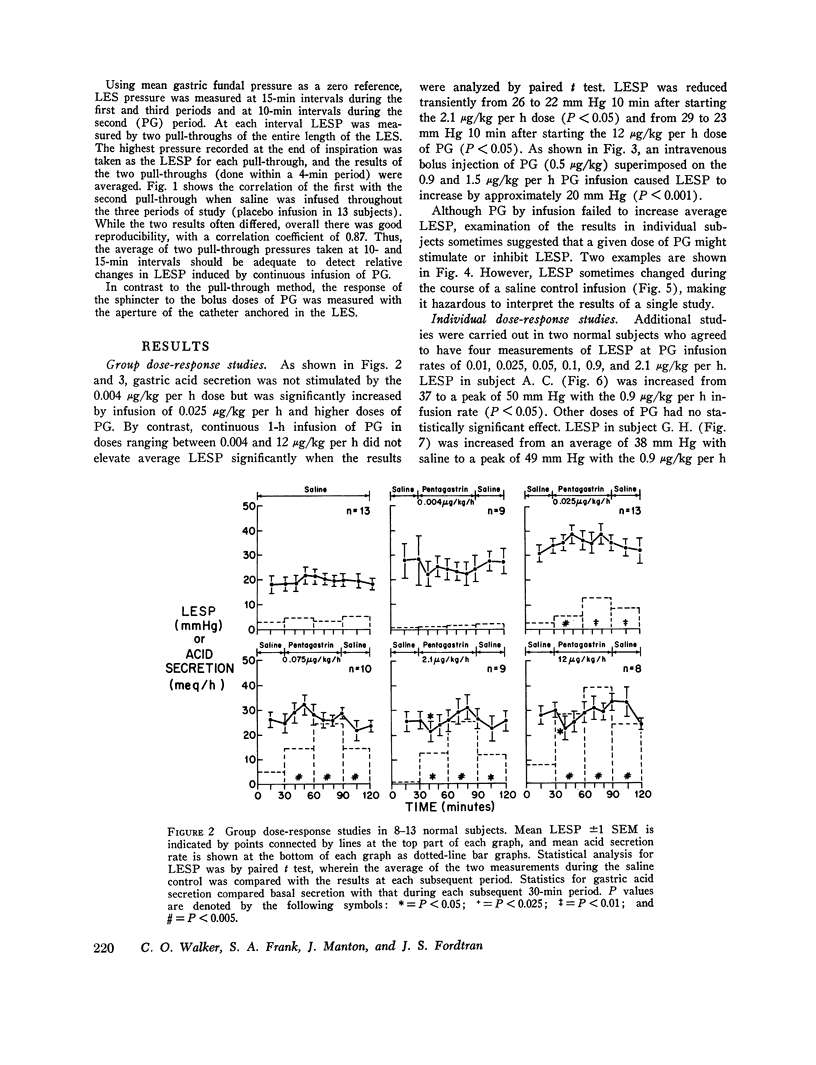
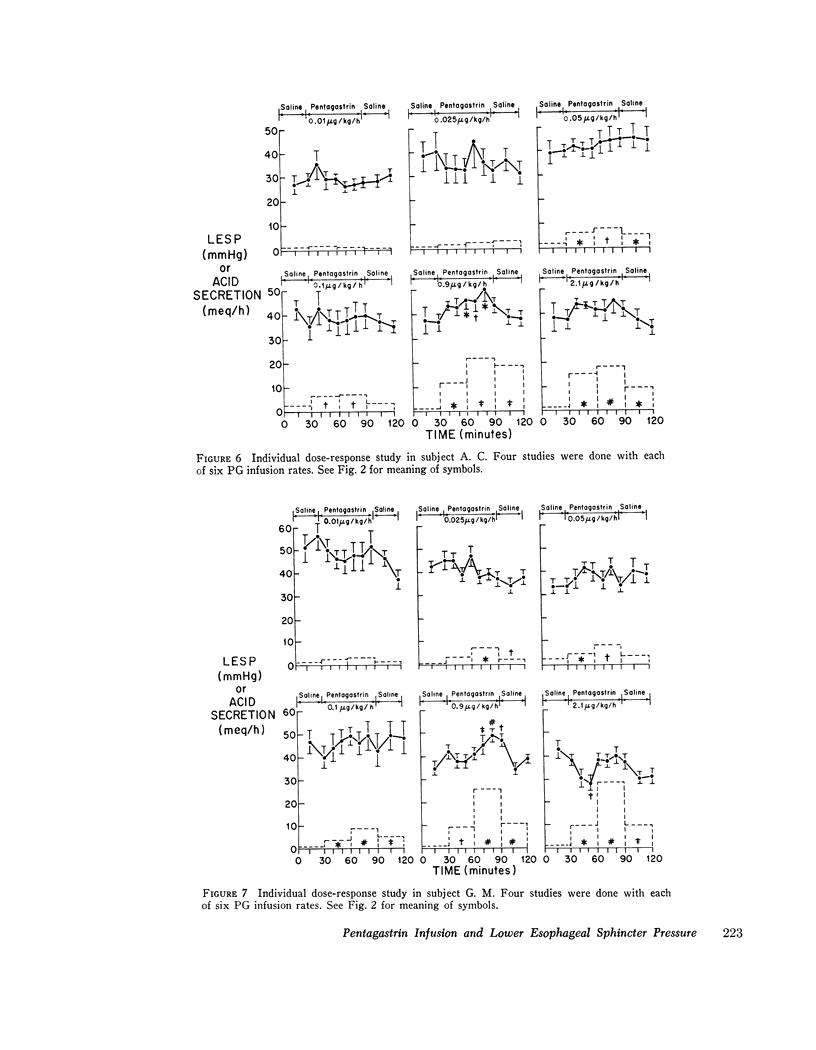
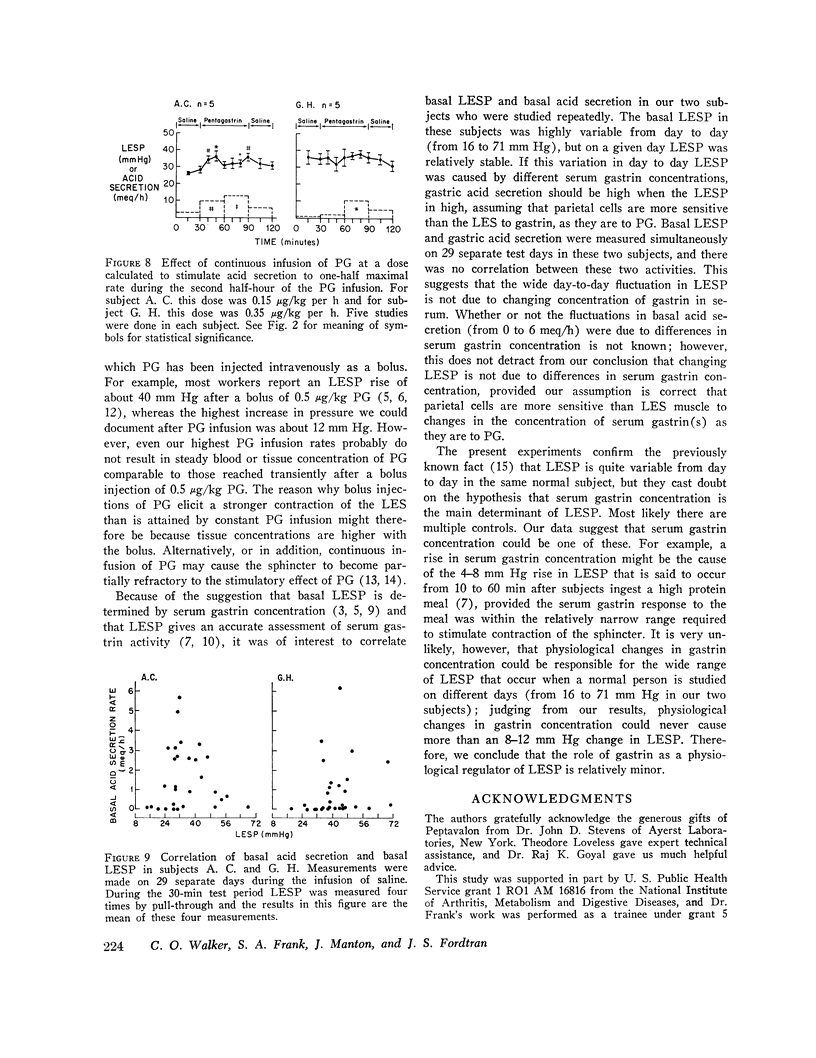
Bolus injections of gastrin or pentagastrin (PG) cause a marked elevation in lower esophageal sphincter pressure (LESP), and it has been suggested that serum gastrin concentration is the main physiological and pathophysiological regulator of LESP. We evaluated this hypothesis by measuring LESP and gastric acid secretion simultaneously in normal subjects during continuous infusion of PG (0.004-12 mjg/kg per h), since continuous infusion of a hormone probably simulates physiological hormone release better than bolus injection. In groups of 8-13 subjects there was no statistically significant increase in average LESP with any of seven PG infusion rates. However, a bolus of PG superimposed on the continuous infusion of PG resulted in a 20-mm Hg increase in LESP. Examination of results in individual subjects suggested that PG by infusion might be stimulating LESP in some subjects and inhibiting it in others. Therefore, individual dose-response studies were performed in two normal subjects. These revealed that 0.9 mug/kg per h PG by infusion elevated LESP by 10-12 mm Hg. This dose of PG also elicited maximal rates of gastric acid secretion. In one of the subjects an infusion of PG calculated to give one-half maximal acid secretion (D50) elevated LESP by 8 mm Hg; in the other the PG-D50 for acid secretion had no effect on sphincter pressure. Infusion of smaller amounts of PG had no effect on LESP, even though gastric acid secretion was stimulated submaximally. Thus, the parietal cells are more sensitive than the lower esophageal sphincter to the effect of PG by infusion. We conclude that PG by continuous infusion elevates LESP to only a modest degree (compared with the contraction that occurs after bolus injections of PG) and that the contraction occurs only within a narrow dose range between the D50 and D100 for acid secretion. Higher doses cause transient relaxation of LESP. Additional studies showed that basal LESP varied between 16 and 71 mm Hg in two subjects studied on 29 separate occasions, but there was no correlation with basal acid secretion. This suggests that the wide day-to-day fluctuations in basal LESP are not due to changing concentrations of gastrin in serum. The results of these experiments cast doubt on the hypothesis that serum gastrin concentration is the major determinant of LESP.
