

Abstract
Introduction
Adenocarcinoma is the most common histologic type of lung cancer. To address advances in oncology, molecular biology, pathology, radiology, and surgery of lung adenocarcinoma, an international multidisciplinary classification was sponsored by the International Association for the Study of Lung Cancer, American Thoracic Society, and European Respiratory Society. This new adenocarcinoma classification is needed to provide uniform terminology and diagnostic criteria, especially for bronchioloalveolar carcinoma (BAC), the overall approach to small nonresection cancer specimens, and for multidisciplinary strategic management of tissue for molecular and immunohistochemical studies.
Methods
An international core panel of experts representing all three societies was formed with oncologists/pulmonologists, pathologists, radiologists, molecular biologists, and thoracic surgeons. A systematic review was performed under the guidance of the American Thoracic Society Documents Development and Implementation Committee. The search strategy identified 11,368 citations of which 312 articles met specified eligibility criteria and were retrieved for full text review. A series of meetings were held to discuss the development of the new classification, to develop the recommendations, and to write the current document. Recommendations for key questions were graded by strength and quality of the evidence according to the Grades of Recommendation, Assessment, Development, and Evaluation approach.
Results
The classification addresses both resection specimens, and small biopsies and cytology. The terms BAC and mixed subtype adenocarcinoma are no longer used. For resection specimens, new concepts are introduced such as adenocarcinoma in situ (AIS) and minimally invasive adenocarcinoma (MIA) for small solitary adenocarcinomas with either pure lepidic growth (AIS) or predominant lepidic growth with ≤5 mm invasion (MIA) to define patients who, if they undergo complete resection, will have 100% or near 100% disease-specific survival, respectively. AIS and MIA are usually nonmucinous but rarely may be mucinous. Invasive adenocarcinomas are classified by predominant pattern after using comprehensive histologic subtyping with lepidic (formerly most mixed subtype tumors with nonmucinous BAC), acinar, papillary, and solid patterns; micropapillary is added as a new histologic subtype. Variants include invasive mucinous adenocarcinoma (formerly mucinous BAC), colloid, fetal, and enteric adenocarcinoma. This classification provides guidance for small biopsies and cytology specimens, as approximately 70% of lung cancers are diagnosed in such samples. Non-small cell lung carcinomas (NSCLCs), in patients with advanced-stage disease, are to be classified into more specific types such as adenocarcinoma or squamous cell carcinoma, whenever possible for several reasons: (1) adenocarcinoma or NSCLC not otherwise specified should be tested for epidermal growth factor receptor (EGFR) mutations as the presence of these mutations is predictive of responsiveness to EGFR tyrosine kinase inhibitors, (2) adenocarcinoma histology is a strong predictor for improved outcome with pemetrexed therapy compared with squamous cell carcinoma, and (3) potential life-threatening hemorrhage may occur in patients with squamous cell carcinoma who receive bevacizumab. If the tumor cannot be classified based on light microscopy alone, special studies such as immunohistochemistry and/or mucin stains should be applied to classify the tumor further. Use of the term NSCLC not otherwise specified should be minimized.
Conclusions
This new classification strategy is based on a multidisciplinary approach to diagnosis of lung adenocarcinoma that incorporates clinical, molecular, radiologic, and surgical issues, but it is primarily based on histology. This classification is intended to support clinical practice, and research investigation and clinical trials. As EGFR mutation is a validated predictive marker for response and progression-free survival with EGFR tyrosine kinase inhibitors in advanced lung adenocarcinoma, we recommend that patients with advanced adenocarcinomas be tested for EGFR mutation. This has implications for strategic management of tissue, particularly for small biopsies and cytology samples, to maximize high-quality tissue available for molecular studies. Potential impact for tumor, node, and metastasis staging include adjustment of the size T factor according to only the invasive component (1) pathologically in invasive tumors with lepidic areas or (2) radiologically by measuring the solid component of part-solid nodules.
Keywords: Lung, Adenocarcinoma, Classification, Histologic, Pathology, Oncology, Pulmonary, Radiology, Computed tomography, Molecular, EGFR, KRAS, EML4-ALK, Gene profiling, Gene amplification, Surgery, Limited resection, Bronchioloalveolar carcinoma, Lepidic, Acinar, Papillary, Micropapillary, Solid, Adenocarcinoma in situ, Minimally invasive adenocarcinoma, Colloid, Mucinous cystadenocarcinoma, Enteric, Fetal, Signet ring, Clear cell, Frozen section, TTF-1, p63
RATIONALE FOR A CHANGE IN THE APPROACH TO CLASSIFICATION OF LUNG ADENOCARCINOMA
Lung cancer is the most frequent cause of major cancer incidence and mortality worldwide.1,2 Adenocarcinoma is the most common histologic subtype of lung cancer in most countries, accounting for almost half of all lung cancers.3 A widely divergent clinical, radiologic, molecular, and pathologic spectrum exists within lung adenocarcinoma. As a result, confusion exists, and studies are difficult to compare. Despite remarkable advances in understanding of this tumor in the past decade, there remains a need for universally accepted criteria for adenocarcinoma subtypes, in particular tumors formerly classified as bronchioloalveolar carcinoma (BAC).4,5 As enormous resources are being spent on trials involving molecular and therapeutic aspects of adenocarcinoma of the lung, the development of standardized criteria is of great importance and should help advance the field, increasing the impact of research, and improving patient care. This classification is needed to assist in determining patient therapy and predicting outcome.
NEED FOR A MULTIDISCIPLINARY APPROACH TO DIAGNOSIS OF LUNG ADENOCARCINOMA
One of the major outcomes of this project is the recognition that the diagnosis of lung adenocarcinoma requires a multidisciplinary approach. The classifications of lung cancer published by the World Health Organization (WHO) in 1967, 1981, and 1999 were written primarily by pathologists for pathologists.5–7 Only in the 2004 revision, relevant genetics and clinical information were introduced.4 Nevertheless, because of remarkable advances over the last 6 years in our understanding of lung adenocarcinoma, particularly in area of medical oncology, molecular biology, and radiology, there is a pressing need for a revised classification, based not on pathology alone, but rather on an integrated multidisciplinary platform. In particular, there are two major areas of interaction between specialties that are driving the need for our multidisciplinary approach to classification of lung adenocarcinoma: (1) in patients with advanced non-small cell lung cancer, recent progress in molecular biology and oncology has led to (a) discovery of epidermal growth factor receptor (EGFR) mutation and its prediction of response to EGFR tyrosine kinase inhibitors (TKIs) in adenocarcinoma patients8–11 and (b) the requirement to exclude a diagnosis of squamous cell carcinoma to determine eligibility patients for treatment with pemetrexed, (because of improved efficacy)12–15 or bevacizumab (because of toxicity)16,17 and (2) the emergence of radiologic-pathologic correlations between ground-glass versus solid or mixed opacities seen by computed tomography (CT) and BAC versus invasive growth by pathology have opened new opportunities for imaging studies to be used by radiologists, pulmonologists, and surgeons for predicting the histologic subtype of adenocarcinomas,18–21 patient prognosis,18–23 and improve preoperative assessment for choice of timing and type of surgical intervention.18–26
Although histologic criteria remain the foundation of this new classification, this document has been developed by pathologists in collaboration with clinical, radiology, molecular, and surgical colleagues. This effort has led to the development of terminology and criteria that not only define pathologic entities but also communicate critical information that is relevant to patient management (Tables 1 and 2). The classification also provides recommendations on strategic handling of specimens to optimize the amount of information to be gleaned. The goal is not only longer to solely provide the most accurate diagnosis but also to manage the tissue in a way that immunohistochemical and/or molecular studies can be performed to obtain predictive and prognostic data that will lead to improvement in patient outcomes.
TABLE 1.
IASLC/ATS/ERS Classification of Lung Adenocarcinoma in Resection Specimens
| Preinvasive lesions |
| Atypical adenomatous hyperplasia |
| Adenocarcinoma in situ (≤3 cm formerly BAC) |
| Nonmucinous |
| Mucinous |
| Mixed mucinous/nonmucinous |
| Minimally invasive adenocarcinoma (≤3 cm lepidic predominant tumor with ≤5 mm invasion) |
| Nonmucinous |
| Mucinous |
| Mixed mucinous/nonmucinous |
| Invasive adenocarcinoma |
| Lepidic predominant (formerly nonmucinous BAC pattern, with >5 mm invasion) |
| Acinar predominant |
| Papillary predominant |
| Micropapillary predominant |
| Solid predominant with mucin production |
| Variants of invasive adenocarcinoma |
| Invasive mucinous adenocarcinoma (formerly mucinous BAC) |
| Colloid |
| Fetal (low and high grade) |
| Enteric |
BAC, bronchioloalveolar carcinoma; IASLC, International Association for the Study of Lung Cancer; ATS, American Thoracic Society; ERS, European Respiratory Society.
TABLE 2.
Proposed IASLC/ATS/ERS Classification for Small Biopsies/Cytology
| 2004 WHO Classification | SMALL BIOPSY/CYTOLOGY: IASLC/ATS/ERS |
|---|---|
| ADENOCARCINOMA Mixed subtype Acinar Papillary Solid |
Morphologic adenocarcinoma patterns clearly present: Adenocarcinoma, describe identifiable patterns present (including micropapillary pattern not included in 2004 WHO classification) Comment: If pure lepidic growth - mention an invasive component cannot be excluded in this small specimen |
| Bronchioloalveolar carcinoma (nonmucinous) | Adenocarcinoma with lepidic pattern (if pure, add note: an invasive component cannot be excluded) |
| Bronchioloalveolar carcinoma (mucinous) | Mucinous adenocarcinoma (describe patterns present) |
| Fetal | Adenocarcinoma with fetal pattern |
| Mucinous (colloid) | Adenocarcinoma with colloid pattern |
| Signet ring | Adenocarcinoma with (describe patterns present) and signet ring features |
| Clear cell | Adenocarcinoma with (describe patterns present) and clear cell features |
| No 2004 WHO counterpart - most will be solid adenocarcinomas |
Morphologic adenocarcinoma patterns not present (supported by special stains): Non-small cell carcinoma, favor adenocarcinoma |
| SQUAMOUS CELL CARCINOMA Papillary Clear cell Small cell Basaloid |
Morphologic squamous cell patterns clearly present: Squamous cell carcinoma |
| No 2004 WHO counterpart |
Morphologic squamous cell patterns not present (supported by stains): Non-small cell carcinoma, favor squamous cell carcinoma |
| SMALL CELL CARCINOMA | Small cell carcinoma |
| LARGE CELL CARCINOMA | Non-small cell carcinoma, not otherwise specified (NOS) |
| Large cell neuroendocrine carcinoma (LCNEC) | Non-small cell carcinoma with neuroendocrine (NE) morphology (positive NE markers), possible LCNEC |
| Large cell carcinoma with NE morphology (LCNEM) | Non-small cell carcinoma with NE morphology (negative NE markers) - see comment Comment: This is a non-small cell carcinoma where LCNEC is suspected, but stains failed to demonstrate NE differentiation. |
| ADENOSQUAMOUS CARCINOMA |
Morphologic squamous cell and adenocarcinoma patterns present: Non-small cell carcinoma, with squamous cell and adenocarcinoma patterns Comment: this could represent adenosquamous carcinoma. |
| No counterpart in 2004 WHO classification |
Morphologic squamous cell or adenocarcinoma patterns not present but immunostains favor separate glandular and adenocarcinoma components Non-small cell carcinoma, NOS, (specify the results of the immunohistochemical stains and the interpretation) Comment: this could represent adenosquamous carcinoma. |
| Sarcomatoid carcinoma | Poorly differentiated NSCLC with spindle and/or giant cell carcinoma (mention if adenocarcinoma or squamous carcinoma are present) |
IASLC, International Association for the Study of Lung Cancer; ATS, American Thoracic Society; ERS, European Respiratory Society; WHO, World Health Organization: NSCLC, non-small cell lung cancer; IHC, immunohistochemistry; TTF, thyroid transcription factor.
For the first time, this classification addresses an approach to small biopsies and cytology in lung cancer diagnosis (Table 2). Recent data regarding EGFR mutation predicting responsiveness to EGFR-TKIs,8–11 toxicities,16 and therapeutic efficacy12–15 have established the importance of distinguishing squamous cell carcinoma from adenocarcinoma and non-small cell lung carcinoma (NSCLC) not otherwise specified (NOS) in patients with advanced lung cancer. Approximately 70% of lung cancers are diagnosed and staged by small biopsies or cytology rather than surgical resection specimens, with increasing use of transbronchial needle aspiration (TBNA), endobronchial ultrasound-guided TBNA and esophageal ultrasound-guided needle aspiration.27 Within the NSCLC group, most pathologists can identify well- or moderately differentiated squamous cell carcinomas or adenocarcinomas, but specific diagnoses are more difficult with poorly differentiated tumors. Nevertheless, in small biopsies and/or cytology specimens, 10 to 30% of specimens continue to be diagnosed as NSCLC-NOS.13,28,29
Proposed terminology to be used in small biopsies is summarized in Table 2. Pathologists need to minimize the use of the term NSCLC or NSCLC-NOS on small samples and aspiration and exfoliative cytology, providing as specific a histologic classification as possible to facilitate the treatment approach of medical oncologists.30
Unlike previous WHO classifications where the primary diagnostic criteria for as many tumor types as possible were based on hematoxylin and eosin (H&E) examination, this classification emphasizes the use and integration of immunohistochemical (i.e., thyroid transcription factor [TTF-1]/p63 staining), histochemical (i.e., mucin staining), and molecular studies, as specific therapies are driven histologic subtyping. Although these techniques should be used whenever possible, it is recognized that this may not always be possible, and thus, a simpler approach is also provided when only H&E-stained slides are available, so this classification may be applicable even in a low resource setting.
METHODOLOGY
Objectives
This international multidisciplinary classification has been produced as a collaborative effort by the International Association for the Study of Lung Cancer (IASLC), the American Thoracic Society (ATS), and the European Respiratory Society. The purpose is to provide an integrated clinical, radiologic, molecular, and pathologic approach to classification of the various types of lung adenocarcinoma that will help to define categories that have distinct clinical, radiologic, molecular, and pathologic characteristics. The goal is to identify prognostic and predictive factors and therapeutic targets.
Participants
Panel members included thoracic medical oncologists, pulmonologists, radiologists, molecular biologists, thoracic surgeons, and pathologists. The supporting associations nominated panel members. The cochairs were selected by the IASLC. Panel members were selected because of special interest and expertise in lung adenocarcinoma and to provide an international and multidisciplinary representation. The panel consisted of a core group (author list) and a reviewer group (Appendix 1, see Supplemental Digital Content 1 available at http://links.lww.com/JTO/A59, affiliations for coauthors are listed in appendix).
Evidence
The panel performed a systematic review with guidance by members of the ATS Documents Development and Implementation Committee. Key questions for this project were generated by each specialty group, and a search strategy was developed (Appendix 2, see Supplemental Digital Content 2 available at http://links.lww.com/JTO/A60). Searches were performed in June 2008 with an update in June 2009 resulting in 11,368 citations. These were reviewed to exclude articles that did not have any relevance to the topic of lung adenocarcinoma classification. The remaining articles were evaluated by two observers who rated them by a predetermined set of eligibility criteria using an electronic web-based survey program (www.surveymonkey.com) to collect responses.31 This process narrowed the total number of articles to 312 that were reviewed in detail for a total of 141 specific features, including 17 study characteristics, 35 clinical, 48 pathologic, 16 radiologic, 16 molecular, and nine surgical (Appendix 2). These 141 features were summarized in an electronic database that was distributed to members of the core panel, including the writing committee. Articles chosen for specific data summaries were reviewed, and based on analysis of tables from this systematic review, recommendations were made according to the Grades of Recommendation, Assessment, Development, and Evaluation (GRADE).32–37 Throughout the rest of the document, the term GRADE (spelled in capital letters) must be distinguished from histologic grade, which is a measure of pathologic tumor differentiation. The GRADE system has two major components: (1) grading the strength of the recommendation and (2) evaluating the quality of the evidence.32 The strength of recommendations is based on weighing estimates of benefits versus downsides. Evidence was rated as high, moderate, or low or very low.32 The quality of the evidence expresses the confidence in an estimate of effect or an association and whether it is adequate to support a recommendation. After review of all articles, a writing committee met to develop the recommendations with each specialty group proposing the recommendations, votes for or against the recommendation, and modifications were conducted after multidisciplinary discussion. If randomized trials were available, we started by assuming high quality but down-graded the quality when there were serious methodological limitations, indirectness in population, inconsistency in results, imprecision in estimates, or a strong suspicion of publication bias. If well-done observational studies were available, low-quality evidence was assumed, but the quality was upgraded when there was a large treatment effect or a large association, all plausible residual confounders would diminish the effects, or if there was a dose-response gradient.36 We developed considerations for good practice related to interventions that usually represent necessary and standard procedures of health care system—such as history taking and physical examination helping patients to make informed decisions, obtaining written consent, or the importance of good communication—when we considered them helpful. In that case, we did not perform a grading of the quality of evidence or strength of the recommendations.38
Meetings
Between March 2008 and December 2009, a series of meetings were held, mostly at Memorial Sloan Kettering Cancer Center, in New York, NY, to discuss issues related to lung adenocarcinoma classification and to formulate this document. The core group established a uniform and consistent approach to the proposed types of lung adenocarcinoma.
