

Abstract
Background and Objectives
Electronic cigarettes (e-cigarettes) are a recent technology that has gained rapid acceptance. Still, little is known about them in terms of safety and effectiveness. A basic question is how effectively they deliver nicotine, however the literature is surprisingly unclear on this point. Here, a population pharmacokinetic (PK) model was developed for nicotine and its major metabolite cotinine with the aim to provide a reliable framework for the simulation of nicotine and cotinine concentrations over time, based solely on inhalation airflow recordings and individual covariates (i.e. weight and breath carbon monoxide CO levels).
Methods
This study included 10 adults self-identified as heavy smokers (at least one pack per day). Plasma nicotine and cotinine concentrations were measured at regular 10-minute intervals for 90 minutes while human subjects inhaled nicotine vapor from a modified e-cigarette. Airflow measurements were recorded every 200 milliseconds throughout the session. A population PK model for nicotine and cotinine was developed based on previously published PK parameters and the airflow recordings. All the analyses were performed with the nonlinear mixed-effect modelling software NONMEM 7.2.
Results
The results show that e-cigarettes deliver nicotine effectively, although the pharmacokinetic profiles are lower than those achieved with regular cigarettes. Our PK model effectively predicts plasma nicotine and cotinine concentrations from the inhalation volume, and initial breath CO.
Conclusion
E-cigarettes are effective at delivering nicotine. This new PK model of e-cigarette usage might be used for pharmacodynamic analysis where the PK profiles are not available.
Keywords: nicotine, cotinine, NONMEM
1 Introduction
The pharmacokinetics of nicotine and cotinine are well characterized in humans [1-3]. In 1992 Robinson et al. published a reliable physiologically based pharmacokinetic (PBPK) model describing the disposition kinetics of nicotine and its major metabolite, cotinine, in humans (1). Very recently, Teeguarden et al. published a multi-route model of nicotine–cotinine pharmacokinetics also in humans[2]. They also developed a PBPK model of nicotine and cotinine in humans after administration via i.v., oral and also inhalation routes using cigarettes (nicotine yield, 1.3 mg). Since the most common administration route for nicotine is inhalation, a focus on i.v. and oral administration route pharmacokinetics analysis might be limited.
The use of electronic cigarettes (e-cigarettes) has increased dramatically over the past few years, leading to a host of legal and regulatory issues over how to classify electronic cigarettes. An e-cigarette is a battery powered device which simulates tobacco smoking. These e-cigarettes generally use a small heating element that vaporizes a liquid solution containing the active ingredients, water, and propylene glycol or a similar solvent. The user simply inhales the resulting vapor in a process called “vaping”, an action similar to regular smoking but with electronic cigarette vapor. Some solutions contain a mixture of nicotine and flavorings, while others release a flavored vapor without nicotine. E-cigarette users generally perceive e-cigarettes to be effective at reducing nicotine cravings and also perceive them to be less harmful than regular cigarettes [4;5]. The benefits and risks of electronic cigarette use are uncertain as the technology is relatively new. While electronic cigarettes may be less harmful than regular cigarettes, they may still contain impurities and toxic ingredients [6]. There is some evidence that they are effective at delivering nicotine [7-9], as e-cigarettes lead to similar plasma cotinine elevations as regular cigarettes [10], although they may yield less nicotine per puff [11]. Users may need a period of weeks to learn how to use them to deliver the most nicotine. Individuals new to e-cigarettes typically obtain lower plasma nicotine concentrations initially, but after four weeks of experience with e-cigarettes, they are able to achieve higher plasma nicotine concentrations and significantly greater overall nicotine intake [12]. However, the literature is ambiguous on how effectively e-cigarettes deliver nicotine to users, as some have reported no measurable increases in plasma nicotine following e-cigarette usage [13;14].The current study addresses how effectively e-cigarettes may deliver nicotine, and how well the delivery can be described with a PK model.
For the current study, a customized electronic cigarette was developed to allow precise measurements of the heated air temperature and time course of inhaled nicotine vapor volume. This allowed for precise control of and measurement of the nicotine vapor delivered. The developed electronic cigarette device is also compatible with magnetic resonance imaging (MRI) to allow direct functional neuroimaging during electronic cigarette usage in future studies. This allows for the direct measurement of brain activity while subjects make decisions about using nicotine as an addictive drug. First however, it is necessary to characterize the nicotine delivery resulting from inhalation from electronic cigarettes and the custom device described in this paper specifically. It should be noted that this custom e-cigarette was designed to be MR-compatible, and although it provides the same functionality as open market e-cigarettes, we did not explicitly compare its performance to available e-cigarettes (see Limitations).
