

Calreticulin (CALR) mutations occur in 20%–25% of myeloproliferative neoplasms (MPN).1,2 At least 40 CALR mutations have been reported to date, all located in exon 9. The most frequent CALR mutations are a 52-bp deletion (type 1) and a 5-bp insertion (type 2). Expression of type 1 CALR mutation was shown to induce constitutive activation of JAK-STAT signaling pathway in a Ba/F3-cell line with STAT5 phosphorylation leading to spontaneous growth in the absence of interleukin-3.1 Furthermore, megakaryocyte lineage has been reported to play a major role in MPN pathophysiology.3,4 In particular, hematopoietic colony formation independent of exogenous cytokines, including endogenous megakaryocytic (EMC) and endogenous erythroid colonies (EEC) was shown to be a functional sign of clonal hematopoiesis due to deregulated signaling pathways in MPN. Altogether, these data suggest a particular link between megakaryocytic (MK) proliferation and deregulation of signaling due to driver mutations. However, to our knowledge, spontaneous growth of hematopoietic progenitors (EMC and EEC) has not been characterized in type 1 or type 2 CALR -mutated patients.
In the current study, we analyzed patterns of EMC and EEC according to molecular status (JAK2V617F, CALR, MPL, triple negative) in a cohort of 302 essential thrombocythemia (ET) patients from 3 French University Hospitals [Grenoble (n=121), Dijon (n=121), and Nantes (n=60)]. The inclusion criteria were ET patients who had benefited from in vitro cultures from bone marrow at diagnosis and for whom DNA was available. The JAK2V617F mutation was assessed using purified granulocytes by tetra-primer ARMS-PCR5 or by allele-specific quantitative PCR.6 MPL mutations were screened by high resolution melt assay7 and confirmed by sequencing. The mutational status of CALR was determined using previously described high-resolution sizing of fluorescent dye-labeled PCR amplificons of exon 9, with Sanger sequencing controls.1 To standardize EMC and EEC, cultures were performed from bone marrow samples using the same standardized collagen medium in all three centers.8,9 Megakaryocytic colonies composed of at least 4 MKs were counted by microscopy after MGG staining of dry collagen dishes.9,10 We analyzed EMC and EEC results both qualitatively [presence or not of EMC and/or EEC (so-called “positive or negative EMC/EEC”)] and quantitatively (number of EMC and/or EEC per 105 cells plated). For statistical analysis, non-parametric tests were applied: Mann-Whitney test (for comparison of two groups) and McNemar test (paired data). χ2 or Fisher tests were used to compare nominal variables, and Spearman rank correlation to compare two continuous variables. P<0.05 was considered statistically significant.
The mutational distribution was 50.8% (153 of 302) for JAK2V617F, 23% (69 of 302) for CALR, 5.3% (17 of 302) for MPL and 19% (57 of 302) for “triple negative”. Six patients lacked MPL and/or CALR data (1.9%). Among the 69 patients with CALR mutations, 35 (50.7%) patients harbored type 1 and 24 (34.8%) patients had type 2. Irrespective of mutational status, overall endogenous hematopoietic growth (defined by presence of EMC and/or EEC) was 58.9% (178 of 302). We observed significantly more EMC (56.3%; 170 of 302) than EEC (13.6%; 41 of 302) whatever the mutational status (P<0.001).
In order to determine the relationship between growth profile and genotype, we compared global spontaneous growth defined by EMC and/or EEC positivity according to mutational status. Patients harboring mutations such as JAK2V617F or CALR showed a significantly higher proportion of overall spontaneous growth (respectively 66% and 73.9%) compared to “triple negative” ones (25%; P<0.001). No difference in frequency of EMC and/or EEC between JAK2V617F and CALR was noted (P=0.24). On the contrary, MPL mutations were less frequently associated with EMC and/or EEC compared to CALR (47% and 73.9%, respectively; P=0.03).