Validation
Separate projects were initiated by individuals involved with this classification effort in an attempt to develop data to test the proposed system. These included projects on small biopsies,39,40 histologic grading,41–43 stage I adenocarcinomas,44 small adenocarcinomas from Japan, international multiple pathologist project on reproducibility of recognizing major histologic patterns of lung adenocarcinoma,45 molecular-histologic correlations, and radiologic-pathologic correlation focused on adenocarcinoma in situ (AIS), and minimally invasive adenocarcinoma (MIA).
The new proposals in this classification are based on the best available evidence at the time of writing this document. Nevertheless, because of the lack of universal diagnostic criteria in the literature, there is a need for future validation studies based on these standardized pathologic criteria with clinical, molecular, radiologic, and surgical correlations.
PATHOLOGIC CLASSIFICATION
Histopathology is the backbone of this classification, but lung cancer diagnosis is a multidisciplinary process requiring correlation with clinical, radiologic, molecular, and surgical information. Because of the multidisciplinary approach in developing this classification, we are recommending significant changes that should improve the diagnosis and classification of lung adenocarcinoma, resulting in therapeutic benefits.
Even after publication of the 1999 and 2004 WHO classifications,4,5 the former term BAC continues to be used for a broad spectrum of tumors including (1) solitary small noninvasive peripheral lung tumors with a 100% 5-year survival,46 (2) invasive adenocarcinomas with minimal invasion that have approximately 100% 5-year survival,47,48 (3) mixed subtype invasive adenocarcinomas,49 –53 (4) mucinous and nonmucinous subtypes of tumors formerly known as BAC,50 –52,54,55 and (5) widespread advanced disease with a very low survival rate.4,5 The consequences of confusion from the multiple uses of the former BAC term in the clinical and research arenas have been the subject of many reviews and editorials and are addressed throughout this document.55– 61
Pathology Recommendation 1
We recommend discontinuing the use of the term “BAC.” Strong recommendation, low-quality evidence.
Throughout this article, the term BAC (applicable to multiple places in the new classification, Table 3), will be referred to as “former BAC.” We understand this will be a major adjustment and suggest initially that when the new proposed terms are used, it will be accompanied in parentheses by “(formerly BAC).” This transition will impact not only clinical practice and research but also cancer registries future analyses of registry data.
TABLE 3.
Categories of New Adenocarcinoma Classification Where Former BAC Concept was Used
|
BAC, bronchioloalveolar carcinoma.
CLASSIFICATION FOR RESECTION SPECIMENS
Multiple studies have shown that patients with small solitary peripheral adenocarcinomas with pure lepidic growth may have 100% 5-year disease-free survival.46,62–68 In addition, a growing number of articles suggest that patients with lepidic predominant adenocarcinomas (LPAs) with minimal invasion may also have excellent survival.47,48 Recent work has demonstrated that more than 90% of lung adenocarcinomas fall into the mixed subtype according to the 2004 WHO classification, so it has been proposed to use comprehensive histologic subtyping to make a semiquantitative assessment of the percentages of the various histologic components: acinar, papillary, micropapillary, lepidic, and solid and to classify tumors according to the predominant histologic subtype.69 This has demonstrated an improved ability to address the complex histologic heterogeneity of lung adenocarcinomas and to improve molecular and prognostic correlations.69
The new proposed lung adenocarcinoma classification for resected tumors is summarized in Table 1.
Preinvasive Lesions
In the 1999 and 2004 WHO classifications, atypical adenomatous hyperplasia (AAH) was recognized as a preinvasive lesion for lung adenocarcinoma. This is based on multiple studies documenting these lesions as incidental findings in the adjacent lung parenchyma in 5 to 23% of resected lung adenocarcinomas70–74 and a variety of molecular findings that demonstrate a relationship to lung adenocarcinoma including clonality,75,76 KRAS mutation,77,78 KRAS polymorphism,79 EGFR mutation,80 p53 expression,81 loss of heterozygosity,82 methylation,83 telomerase overexpression,84 eukaryotic initiation factor 4E expression,85 epigenetic alterations in the Wnt pathway,86 and FHIT expression.87 Depending on the extensiveness of the search, AAH may be multiple in up to 7% of resected lung adenocarcinomas.71,88
A major change in this classification is the official recognition of AIS, as a second preinvasive lesion for lung adenocarcinoma in addition to AAH. In the category of preinvasive lesions, AAH is the counterpart to squamous dysplasia and AIS the counterpart to squamous cell carcinoma in situ.
Atypical Adenomatous Hyperplasia
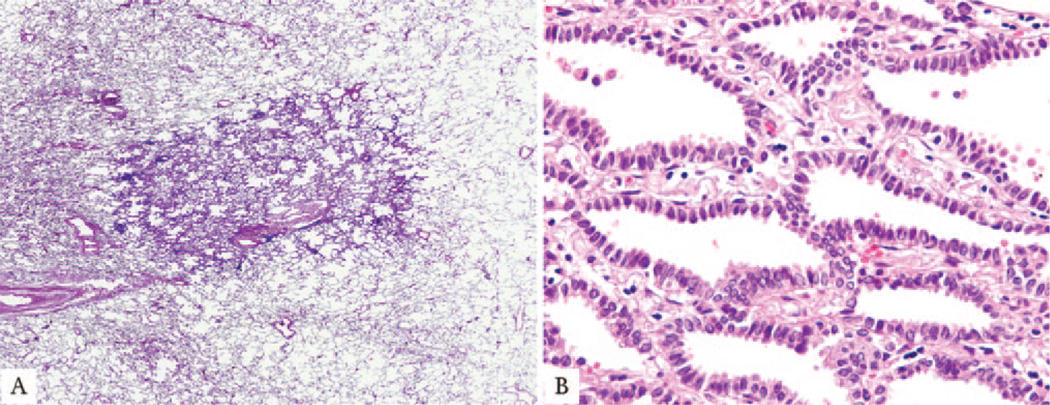
AAH is a localized, small (usually 0.5 cm or less) proliferation of mildly to moderately atypical type II pneumocytes and/or Clara cells lining alveolar walls and sometimes, respiratory bronchioles (Figures 1A, B).4,89,90 Gaps are usually seen between the cells, which consist of rounded, cuboidal, low columnar, or “peg” cells with round to oval nuclei (Figure 1B). Intranuclear inclusions are frequent. There is a continuum of morphologic changes between AAH and AIS.4,89,90 A spectrum of cellularity and atypia occurs in AAH. Although some have classified AAH into low- and high-grade types,84,91 grading is not recommended.4 Distinction between more cellular and atypical AAH and AIS can be difficult histologically and impossible cytologically.
Figure 1.

Atypical adenomatous hyperplasia. A, This 3-mm nodular lesion consists of atypical pneumocytes proliferating along preexisting alveolar walls. There is no invasive component. B, The slightly atypical pneumocytes are cuboidal and show gaps between the cells. Nuclei are hyperchromatic, and a few show nuclear enlargement and multinucleation.
AIS, Nonmucinous, and/or Mucinous
AIS (one of the lesions formerly known as BAC) is a localized small (≤3 cm) adenocarcinoma with growth restricted to neoplastic cells along preexisting alveolar structures (lepidic growth), lacking stromal, vascular, or pleural invasion. Papillary or micropapillary patterns and intraalveolar tumor cells are absent. AIS is subdivided into nonmucinous and mucinous variants. Virtually, all cases of AIS are nonmucinous, consisting of type II pneumocytes and/or Clara cells (Figures 2A, B). There is no recognized clinical significance to the distinction between type II or Clara cells, so this morphologic separation is not recommended. The rare cases of mucinous AIS consist of tall columnar cells with basal nuclei and abundant cytoplasmic mucin; sometimes they resemble goblet cells (Figures 3A, B). Nuclear atypia is absent or inconspicuous in both nonmucinous and mucinous AIS (Figures 2B and 3B). Septal widening with sclerosis is common in AIS, particularly the nonmucinous variant.
Figure 2.
Nonmucinous adenocarcinoma in situ. A, This circumscribed nonmucinous tumor grows purely with a lepidic pattern. No foci of invasion or scarring are seen. B, The tumor shows atypical pneumocytes proliferating along the slightly thickened, but preserved, alveolar walls.
Figure 3.
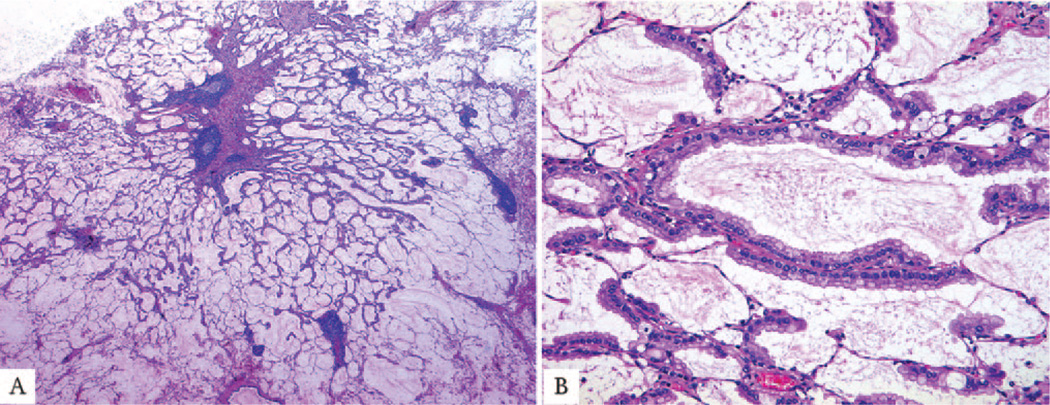
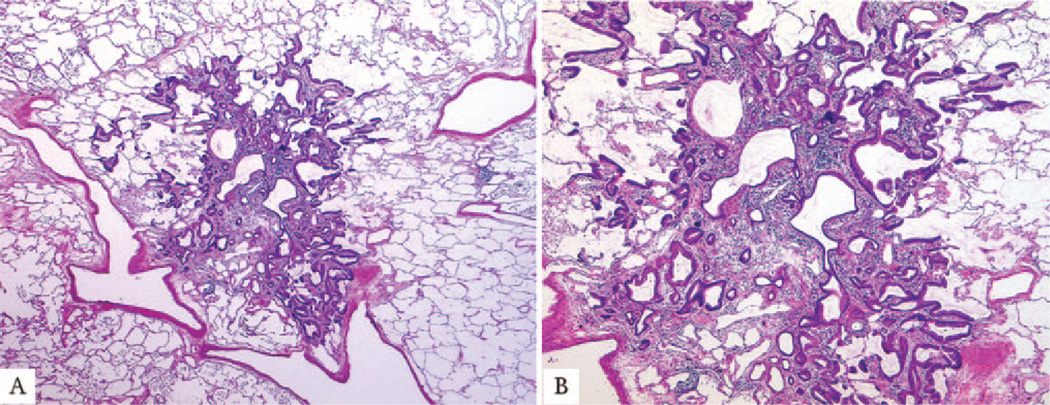
Mucinous adenocarcinoma in situ. A, This mucinous AIS consists of a nodular proliferation of mucinous columnar cells growing in a purely lepidic pattern. Although there is a small central scar, no stromal or vascular invasion is seen. B, The tumor cells consist of cuboidal to columnar cells with abundant apical mucin and small basally oriented nuclei. AIS, adenocarcinoma in situ.
Tumors that meet criteria for AIS have formerly been classified as BAC according to the strict definition of the 1999 and 2004 WHO classifications and type A and type B adenocarcinoma according to the 1995 Noguchi classification.4,46 Multiple observational studies on solitary lung adenocarcinomas with pure lepidic growth, smaller than either 2 or 3 cm have documented 100% disease-free survival.46,62–68 Although most of these tumors are nonmucinous, 2 of the 28 tumors reported by Noguchi as types A and B in the 1995 study were mucinous.46 Small size (≤3 cm) and a discrete circumscribed border are important to exclude cases with miliary spread into adjacent lung parenchyma and/or lobar consolidation, particularly for mucinous AIS.
Pathology Recommendation 2
For small (≤3 cm), solitary adenocarcinomas with pure lepidic growth, we recommend the term “Adenocarcinoma in situ” that defines patients who should have 100% disease-specific survival, if the lesion is completely resected (strong recommendation, moderate quality evidence).
Remark: Most AIS are nonmucinous, rarely are they mucinous.
MIA, Nonmucinous, and/or Mucinous
MIA is a small, solitary adenocarcinoma (≤3 cm), with a predominantly lepidic pattern and ≤5 mm invasion in greatest dimension in any one focus.47,48,92 MIA is usually nonmucinous (Figures 4A–C) but rarely may be mucinous (Figures 5A, B).44 MIA is, by definition, solitary and discrete. The criteria for MIA can be applied in the setting of multiple tumors only if the other tumors are regarded as synchronous primaries rather than intrapulmonary metastases.
Figure 4.
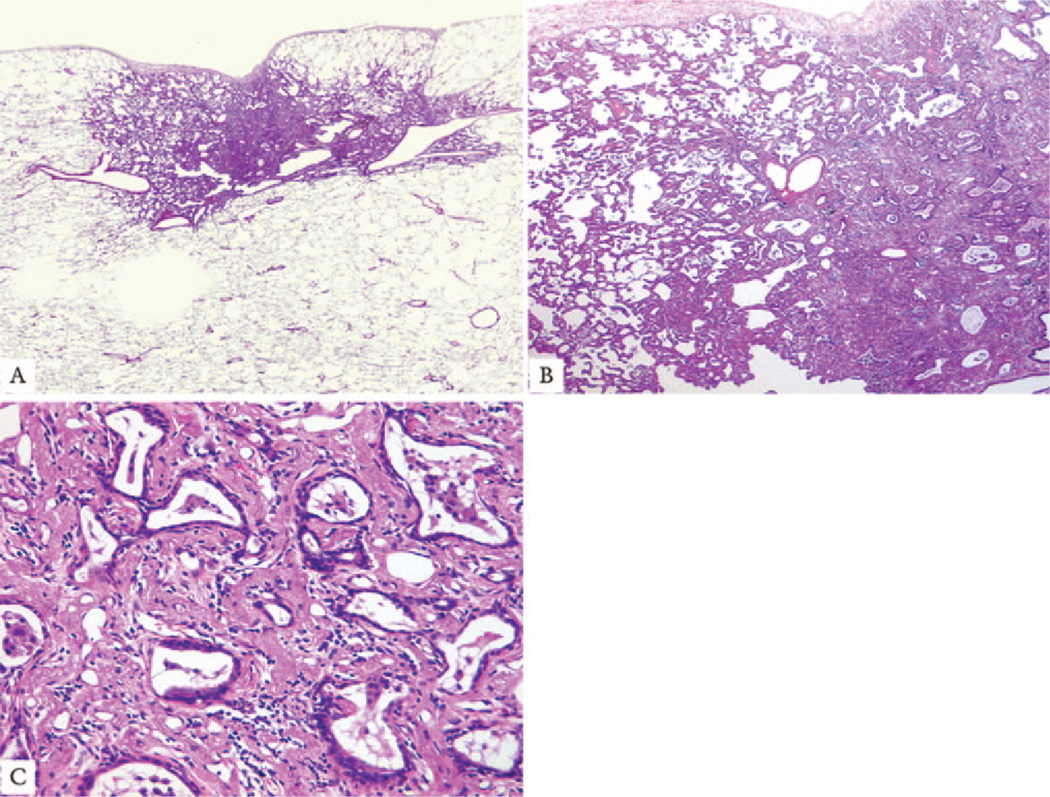
Nonmucinous minimally invasive adenocarcinoma. A, This subpleural adenocarcinoma tumor consists primarily of lepidic growth with a small (<0.5 cm) central area of invasion. B, To the left is the lepidic pattern and on the right is an area of acinar invasion. C, These acinar glands are invading in the fibrous stroma.
Figure 5.
Mucinous minimally invasive adenocarcinoma. A, This mucinous MIA consists of a tumor showing lepidic growth and a small (<0.5 cm) area of invasion. B, The tumor cells consist of mucinous columnar cells growing mostly in a lepidic pattern along the surface of alveolar walls. The tumor invades the areas of stromal fibrosis in an acinar pattern. MIA, minimally invasive adenocarcinoma.