Full text
PDF


Images in this article
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Castell D. O., Harris L. D. Hormonal control of gastroesophageal-sphincter strength. N Engl J Med. 1970 Apr 16;282(16):886–889. doi: 10.1056/NEJM197004162821602. [DOI] [PubMed] [Google Scholar]
- Castell D. O., Levine S. M. Lower esophageal sphincter response to gastric alkalinization. A new mechanism for treatment of heartburn with antacids. Ann Intern Med. 1971 Feb;74(2):223–227. doi: 10.7326/0003-4819-74-2-223. [DOI] [PubMed] [Google Scholar]
- Cohen S. Hypogastrinemia and sphincter incompetence. N Engl J Med. 1973 Jul 26;289(4):215–217. doi: 10.1056/NEJM197307262890413. [DOI] [PubMed] [Google Scholar]
- Cohen S., Lipshutz W. Hormonal regulation of human lower esophageal sphincter competence: interaction of gastrin and secretin. J Clin Invest. 1971 Feb;50(2):449–454. doi: 10.1172/JCI106512. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cohen S., Lipshutz W., Hughes W. Role of gastrin supersensitivity in the pathogenesis of lower esophageal sphincter hypertension in achalasia. J Clin Invest. 1971 Jun;50(6):1241–1247. doi: 10.1172/JCI106601. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Farrell R. L., Castell D. O., McGuigan J. E. Measurements and comparisons of lower esophageal sphincter pressures and serum gastrin levels in patients with gastroesophageal reflux. Gastroenterology. 1974 Sep;67(3):415–422. [PubMed] [Google Scholar]
- Giles G. R., Mason M. C., Humphries C., Clark C. G. Action of gastrin on the lower oesophageal sphincter in man. Gut. 1969 Sep;10(9):730–734. doi: 10.1136/gut.10.9.730. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hirschowitz B. I., Sachs G. Pentagastrin in the gastric fistula dog. Gastroenterology. 1969 Mar;56(3):456–467. [PubMed] [Google Scholar]
- Lipshutz W. H., Gaskins R. D., Lukash W. M., Sode J. Pathogenesis of lower-esophageal-sphincter incompetence. N Engl J Med. 1973 Jul 26;289(4):182–184. doi: 10.1056/NEJM197307262890404. [DOI] [PubMed] [Google Scholar]
- Lipshutz W., Hughes W., Cohen S. The genesis of lower esophageal sphincter pressure: its identification through the use of gastrin antiserum. J Clin Invest. 1972 Mar;51(3):522–529. doi: 10.1172/JCI106840. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MOORE E. W., SCARLATA R. W. THE DETERMINATION OF GASTRIC ACIDITY BY THE GLASS ELECTRODE. Gastroenterology. 1965 Aug;49:178–188. [PubMed] [Google Scholar]
- Makhlouf G. M. The neuroendocrine design of the gut. The play of chemicals in a chemical playground. Gastroenterology. 1974 Jul;67(1):159–184. [PubMed] [Google Scholar]
- Nebel O. T., Castell D. O. Lower esophageal sphincter pressure changes after food ingestion. Gastroenterology. 1972 Nov;63(5):778–783. [PubMed] [Google Scholar]
- Winans C. S., Harris L. D. Quantitation of lower esophageal sphincter competence. Gastroenterology. 1967 May;52(5):773–778. [PubMed] [Google Scholar]