As higher platelets counts were reported in patients with CALR mutations in comparison with JAK2V617F patients,11 we attempted to compare the proportion of EMC in these two subgroups (Figure 1). EMC were more frequently observed in CALR than in JAK2V617F (73.9% and 61.4%, respectively) without reaching statistical significance (P=0.07). To strengthen the link between genotypes and megakaryocytic proliferation, we also compared the mean number of EMC according to the molecular status. CALR mutations were associated with a significantly higher mean number of EMC compared to “triple negative” and JAK2V617F patients: 9.36 (0–81.5), 1.75 (0–23.3), and 5.5 (0–53.3), respectively; P<0.01 and P=0.02. A tendency towards a higher number of EMC was observed between CALR and MPL but without statistical significance (P=0.07). Interestingly, concerning EEC, CALR-mutated patients displayed a significantly weaker proportion of EEC positivity compared to JAK2V617F-mutated patients (1.4% vs. 22.8%; P<0.001). This percentage of EEC in JAK2V617F ET is consistent with previous data obtained with a serum-free assay.6,9,12 EEC were rare in the CALR-mutated population; only one type 2-mutated patient among 69 showed 2 EEC per 105 cells. A significantly higher proportion of EEC were associated with JAK2V617F compared to triple negative (P<0.001) and MPL (P<0.05).
Figure 1.
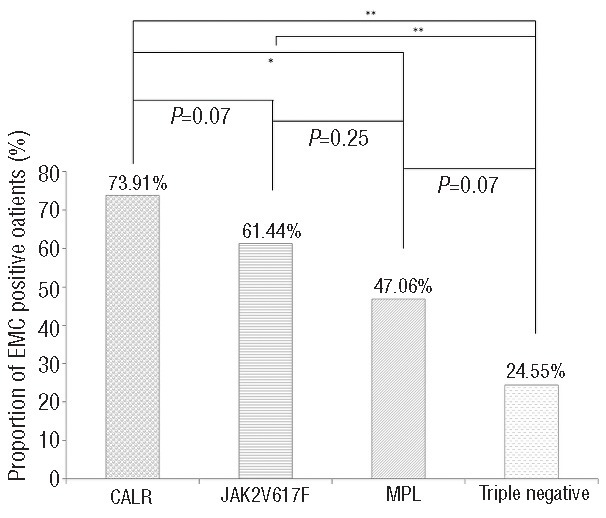
Proportion of patients presenting respectively EMC growth according to mutational status in ET. Statistical differences between mutations were analyzed in pairs (χ2 test). *means P value <0.05; ** means P <0.01.
Next, the endogenous megakaryocytic profile between types 1 and 2 CALR mutants and “variants” was compared. “Variants” have neither type 1 nor type 2 CALR mutations (n=10 patients). EMC frequencies were similar in type 1 and type 2 patients (82.8% and 70.8%, respectively; P=0.34). The proportion of EMC in “variants” was significantly lower than in type 1 mutants (50%; P=0.04), although a higher allelic burden was observed compared to type 1 (P<0.01). Among the population presenting EMC (Figure 2), type 2 patients induced more EMC than type 1 [mean2=19.2 (2.5–81.5) vs. mean1=8.6 (1–46.6), respectively; P=0.03]. Interestingly, among these patients, we observed a significant difference in allelic ratio between type 1 and type 2 [mean1=41.8% (5–65%) and mean2=48.1% (30–73.9%), respectively; P=0.03].
Figure 2.
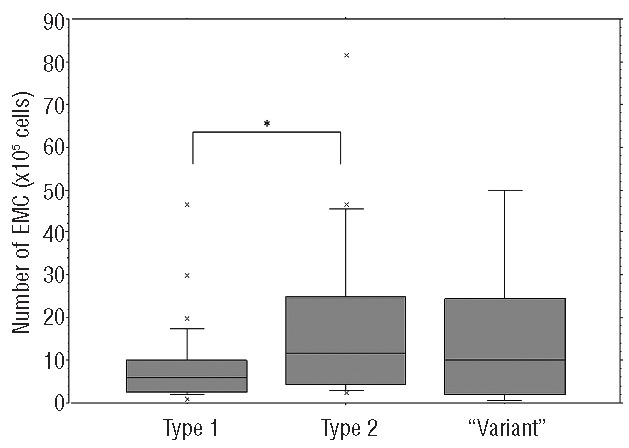
Distribution of number of endogenous megakaryocytic colonies (EMC) among CALR population showing EMC growth. “Variant” corresponds to neither type 1 nor type 2 mutations. Whisker plots represent numbers of EMC expressed per 105 cells plated according to type of CALR mutation. *means P <0.05.
Among the population presenting EMC, no difference in the number of EMC was observed between “variants” and either type 1 or type 2, even if “variants” patients displayed a higher allelic burden than type 1 [meanvariant=56.2% (48–80%); P<0.01] and type 2 (P<0.05). We wondered if there was a correlation between the number of EMC and allelic burden in the CALR-mutated population and according to type of mutation (Figure 3). Overall, no linear correlation was observed either in the whole CALR population (n=68), or in type 1 and type 2 (rho=0.07, P=0.56; rho1=−0.069, P1=0.686 and rho2=0.084, P2=0.69, respectively). However, in the “variants”, we observed a linear correlation between allelic burden and spontaneous megakaryocytic growth (rho=0.705, P<0.05).