In this work, a population PK model for nicotine and its major metabolite, cotinine was developed, based on the airflow recordings of e-cigarettes, the loading dose for the e-cigarette, the individual covariates, and on the nicotine and cotinine PK parameters published by Robinson et al. [3]. The purpose of this model was to provide a framework for the simulation of nicotine and cotinine concentrations over time, based solely on airflow recordings and individual covariates (i.e. weight and initial CO levels). To the best of our knowledge, this is the first population PK model describing nicotine and cotinine exposure with the use of e-cigarettes. This model can be used for pharmacodynamic analysis where the PK profiles are not available (kinetic-pharmacodynamic, KPD).
2 Methods
2.1 Electronic nicotine delivery system: custom e-cigarette
A customized electronic nicotine delivery system, “custom e-cigarette” compatible with MRI was developed. The custom e-cigarette is contained in an approximately 12” long section of 2” diameter PVC tubing. Inside the tubing is a ceramic heater set to maintain a controlled temperature of 300 degrees Fahrenheit. The heated air is drawn over a small wad of nonferromagnetic metallic wool, which served to provide a matrix with a large surface area for the heated air to vaporize the nicotine liquid. The wool is also non-combustible at the temperatures used, which helps avoid a burnt smell that otherwise may occur in e-cigarettes. The wool was loaded with 0.45 mL of 18mg/mL nicotine liquid (JC original smoke juice, Johnson Creek, ISO 9001:2008 certified). We chose a US-based smoke juice supplier to minimize concerns regarding the quality and purity of the smoke juice, and we used an external supplier so that we could provide a realistic e-cigarette experience. Nicotine is readily absorbed in liquid form through the skin, so the custom e-cigarette was never loaded with more than 0.45mL at a time in order to minimize the risk of nicotine overdose from accidental liquid contact or ingestion. The heated air vaporizes the liquid held in the metal wool, and the heated nicotine vapor then flows into a 12” long, ½” diameter clear plastic tube. At the other end of the tube there is a disposable oneway valve which is inserted into the subject's mouth. In this way subjects can inhale heated nicotine vapor. The exhaled breath is subsequently vacuumed from a facemask on the subject's face and then forced through a carbon filter to avoid filling the experiment room with nicotine vapor.
The air flow into the custom e-cigarette is measured and controlled by a Controller. The Controller maintained the ceramic heater at 300° F and included an air flow measuring device (Omega FMA1700/1800). Air flow measurements were sampled at 5Hz by an A-to-D converter and stored in a host computer for further processing. The Controller also had a solenoid valve that allowed access to the custom e-cigarette to be enabled or disabled by a host computer, but this feature was not used in the current study as the device was kept open for ad libitum consumption.
2.2 Study design
Subjects were included in the study if they self-identified as heavy smokers (at least one pack per day) and had no stated intention of trying to stop smoking. Subjects (N=10, 5 females, ages 18 to 24, mean 20.3) gave informed consent to participate. All procedures were reviewed and approved by the Indiana University Institutional Review Board. Subjects were asked to abstain from smoking for six hours prior to the study. After providing informed consent, the subjects were then weighed. Their exhaled breath carbon monoxide was measured (Smokerlyzer piCO, Covita) in parts per million. This measurement provided some information about how recently they had likely smoked and how much. More importantly, it also allowed us the option to screen out subjects who had recently smoked substantially and were therefore not likely to desire significant additional nicotine at the time [15]. The fact that subjects knew we would perform an initial CO screen provided additional incentive for them to abstain from cigarettes prior to the session. In practice, no subjects were excluded for excessive exhaled CO. After the CO measurement, study subjects were seated comfortably and then given an IV saline lock cannula by a registered nurse. The nurse drew 4 mL of blood at the start of the experiment and then again every 10 minutes throughout the experiment, for a total of ten blood draws throughout the ninety minute session. Subjects were instructed to sit comfortably and inhale ad libitum for the duration. In some cases, if subjects noted that the vapor seemed to be depleted of nicotine, an additional amount of nicotine liquid was added to the custom e-cigarette. After the procedure, the blood samples were spun down for ten minutes, and the plasma was pipetted off and stored at −20 degrees Celsius. Four additional subjects completed the study but could not be analyzed due to equipment malfunction, leaving ten subjects reported in the analyses below.