The invasive component to be measured in MIA is defined as follows: (1) histological subtypes other than a lepidic pattern (i.e., acinar, papillary, micropapillary, and/or solid) or (2) tumor cells infiltrating myofibroblastic stroma. MIA is excluded if the tumor (1) invades lymphatics, blood vessels, or pleura or (2) contains tumor necrosis. If multiple microinvasive areas are found in one tumor, the size of the largest invasive area should be measured in the largest dimension, and it should be ≤5 mm in size. The size of invasion is not the summation of all such foci, if more than one occurs. If the manner of histologic sectioning of the tumor makes it impossible to measure the size of invasion, an estimate of invasive size can be made by multiplying the total percentage of the invasive (nonlepidic) components times the total tumor size.
Evidence for a category of MIA with 100% disease-free survival can be found in the 1995 article by Noguchi et al., where vascular or pleural invasion was found in 10% of the small solitary lung adenocarcinomas that otherwise met the former definition of pure BAC. Even these focally invasive tumors also showed 100% disease-free survival.46 Subsequent articles by Suzuki et al. and Sakurai et al.19,21 defined subsets of small lung adenocarcinomas with 100% disease-free survival using scar size less than 5 mm and stromal invasion in the area of bronchioloalveolar growth, respectively. More recently, articles by Yim et al., Borczuk et al., and Maeshima et al.47,48,92 have described patients with MIA defined similar to the above criteria, and these have demonstrated near 100% disease specific or very favorable overall survival. There is very limited data regarding mucinous MIA; however, this seems to exist. A mucinous MIA with a minor mixture of a nonmucinous component is being reported.44 The recent report by Sawada et al.93 of localized mucinous BAC may have included a few cases of mucinous AIS or MIA, but details of the pathology are not specific enough to be certain. A recent series of surgically resected solitary mucinous BAC did not document histologically whether focal invasion was present or not, so AIS versus MIA status cannot be determined, but all eight patients with tumors measuring ≤3 cm had 100% overall 5-year survival rates.94 Presentation as a solitary mass, small size, and a discrete circumscribed border is important to exclude cases of miliary involvement of adjacent lung parenchyma and/or lobar consolidation, particularly for mucinous AIS.
Pathology Recommendation 3
For small (≤3 cm), solitary, adenocarcinomas with predominant lepidic growth and small foci of invasion measuring ≤0.5 cm, we recommend a new concept of “Minimally invasive adenocarcinoma” to define patients who have near 100%, disease-specific survival, if completely resected (strong recommendation, low-quality evidence).
Remark: Most MIA are nonmucinous, rarely are they mucinous.
Tumor Size and Specimen Processing Issues for AIS and MIA
The diagnosis of AIS or MIA cannot be firmly established without entire histologic sampling of the tumor. If tumor procurement is performed, it should be done strategically as discussed in the molecular section.
Because most of the literature on the topic of AIS and MIA deal with tumors 2.0 or 3.0 cm or less, there is insufficient evidence to support that 100% disease-free survival can occur in completely resected, solitary tumors suspected to be AIS or MIA that are larger than 3.0 cm. Until data validate 100% disease-free survival for completely resected, solitary, adenocarcinomas larger than 3.0 cm suspected to be AIS or MIA after complete sampling, the term “lepidic predominant adenocarcinoma, suspect AIS or MIA” is suggested. In such a tumor larger than 3.0 cm, particularly if it has not been completely sampled, the term “lepidic predominant adenocarcinoma” is best applied with a comment that the clinical behavior is uncertain and/or that an invasive component cannot be excluded.
Invasive Adenocarcinoma
As invasive adenocarcinomas represent more than 70 to 90% of surgically resected lung cases, one of the most important aspects of this classification is to present a practical way to address these tumors that are composed of a complex heterogeneous mixture of histologic subtypes. This complex mixture of histologic subtypes has presented one of the greatest challenges to classification of invasive lung adenocarcinomas. In recent years, multiple independent research groups have begun to classify lung adenocarcinomas according to the most predominant subtype.43,44,69,95–102 This approach provides better stratification of the “mixed subtype” lung adenocarcinomas according to the 1999/2004 WHO Classifications and has allowed for novel correlations between histologic subtypes and both molecular and clinical features.43,44,69,95–102
In the revised classification, the term “predominant” is appended to all categories of invasive adenocarcinoma, as most of these tumors consist of mixtures of the histologic subtypes (Figures 6A–C). This replaces the use of the term adenocarcinoma, mixed subtype. Semiquantitative recording of the patterns in 5% increments encourages the observer to identify all patterns that may be present, rather than focusing on a single pattern (i.e., lepidic growth). This method provides a basis for choosing the predominant pattern. Although most previous studies on this topic used 10% increments, using 5% allows for greater flexibility in choosing a predominant subtype when tumors have two patterns with relatively similar percentages; it also avoids the need to use 10% for small amounts of components that may be prognostically important such as micropapillary or solid patterns. Recording of these percentages also makes it clear to the reader of a report when a tumor has relatively even mixtures of several patterns versus a single dominant pattern. In addition, it provides a way to compare the histology of multiple adenocarcinomas (see later).102 This approach may also provide a basis for architectural grading of lung adenocarcinomas.43 A recent reproducibility study of classical and difficult selected images of the major lung adenocarcinoma subtypes circulated among a panel of 26 expert lung cancer pathologists documented kappa values of 0.77 ± 0.07 and 0.38 ± 0.14, respectively.45 This study did not test recognition of predominant subtype.
Figure 6.
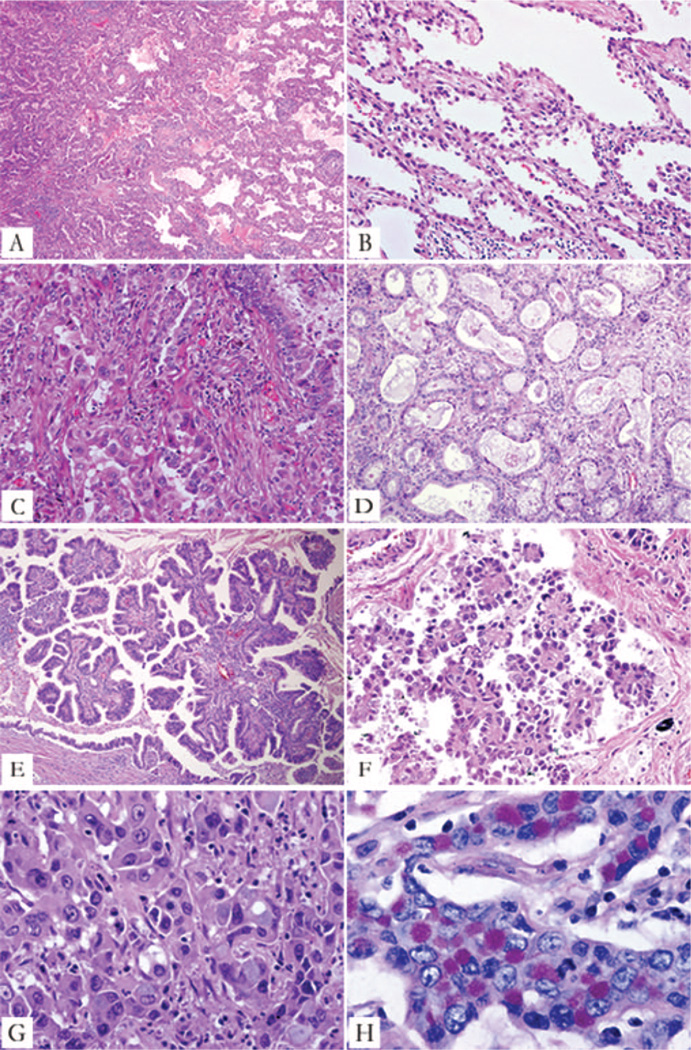
Major histologic patterns of invasive adenocarcinoma. A, Lepidic predominant pattern with mostly lepidic growth (right) and a smaller area of invasive acinar adenocarcinoma (left). B, Lepidic pattern consists of a proliferation type II pneumocytes and Clara cells along the surface alveolar walls. C, Area of invasive acinar adenocarcinoma (same tumor as in A and B). D, Acinar adenocarcinoma consists of round to oval-shaped malignant glands invading a fibrous stroma. E, Papillary adenocarcinoma consists of malignant cuboidal to columnar tumor cells growing on the surface of fibrovascular cores. F, Micropapillary adenocarcinoma consists of small papillary clusters of glandular cells growing within this airspace, most of which do not show fibrovascular cores. G, Solid adenocarcinoma with mucin consisting of sheets of tumor cells with abundant cytoplasm and mostly vesicular nuclei with several conspicuous nucleoli. No acinar, papillary, or lepidic patterns are seen, but multiple cells have intracytoplasmic basophilic globules that suggest intracytoplasmic mucin. H, Solid adenocarcinoma with mucin. Numerous intracytoplasmic droplets of mucin are highlighted with this DPAS stain. DPAS, diastase-periodic acid Schiff.
Pathology Recommendation 4
For invasive adenocarcinomas, we suggest comprehensive histologic subtyping be used to assess histologic patterns semiquantitatively in 5% increments, choosing a single predominant pattern. Individual tumors are then classified according to the predominant pattern and the percentages of the subtypes are also reported (weak recommendation, low-quality evidence).
Histologic Comparison of Multiple Adenocarcinomas and Impact on Staging
Comprehensive histologic subtyping can be useful in comparing multiple lung adenocarcinomas to distinguish multiple primary tumors from intrapulmonary metastases. This has a great impact on staging for patients with multiple lung adenocarcinomas. Recording the percentages of the various histologic types in 5% increments, not just the most predominant type, allows these data to be used to compare multiple adenocarcinomas, particularly if the slides of a previous tumor are not available at the time of review of the additional lung tumors.102 In addition to comprehensive histologic subtyping, other histologic features of the tumors such as cytologic (clear cell or signet ring features) or stromal (desmoplasia or inflammation) characteristics may be helpful to compare multiple tumors.102
Pathology Recommendation 5
In patients with multiple lung adenocarcinomas, we suggest comprehensive histologic subtyping may facilitate in the comparison of the complex, heterogeneous mixtures of histologic patterns to determine whether the tumors are metastases or separate synchronous or metachronous primaries (weak recommendation, low-quality evidence).
LPA typically consists of bland pneumocytic cells (type II pneumocytes or Clara cells) growing along the surface of alveolar walls similar to the morphology defined in the above section on AIS and MIA (Figures 6A, B). Invasive adenocarcinoma is present in at least one focus measuring more than 5 mm in greatest dimension. Invasion is defined as (1) histological subtypes other than a lepidic pattern (i.e., acinar, papillary, micropapillary, and/or solid) or (2) myofibroblastic stroma associated with invasive tumor cells (Figure 6C). The diagnosis of LPA rather than MIA is made if the tumor (1) invades lymphatics, blood vessels, or pleura or (2) contains tumor necrosis. It is understood that lepidic growth can occur in metastatic tumors and invasive mucinous adenocarcinomas. Nevertheless, the specific term “Lepidic predominant adenocarcinoma (LPA)” in this classification defines a nonmucinous adenocarcinoma that has lepidic growth as its predominant component, and these tumors are now separated from invasive mucinous adenocarcinoma. The term LPA should not be used in the context of invasive mucinous adenocarcinoma with predominant lepidic growth.
In the categories of mixed subtype in the 1999/2004 WHO classifications and type C in the Noguchi classification,4,46 there was no assessment of the percentage of lepidic growth (former BAC pattern), so in series diagnosed according to these classification systems, most of the LPAs are buried among a heterogeneous group of tumors that include predominantly invasive adenocarcinomas. Nevertheless, several studies have shown lepidic growth to be associated with more favorable survival in small solitary resected lung adenocarcinomas with an invasive component.47,64,103–105 One recent study of stage I adenocarcinomas using this approach demonstrated 90% 5-year recurrence free survival.44
Pathology Recommendation 6
For nonmucinous adenocarcinomas previously classified as mixed subtype where the predominant subtype consists of the former nonmucinous BAC, we recommend use of the term LPA and discontinuing the term “mixed subtype” (strong recommendation, low-quality evidence).
Acinar predominant adenocarcinoma shows a majority component of glands, which are round to oval shaped with a central luminal space surrounded by tumor cells (Figure 6D).4 The neoplastic cells and glandular spaces may contain mucin. Acinar structures also may consist of rounded aggregates of tumor cells with peripheral nuclear polarization with central cytoplasm without a clear lumen. AIS with collapse may be difficult to distinguish from the acinar pattern. Nevertheless, when the alveolar architecture is lost and/or myofibroblastic stroma is present, invasive acinar adenocarcinoma is considered present. Cribriform arrangements are regarded as a pattern of acinar adenocarcinoma.106
Papillary predominant adenocarcinoma shows a major component of a growth of glandular cells along central fibrovascular cores (Figure 6E).4 This should be distinguished from tangential sectioning of alveolar walls in AIS. If a tumor has lepidic growth, but the alveolar spaces are filled with papillary structures, the tumor is classified as papillary adenocarcinoma. Myofibroblastic stroma is not needed to diagnose this pattern.
Micropapillary predominant adenocarcinoma has tumor cells growing in papillary tufts, which lack fibrovascular cores (Figure 6F).4 These may appear detached and/or connected to alveolar walls. The tumor cells are usually small and cuboidal with minimal nuclear atypia. Ring-like glandular structures may “float” within alveolar spaces. Vascular invasion and stromal invasion are frequent. Psammoma bodies may be seen.
The micropapillary pattern of lung adenocarcinoma was cited in the 2004 WHO classification in the discussion,4 but there were too few publications on this topic to introduce it as a formal histologic subtype.107–109 Although most of the studies have used a very low threshold for classification of adenocarcinomas as micropapillary, including as low as 1 to 5%,108,109 it has recently been demonstrated that tumors classified as micropapillary according to the predominant subtype also have a poor prognosis similar to adenocarcinomas with a predominant solid subtype.44 All articles on the topic of micropapillary lung adenocarcinoma in early-stage patients have reported data indicating that this is a poor prognostic subtype.95,108–119 Additional evidence for the aggressive behavior of this histologic pattern is the overrepresentation of the micropapillary pattern in metastases compared with the primary tumors, where it sometimes comprises only a small percentage of the overall tumor.43
Pathology Recommendation 7
In patients with early-stage adenocarcinoma, we recommend the addition of “micropapillary predominant adenocarcinoma,” when applicable, as a major histologic subtype due to its association with poor prognosis (strong recommendation, low-quality evidence).
Solid predominant adenocarcinoma with mucin production shows a major component of polygonal tumor cells forming sheets, which lack recognizable patterns of adenocarcinoma, i.e., acinar, papillary, micropapillary, or lepidic growth (Figure 6G).4 If the tumor is 100% solid, intracellular mucin should be present in at least five tumor cells in each of two high-power fields, confirmed with histochemical stains for mucin (Figure 6H).4 Solid adenocarcinoma must be distinguished from squamous cell carcinomas and large cell carcinomas both of which may show rare cells with intracellular mucin.
Variants
Rationale for Changes in Adenocarcinoma Histologic Variants
Rationale for separation of invasive mucinous adenocarcinoma (formerly mucinous BAC) from nonmucinous adenocarcinomas
Multiple studies indicate that tumors formerly classified as mucinous BAC have major clinical, radiologic, pathologic, and genetic differences from the tumors formerly classified as nonmucinous BAC (Table 4).55,77,120,121,125–127,136,145–148 In particular, these tumors show a very strong correlation with KRAS mutation, whereas nonmucinous adenocarcinomas are more likely to show EGFR mutation and only occasionally KRAS mutation (Table 4). Therefore, in the new classification, these tumors are now separated into different categories (Table 1). The neoplasms formerly termed mucinous BAC, now recognized to have invasive components in the majority of cases, are classified as invasive mucinous adenocarcinoma (formerly mucinous BAC).149
TABLE 4.
Difference between Invasive Mucinous Adenocarcinoma and Nonmucinous Adenocarcinoma In Situ/Minimally Invasive Adenocarcinoma/Lepidic Predominant Adenocarcinoma
| Invasive Mucinous Adenocarcinoma (Formerly Mucinous BAC) |
Nonmucinous AIS/MIA/LPA (Formerly Nonmucinous BAC) |
|
|---|---|---|
| Female | 49/84 (58%)52,120–123 | 101/140 (72%)52,120–123 |
| Smoker | 39/87 (45%)52,120–122,124 | 75/164 (46%)52,120–122,124 |
| Radiographic appearance | Majority consolidation; air bronchogram125 | Majority ground-glass attenuation23,56,58,103,129–134 |
| Frequent multifocal and multilobar presentation56,125–128 | ||
| Cell type | Mucin-filled, columnar, and/or goblet50–52,125,135 | Type II pneumocyte and/or Clara cell50–52,125,135 |
| Phenotype | ||
| CK7 | Mostly positive (~88%)a54,55,136–139 | Positive (~98%)a54,55,136–139 |
| CK20 | Positive (~54%)a54,55,136–139 | Negative (~5%)a54,55,136–139 |
| TTF-1 | Mostly negative (~17%)1a54,55,120,137–139 | Positive (~67%)a54,55,120,137–139 |
| Genotype | ||
| KRAS mutation | Frequent (~76%)a55,94,121,127,140–144 | Some (~13%)a55,121,127,140–144 |
| EGFR mutation | Almost none (~3)a55,121,127,140–142 | Frequent (~45%)a55,121,127,140–142 |
Numbers represent the percentage of cases that are reported to be positive.