Figure 3.
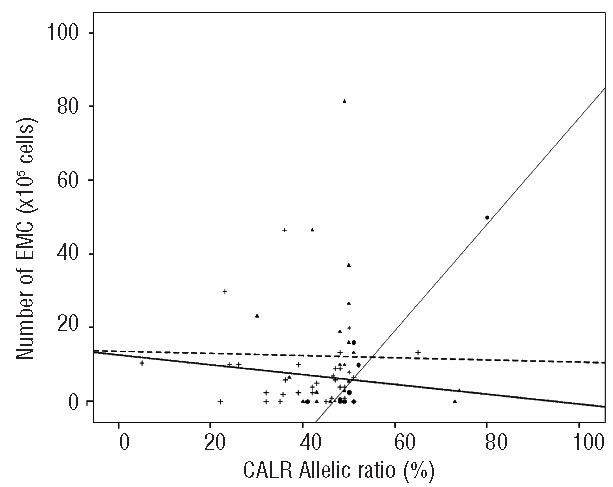
Linear regression of CALR allelic burden according to number of endogenous megakaryotic colonies (EMC). Each symbol represents a patient (respectively + for type 1, ▲for type 2, • for “variants”). Linear regression was done according to type of CALR mutations (- - - for type 1, ▪▪▪ for type 2 and - - - - for “variants”).
Klampfl et al. showed that type 1 CALR mutation induced a cytokine independent growth of the murine Ba/F3 cell line.1 Our study confirmed this finding with the difference that our patient cohort was made up of a ‘real-life’ group of MPN patients and our patient selection did not discriminate between type 1 or type 2 mutations. Moreover, our results highlight a special link between CALR and megakaryocyte proliferation. Firstly, we demonstrated that a significantly higher proportion of CALR patients displayed EMC in comparison to “triple negative” and to MPL-mutated patients. CALR-mutated patients also expressed a higher number of EMC compared to JAK2V617F-mutated patients. The more frequent EMC and the higher number of EMC in CALR-mutated patients argue for an impact of CALR on autonomous MK proliferation. In the same way, it is consistent with the almost complete absence of CALR mutations in polycythemia vera (PV)13 (despite the fact that rare PV cases with CALR mutations have recently been reported14), the higher platelet counts in CALR patients,11 and the preferential expression of CALR-mutated protein in megakaryocytes.15 Our results also confirm that EEC is a characteristic feature of JAK2V617F mutation. No EEC was observed in MPL-mutated patients and only one patient carrying CALR mutation was EEC positive. These functional differences could be related to lower hemoglobin counts observed in CALR patients compared to those with JAK2V617F mutations. These differences in the balance between erythroid and MK proliferation strengthen the evidence for a megakaryocytic role for CALR mutants in ET pathogenesis, and define different growth profiles of ET: JAK2V617F patients harbor a “mixed profile” (erythroid and MK) compared to the “MK profile” of CALR patients.
Among populations presenting EMC, we observed significantly more EMC and a higher allelic burden in type 2 than in type 1. This supports the hypothesis that, in CALR-mutated patients, the greater allele burden induces increased cytokine-independent MK proliferation and subsequent clone enlargement. This suggests not only a contribution of mutation type but also of CALR allele burden on ET phenotypes. Nevertheless, the CALR allelic burden did not show any linear correlation with the number of EMC either in type 1 or in type 2 mutants. Hence, the CALR allelic burden may not be the only factor determining the intensity of EMC growth: others mutations or genetic modifiers (i.e. epigenetic, RNA splicing) could impact MK activation, and thereby disease evolution.
Finally, our study showed that a “variant” subpopulation displayed EMC in 50% of cases. Even though MK “variants” appear to be less proliferative (less frequent EMC) than type 1 CALR, a linear and positive correlation between the number of EMC and allelic burden was observed. This suggests that, in this heterogeneous subgroup, EMC could identify patients in whom CALR plays a pivotal role in autonomous activation of MK. In our opinion, it may be interesting to study “not type 1 nor type 2” variants in a larger cohort and according to their clinical features. In conclusion, our study underlines the functional link between CALR mutants and megakaryocyte growth stimulation. These findings improve our understanding of phenotypic differences observed among patients with different driver mutations and different CALR genotypes.