2.3 Mass spectroscopy analysis
Nicotine, (+/−) cotinine, trans-3’-OH cotinine, and (S)cotinine N-oxide were quantified in plasma using phenacetin as the internal standard, liquid-liquid extraction, and HPLC-MS/MS (API3200, Applied Biosystems). Separation of all analytes was performed with gradient HPLC (acetonitrile:10 mM ammonium acetate, pH=5.0) using a CN column (Luna, 5 μm, 4.6 X 150 mm). The mass spectrometer was run in positive mode and the Q1/Q3 settings for each analyte were 163/130, 177/80, 193/80, 193/96 and 180/65 for nicotine, cotinine, trans-3’-OH cotinine, cotinine-N-oxide, and phenacetin, respectively. In total, 560 concentrations were measured (140 x 4 analytes). The limit of quantification (LOQ) is 0.1 ng/mL for both compounds: 32 measurements below the LOQ (5.71% ).
2.4 Data analysis
All analyses were performed using NONMEM version 7.2 (Icon Development Solutions, Hanover, Maryland). Data below the limit of quantification (BLQ) were reported for both nicotine and metabolite at 0.1 ng/mL (see Mass spectroscopy analysis section for more details). BLQ values were included in the analyses and treated as censored information using the M3 method [18]. With the M3 method, the BQL observations in particular are taken to be the likelihoods that these observations are indeed below the limit. The Laplacian numerical estimation method was used for parameter estimation. Nicotine and cotinine concentrations were simultaneously described. Due to the specific study design, some of the PK parameters were fixed to literature values. Inter-subject variability (ISV) was modeled using exponential functions. An additive model was used to describe residual variability for log-transformed data. This is consistent with a proportional error on the linear scale. Other residual error structures were also evaluated (e.g. combined error).
2.4.1 Dose and airflow
Inhaled nicotine is assumed to enter lung blood instantaneously, consistent with experimental data showing rapid uptake via inhalation [16;17]. The amount of nicotine that reaches the systemic circulation is assumed to be proportional to the airflow recordings. The inhaled airflow was recorded every 200 milliseconds throughout the 90 minute session, even when the subject was not actively inhaling. Therefore, the airflow recordings were processed as follows: (i) Every negative value was transformed to zero; (ii) the 97.5th percentile of the airflow values was calculated based on all subjects (0.4 mL/min); (iii) Every value below this threshold was transformed to zero, implying no drug input at those times. The selection of the 97.5th percentile was based on the empirical distribution function of the airflows (no negative values) (supplementary material, online resource 1) with the aim to ensure the identification of the dose events (the patient is inhaling nicotine vapor) and to reduce the noise in the inputs. The dose events were defined based on this processed airflow (airflowP), the custom e-cigarette loading dose (LD - 18mg/mL) and a scaling factor (F) as follows:
| (eq. 1) |
The parameter F is a scaling factor that links the airflow recoding and the loading dose with the actual drug amount that reaches the systemic circulation.
2.4.2 Pharmacokinetic modeling
The population PK model for nicotine and its major metabolite cotinine developed in this analysis is based on the physiologically based pharmacokinetic (PBPK) model published by Robinson et al. [3] in 1992. This PBPK model accurately describes the disposition kinetics of nicotine and its major metabolite, cotinine, in human. Robinson et al. derived different rates and parameters from previously published human and animal data.Then, the PBPK model was tested comparing simulations of published studies, using similar dosing protocols to those reported. Total plasma clearances [CLT=CLH+CLR] and volumes of distribution for nicotine and cotinine (Vd) were then calculated from the PBPK ouput.
Due to the nature of the study design presented here, those model PK parameters were not directly estimable and were therefore fixed to the values reported by Robinson et al [3]: (i) Total plasma clearance (CLT = CLH + CLR) was fixed to 1.56 L/min for nicotine and 0.067 L/min for cotinine; (ii) Nicotine hepatic clearance (CLH) was fixed to 1.09 L/min, where the 80% goes to cotinine (CL2COT = 0.872 L/min)[19] and the rest to other metabolites (CL2METO = 0.218 L/min); (iii) total plasma clearance for cotinine was fixed to CLCOT = 0.065 L/min (CLH=0.055 and CLR=0.010 L/min); (iv) Apparent volume of distribution (Vd) for nicotine and cotinine were fixed to 207 L and 73 L respectively based on the values reported by Robinson et al. [3]. All physiological parameters were based on population values for a 70-kg man. Both nicotine and cotinine pharmacokinetics were simultaneously described with a one compartment linear model for each compound. Only the input parameters were estimated for this model based on the inhalation rates shown in equation 1.
2.4.3 CO levels: Covariate analysis
Exhaled carbon monoxide (CO, in parts per million) is a biomarker of recent smoking history [15] that might impact the nicotine and cotinine pharmacokinetic profiles. The potential effect of this covariate was evaluated in all model parameters. As expected, higher exhaled CO concentration was associated with higher initial concentrations for nicotine and cotinine. Linear and nonlinear models were explored connecting the initial concentrations for nicotine and cotinine based on the CO measurements. The selected models are shown in equation 2 for nicotine and in equation 3 for its major metabolite:
| (eq. 2) |
| (eq. 3) |
where CO is the individual level of carbon monoxide, θNIC and θCOT are the initial concentrations for nicotine and cotinine respectively in absence of CO, and γNIC and γCOT the nonlinear factors.