BAC, bronchioloalveolar carcinoma; AIS, adenocarcinoma in situ; MIA, minimally invasive adenocarcinoma; LPA, lepidic predominant adenocarcinoma; EGFR, epidermal growth factor receptor; TTF, thyroid transcription factor.
Rationale for including mucinous cystadenocarcinoma in colloid adenocarcinoma
Tumors formerly classified as “Mucinous cystadenocarcinoma” are very rare, and they probably represent a spectrum of colloid adenocarcinoma. Therefore, we suggest that these adenocarcinomas that consist of uni- or oligolocular cystic structures by imaging and/or gross examination be included in the category of colloid adenocarcinoma.150 For such tumors, a comment could be made that the tumor resembles that formerly classified as mucinous cystadenocarcinoma.
Rationale for removing clear cell and signet ring carcinoma as adenocarcinoma subtypes
Clear cell and signet ring cell features are now regarded as cytologic changes that may occur in association with multiple histologic patterns.151,152 Thus, their presence and extent should be recorded, but data are not available that show a clinical significance beyond a strong association with the solid subtype. They are not considered to be specific histologic subtypes, although associations with molecular features are possible such as the recent observation of a solid pattern with more than 10% signet ring cell features in up to 56% of tumors from patients with echinoderm microtubule-associated protein-like 4 (EML4) and anaplastic lymphoma kinase (ALK) gene fusions (EML4-ALK).153
Rationale for adding enteric adenocarcinoma
Enteric adenocarcinoma is added to the classification to draw attention to this rare histologic type of primary lung adenocarcinoma that can share some morphologic and immunohistochemical features with colorectal adenocarcinoma.154 Because of these similarities, clinical evaluation is needed to exclude a gastrointestinal primary. It is not known whether there are any distinctive clinical or molecular features.
Histologic Features
Invasive mucinous adenocarcinoma (formerly mucinous BAC) has a distinctive histologic appearance with tumor cells having a goblet or columnar cell morphology with abundant intracytoplasmic mucin (Figures 7A, B). Cytologic atypia is usually inconspicuous or absent. Alveolar spaces often contain mucin. These tumors may show the same heterogeneous mixture of lepidic, acinar, papillary, micropapillary, and solid growth as in nonmucinous tumors. The clinical significance of reporting semiquantitative estimates of subtype percentages and the predominant histologic subtype similar to nonmucinous adenocarcinomas is not certain. When stromal invasion is seen, the malignant cells may show less cytoplasmic mucin and more atypia. These tumors differ from mucinous AIS and MIA by one or more of the following criteria: size (>3 cm), amount of invasion (>0.5 cm), multiple nodules, or lack of a circumscribed border with miliary spread into adjacent lung parenchyma.
Figure 7.
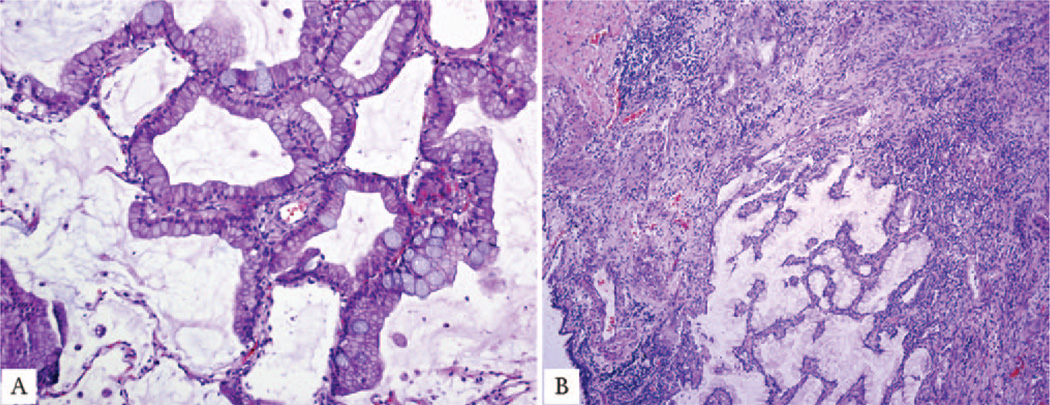
Invasive mucinous adenocarcinoma. A, This area of invasive mucinous adenocarcinoma demonstrates a pure lepidic growth. The tumor consists of columnar cells filled with abundant mucin in the apical cytoplasm and shows small basal oriented nuclei. B, Nevertheless, elsewhere this tumor demonstrated invasion associated with desmoplastic stroma and an acinar pattern.
There is a strong tendency for multicentric, multilobar, and bilateral lung involvement, which may reflect aerogenous spread. Mixtures of mucinous and nonmucinous tumors may rarely occur; then the percentage of invasive mucinous adenocarcinoma should be recorded in a comment. If there is at least 10% of each component, it should be classified as “Mixed mucinous and nonmucinous adenocarcinoma.” Invasive mucinous adenocarcinomas (formerly mucinous BAC) need to be distinguished from adenocarcinomas that produce mucin but lack the characteristic goblet cell or columnar cell morphology of the tumors that have historically been classified as mucinous BAC. When mucin is identified by light microscopy or mucin stains in adenocarcinomas that do not meet the above criteria, this feature should be reported in a comment after classifying the tumor according to the appropriate terminology and criteria proposed in this classification. This can be done by adding a descriptive phrase such as “with mucin production” or “with mucinous features” rather than the term “invasive mucinous adenocarcinoma.”
Pathology Recommendation 8
For adenocarcinomas formerly classified as mucinous BAC, we recommend they be separated from the adenocarcinomas formerly classified as nonmucinous BAC and depending on the extent of lepidic versus invasive growth that they be classified as mucinous AIS, mucinous MIA, or for overtly invasive tumors “invasive mucinous adenocarcinoma” (weak recommendation, low-quality evidence).
Colloid adenocarcinoma shows extracellular mucin in abundant pools, which distend alveolar spaces with destruction of their walls (Figure 8A). The mucin pools contain clusters of mucin-secreting tumor cells, which may comprise only a small percentage of the total tumor and, thus, be inconspicuous (Figure 8A).155,156 The tumor cells may consist of goblet cells or other mucin secreting cells. Colloid adenocarcinoma is found more often as a mixture with other adenocarcinoma histologic subtypes rather than as a pure pattern. A tumor is classified as a colloid adenocarcinoma when it is the predominant component; the percentages of other components should be recorded.150 Cystic gross and histologic features are included in the spectrum of colloid adenocarcinoma, but in most cases, this is a focal feature. Cases previously reported as mucinous cystadenocarcinoma are extremely rare, and now these should be classified as colloid adenocarcinoma with cystic changes. The cysts are filled with mucin and lined by goblet or other mucin secreting cells (Figure 8B). The lining epithelium may be discontinuous and replaced with inflammation including a granulomatous reaction or granulation tissue. Cytologic atypia of the neoplastic epithelium is usually minimal.157
Figure 8.
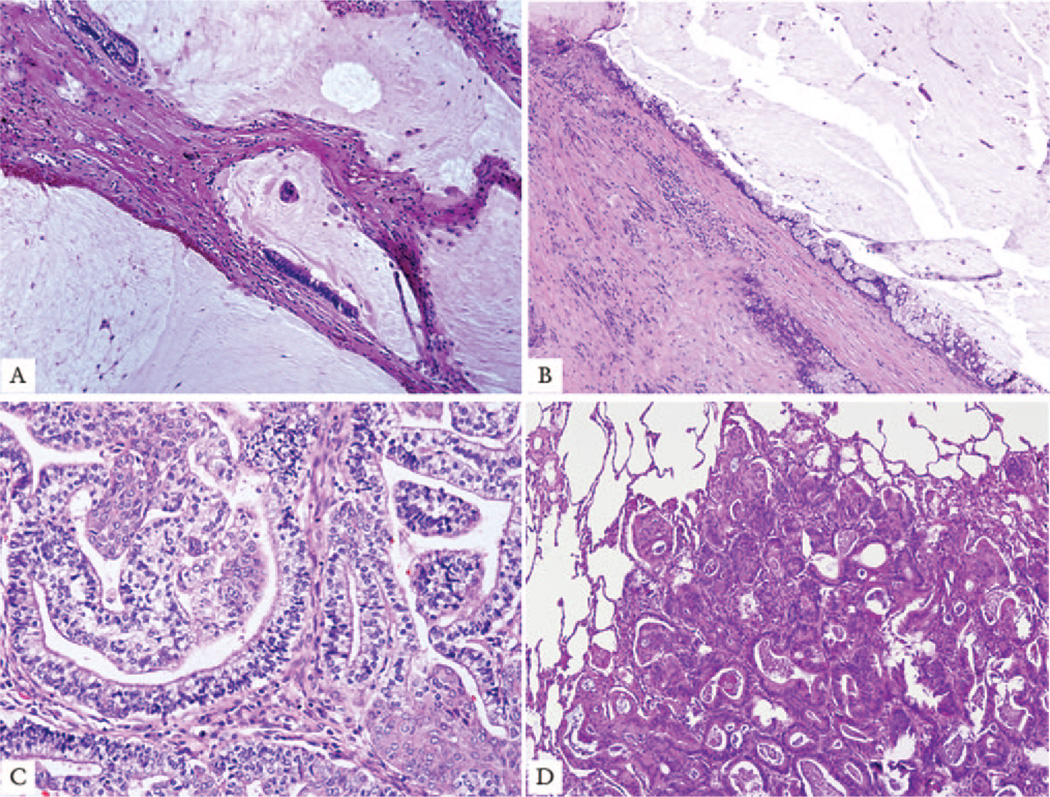
Adenocarcinoma, variants. A, Colloid adenocarcinoma consists of abundant pools of mucin growing within and distending airspaces. Focally well-differentiated mucinous glandular epithelium grows along the surface of fibrous septa and within the pools of mucin. Tumor cells may be very inconspicuous. B, This colloid adenocarcinoma contains a cystic component surrounded by a fibrous wall that is filled with pools of mucin; such a pattern was previously called mucinous cystadenocarcinoma. The surface of the fibrous wall is lined by well-differentiated cuboidal or columnar mucinous epithelium. C, Fetal adenocarcinoma consists of malignant glandular cells growing in tubules and papillary structures. These tumor cells have prominent clear cytoplasm, and squamoid morules are present. D, Enteric adenocarcinoma consists of an adenocarcinoma that morphologically resembles colonic adenocarcinoma with back-to-back angulated acinar structures. The tumor cells are cuboidal to columnar with nuclear pseudostratification.
Fetal adenocarcinoma consists of glandular elements with tubules composed of glycogen-rich, nonciliated cells that resemble fetal lung tubules (Figure 8C).4 Subnuclear vacuoles are common and characteristic. Squamoid morules may be seen within lumens. Most are low grade with a favorable outcome. High-grade tumors occur. When mixtures occur with other histologic subtypes, the tumor should be classified according to the predominant component.158 This tumor typically occurs in younger patients than other adenocarcinomas. Uniquely, these tumors appear driven by mutations in the beta-catenin gene, and the epithelial cells express aberrant nuclear and cytoplasmic staining with this antibody by immunohistochemistry.159,160 Nakatani et al. and Sekine et al.159,160 have suggested that up-regulation of components in the Wnt signaling pathway such as β-catenin is important in low-grade fetal adenocarcinomas and in biphasic pulmonary blastomas in contrast to high-grade fetal adenocarcinomas.
Enteric differentiation can occur in lung adenocarcinoma, and when this component exceeds 50%, the tumor is classified as pulmonary adenocarcinoma with enteric differentiation. The enteric pattern shares morphologic and immunohistochemical features with colorectal adenocarcinoma.154 In contrast to metastatic colorectal adenocarcinoma, these tumors are histologically heterogeneous with some component that resembles primary lung adenocarcinoma such as lepidic growth. Recording of the percentages of these other components may be useful. The enteric pattern consists of glandular and/or papillary structures sometimes with a cribriform pattern, lined by tumor cells that are mostly tall-columnar with nuclear pseudostratification, luminal necrosis, and prominent nuclear debris (Figure 8D).154 Poorly differentiated tumors may have a more solid pattern. These tumors show at least one immunohistologic marker of enteric differentiation (CDX-2, CK20, or MUC2). Consistent positivity for CK7 and expression of TTF-1 in approximately half the cases helps in the distinction from metastatic colorectal adenocarcinoma.154,161 CK7-negative cases may occur.162 Primary lung adenocarcinomas that histologically resemble colorectal adenocarcinoma but lack immunohistochemical markers of enteric differentiation are probably better regarded as lung adenocarcinomas with enteric morphology rather than pulmonary adenocarcinoma with enteric differentiation.163
CLASSIFICATION FOR SMALL BIOPSIES AND CYTOLOGY
Clinical Relevance of Histologic Diagnosis Drives Need to Classify NSCLC Further
This section applies to pathologic diagnosis of the majority of patients with lung cancer due to presentation with locally advanced or metastatic disease. Because of the need for improved separation of squamous cell carcinoma from adenocarcinoma, as it determines eligibility for molecular testing and impacts on specific therapies, there is now greater clinical interest in application of additional pathology tools to refine further the diagnosis in small biopsies (bronchoscopic, needle, or core biopsies) and cytology specimens from patients with advanced lung cancer, when morphologic features are not clear.30,39,40,164,165 Patients with adenocarcinoma should be tested for EGFR mutations (see evidence in Clinical Recommendation section) because patients with EGFR mutation-positive tumors may be eligible for first-line TKI therapy.8–11 Adenocarcinoma patients are also eligible for pemetrexed12–15 or bevacizumab-based chemotherapy regimens (see Clinical Recommendation section).16,17
Pathology Recommendation 9
For small biopsies and cytology, we recommend that NSCLC be further classified into a more specific histologic type, such as adenocarcinoma or squamous cell carcinoma, whenever possible (strong recommendation, moderate quality evidence).
Data Driving Need to Classify NSCLC Further are Based Only on Light Microscopy
All current data that justify the importance of the distinction between histologic types of NSCLC in patients with advanced lung cancer are based on light microscopy alone.8–16 Thus, the diagnosis for clinical work, research studies, and clinical trials should be recorded in a manner, so it is clear how the pathologist made their determination: based on light microscopy alone or light microscopy plus special studies.
Pathology Consideration for Good Practice
When a diagnosis is made in a small biopsy or cytology specimen in conjunction with special studies, it should be clarified whether the diagnosis was established based on light microscopy alone or whether special stains were required.
Management of Tissue for Molecular Studies is Critical
Strategic use of small biopsy and cytology samples is important, i.e., use the minimum specimen necessary for an accurate diagnosis, to preserve as much tissue as possible for potential molecular studies (Figure 9).166 Methods that use substantial amounts of tissue to make a diagnosis of adenocarcinoma versus squamous cell carcinoma, such as large panels of immunohistochemical stains or molecular studies, may not provide an advantage over routine light microscopy with a limited immunohistochemical workup.165
Figure 9.

Algorithm for adenocarcinoma diagnosis in small biopsies and/or cytology. Step 1: When positive biopsies (fiberoptic bronchoscopy [FOB], transbronchial [TBBx], core, or surgical lung biopsy [SLBx]) or cytology (effusion, aspirate, washings, and brushings) show clear adenocarcinoma (ADC) or squamous cell carcinoma (SQCC) morphology, the diagnosis can be firmly established. If there is neuroendocrine morphology, the tumor may be classified as small cell carcinoma (SCLC) or non-small cell lung carcinoma (NSCLC), probably large cell neuroendocrine carcinoma (LCNEC) according to standard criteria (+ = positive, − = negative, and ± = positive or negative). If there is no clear ADC or SQCC morphology, the tumor is regarded as NSCLC-not otherwise specified (NOS). Step 2: NSCLC-NOS can be further classified based on (a) immunohistochemical stains (b) mucin (DPAS or mucicarmine) stains, or (c) molecular data. If the stains all favor ADC: positive ADC marker(s) (i.e., TTF-1 and/or mucin positive) with negative SQCC markers, then the tumor is classified as NSCLC, favor ADC. If SQCC markers (i.e., p63 and/or CK5/6) are positive with negative ADC markers, the tumor is classified as NSCLC, favor SQCC. If the ADC and SQCC markers are both strongly positive in different populations of tumor cells, the tumor is classified as NSCLC-NOS, with a comment it may represent adenosquamous carcinoma. If all markers are negative, the tumor is classified as NSCLC-NOS. See text for recommendations on NSCLCs with marked pleomorphic and overlapping ADC/SQCC morphology. †EGFR mutation testing should be performed in (1) classic ADC, (2) NSCLC, favor ADC, (3) NSCLC-NOS, and (4) NSCLC-NOS, possible adenosquamous carcinoma. In a NSCLC-NOS, if EGFR mutation is positive, the tumor is more likely to be ADC than SQCC. Step 3: If clinical management requires a more specific diagnosis than NSCLC-NOS, additional biopsies may be indicated (−ve = negative; +ive = positive; TTF-1: thyroid transcription factor-1; DPAS +ve: periodic-acid-Schiff with diastase; +ve: positive; e.g., IHC, immunohistochemistry; NE, neuroendocrine; CD, cluster designation; CK, cytokeratin; NB, of note). EGFR, epidermal growth factor receptor; DPAS, diastase-periodic acid Schiff.