Acknowledgments
We thank T. Jouve (University Hospital, Grenoble, France) for his statistical expertise, A M Foote (Grenoble Clinical Research Center) for language editing, and S. Hermouet for reviewing.
Footnotes
Funding: the study was supported by FIM (French Intergroup for MPN).
Information on authorship, contributions, and financial & other disclosures was provided by the authors and is available with the online version of this article at www.haematologica.org.
References
- 1.Klampfl T, Gisslinger H, Harutyunyan AS, et al. Somatic mutations of calreticulin in myeloproliferative neoplasms. N Engl J Med. 2013; 369(25):2379–2390. [DOI] [PubMed] [Google Scholar]
- 2.Nangalia J, Massie CE, Baxter EJ, et al. Somatic CALR mutations in myeloproliferative neoplasms with nonmutated JAK2. N Engl J Med. 2013;369(25):2391–2405. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Balduini A, Badalucco S, Pugliano MT, et al. In vitro megakaryocyte differentiation and proplatelet formation in Ph-negative classical myeloproliferative neoplasms: distinct patterns in the different clinical phenotypes. PLoS One. 2011;6(6):e21015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Cazzola M, Kralovics R. From Janus kinase 2 to calreticulin: the clinically relevant genomic landscape of myeloproliferative neoplasms. Blood. 2014;123(24):3714–3719. [DOI] [PubMed] [Google Scholar]
- 5.Jones AV, Kreil S, Zoi K, et al. Widespread occurrence of the JAK2 V617F mutation in chronic myeloproliferative disorders. Blood. 2005; 106(6):2162–2168. [DOI] [PubMed] [Google Scholar]
- 6.Lippert E, Boissinot M, Kralovics R, et al. The JAK2-V617F mutation is frequently present at diagnosis in patients with essential thrombocythemia and polycythemia vera. Blood. 2006;108(6):1865–1867. [DOI] [PubMed] [Google Scholar]
- 7.Boyd EM, Bench AJ, Goday-Fernandez A, et al. Clinical utility of routine MPL exon 10 analysis in the diagnosis of essential thrombocythaemia and primary myelofibrosis. Br J Haematol. 2010; 149(2):250–257. [DOI] [PubMed] [Google Scholar]
- 8.Dobo I, Donnard M, Girodon F, et al. Standardization and comparison of endogenous erythroid colony assays performed with bone marrow or blood progenitors for the diagnosis of polycythemia vera. Hematol J. 2004;5(2):161–167. [DOI] [PubMed] [Google Scholar]
- 9.Dobo I, Boiret N, Lippert E, et al. A standardized endogenous megakaryocytic erythroid colony assay for the diagnosis of essential thrombocythemia. Haematologica. 2004;89(10):1207–1212. [PubMed] [Google Scholar]
- 10.Mi JQ, Blanc-Jouvan F, Wang J, et al. Endogenous megakaryocytic colony formation and thrombopoietin sensitivity of megakaryocytic progenitor cells are useful to distinguish between essential thrombocythemia and reactive thrombocytosis. J Hematother Stem Cell Res. 2001;10(3):405–409. [DOI] [PubMed] [Google Scholar]
- 11.Rotunno G, Mannarelli C, Guglielmelli P, et al. Impact of calreticulin mutations on clinical and hematological phenotype and outcome in essential thrombocythemia. Blood. 2014;123(10):1552–1555. [DOI] [PubMed] [Google Scholar]
- 12.Boissinot M, Lippert E, Girodon F, et al. Latent myeloproliferative disorder revealed by the JAK2-V617F mutation and endogenous megakaryocytic colonies in patients with splanchnic vein thrombosis. Blood. 2006;108(9):3223–3224. [DOI] [PubMed] [Google Scholar]
- 13.Rumi E, Pietra D, Ferretti V, et al. JAK2 or CALR mutation status defines subtypes of essential thrombocythemia with substantially different clinical course and outcomes. Blood. 2014;123(10):1544–1551. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Broseus J, Park JH, Carillo S, Hermouet S, Girodon F. Presence of calreticulin mutations in JAK2-negative polycythemia vera. Blood. 2014;124(26):3964–3966. [DOI] [PubMed] [Google Scholar]
- 15.Vannucchi AM, Rotunno G, Bartalucci N, et al. Calreticulin mutation-specific immunostaining in myeloproliferative neoplasms: pathogenetic insight and diagnostic value. Leukemia. 2014; 28(9):1811–1888. [DOI] [PMC free article] [PubMed] [Google Scholar]