2.4.4 Model selection criteria and evaluation
The minimum value of the objective function (OFV) provided by NONMEM, which corresponds approximately to −2 ×log(likelihood) [−2LL], served as a criteria for model comparison during the model development process. A decrease in −2LL of 6.63 points for one additional parameter, was regarded as a significant model improvement corresponding to a p-value of 0.01 for nested models. The Akaike information criteria (AIC), calculated as AIC=−2LL+2×NP, where NP is the number of parameter in the model, was used for selection among non-nested models [20]. The choice of the final model was based also on the OFV value, the precision of parameter estimates, goodness-of-fit plots and individual visual predictive checks (IVPCs). Precision of parameter estimates expressed as the 5th and 95th percentiles of the parameter distribution were computed from the analysis of 300 bootstrap data sets (sampling with replacement). The bootstrap analysis was performed using Perl-speaks-NONMEM [21]. Model parameter estimates were presented together (Table 1) with the corresponding relative standard error RSE(%), as a measure of parameter imprecision computed from the results of the bootstrap analysis. The degree of inter-subject variability (ISV) was expressed as a coefficient of variation CV(%). Inspection of goodness-of-fit plots included conditional weighted residuals (CWRES) and normalized prediction distribution errors (NPDE) [22;23]. Model performance was evaluated with individual visual predictive checks (IVPC): For every subject, based on the airflow and specific individual measurements (e.g. weight and level of CO), two hundred virtual individuals were simulated. At each time-point the 2.5, 50 and 97.5th percentiles were calculated in every simulated study for nicotine and cotinine concentrations. Then, the 95% prediction interval from the resultant percentiles was computed and represented over time together with the raw individual data. Predictive checks were performed using MATLAB environment (The Mathworks, MA, United States).
Table 1.
PK parameters.
| Bootstrap analysis Median [2.5-97.5th percentiles] |
||||
|---|---|---|---|---|
| Parameters | Estimate(RSE%) | ISV (RSE%) | Estimate | ISV |
| F (min/mL · mg) | 0.123 (26.87) | 80.62 (49.78) | 0.128 [0.087 0.196] | 76.35 [18.34 104.9] |
| VC (L) | 207 fixed | |||
| VM (L) | 73 fixed | 30.98 (43.44) | 29.34 [1.761 38.69] | |
| CL2COT (L/min) | 0.872 fixed | |||
| CL = CLEX + CL2METO (L/min) | CL2METO = 0.218 fixed | |||
| CLEX = 0.17 fixed | ||||
| CLCOT (L/min) | 0.065 fixed | |||
| θNIC (ng/mL) | 7.87 (70.75) | 132 (68.34) | 6.475 [0.355 17.813] | 117.2 [73.74 186.9] |
| θCOT (ng/mL) | 329 (39.21) | 40 (45.47) | 297.5 [115.3 524.0] | 34.03 [12.01 48.53] |
| γNIC (no units) | 1.5 (40.05) | 1.648 [1.105 2.996] | ||
| γCOT (no units) | 1.32 (18.25) | 1.364 [1.059 1.789] | ||
| cov(σNICO,σCOTO) | 0.527 (42.58) | 0.394 [0.087 0.771] | ||
| Res Error nicotine [log(ng/mL)] * | 0.507 (14.62) | 0.489 [0.378 0.611] | ||
| Res Error cotinine [log(ng/mL)] * | 0.217 (13.91) | 0.210 [0.161 0.254] | ||
Additive error model in log scale
F, scaling factor for dose calculation and bioavailability; VC and VM, the volumes of distribution of the central compartment for nicotine and cotinine respectively; CL2COT and CL2METO are the formation rates for cotinine and other metabolites respectively; CLEX and CLCOT are the elimination rates for nicotine and cotinine; θNIC and θCOT are the initial concentrations for nicotine and cotinine respectively in absence of CO, and γNIC and γCOT the nonlinear factors
3 Results
A customized electronic nicotine delivery system, “custom e-cigarette” compatible with MRI was developed (Figure 1). The airflow recordings were used in order to establish the nicotine dose events (Figure 2) (one individual example on the online resource 2). Prior to the model development, the data were explored in an attempt to evaluate the link between those recordings and the nicotine plasma concentrations. The visualization of the individual airflow patterns (Figure 3A) and the corresponding individual PK profiles of the parent compound (nicotine) (Figure 3B) indicated that the “custom e-cigarette” actually delivers nicotine. Individuals with higher number (and intensity) of dose events (inhalations) tend to have higher concentrations throughout the 90 minute duration of the study.