Pathology Consideration for Good Practice
Tissue specimens should be managed not only for diagnosis but also to maximize the amount of tissue available for molecular studies.
To guide therapy for patients with advanced lung adenocarcinoma, each institution should develop a multidisciplinary team that coordinates the optimal approach to obtaining and processing biopsy/cytology specimens to provide expeditious diagnostic and molecular results.
If Light Microscopic Diagnosis is Clearly Adenocarcinoma or Squamous Cell Carcinoma, Use These WHO Diagnostic Terms
Squamous cell carcinoma and adenocarcinoma should be diagnosed on biopsy and cytological materials when the criteria for specific diagnosis of these tumor types in the 2004 WHO classification are met. Nevertheless, for tumors that do not meet these criteria, newly proposed terminology and criteria are outlined in Table 2 and Figure 9.4
Histologic Heterogeneity of Lung Cancer is an Underlying Complexity
Because of histologic heterogeneity, small biopsy and/or cytology samples may not be representative of the total tumor, and there may be a discrepancy with the final histologic diagnosis in a resection specimen. Still, combined histologic types that meet criteria for adenosquamous carcinoma comprise less than 5% of all resected NSCLCs.4 A much more common difficulty in small biopsies or cytologies is classifying poorly differentiated tumors where clear differentiation is difficult or impossible to appreciate on light microscopy. The heterogeneity issue also makes it impossible to make the diagnosis of AIS, MIA, large cell carcinoma, or pleomorphic carcinoma in a small biopsy or cytology, because resection specimens are needed to make these interpretations. The term “large cell carcinoma” has been used in some clinical trials, but the pathologic criteria for that diagnosis are not defined, and it is not clear how these tumors were distinguished from NSCLC-NOS, as this diagnosis specimens used to diagnose the patients with advanced-stage lung cancer studied in these trials.13,15,167
Pathology Considerations for Good Practice
The terms AIS or MIA should not be diagnosed in small biopsies or cytology specimens. If a noninvasive pattern is present in a small biopsy, it should be referred to as a lepidic growth pattern.
The term large cell carcinoma should not be used for diagnosis in small biopsy or cytology specimens and should be restricted to resection specimens where the tumor is thoroughly sampled to exclude a differentiated component.
Use Minimal Stains to Diagnose NSCLC, Favor Adenocarcinoma, or Favor Squamous Cell Carcinoma
In those cases where a specimen shows NSCLC lacking either definite squamous or adenocarcinoma morphology, immunohistochemistry may refine diagnosis (Figure 9, step 2). To preserve as much tissue as possible for molecular testing in small biopsies, the workup should be minimal.165 Realizing that new markers are likely to be developed, we suggest the initial evaluation use as only one adenocarcinoma marker and one squamous marker. At the present time, TTF-1 seems to be the single best marker for adenocarcinoma. TTF-1 provides the added value of serving as a pneumocyte marker that can help confirm a primary lung origin in 75 to 85% of lung adenocarcinomas.69,168,169 This can be very helpful in addressing the question of metastatic adenocarcinoma from other sites such as the colon or breast. Diastase-periodic acid Schiff or mucicarmine mucin stains may also be of value. p63 is consistently reported as a reliable marker for squamous histology and CK5/6 also can be useful.39,40,170–176 Cytokeratin 7 also tends to stain adenocarcinoma more often than squamous cell carcinoma.177 Other antibodies (34βE12 and S100A7) are less specific and sensitive for squamous differentiation. These data have been confirmed using resections where biopsies were interpreted as NSCLC39 and also work on most needle aspirate specimens.40 It is possible that cocktails of nuclear and cytoplasmic markers (TTF-1/CK5/6 or p63/napsin-A) may allow for use of fewer immunohistochemical studies of multiple antibodies.164 Cases positive for an adenocarcinoma marker (i.e.,TTF-1) and/or mucin with a negative squamous marker (i.e., p63) should be classified as “NSCLC favor adenocarcinoma” (Figures 10A–C) and those that are positive for a squamous marker, with at least moderate, diffuse staining, and a negative adenocarcinoma marker and/or mucin stains, should be classified as “NSCLC favor squamous cell carcinoma,” with a comment specifying whether the differentiation was detected by light microscopy and/or by special stains. These two small staining panels are generally mutually exclusive. If an adenocarcinoma marker such as TTF-1 is positive, the tumor should be classified as NSCLC, favor adenocarcinoma despite any expression of squamous markers.164,165 If the reactivity for adenocarcinoma versus squamous markers is positive in a different population of tumor cells, this may suggest adenosquamous carcinoma. If tumor tissue is inadequate for molecular testing, there may be a need to rebiopsy the patient to perform testing that will guide therapy (step 3, Figure 9).
Figure 10.
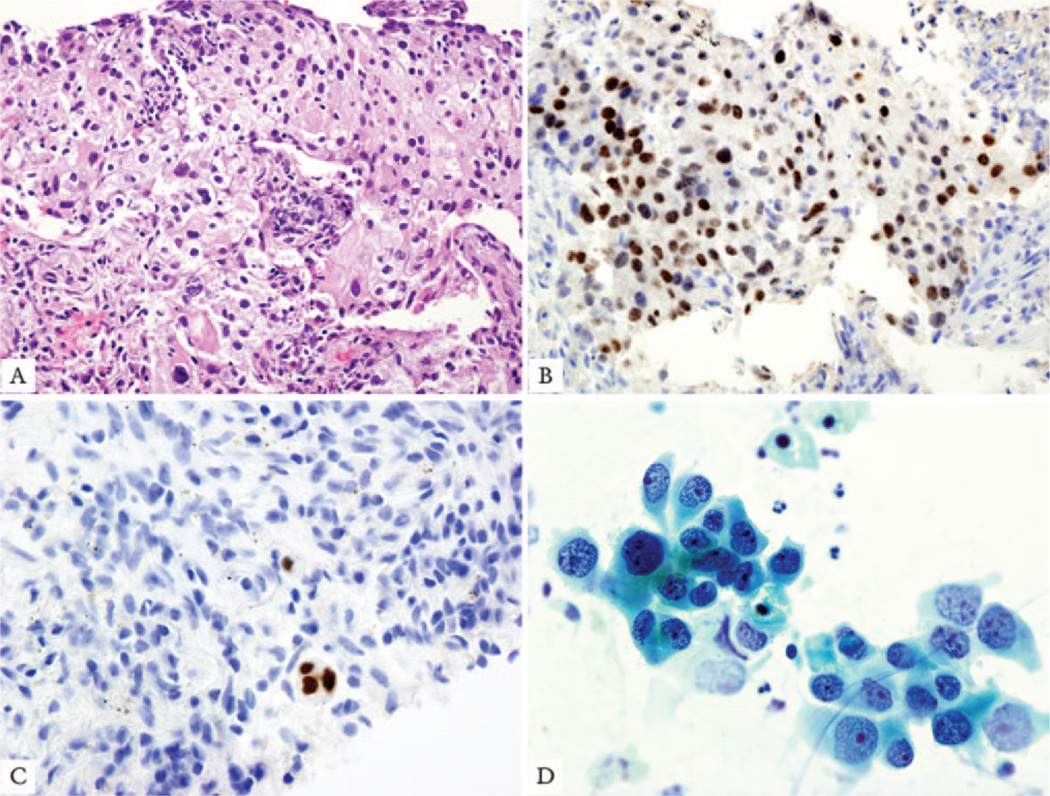
Adenocarcinoma in small biopsy and cytology. Poorly differentiated non-small cell carcinoma, favor adenocarcinoma. A, This core biopsy shows a solid pattern of growth, and morphologically, it lacks any acinar, papillary, or lepidic patterns. The mucin stain was also negative. B, The TTF-1 stain is strongly positive. C, The p63 stain is very focally positive. The strongly and diffusely positive TTF-1 and only focal p63 staining favor adenocarcinoma. In this case, EGFR mutation was positive. D, Cytology from different adenocarcinoma shows large malignant cells with abundant cytoplasm and prominent nuclei growing in an acinar structure. EGFR, epidermal growth factor receptor; TTF, thyroid transcription factor.
There may be cases where multidisciplinary correlation can help guide a pathologist in their evaluation of small biopsies and/or cytology specimens from lung adenocarcinomas. For example, if a biopsy showing NSCLC-NOS is obtained from an Asian, female, never smoker with ground-glass nodules (GGNs) on CT, the pathologist should know this information as the tumor is more likely to be adenocarcinoma and have an EGFR mutation.
Cytology is a Useful Diagnostic Method, Especially When Correlated with Histology
Cytology is a powerful tool in the diagnosis of lung cancer, in particular in the distinction of adenocarcinoma from squamous cell carcinoma.178 In a recent study, of 192 preoperative cytology diagnoses, definitive versus favored versus unclassified diagnoses were observed in 88% versus 8% versus 4% of cases, respectively.179 When compared with subsequent resection specimens, the accuracy of cytologic diagnosis was 93% and for definitive diagnoses, it was 96%. For the adenocarcinoma and squamous cell carcinoma cases, only 3% of cases were unclassified, and the overall accuracy was 96%. When immunohistochemistry was used in 9% of these cases, the accuracy was 100%.179
Whenever possible, cytology should be used in conjunction with histology in small biopsies (Figure 10D).40,180 In another study where small biopsies were evaluated in conjunction with cytology for the diagnosis of adenocarcinoma versus squamous cell carcinoma versus unclassified (NSCLC-NOS), the result for cytology was 70% versus 19% versus 11% and for biopsies, it was 72%, 22%, and 6%, respectively.180 Still when cytology was correlated with biopsy, the percentage of cases diagnosed as NSCLC-NOS was greatly reduced to only 4% of cases.180 In a small percentage of cases (<5%), cytology was more informative than histology in classifying tumors as adenocarcinoma or squamous cell carcinoma.180 The factors that contributed the greatest to difficulty in a specific diagnosis in both studies were poor differentiation, low specimen cellularity, and squamous histology.179,180
Pathology Consideration for Good Practice
When paired cytology and biopsy specimens exist, they should be reviewed together to achieve the most specific and nondiscordant diagnoses.
Preservation of Cell Blocks from Cytology Aspirates or Effusions for Molecular Studies
The volume of tumor cells in biopsies may be small due to frequent prominent stromal reactions, so that there may be insufficient material for molecular analysis. Material derived from aspirates or effusions may have more tumor cells than a small biopsy obtained at the same time, so any positive cytology samples should be preserved as cell blocks, so that tumor is archived for immunohistochemical and molecular studies. Furthermore, these materials should be used judiciously in making the diagnosis to preserve as much material as possible for potential molecular studies.40,181–183 In a recent study, material from cell blocks prepared from 128 lung cancer cytology specimens was suitable for molecular analysis for EGFR and KRAS mutations in 126 (98%) of specimens.179
Pathology Consideration for Good Practice
Cell blocks should be prepared from cytology samples including pleural fluids.
NSCLC-NOS: If No Clear Differentiation by Morphology or Immunohistochemistry
There will remain a minority of cases where the diagnosis remains NSCLC-NOS, as no differentiation can be established by routine morphology and/or immunohistochemistry (Figure 9, step 2). In the setting of a tumor with a negative adenocarcinoma marker (i.e., TTF-1), and only weak or focal staining for a squamous marker, it is best to classify the tumor as NSCLC-NOS rather than NSCLC, favor squamous cell carcinoma. These cases may benefit from discussion in a multidisciplinary setting (a) to determine the need for a further sample if subtyping will affect treatment; (b) whether molecular data should be sought, again if treatment will be defined by such data; (c) whether noninvasive features such as imaging characteristics (e.g., peripheral GGN supporting adenocarcinoma) favor a tumor subtype; and (d) whether clinical phenotype (e.g., female, never smoker, and Asian) may assist in determining future management (Figure 9, step 3).
Pathology Recommendation 10
We recommend that the term NSCLC-NOS be used as little as possible, and we recommend it be applied only when a more specific diagnosis is not possible by morphology and/or special stains (strong recommendation, moderate quality evidence).
Pathology Consideration for Good Practice
The term nonsquamous cell carcinoma should not be used by pathologists in diagnostic reports. It is a categorization used by clinicians to define groups of patients with several histologic types who can be treated in a similar manner; in small biopsies/cytology, pathologists should classify NSCLC as adenocarcinoma, squamous cell carcinoma, NSCLC-NOS, or other terms outlined in Table 2 or Figure 9.
NSCLC-NOS: When Morphology and Immunohistochemistry are Conflicting
Rarely, small samples may show either morphologic features of both squamous cell carcinoma and adenocarcinoma with routine histology or by immunohistochemical expression of both squamous and adenocarcinoma markers; these should be termed as “NSCLC-NOS” with a comment recording the features suggesting concurrent glandular and squamous cell differentiation, specifying whether this was detected by light microscopy or immunohistochemistry. As p63 expression can occur in up to one third of adenocarcinomas,40,184,185 in a tumor that lacks squamous cell morphology, virtually all tumors that show coexpression of p63 and TTF-1 will be adenocarcinomas. It is possible that the tumor may be an adenosquamous carcinoma but that diagnosis cannot be established without a resection specimen showing at least 10% of each component. If TTF-1 and p63 positivity are seen in different populations of tumor cells, it is possible that this may be more suggestive of adenosquamous carcinoma than if these markers are coexpressed in the same tumor cells.
Interpret Morphologic and Staining Patterns to Maximize Patient Eligibility for Therapies
Presently, the recommendation for EGFR mutation testing and candidacy for pemetrexed or bevacizumab therapy is for the diagnosis of (1) adenocarcinoma, (2) NSCLCNOS, favor adenocarcinoma, or (3) NSCLC-NOS (see Clinical Recommendation section later). For this reason, in most NSCLC, the primary decision pathologists need to focus on, while interpreting small biopsies and cytology specimens, whether the tumor is a definite squamous cell carcinoma or NSCLC, favor squamous cell carcinoma versus one of the above diagnoses. Thus, when morphology or immunohistochemical findings are equivocal, pathologists need to keep in mind that a diagnosis of squamous cell carcinoma or NSCLC, favor squamous cell carcinoma will exclude them from histologically driven molecular testing or chemotherapy. In such a situation, it may be best to favor NSCLC-NOS, to allow the patient to be eligible for the therapeutic options mentioned earlier in the text. Hopefully, effective therapies, perhaps based on molecular targets, will become available for squamous cell carcinoma in the near future.
Pathology Consideration for Good Practice
The above strategy for classification of adenocarcinoma versus other histologies and the terminology in Table 2 and Figure 9 should be used in routine diagnosis and future research and clinical trials, so that there is uniform classification of disease cohorts in relationship to tumor subtypes and data can be stratified according to diagnoses made by light microscopy alone versus diagnoses requiring special stains.
Distinction of Adenocarcinoma from Sarcomatoid Carcinomas
Cases that show sarcomatoid features such as marked nuclear pleomorphism, malignant giant cells, or spindle cell morphology should be preferentially regarded as adenocarcinoma or squamous cell carcinoma if these features are clearly present, as this is apt to influence management. Nevertheless, pleomorphic carcinoma, carcinosarcoma, and blastoma are very difficult to diagnose in small specimens due to the limited ability to assess for mixed histologies. Nevertheless, if a small biopsy shows what is probably an adenocarcinoma with pleomorphism, a comment should be made, e.g., “NSCLC, favor adenocarcinoma, with giant and/or spindle cell features” (depending on which feature is identified).
Pathology Consideration for Good Practice
Tumors that show sarcomatoid features, such as marked nuclear pleomorphism, malignant giant cells, or spindle cell morphology, should be preferentially regarded as adenocarcinoma or squamous cell carcinoma if clear glandular or squamous features are present, as this is apt to influence management. If such features are not present, the term “poorly differentiated non-small cell carcinoma with giant and/or spindle cell features” (depending on what feature is present) should be used.
Distinction of Adenocarcinoma from Neuroendocrine Carcinomas
Some cases of NSCLC may suggest neuroendocrine (NE) morphology; these should be assessed with NE markers (CD56, chromogranin, and/or synaptophysin), so that a diagnosis of large cell NE carcinoma (LCNEC) can be suggested. The term NSCLC, possible LCNEC is usually the best term when this diagnosis is suspected as it is difficult to establish a diagnosis of LCNEC on small biopsies. In those lacking NE morphology, we recommend against using routine staining with NE markers, as immunohistochemical evidence of NE differentiation in otherwise definite adenocarcinoma and squamous cell carcinoma does not seem to affect prognosis186,187 or treatment.
Pathology Consideration for Good Practice
NE immunohistochemical markers should only be performed in cases where there is suspected NE morphology. If NE morphology is not suspected, NE markers should not be performed.
GRADING OF ADENOCARCINOMAS
No well-established histologic or cytologic grading system exists for lung adenocarcinoma. Most publications which grade adenocarcinomas do not cite specific morphologic criteria. The overall grade of a tumor is typically determined by the component with the worst grade. Only a few studies have evaluated detailed morphologic grading systems.41,188–191 The primary approaches are based on architectural and/or nuclear attributes. Nevertheless, the following histologic features are promising candidates for components of a grading system. By architecture, the following prognostic associations have been reported: poor (solid41,43,44,53,69 and micropapillary),43,44,108,109 favorable (nonmucinous lepidic43,44,46,192 [formerly BAC]), and intermediate (papillary and acinar).43,44 Thus, comprehensive histologic subtyping method and subclassification of invasive tumors by the predominant subtype may be a simple way to develop the architectural grade of lung adenocarcinomas,43,44 similar to the Gleason grading system for prostate cancer.193 By nuclear criteria, preliminary data suggest poor prognosis may be associated with large nuclei and variability in nuclear size and shape.190,191,194 As stated earlier in the text, histologic grading should not be confused with the GRADE method of formulating recommendations and weighing evidence.190,191
STRATEGIC USE OF PATHOLOGIC SPECIMENS FOR MOLECULAR STUDIES
With the emerging importance of molecular diagnostics to guide therapy, a multidisciplinary approach is needed to set a consistent strategy for obtaining and preserving tissue samples optimized to perform studies such as DNA sequence analysis, fluorescence in situ hybridization (FISH), and, in some settings, RNA-based studies. It is not yet possible to provide specific guidelines on how to do this in the current document because of the wide variation in infrastructure and expertise from one institution to another. Still, this process begins with the method of obtaining tissue (fine needle aspiration [FNA], core or transbronchial biopsy, and surgical resection) and continues with the processing of the specimen in the pathology department, to delivery of material for molecular analysis, and communication of the molecular results in pathology reports.
If a portion of a sampled tumor is snap frozen for molecular studies, a few considerations exist as regards resection specimens. As most critical molecular studies can be performed from formalin-fixed paraffin-embedded tissue, there is a need for frozen samples only for certain techniques such as comparative genomic hybridization (CGH) and gene expression profiling. If frozen tissue is being obtained from tumors with lepidic predominant tumors where AIS or MIA is in the differential diagnosis, efforts should be made to ascertain whether this frozen piece has an invasive component. The CT and gross appearance of the lesion should be considered to ensure a solid component is sampled in a tumor that appeared part solid on CT. Another approach is to perform a frozen section from the tissue saved for storage in a freezer.
Small biopsies and/or cytologic samples including pleural fluids can be used for many molecular analyses.179,181,183,195–205 EGFR mutation testing and KRAS mutation testing are readily performed on these specimens.179–181,195–199,203–205 Formalin-fixed paraffin-embedded samples can be used effectively for polymerase chain reaction-based mutation testing and for FISH or chromogenic in situ hybridization (CISH) testing for gene amplification and for immunohistochemistry. Cytology smears can be analyzed for immunohistochemical and certain molecular studies, but it is far preferable if cell blocks are available. Manual or laser-guided microdissection may enrich tumor cells for molecular studies. Assessment of EGFR mutations helps in selecting patients to be treated with EGFR-TKIs. Molecular testing in the setting of clinical trials can stratify patients by results of gene expression or markers of sensitivity to specific cytotoxic agents such as excision repair cross-complementation group 1 or breast cancer 1 for platinum, ribonucleotide reductase M1 for gemcitabine or thymidylate synthase for antifolates.206–211
Summary of Pathology Recommendations
We recommend discontinuing the use of the term “BAC” (strong recommendation, low-quality evidence).
For small (≤3 cm), solitary adenocarcinomas with pure lepidic growth, we recommend the term “Adenocarcinoma in situ” that defines patients who should have 100% disease-specific survival, if the lesion is completely resected (strong recommendation, moderate quality evidence). Remark: Most AIS are nonmucinous, rarely are they mucinous.
For small (≤3 cm), solitary, adenocarcinomas with predominant lepidic growth and small foci of invasion measuring ≤0.5 cm, we recommend a new concept of “Minimally invasive adenocarcinoma” to define patients who should have near 100%, disease-specific survival, if completely resected (strong recommendation, low-quality evidence). Remark: Most MIA are nonmucinous, rarely are they mucinous.
For invasive adenocarcinomas, we suggest comprehensive histologic subtyping be used to assess histologic patterns semiquantitatively in 5% increments, choosing a single predominant pattern. We also suggest that individual tumors be classified according to the predominant pattern and that the percentages of the subtypes be reported (weak recommendations and low-quality evidence).
In patients with multiple lung adenocarcinomas, we suggest comprehensive histologic subtyping in the comparison of the complex, heterogeneous mixtures of histologic patterns to determine whether the tumors are metastases or separate synchronous or metachronous primaries (weak recommendation, low-quality evidence).
For nonmucinous adenocarcinomas previously classified as mixed subtype where the predominant subtype consists of the former nonmucinous BAC, we recommend use of the term LPA and discontinuing the term “mixed subtype” (strong recommendation, low-quality evidence).
In patients with early-stage adenocarcinoma, we recommend the addition of “micropapillary predominant adenocarcinoma,” when applicable, as a major histologic subtype due to its association with poor prognosis (strong recommendation, low-quality evidence).
For adenocarcinomas formerly classified as mucinous BAC, we recommend that they be separated from the adenocarcinomas formerly classified as nonmucinous BAC and depending on the extent of lepidic versus invasive growth that they be classified as mucinous AIS, mucinous MIA, or for overtly invasive tumors “invasive mucinous adenocarcinoma” (weak recommendation, low-quality evidence).
For small biopsies and cytology, we recommend that NSCLC be further classified into a more specific type, such as adenocarcinoma or squamous cell carcinoma, whenever possible (strong recommendation, moderate quality evidence).
We recommend that the term NSCLC-NOS be used as little as possible, and we recommend it be applied only when a more specific diagnosis is not possible by morphology and/or special stains (strong recommendation, moderate quality evidence).
Summary of Pathology Considerations for Good Practice
When a diagnosis is made in a small biopsy or cytology specimen in conjunction with special studies, it should be clarified whether the diagnosis was established based on light microscopy alone or whether special stains were required.
Tissue specimens should be managed not only for diagnosis but also to maximize the amount of tissue available for molecular studies.
To guide therapy for patients with advanced lung adenocarcinoma, each institution should develop a multidisciplinary team that coordinates the optimal approach to obtaining and processing biopsy/cytology specimens to provide expeditious diagnostic and molecular results.
The terms AIS or MIA should not be used in small biopsies or cytology specimens. If a noninvasive pattern is present in a small biopsy, it should be referred to as lepidic growth.
The term large cell carcinoma should not be used for diagnosis in small biopsy or cytology specimens and should be restricted to resection specimens where the tumor is thoroughly sampled to exclude a differentiated component.
When paired cytology and biopsy specimens exist, they should be reviewed together to achieve the most specific and nondiscordant diagnoses.
Cell blocks should be prepared from cytology samples including pleural fluids.
The term nonsquamous cell carcinoma should not be used by pathologists in diagnostic reports. It is a categorization used by clinicians to define groups of patients with several histologic types who can be treated in a similar manner; in small biopsies/cytology, pathologists should classify NSCLC as adenocarcinoma, squamous cell carcinoma, NSCLC-NOS, or other terms outlined in Table 2 or Figure 9.
The above strategy for classification of adenocarcinoma versus other histologies and the terminology in Table 2 and Figure 9 should be used in routine diagnosis and future research and clinical trials, so that there is uniform classification of disease cohorts in relationship to tumor subtypes and data can be stratified according to diagnoses made by light microscopy alone versus diagnoses requiring special stains.
Tumors that show sarcomatoid features, such as marked nuclear pleomorphism, malignant giant cells, or spindle cell morphology, should be preferentially regarded as adenocarcinoma or squamous cell carcinoma if clear glandular or squamous features are present, as this is apt to influence management. If such features are not present, the term “poorly differentiated non-small cell carcinoma with giant and/or spindle cell features” (depending on what feature is present) should be used.
NE immunohistochemical markers should only be performed in cases where there is suspected NE morphology. If NE morphology is not suspected, NE markers should not be performed.
Pathology Research Recommendations
Criteria for MIA are based on limited published data and require further validation. Persistent questions include what is the optimal method for measuring the size of the invasive component? Is 0.5 cm the best size cut off? If multiple areas of invasion are present, should the greatest dimension of the largest invasive focus be used or the total size multiplied times the percentage of the invasive components? What should be the impact of scar size or prominent stromal desmoplasia and stromal inflammation on determining size of the invasive component? Should criteria for MIA be different for mucinous versus nonmucinous tumors?
Lepidic growth may also be composed of neoplastic cells with nuclear atypia resembling that of the adjacent invasive patterns. Whether there is any clinical implication is unknown. That is, it is not established if this is in situ or invasive carcinoma.
The level of reproducibility for identifying predominant histologic patterns is untested. In particular, how should the lepidic pattern be distinguished from other invasive patterns such as acinar and papillary?
Do tumors that meet criteria for MIA have 100% disease-free survival if the invasive component is predominantly solid, micropapillary or if they show giant cell and spindle cell components that fail to qualify for a diagnosis pleomorphic carcinoma?
What is the long-term follow-up for completely resected solitary mucinous MIA? Can this be the initial presentation for multifocal invasive mucinous adenocarcinoma?
Does the micropapillary pattern have a similar poor prognostic significance in advanced stage and early stage?
Is there any prognostic significance to the aggressive micropapillary or solid components when present in relatively small amounts if they do not represent the predominant pattern? If so, what percentage is needed for such significance?
Is immunohistochemical testing using EGFR mutation-specific antibodies a reliable method for predicting the presence of an EGFR mutation?
It is unknown whether there is any added value provided by refining NSCLC-NOS via immunohistochemistry on small biopsies or cytology samples. This requires assessment in future trials using systemic therapy.
Additional markers for squamous or adenocarcinoma differentiation, such as desmocoglein-3212 or desmocollin213 for squamous cell carcinoma or napsin-A for adenocarcinoma,214 need further evaluation.
The ability of pathologists to distinguish AIS from invasive disease at frozen section is not proven.
Currently, we cannot recommend any specific grading system. Further investigation is needed to determine whether the optimal grading system should include architectural versus nuclear assessment or both.
In specimens from metastatic sites, is there any clinical significance to recognizing histologic patterns, including the predominant pattern?
CLINICAL FEATURES
Several important clinical facts have had a significant impact on this classification: (1) adenocarcinoma histology is a strong predictor for outcome to pemetrexed therapy in advanced-stage patients.13–15 (2) Distinction between adenocarcinoma or other non-small cell histologies and squamous cell carcinoma is important because of potential life-threatening hemorrhage in patients with squamous cell carcinoma who receive bevacizumab therapy.16 (3) EGFR mutation is a validated predictive marker for response and progression-free survival (PFS) with EGFR-TKIs in the first-line therapy in advanced lung adenocarcinoma.8,215–218 (4) Molecular markers are an important evolving area in evaluation and management of patients with lung adenocarcinoma.219 More data are needed regarding other molecular markers beyond EGFR mutation, such as KRAS mutation, EGFR gene copy number, and EML4-ALK fusion, before they can be accepted as validated markers for a recommendation in this document.153,220
Biopsy and Pathology Issues for the Clinician
After initial evaluation, a plan for an invasive procedure to obtain a diagnosis and complete staging should be made in a multidisciplinary setting.221 The site for the biopsy should be chosen to yield the maximal information with the least risk. A key element in determining the type of procedure is the need to obtain adequate tissue for all pathologic and molecular evaluations (e.g., mutation analysis and immunohistochemistry).
For sampling a peripheral nodular lesion that contains a solid component, the suitable invasive procedures are transthoracic biopsy such as CT-guided biopsies, bronchoscopy/navigation-assisted bronchoscopy, sublobar resection, or lobectomy (e.g., by video-assisted thoracic surgery, VATS, or thoracoscopy). Either a core biopsy or a FNA with a cell block will reliably obtain adequate tissue.179,203 For mediastinal involvement, sampling can be achieved by blind TBNA, endobronchial endoscopy (endobronchial ultrasound) -guided TBNA, EUS-guided FNA, mediastinoscopy, VATS, or Chamberlain procedure. For patients with recurrent disease, repeat biopsy can be useful not only to confirm the diagnosis but also the molecular profile.
Prognostic and Predictive Factors
Multiple clinical, pathologic, and molecular factors have been explored for their association with patient outcome. To facilitate the discussion, we divided them into two categories although both categories are prognostic factors in the strict sense: prognostic factors, which dictate the virulence of the disease (e.g., progression and recurrence), and predictive factors, which are correlated with the outcome for specific therapies. Predictive and prognostic factors may overlap; however, they are often different.
The main independent clinical prognostic factors for patients with lung adenocarcinoma are stage, performance status, age, and sex.222 The independent prognostic value of stage exists whether using clinical223 or pathological224 staging. Data also suggest that smoking history may be an independent prognostic factor.225
Although clinical factors provide important prognostic information, recently there has been greater focus on predictive factors for specific therapies, initially focusing on histology.219 In early clinical trials of erlotinib and gefitinib, some patients with good responses to these drugs were those with adenocarcinoma with lepidic growth patterns (formerly known as BAC).226 This led to trials of gefitinib and erlotinib in patients formerly diagnosed with BAC. West et al.227 reported the results of a Southwest Oncology Group trial in which 17% of patients had a response to gefitinib. Similarly, Miller et al.198 reported a 22% response rate to erlotinib in patients formerly diagnosed with BAC or adenocarcinoma with BAC features. In the new classification, many of these tumors would be regarded to be invasive adenocarcinomas with varying degrees of lepidic growth.