Figure 1. Diagram of custom e-cigarette apparatus.
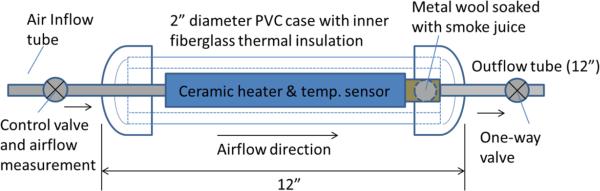
Air passed through a ceramic heater encased in 2” diameter PVC pipe, where it was heated to a controlled temperature of 300F. The heated air passed through a small orifice and over a ½” diameter ball of non-ferromagnetic metallic wool, which was saturated with 0.45mL of smoke juice (Johnson Creek, nominal 18 mg/mL nicotine). The resulting heated vapor passed through a one-way check valve along a 12” section of flexible tubing and into the user's mouth. Inhaled airflow was measured in mL/min.
Figure 2. A. Airflow: Raw data. B. Airflow: Processed data.

The processing was developed in three consecutive steps: (i) Every negative value was transformed to zero; (ii) the 97.5th percentile was calculated based on all subjects; (iii) Every value below such percentile was transformed to zero. C. Airflow: Dose events. The dose events and their intensities were defined as processed airflow recordings bigger than zero (see methods for more details).
Figure 3.

A. Individual dose events identified from the airflow Every subplot corresponds a different individual. Circles represent the dose events, the individual is inhaling, based on the airflow measurements. B. Individual nicotine plasma concentrations. Circles are the observed nicotineconcentrations for every individual. Dashed lines are a linear interpolation between the observations. Solid black line shows the observed median kinetic for nicotine. Every color corresponds to a different individual. Same color code was used than for the individual dose events subplots, allowing the connection between airflow – dose events and the nicotine PK profiles.
The structure of the selected model is shown in Figure 4. The meaning of the model parameters are shown in the legend. The corresponding NONMEM control stream for the selected model is shown in the supplementary material (Online Resource 3). Inter-subject variability (ISV) was found to be significant for the dose scaling factor F, the distribution volume in the central compartments for cotinine VM, and in the initial plasma concentrations for nicotine and cotinine NIC0 and COT0 respectively (Table 1). η-shrinkage (%) was 1.14 (F), 6.55 (Vm), 3.87 (NIC0) and 4.03 (COT0). The inclusion of a positive correlation between the BSV associated to the initial nicotine and cotinine concentrations significantly improved the OFV provided by NONMEM, as well as the visual model fitting. Part of the variability associated to these two parameters was explained by the measured levels of carbon monoxide (CO) at the beginning of the experiment. This reinforces the CO measurement as a very informative biomarker of recent smoking history. The weight of the individuals was also evaluated for correlation with the PK parameters but did not improve the model predictions. No other covariates were explored. Model parameter estimates are presented in Table 1 with the corresponding RSE%.
Figure 4. Structural pharmacokinetic model for nicotine and its major metabolite cotinine.

Circles represent the central compartments for nicotine and cotinine. PK parameters: F, scaling factor for dose calculation and bioavailability; VC and VM are the volumes of distribution of the central compartment for nicotine and cotinine respectively, CL2COT and CL2METO are the formation rates for cotinine and other metabolites respectively; CLEX and CLCOT are the elimination rates for nicotine and cotinine.
Individual and population model predictions as well as the empirical data are shown in figure 5. Figure 6 displays the goodness of fit plots for nicotine and cotinine, indicating that the selected model reasonably describes the observations. Observations were compared with the population model predictions (figure 6, left) as well as with individual predictions (figure 6, center). No dose bias and misspecifications were observed. Evaluation of the NPDE did not show any tendency or model misspecification either (figure 6, right).
Figure 5. Individual predictions versus observations for nicotine (A) and cotinine (B).

The grey colors in (A) denote nicotine; and the light blue colors in (B) denote cotinine. Circles represent observations above the minimum quantification level. Squares represent observations below the quantification level. The red dashed lines represent the population prediction. The solid lines represent the individual predictions.
Figure 6.

Goodness of fit plots of the selected population PK model for (A) nicotine (grey) and (B) cotinine (light blue). PRED corresponds to the population model predictions, IPRED to the individual model predictions and NPDE the normalized prediction distribution errors. Solid lines show the identity lines for the first two columns and 0 line for the last column.
Model performance was also evaluated with individual visual predictive checks (IVPC) (Figure 7); based on the individual airflow time series, and on the corresponding individual CO levels, the 95% predicted interval was calculated for nicotine and cotinine plasma concentrations.
Figure 7. Individual Visual Predictive Checks.

Results from 200 simulated studies. Shaded areas represent the 95% prediction interval (PI) for every individual based on their airflow, CO levels and weight. The black lines correspond to the median of the simulated subjects. Points are the observations. The grey color stands for nicotine (A) and light blue for the major metabolite cotinine (B).
4 Discussion
Efficacy
Our results demonstrate that electronic cigarettes provide effective and measurable nicotine delivery, and that the subsequent nicotine pharmacokinetics and metabolism can be accounted for by existing models. Furthermore, with a sufficiently strong nicotine concentration in the liquid “smoke juice” loaded into the e-cigarette, the plasma nicotine reaches lower but still comparable levels to those resulting from conventional cigarette smoking (Figure 3). This demonstration of effective nicotine delivery by e-cigarettes stands in contrast with earlier report[13;14], but is consistent with more recent report showing effectiveness at increasing plasma nicotine [8;9], and also with other reports showing increased plasma cotinine as a result of e-cigarette use [10][11]. The present results are also consistent with self-reported effectiveness at reducing nicotine cravings [4;5].
Accuracy
Besides demonstrating the efficacy of e-cigarettes in terms of delivering nicotine, the model developed in this paper provides the first description of the concentration time profiles for nicotine and cotinine after inhalation from an electronic cigarette device. Thus, the model allows the plasma nicotine and cotinine levels to be predicted non-invasively. Furthermore, the developed model had well determined parameters as evidenced by the low RSE values and predicted individual concentration profiles well. The results are consistent with earlier modeling approaches to nicotine from cigarettes [3]. Nevertheless, the results should be replicated independently in order to increase confidence in the model.
A key technical aspect of being able to manage the 5Hz measurement frequency for the airflow was to filter what were apparent “noise” signals that represented most of the measurements over time. It was not likely that this very low flow rates (<0.4mL/min) would have contributed to the overall observed concentration and their inclusion would have made the modeling approach untenable. By filtering above the 97.5th percentile, key input events for nicotine inhalation/dose delivery were captured (see figures 1B and 1C).
The accuracy of the model depends on having a good estimate of the initial conditions of plasma concentrations. We explicitly measured the starting plasma concentrations, and we additionally measured exhaled CO as an additional (though limited) correlate of initial plasma concentrations. The exhaled CO is only useful as a predictor of recent cigarette smoking and would not be expected to correlate with recent e-cigarette usage, as these generate no significant CO. The CO is primarily utilized to predict the baseline concentrations and, at least statistically, significantly improved the description by the model of the baseline values. Thus, it is not the CO that is the target of interest but rather the impact on predicting the likely baseline nicotine level where this CO measure appears to be useful. Still, if e-cigarette airflow is measured for a sufficiently long period of time, the impact of the initial conditions (and associated inaccuracies) will diminish toward zero over time.
E-cigarettes
Many questions remain open regarding the safety and effectiveness of e-cigarettes, especially as aids to smoking cessation. Our results do not address whether e-cigarettes are safe for the public, although our very modest sample size revealed no immediate adverse events. Our results also do not indicate whether e-cigarettes are effective as an aid to smoking cessation. What our results do show as a first step however is that e-cigarettes can be effective in delivering nicotine specifically in a way that is well-characterized by our pharmacokinetic model.
As e-cigarette use becomes more and more common, understanding associated nicotine delivery and both cognitive and addictive effects will become more important. This model represents a tool that can help to more precisely understand the relationship between the inhalation delivered nicotine dose and nicotine and cotinine plasma concentration levels. The plasma concentration levels can then be evaluated in the context of any number of target responses or toxicities.
Looking ahead, we are currently planning to use our custom electronic cigarette device to carry out functional neuroimaging studies of e-cigarette use. The present study provides a foundation for our planned functional neuroimaging, as our device is MR-compatible. In this way, it will be possible to predict plasma nicotine and cotinine concentrations in subjects without having to simultaneously draw blood. This non-invasive approach may be particularly helpful in experiments involving many interventions, where the action of a blood draw may skew patient responses in MRI based studies as well as increase the costs associated with the study. This first issue is particularly important when assessing the cognitive and addiction liability effects of nicotine inhalation using the MRI paradigm.