Although histology will continue to play an important predictive role, recently the use of molecular markers for predicting response to therapy has become more prominent, particularly after the discovery of EGFR mutations and their association with sensitivity to erlotinib and gefitinib.215–217,219 Although KRAS mutations were identified in patients with NSCLC more than 20 years ago, their clinical role as predictive and prognostic biomarkers remains controversial. Several phase 2 clinical trials228–233 verified use of EGFR mutations as predictors of response to erlotinib and gefitinib. EGFR mutations occur most frequently in East Asian patients and in those patients with little or no smoking history. The EGFR mutations that are most common and recognized to be of greatest clinical significance are somatic point mutations in codon L858R in exon 21 and in-frame deletions in exon 19.215–217,219 Four recent phase 3 trials were based on patients with either pure or predominantly lung adenocarcinoma histology; one which selected patients clinically and three which selected patients by EGFR mutations have demonstrated that patients with EGFR mutation lung cancer have better treatment outcomes (response rate and PFS) when treated with the EGFR inhibitor gefitinib than with conventional platin-based doublet chemotherapy.8–11 In the Iressa Pan Asian Survival Study trial, molecular subset analysis showed that PFS benefit was limited to the patients with EGFR mutation (hazard ratio [HR]: 0.48, 95% confidence interval [CI]: 0.36–0.64) and that gefitinib therapy was detrimental for those without mutations (HR: 2.85, 95% CI: 2.05–3.98).8 Maemondo et al.10 showed PFS of patients with EGFR mutations was 10.8 months in patients who received gefitinib compared with 5.4 months in those who received carboplatin plus paclitaxel (HR: 0.30, 95% CI: 0.22– 0.41, p < 0.001) and a higher response rate (73.7% versus 30.7%, p < 0.001). Mitsudomi et al.9 showed that patients with EGFR mutations who received gefitinib had significantly longer median PFS of 9.2 months versus 6.3 months (HR: 0.489, 95% CI: 0.336–0.710, p < 0.001). Zhou et al.11 showed that patients with EFGR mutations treated with erlotinib have significantly longer median PFS of 13.1 months compared with 4.6 months for those treated with gemcitabine/carboplatin (HR: 0.16, 95% CI: 0.10–0.26, p < 0.0001). These trials do not demonstrate significant differences in overall survival for gefitinib treatment, likely an effect of cross-over treatment with gefitinib or erlotinib in secondline therapy. Similarly, in a chemotherapy-controlled phase III study (INTEREST) comparing gefitinib with docetaxel, EGFR mutation-positive patients had longer PFS and higher objective response rates (42% versus 7%) than those without mutations for gefitinib.234 The finding that EGFR mutation is predictive of important benefit for PFS and responsiveness to TKI therapy is also supported by multiple phase 2 clinical trials.228 –233
Other molecular predictors of outcome have also been explored for erlotinib and gefitinib treatment. Retrospective analysis of data from the Iressa Survival Evaluation in Lung Cancer study showed that EGFR copy number and protein expression were predictive of significantly better overall survival after treatment with gefitinib.235 A multivariate analysis of data from the Canadian BR.21, phase 3 randomized, placebo-controlled trial of erlotinib in advanced NSCLC showed that EGFR copy number (but not EGFR mutation status) was associated with worse survival (HR: 1.9, 95% CI: 1.1–3.4) and a better response to erlotinib (p = 0.005), after controlling for race, performance status, weight loss, smoking history, prior treatment, and response to prior treatment.236 In a second-line, chemotherapy controlled phase III study (INTEREST) comparing gefitinib with docetaxel, overall survival was similar in the two arms, and there were no statistically significant interactions between treatment and EGFR copy number, protein expression, or mutation status.234 The results of all three of these studies may be influenced by inclusion of large numbers of patients with histologies other than adenocarcinoma and should be regarded as exploratory.234–236
For treatment of advanced NSCLC, response and outcome to EGFR-TKIs have been demonstrated in most studies to be better predicted by EGFR mutation testing rather than copy number or immunohistochemistry. In a phase II study of erlotinib-treated patients, multivariate analysis of molecular predictors showed that EGFR mutations, but not copy number, was predictive of response to erlotinib with a response of 83% in patients with EGFR mutations versus 7% in those without (p < 0.01).198 In this study, immunohistochemistry was not predictive of response.198 Another study by Sholl et al.237 found EGFR mutation status, but not FISH, CISH, or immunohistochemistry, was useful for predicting response and PFS for TKI therapy. The recent development of new mutation-specific antibodies for EGFR exon 19 deletion and L858R mutation seems to be much more reliable in predicting EGFR mutation status, and these need to be evaluated in future clinical trials.238 –240 In the Iressa Pan Asian Survival Study, in FISH+ patients, gefitinib was worse than chemotherapy if those patients lacked EGFR mutations.241 All these studies used RECIST to measure response to therapy.8 –11,198,234 –236,241
More recently, investigators have noted that all NSCLC histologies other than squamous cell carcinoma seem to garner more benefit from two drugs, pemetrexed for efficacy and bevacizumab for avoidance of toxicity. Nevertheless, most of the analyses are subgroup analyses with the known shortcomings. Pemetrexed, a multitargeted antifolate agent, seems to have greater activity in NSCLCs with nonsquamous histology (adenocarcinoma and NSCLC-NOS), with the greatest proportion of benefit observed in patients with adenocarcinomas as demonstrated in two phase 3 trials.12–15 In a phase 3 trial, comparing cisplatin/pemetrexed with cisplatin/gemcitabine, preplanned subgroup analysis, revealed median overall survival was significantly better for patients with adenocarcinoma (12.6 versus 10.9 months, HR = 0.81, 95% CI: 0.71– 0.99, p = 0.03) and large cell carcinoma (would be called NSCLC-NOS by the current proposal), overall survival of 10.4 versus 6.7 months (HR = 0.67; CI: 0.48–0.96), whereas no benefit was seen with squamous cell carcinoma or with all histologies combined.13 Follow-up analysis of the same patients from this phase 3 study but focusing on those without grade 3 or 4 drug toxicity, a similar benefit for overall survival was found in patients with nonsquamous histology comparing cisplatin pemetrexed with cisplatin/gemcitabine (median survival of 5.6 months versus 2.8 months, respectively, HR = 0.64, 95% CI: 0.56–0.72, p < 0.001).12 Ciuleanu et al. showed in a phase 3 trial comparing pemetrexed versus placebo, where prespecified analysis for histology were performed, that patients with adenocarcinoma histology had better median PFS (4.5 versus 1.5 months, HR = 0.511; CI: 0.38–0.68; p < 0.0001) and median overall survival (16.8 versus 11.5 months; HR = 0.73; CI: 0.56– 0.96; p < 0.026). The benefit was also significant for nonsquamous carcinomas classified as other, and for nonsquamous cell carcinoma overall, but not for large cell carcinomas or squamous cell carcinomas.14 Several phase II studies have also shown a benefit for pemetrexed in patients with advanced NSCLC with nonsquamous histologic subtypes.242,243 Nevertheless, a recent phase III trial, with primary end point as the assessment of quality of life, observed similar outcomes for patients treated with pemetrexed/carboplatin regardless of histology.244 Patients with adenocarcinoma or NSCLC-NOS (nonsquamous NSCLC histology) are the only patients who have been demonstrated to benefit from bevacizumab in combination with chemotherapy.245 Indeed, patients with squamous cell carcinoma are at greater risk of adverse events, and therefore, such patients have been excluded from receiving this drug by the Food and Drug Administration,17 but they are eligible for adjuvant therapy in ongoing trials.16
Very recently, a new predictive biomarker has been identified in patients with NSCLC, the EML4/ALK translocation. This translocation leads to an oncogenic constitutive activation of ALK.220,246,247 A recent study of 82 patients with NSCLC confirmed to have ALK fusion by FISH demonstrated a 57% overall response rate to crizotinib (PF-02341066), an inhibitor of MET and ALK, and the estimated 6-month PFS was 72%.248 De novo resistance mutations in the kinase domain of EML4-ALK have been reported to develop during ALK inhibitor therapy.249
Clinical Implications of Histology and Molecular Testing
Accurate histologic subtyping and EGFR mutation testing are important and should be included in the initial work-up of patients with advanced lung adenocarcinoma because it may guide treatment decisions. Whether other EGFR tests should be recommended (i.e., immunohistochemistry and FISH) and/or KRAS mutation as an indicator of TKI resistance is not yet clear.250,251 In addition to EGFR mutation analysis, additional molecular tests are in development and may be more useful when further clinical data support their use.
Surgically Resectable NSCLC
Twenty to 30% of patients with NSCLC are diagnosed with stage I to stage IIIA disease and, thus, may be amenable to surgical resection. Patients who undergo resection have differing prognoses based on pathologic stage. The recent IASLC staging project has demonstrated overall 5-year survival of 73% for stage IA, 58% for stage IB, 46% for stage IIA, 36% for stage IIB, 24% for stage IIIA, and 9% for stage IIIB.252,253 The introduction of adjuvant cisplatin-based chemotherapy represented a major step forward with a 5% increase in cure rate.254 Still, 27% of patients with stage IA disease and 42% of patients with stage IB NSCLC eventually recur and die of their disease; there is no accurate way to predict which of these patients have poor-risk disease and are likely to recur. Similarly, 41% of patients with stage II NSCLC are cured by surgery alone and do not need any adjuvant therapy.252,253 Thus, an urgent need to identify factors, which will select patients for adjuvant therapy, exists. Several predictive factors for better efficacy of adjuvant chemotherapy have been described in retrospective analyses of phase III randomized adjuvant studies. An example is low expression of the DNA repair genes excision repair cross-complementation group 1 for greater benefit from cisplatin-based chemotherapy, although this needs further validation.207 Based on initial data showing striking differences in survival predicted by histologic subtyping according to this proposed classification of lung adenocarcinomas in resected specimens,44 it is possible in the future that histology will play an important role in selecting patients for adjuvant therapy.
Clinical Recommendation
In patients with advanced lung adenocarcinoma, we recommend testing for EGFR mutation (strong recommendation, moderate quality evidence).
Remarks: This is a strong recommendation because potential benefits clearly outweigh harms. This recommendation assumes that correct classification by EGFR mutation status is associated with important benefit based on randomized phase 3 clinical trials of EGFR-TKI therapy, which demonstrate a predictive benefit for response rate and PFS, but not overall survival, and subset analyses of multiple additional studies.
Clinical Consideration for Good Practice
If molecular testing is planned, appropriate biopsy methods should be used to obtain sufficient tissue for both pathologic diagnosis and molecular analyses, and the specimens should be handled appropriately.
Clinical Research Recommendations
How can this histological and/or molecular classification improve our ability to estimate prognosis and optimize the selection of patients for a specific therapy?
What is the relative importance of histologic versus molecular data for identifying prognostic or predictive markers based on small biopsies and cytology versus resected specimens?
Is immunohistochemical testing using EGFR mutation-specific antibodies as predictive of response to EGFRTKIs as EGFR mutations?
In advanced lung adenocarcinomas, are the prognostic and therapeutic implications of histology any different if the pathologic diagnosis is based on a combination of histology and immunohistochemistry (i.e., TTF-1 and/or p63) versus conventional light microscopy alone which is the basis for current data?
In metastatic lung adenocarcinomas, what are the clinical implications of any potential differences in molecular or histologic features compared with primary tumors?
What are the clinical, epidemiological, molecular, and histologic characteristics of never smokers with lung adenocarcinoma?
MOLECULAR FEATURES
There are several molecular observations that have important implications for lung adenocarcinoma patients: (1) EGFR mutation is a validated predictive marker for response and PFS with EGFR-TKIs in the first-line therapy in advanced lung adenocarcinoma.8,215–218 (2) Tumors with an EGFR mutation have been associated with a more indolent course.8,234 (3) EGFR and KRAS mutations are virtually mutually exclusive.236,255 (4) EGFR/KRAS mutation-negative cases may have detectable fusion of EML4-ALK.153,220
Histogenetic Origins of Lung Adenocarcinoma Subtypes
Normal lung tissues, from which lung cancers arise, can be anatomically divided into two major components, the air-conducting system and the peripheral lung parenchyma where gases are exchanged. After generation of the two embryologic lung buds, repeated branching morphogenesis results in conducting airways and the subsequent development of the terminal sac and alveoli. During the later stages, the regulatory TTF-1 is ubiquitously expressed in the peripheral lung epithelial cells such as small bronchioles and alveoli.256 TTF-1 is potentially a lineage-specific survival oncogene of some lung adenocarcinomas.257,258 The peripheral bronchioloalveolar compartment (terminal bronchioles, alveolar ducts, and alveoli) also contains two potential tumor cells of origin, the Clara cells and type II pneumocytes,259 which together comprise the terminal respiratory unit (TRU) and give rise to tumors expressing TTF-1. These often manifest as a GGN on CT. The central conducting airways (bronchi) contain two potential candidate progenitor cells that give rise to tumors: the bronchial basal cells and the mucous cells.259,260 These tumors are TTF-1 negative and demonstrate a solid appearance on CT. Hierarchical clustering analysis of lung adenocarcinoma based on the expression profile demonstrated two major clusters, which correspond to TRU and non-TRU-type adenocarcinomas and thus two major subsets of adenocarcinoma with distinct histogenetic origins.261
It is hypothesized that a subset of lung adenocarcinomas undergoes progression from AAH to AIS to invasive carcinoma and that this may be a stepwise process triggered by multiple genetic changes that supplement those responsible for initiation of the malignant phenotype.4,77,262,263 Although EGFR and KRAS mutations are observed from the earliest stages including normal epithelium264,265 and AAH, to invasive adenocarcinoma, EGFR gene copy number changes become widespread later at the stage of invasion and metastases.266,267 EGFR, KRAS, and TTF-1 amplification are characteristic of this progression.258,266,268 p53 mutation is more often found in invasive compared with noninvasive adenocarcinomas.48,269–273 Nevertheless, p53 mutation has not been identified as a reliable prognostic marker or a therapeutic target.
Histologic Molecular Correlations
High-throughput analysis of DNA mutations has reshaped the molecular landscape of lung adenocarcinomas.98 DNA sequencing of 623 known cancer-related genes in 188 adenocarcinomas identified 1013 somatic mutations.98 In addition to confirmation of known tumor suppressor genes p53, P16INK4, and STK11/LKB1, newly described mutations in NF1 and RB1 were detected at a frequency of 10% each. There were two other important findings: (1) mutations were often detected in the tyrosine kinase gene family members EGFR, KRAS, ERBB4, EPHA4, EPH3, KDR, and FGFR4 that are potentially targetable by tyrosine-kinase inhibitors and (2) mutual exclusivity was demonstrated in several gene mutation pairs including EGFR/KRAS, EGFR/STK11, and NF1 and p53/ATM.98,274 Mutation frequency showed negative correlations between acinar, papillary, and BAC subtypes with mutations in LRP1B, p53, and INHBA.98 Nevertheless, these mutations showed significant positive correlations with the solid subtype (Table 5).98
TABLE 5.
Adenocarcinoma Histologic Subtypes, Molecular, and Radiological Associations
| Histological Subtype Predominant |
Molecular Features | CT Scan Appearance | Gene Pathways Associated | References |
|---|---|---|---|---|
| Nonmucinous AIS and MIA | TTF-1 + (100%) | GGN, part-solid nodule | Not known | 141, 261, 275–277 |
| EGFR mutation never smokers: 10–30% | ||||
| KRAS mutation smokers: 10–30% | ||||
| Lepidic (nonmucinous) | TTF-1 + (100%) | Part solid nodule | Low cell cycle stimulatory278 | 69, 261, 266, 276, 279–283 |
| EGFR mutation never smokers: 10–30% | GGN or solid nodule | High Wnt | ||
| EGFR amplification: 20–50% | ||||
| KRAS mutation smokers: 10% | ||||
| BRAF mutations: 5% | ||||
| Papillary | TTF-1 + (90–100%) | Solid nodule | Low cell cycle278stimulatory | 69, 98, 264, 266, 279, 280–282, 284–286 |
| EGFR mutation: 10–30% | ||||
| EGFR amplification: 20–50% | High EGFR | |||
| KRAS mutation 3% (lack of KRAS) | High notch | |||
| ERBB2 mutations: 3% | ||||
| p53 mutations: 30% | ||||
| BRAF mutations: 5% | ||||
| Acinar | TTF-1 + or − | Solid nodule | High PDGF278 | 69, 98, 269, 287 |
| KRAS mutation in smokers (20%) | Low EGFR | |||
| EGFR mutations <10% nonsmokers | Low angiogenesis | |||
| EGFR amplification: 10% | ||||
| EML4/ALK translocation: >5% | ||||
| P53 mutations: 40% | ||||
| Micropapillary | KRAS mutations (33%) | Unknown | Unknown | 69, 95, 283 |
| EGFR mutations (20%) | ||||
| BRAF mutations (20%) | ||||
| Solid | TTF-1 (70%) | Solid | High cell cycle stimulatory +278 | 69, 98, 125, 269, 287, 288 |
| MUC1 positive | High angiogenesis | |||
| KRAS mutation smokers: 10–30% | High JAK-STAT | |||
| EGFR mutation never smokers: 10–30% | Low notch | |||
| EGFR amplification: 20–50% | ||||
| EML4/ALK translocation >5% | ||||
| p53 mutation: 50% | ||||
| LRP1B mutations | ||||
| INHBA mutations | ||||
| Invasive mucinous adenocarcinoma | TTF-1 (0–33% positive) | Consolidation, air bronchograms; less often GGO | Not known | 123, 125, 126, 137, 140–142, 286, 289–291 |
| KRAS mutation: 80–100% | ||||
| No EGFR mutation | ||||
| MUC5+ MUC6+ MUC2+ |
AIS, adenocarcinoma in situ; MIA, minimally invasive adenocarcinoma; GGN, ground-glass nodule; EGFR, epidermal growth factor receptor; TTF, thyroid transcription factor.