Limitations
The study has several limitations. Our custom e-cigarette was designed to be MR-compatible, and as such, it may not be identical to e-cigarettes available on the open market. We did not directly compare our custom e-cigarette against commercial e-cigarettes. The commercial e-cigarettes may vary among brands in their effectiveness at delivering nicotine. Likewise, available smoke juice formulations may differ in composition and effective bioavailability. Thus, we have not shown that every available e-cigarette effectively delivers nicotine, and it is beyond the scope of the current study to do so. Also, we have not shown that every available e-cigarette smoke juice effectively delivers nicotine, as the effective bioavailability may vary as a function of solution pH and other ingredients in the smoke juice. The estimated value for the scaling factor F will have to be re-estimated if other e-cigarettes are used, since it could vary among brands. Due to the data available and study design, other factors that might affect nicotine delivery have not been explored here.
Our study specifically showed that at least the present custom e-cigarette with an airflow temperature of 300° F over a non-combustible medium (metallic wool) and with the particular smoke juice can effectively deliver nicotine. Also, we have shown that the nicotine delivery can be accounted for with a PK model similar to one that is valid for regular cigarettes, as a function of inhaled e-cigarette vapor volume. Another potential limitation of the current study is that e-cigarette users become more proficient at using the e-cigarette over time, so that they are able to increase their plasma nicotine levels more effectively after a few weeks of use. We did not control for the length of time subjects had used e-cigarettes. However, are recruitment criteria required that subjects be current heavy smokers with no stated intention of quitting. This means that our subjects were generally not e-cigarette users, and they would therefore be less proficient at increasing their plasma nicotine levels. The fact that we found measurable plasma nicotine increases suggests that the relative lack of experience did not prevent them from obtaining nicotine from our custom e-cigarette. Furthermore, our detailed measurements of airflow account for any individual differences based on levels of experience with e-cigarettes. Finally, due to the limited sample size of the present study, the model we present here should be validated in an independent sample of subjects.
5 Conclusion
A well estimated population pharmacokinetic model for plasma concentrations of nicotine and cotinine after e-cigarette nicotine delivery was developed and will provide the basis for the determination of typical nicotine levels for any given pattern of e-cigarette associated airflow delivery of nicotine.
Supplementary Material
Key Points.
Electronic cigarettes (e-cigarettes) are rapidly gaining acceptance, but their pharmacokinetic effect with respect to nicotine is unclear.
We measured initial carbon monoxide (CO) breath, e-cigarette inhalation airflow and plasma nicotine and cotinine concentrations for 90 minutes while human subjects are using the e-cigarette. Based on these data we developed a population PK model able to simultaneously describe nicotine and cotinine profiles in plasma.
E-cigarettes deliver nicotine effectively, although the pharmacokinetic profiles are lower to those achieved with regular cigarettes. The model might be extremely useful for nicotine drug effect analysis and quantification when the actual PK profiles are not available.
Abbreviations
- e-cigarette
electronic cigarette
- ISV
inter- subject variability
- NPDE
normalized prediction distribution errors
- RSE
relative standard error
- CV
coefficient of variation
- CO
carbon monoxide
- LOQ
lower limit of quantification
Reference List
- 1.Yamazaki H, Horiuchi K, Takano R, Nagano T, Shimizu M, Kitajima M, et al. Human blood concentrations of cotinine, a biomonitoring marker for tobacco smoke, extrapolated from nicotine metabolism in rats and humans and physiologically based pharmacokinetic modeling. Int J Environ Res Public Health. 2010;7:3406–3421. doi: 10.3390/ijerph7093406. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Teeguarden JG, Housand CJ, Smith JN, Hinderliter PM, Gunawan R, Timchalk CA. A multi-route model of nicotine-cotinine pharmacokinetics, pharmacodynamics and brain nicotinic acetylcholine receptor binding in humans. Regul Toxicol Pharmacol. 2013;65:12–28. doi: 10.1016/j.yrtph.2012.10.007. [DOI] [PubMed] [Google Scholar]
- 3.Robinson DE, Balter NJ, Schwartz SL. A physiologically based pharmacokinetic model for nicotine and cotinine in man. J Pharmacokinet Biopharm. 1992;20:591–609. doi: 10.1007/BF01064421. [DOI] [PubMed] [Google Scholar]
- 4.Etter JF, Bullen C. Electronic cigarette: users profile, utilization, satisfaction and perceived efficacy. Addiction. 2011;106:2017–2028. doi: 10.1111/j.1360-0443.2011.03505.x. [DOI] [PubMed] [Google Scholar]
- 5.Caponnetto P, Campagna D, Cibella F, Morjaria JB, Caruso M, Russo C, et al. EffiCiency and Safety of an eLectronic cigAreTte (ECLAT) as tobacco cigarettes substitute: a prospective 12-month randomized control design study. PLoS One. 2013;8:e66317. doi: 10.1371/journal.pone.0066317. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Cheng T. Chemical evaluation of electronic cigarettes. Tob Control. 2014;23(Suppl 2):ii11–ii17. doi: 10.1136/tobaccocontrol-2013-051482. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Grana R, Benowitz N, Glantz SA. E-cigarettes: a scientific review. Circulation. 2014;129:1972–1986. doi: 10.1161/CIRCULATIONAHA.114.007667. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Dawkins L, Corcoran O. Acute electronic cigarette use: nicotine delivery and subjective effects in regular users. Psychopharmacology (Berl) 2014;231:401–407. doi: 10.1007/s00213-013-3249-8. [DOI] [PubMed] [Google Scholar]
- 9.Vansickel AR, Eissenberg T. Electronic cigarettes: effective nicotine delivery after acute administration. Nicotine Tob Res. 2013;15:267–270. doi: 10.1093/ntr/ntr316. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Flouris AD, Poulianiti KP, Chorti MS, Jamurtas AZ, Kouretas D, Owolabi EO, et al. Acute effects of electronic and tobacco cigarette smoking on complete blood count. Food Chem Toxicol. 2012;50:3600–3603. doi: 10.1016/j.fct.2012.07.025. [DOI] [PubMed] [Google Scholar]
- 11.Schroeder MJ, Hoffman AC. Electronic cigarettes and nicotine clinical pharmacology. Tob Control. 2014;23(Suppl 2):ii30–ii35. doi: 10.1136/tobaccocontrol-2013-051469. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Hajek P, Goniewicz ML, Phillips A, Myers SK, West O, McRobbie H. Nicotine Intake From Electronic Cigarettes on Initial Use and After 4 Weeks of Regular Use. Nicotine Tob Res. 2014 doi: 10.1093/ntr/ntu153. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Vansickel AR, Cobb CO, Weaver MF, Eissenberg TE. A clinical laboratory model for evaluating the acute effects of electronic “cigarettes”: nicotine delivery profile and cardiovascular and subjective effects. Cancer Epidemiol Biomarkers Prev. 2010;19:1945–1953. doi: 10.1158/1055-9965.EPI-10-0288. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Eissenberg T. Electronic nicotine delivery devices: ineffective nicotine delivery and craving suppression after acute administration. Tob Control. 2010;19:87–88. doi: 10.1136/tc.2009.033498. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Middleton ET, Morice AH. Breath carbon monoxide as an indication of smoking habit. Chest. 2000;117:758–763. doi: 10.1378/chest.117.3.758. [DOI] [PubMed] [Google Scholar]
- 16.Hukkanen J, Jacob P, III, Benowitz NL. Metabolism and disposition kinetics of nicotine. Pharmacol Rev. 2005;57:79–115. doi: 10.1124/pr.57.1.3. [DOI] [PubMed] [Google Scholar]
- 17.Armitage AK, Dollery CT, George CF, Houseman TH, Lewis PJ, Turner DM. Absorption and metabolism of nicotine from cigarettes. Br Med J. 1975;4:313–316. doi: 10.1136/bmj.4.5992.313. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Beal SL. Ways to fit a PK model with some data below the quantification limit. J Pharmacokinet Pharmacodyn. 2001;28:481–504. doi: 10.1023/a:1012299115260. [DOI] [PubMed] [Google Scholar]
- 19.Benowitz NL, Porchet H, Jacob P., III Nicotine dependence and tolerance in man: pharmacokinetic and pharmacodynamic investigations. Prog Brain Res. 1989;79:279–287. doi: 10.1016/s0079-6123(08)62487-5. [DOI] [PubMed] [Google Scholar]
- 20.Ludden TM, Beal SL, Sheiner LB. Comparison of the Akaike Information Criterion, the Schwarz criterion and the F test as guides to model selection. J Pharmacokinet Biopharm. 1994;22:431–445. doi: 10.1007/BF02353864. [DOI] [PubMed] [Google Scholar]
- 21.Lindbom L, Ribbing J, Jonsson EN. Perl-speaks-NONMEM (PsN)--a Perl module for NONMEM related programming. Comput Methods Programs Biomed. 2004;75:85–94. doi: 10.1016/j.cmpb.2003.11.003. [DOI] [PubMed] [Google Scholar]
- 22.Hooker AC, Staatz CE, Karlsson MO. Conditional weighted residuals (CWRES): a model diagnostic for the FOCE method. Pharm Res. 2007;24:2187–2197. doi: 10.1007/s11095-007-9361-x. [DOI] [PubMed] [Google Scholar]
- 23.Comets E, Brendel K, Mentre F. Computing normalised prediction distribution errors to evaluate nonlinear mixed-effect models: the npde add-on package for R. Comput Methods Programs Biomed. 2008;90:154–166. doi: 10.1016/j.cmpb.2007.12.002. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.