Many publications have studied the prevalence and specificity of KRAS and EGFR alterations in lung adenocarcinoma (Table 5). The frequency of KRAS and EGFR mutations is each 10 to 30% with higher EGFR mutation frequency in Asians, never smokers, and nonmucinous tumors, whereas KRAS mutations are most common in non-Asians, smokers, and in invasive mucinous adenocarcinoma.140 Mutations in EGFR mainly affect the adenosinetriphosphatebinding pocket within the tyrosine kinase domain. The most common mutations result in an arginine for leucine substitution at amino acid 858 and in-frame deletions at exon 19. EGFR mutation status has been reported to be significantly associated with AIS, LPA, papillary, and micropapillary adenocarcinoma subtypes, although EGFR mutations can be seen in tumors with other histologic subtypes (Table 5). A large cohort of 806 NSCLC specimens showed a correlation between the presence of EGFR mutation and adenocarcinomas formerly classified as BAC or with BAC features (probably including AIS, MIA, and LPA),275 but another study with pathology review of 97 adenocarcinomas showed no difference.274 Predominant solid subtype has been shown to be significantly associated with KRAS mutations288 but not in all studies.69 V600E BRAF mutations, occur in less than 5% of cases, and they have been associated with papillary, micropapillary, and lepidic components of invasive lung adenocarcinomas.95,279 Other less common types of BRAF mutations are reported such as V599E in a patient with a “well differentiated adenocarcinoma” (no subtyping information)292 and two cases with missense mutations in exon 11 (G465V) and in exon 15 (L596R) where no histologic subtyping was reported.293
Table 5 summarizes our present knowledge on the molecular features associated with predominant patterns of adenocarcinoma. The only example of a strong correlation between a histologic subtype and a set of molecular and biologic features is that of invasive mucinous adenocarcinoma (former mucinous BAC), which typically have KRAS mutations and lack of EGFR mutation.55,140,141–144 Most of these tumors are negative for TTF-1, and they may express MUC 2-5-6 because of their derivation from bronchiolar mucinous goblet cells.146,289
EGFR mutation is a specific target for therapy by EGFR-TKIs and is a validated biomarker of treatment response based on three recent phase 3 trials (see detailed explanation in Clinical Recommendation section)8–11 and multiple phase 2 trials.228–233 Recently described mutation-specific antibodies for the EGFR exon 19 deletion and L858R mutation seem to be much more reliable in predicting EGFR mutation status than previous antibodies, but they require further testing and validation in clinical trials.238–240 Specific acquired EGFR mutations such as T790M as well as, other genetic alterations in MET (amplification), ERBB3 (overexpression), and epiregulin (autocrine loop activation), account for approximately 50% of cases of TKI resistance.236,250,294–299
Lung Cancers with ALK Translocations
A minority of lung tumors harbor a small inversion within chromosome 2p giving rise to the transforming fusion gene EML4-ALK. No activating mutations in the kinase domain are observed; the dimerization of the fusion protein causes its activation.246 Epidemiological characteristics include prevalence in 5% of lung adenocarcinomas. Younger age, male gender, and never or light smokers may identify a population of patients with greater chance of harboring this aberration.153,220,248,300 A variety of histologic features are reported including acinar, papillary, cribriform, mucin production (intra- and extracytoplasmic), and signet-ring patterns.153,220,300–304
It is still at issue whether other histological types such as squamous cell carcinoma and mucoepidermoid carcinoma also contain EML4-ALK translocations. Detection of the EML4-ALK translocations can be difficult and can be approached with several methods including immunohistochemistry, FISH, and reverse transcription-polymerase chain reaction.153,248,249,300 –303,305 Immunohistochemistry requires use of antibodies and methods that are validated to correspond well to EML4-ALK translocations, and it may serve as a useful screening method.153,302,306–308 Most tumors with EML4-ALK translocations are positive for TTF-1 and may be p63 positive.301,303 Tumors with EML4-ALK translocations seem to be mutually exclusive with EGFR and KRAS mutations and have a lower frequency of p53 mutations.153,247,300,301,303 Another ALK translocation involving KIF5B-ALK fusion has been recently identified in lung adenocarcinomas; however, at present, insufficient data exist to define its specific histological nature.302 De novo resistance mutations in the kinase domain of EML4-ALK have been reported to develop during ALK inhibitor therapy.249
Lung Adenocarcinoma Gene Expression Analyses
The messenger RNA genomic profiling of tumors can provide important information about pathogenesis, patient prognosis, and prediction of response to therapy in a fashion that complements histological evaluation. Unsupervised clustering analysis consistently shows three distinct groups of adenocarcinomas associated with tumor morphology69,261,309,310 and with lung developmental pathways. Beer et al.309 showed that tumors within the three clusters were significantly correlated with differentiation, stage, and morphology as classified by bronchial-derived or lepidic morphology. Borczuk et al.310 showed that invasive features were associated with the cluster containing more aggressive tumors. The three groups consisted of noninvasive and minimally invasive tumors (≤5 mm); mixed-invasive and lepidic pattern tumors; and solid-invasive cancers. Motoi et al.69 demonstrated that the three clusters correlated strongly with former BAC, solid, and papillary subtypes, respectively. Takeuchi et al.261 showed that expression profile-defined adenocarcinoma subtypes were correlated with morphology and with normal lung developmental pathways. Morphologic analysis revealed two branches consisted of TRU-type adenocarcinomas, which are based on lepidic pattern and expression of TTF-1 and surfactant proteins, and non-TRU adenocarcinomas that lack these characteristics. TRU tumors were further divided into TRU-a and TRU-b classes. Functional annotation showed retention of normal peripheral differentiated lung features in the TRU types, which contrasted with the cell cycling and proliferation enriched annotation of genes associated with the non-TRU tumors.
Although EGFR mutations are found in association with papillary predominant adenocarcinomas (Table 5)69,98 and TRU-a tumors, whereas KRAS mutations are more frequent in the solid and TRU-b tumors, it is clear that oncogene mutation status is not a primary determinant of the molecular subtypes as defined by gene expression profiling.311 Taken together, unsupervised clustering defines three morphologically distinct groups of lung adenocarcinomas. These include (1) AIS and MIA; (2) invasive nonsolid adenocarcinoma; and (3) invasive adenocarcinoma, predominantly solid.69,261,309,310 Thus, these molecular profiles provide biological plausibility for the proposed classification scheme that creates separate categories based on evaluation of lepidic pattern and other components, including solid pattern.
Recently Bryant et al.278 used the lung adenocarcinoma gene expression data from Shedden et al.99 together with complete pathological review to examine associations between 27 known cancer-related pathways and the adenocarcinoma subtype, clinical characteristics, and patient survival. Unsupervised clustering of adenocarcinoma and gene expression enrichment analysis reveals three main clusters and that cell proliferation is the most important pathway separating tumors into subgroups.278 Further, adenocarcinomas with increased cell proliferation demonstrate significantly poorer outcome and an increased solid subtype component. Interestingly, tumors with any solid component have decreased survival, when compared with tumors without a solid component. Significant associations between specific histologic subtypes, gene expression pathways, and clusters were also reported, some of these are included in Table 5. The consistency of these findings was demonstrated using two independent lung adenocarcinoma cohorts from Japan (N = 87) and France (N = 89) using the identical analytic procedures.278
Tumor messenger RNA profiling is emerging as a source of clinically significant information regarding patient outcome after resection. Several predictors have been developed based on methodologically sound approaches that include independent validation.312–324 The results of these studies are heterogeneous in terms of the number of genes both in the predictors and in the specific genes included in each signature. This heterogeneity is expected given differences in study design, assay platform, tumor histology, and patient selection. A large, multicenter, blinded evaluation of eight independently derived genomic signatures of prognosis in 442 adenocarcinomas demonstrated that the addition of clinical covariates enhanced the performance of the signatures, relative to using gene expression alone.99 A method that relied on the correlated expression of 100 gene clusters to predict subject outcome produced relatively good performance with several other methods showing similar performance.99 Relatively higher expression of a cluster of 545 genes enriched for cell proliferation was associated with poor outcome. This study is a model for the careful handling of challenges inherent in translational cancer genomic studies and for its vast repository of clinical and pathologically annotated data. Independent prospective evaluation of the predictive accuracy of these signatures, prospective clinical trials, and application to small biopsy specimens200–203 will be required to extend this area of research.
Copy Number Analyses of Lung Adenocarcinoma Subtypes
Multiple studies have defined lung adenocarcinoma subtypes by using techniques to assess DNA copy number changes.41,69,257,280,284,325–327 Adenocarcinoma subtype was examined in a comprehensive analysis using CGH by Aviel-Ronen et al.,326 who contrasted former BAC and invasive mixed-type adenocarcinoma with former BAC features, most of which would probably be classified as invasive adenocarcinoma with predominant lepidic growth in the new classification. A large number of specific chromosomal alterations were detected such as gain at 1p, 2q, 5p, 7p, 11p, 11q, 12q, 16p, 16q, 17q, 20q, and 21q in both former BAC and the adenocarcinomas with lepidic growth. Although both types had similar chromosomal changes, the invasive adenocarcinomas with lepidic growth showed greater variability and frequency of chromosomal changes and with longer segmental alterations and deletions. Deletions were also more common in adenocarcinomas with lepidic growth and were observed mainly on 3p and 5q and to a lesser extent on 4q and 6q. The genomic profile of former BAC seems to be distinguishable from that of invasive adenocarcinoma with lepidic growth, with the latter displaying greater genomic aberrations. This demonstrates a progression at the genomic level from former BAC to the invasive areas of adenocarcinoma with lepidic growth.
Weir et al.257 found the most common focal amplification event in lung adenocarcinoma involved chromosome 14q13.3 in 12% of cases and TTF-1, also known as NKX2-1 was identified in this region. Barletta et al.41 examined histologic correlations with amplification of the TTF-1 gene, and six cases demonstrated TTF-1 amplification among the 49 acinar, papillary, and solid subtypes but not in tumors classified formerly as BAC.
EGFR gene amplification was examined using FISH by Hirsch et al.,284 who demonstrated that EGFR gene copy number detected by FISH is associated with improved response to gefitinib therapy in patients with advanced-stage former BAC and in adenocarcinomas with lepidic growth. A strong relationship between mutation and EGFR amplification was also reported by Cappuzzo et al.328 Conde et al.280 reported similar results with a higher percentage of mutations among adenocarcinomas with former BAC and papillary morphologies relative to adenocarcinomas without these features. Chang et al.327 used CISH and found that TKI responsiveness was significantly associated with EGFR mutation and adenocarcinoma morphology but only marginally with increased EGFR gene copy number. Other studies report similar findings, but the relationship between adenocarcinoma subtype and EGFR copy number changes is often not indicated.195,198,287 Motoi et al.69 was one of the first studies to examine this and found no strong correlations between adenocarcinoma subtype and EGFR amplification using CISH.
EGFR copy number analysis during the progression of adenocarcinomas has been examined.264,267 EGFR mutations precede copy number abnormalities. EGFR copy number heterogeneity was greater in the primary tumor than in corresponding metastases.264 EGFR amplification correlated with high histologic grade and/or invasive growth and was rare in the precursor lesions AAH and former BAC.267 Thus, tumors with these changes appear more aggressive. Zhu et al.236 showed that using a multivariate Cox model, high EGFR copy number was both a significant prognostic factor for poor survival (HR: 1.93, CI: 1.09 –3.44, p < 0.025) and a significant predictive factor of an erlotinib effect on survival (HR: 0.33, CI: 0.15– 0.71, p < 0.005). The amplification of MET may be one possible mechanism associated with tumor resistance to erlotinib.267 Finally, the application of these types of FISH analyses to small diagnostic samples was examined by Zudaire et al.201 They found that more than 90% of cases of paraffin-embedded transthoracic FNA samples were suitable for FISH for both EGFR and c-MYC analyses. These studies suggest that even when limited tumor material is available, copy number analyses may provide prognostic information for EGFR amplification and an explanation for resistance to EGFR-TKIs for MET amplification. Nevertheless, EGFR mutation is more predictive of response to EGFRTKIs than amplification.198,241
Multiple Pulmonary Nodules
Several techniques have been tested to distinguish metastases from synchronous primary tumors including DNA microsatellite analysis,329,330 CGH,331 DNA mutation sequencing,332–336 immunohistochemistry,337 and gene expression analysis. The utility of these assays is enhanced by their potential application to small biopsy specimens. These approaches have not been prospectively validated; thus, their performance and efficacy in routine clinical practice remain to be established. Nevertheless, these molecular techniques offer promising new ways to help in the distinction of synchronous primary tumors from metastases in patients with multiple adenocarcinoma nodules, which is critical for accurate tumor staging, determination of prognosis, and for planning treatment.338,339
Molecular Differences in Metastases versus Primary Tumors
There may be important differences between the primary tumor and metastases of lung adenocarcinoma both with respect to morphology and biomarker expression; however, more study of this problem is needed.340 The mutation status of metastases can be the same341,342 or different from that of the primary tumor and also among metastases, so a multidisciplinary approach is needed.343,344 The available data regarding EGFR mutations is mainly from tumor material collected at the time of diagnosis (either from the primary tumor or from metastases) and not from the point in time at which treatment with EGFR inhibitors is given.
Molecular Prognostic Factors
Biomarkers that can predict patient prognosis have been extensively sought during the past 20 years. Immunohistochemical markers for which meta-analyses have been done include EGFR,345 TTF-1,346 p21ras,347 HER2,348 p53,349,350 Ki67,351 BclII,352 and cyclooxygenase 2.353 All but EGFR, p21 ras, and cyclooxygenase 2 were statistically significant by meta-analysis. Nevertheless, the magnitude of the association is generally weak with HRs that range from 1.13 to 1.57.
Meta-analyses347,349,350 showed that although prognostic impact of mutations of p53 or KRAS gene might be statistically significant, their impact was not strong enough to be recommended for routine clinical use. In contrast, there is a suggestion that patients who underwent surgical resection for lung adenocarcinomas that have EGFR mutations seem to have better prognosis in the absence of EGFR-TKI therapy than those without, based on two retrospective observational studies.354,355
Molecular Research Recommendations
More investigation is needed of copy number variation, genomic, and proteomic markers for their relationship to clinical and pathologic variables.
EML4-ALK fusion gene needs further study, particularly in EGFR/KRAS-negative cases.
We recommend that research studies of molecular markers be based on well-annotated clinical and pathologic datasets, with adenocarcinomas diagnosed according to this classification.
MicroRNAs need further evaluation to determine whether they can be helpful in lung adenocarcinoma risk stratification and outcome prediction.356,357 There is limited information regarding correlation with adenocarcinoma subtype classification.
Investigations combining both genomic and proteomic studies are needed to determine whether they can provide more accurate subclassification of NSCLC and adenocarcinoma, and more precise information regarding the risk stratification, outcome prediction, and treatment selection for different subtypes of adenocarcinoma.
RADIOLOGIC FEATURES
A number of terms have been used to describe lung adenocarcinomas by CT imaging. In particular, for tumors that present as small nodules, the terms used have reflected the various ground glass (nonsolid), solid, or part-solid appearances that can occur. Largely based on the Fleischner Society glossary of terms358 and the recently suggested guidelines by Godoy and Naidich359 for subsolid nodules, we propose the following definitions: (1) a pure GGN (synonym: nonsolid nodule) as a focal area of increased lung attenuation within which the margins of any normal structures, e.g., vessels, remain outlined, (2) a solid nodule as a focal area of increased attenuation of such density that any normal structures, e.g., vessels, are completely obscured, and (3) part-solid nodule (synonym: semisolid nodule) as a focal nodular opacity containing both solid and ground-glass components.358,359 The Fleischner Society glossary of terms for thoracic imaging defines a nodule on a CT scan as “a rounded or irregular opacity, well or poorly defined, measuring up to 3 cm in greatest diameter” in any plane.358 If the opacity is greater than 3 cm, it is referred to as a mass.358 The ≤3 cm cutoff is in keeping with our concept of the maximum accepted size for the pathologic diagnosis of AIS and MIA. The term subsolid nodule has also entered common radiologic usage, referring to both part-solid nodules and pure GGN.359 Optimal evaluation of subsolid nodules requires thin-section CT scans (≤3 mm thickness) to assess the solid versus ground-glass components.359,360
Radiologic Spectrum According to Histologic Subtype
AAH is the earliest preinvasive lesion for lung adenocarcinoma detectable by thin-section CT. It appears as a small (usually ≤5 mm), GGN (Figure 11).19,23,129,361–365 AAH characteristically appears as a very faint pure GGN usually measuring ≤5 mm.130,366 The pure GGN of AAH can be single or multiple.129,365,367
Figure 11.

CT of preinvasive lesion (AAH or AIS). Axial 2-mm image through the left upper lobe shows a 5 mm pure ground-glass nodule (GGN), which has remained stable for 8 years (arrow). AAH and AIS can be single or multiple. AIS, adenocarcinoma in situ; CT, computed tomography.
AIS is best demonstrated at CT (preferably thin section) and sometimes can be seen on chest radiography. It is a noninvasive lesion and nonmucinous AIS presents typically as a pure GGN (Figure 12) but sometimes as a part solid or occasionally a solid nodule.19,23,128,131,362,367–370 AIS can be bubble like.131,365,370,371 Mucinous AIS can appear as a solid nodule or consolidation (Figure 13). The pure GGN of AIS usually appears at thin-section CT as slightly higher attenuation than the very faint GGN of AAH.130,366,367 AIS also can be single or multiple.19,128,131,365,370
Figure 12.

CT of a peripheral 2 cm nonmucinous AIS. A, Axial CT section. B, Coronal maximal intensity projection (MIP) image shows a pure GGN in the left lower lobe. Vessels and lung architecture are seen through the nodule. AIS, adenocarcinoma in situ; CT, computed tomography; GGN, ground-glass nodule.
Figure 13.

CT of mucinous adenocarcinoma in situ; 2 cm predominantly solid nodule with air bronchogram (arrow) is noted in the left upper lobe. CT, computed tomography.
MIA is variable in its imaging presentation and is, as yet, not fully described, but a provisional description of the nonmucinous type at thin-section CT is a part-solid nodule consisting of a predominant ground-glass component and a small central solid component measuring 5 mm or less (Figure 14).47,58 Mucinous MIA (Figure 14) is less common than nonmucinous MIA and appears as a solid or part-solid nodule.52,93,126 There is an overlap among imaging features of AAH, AIS, and MIA.
Figure 14.

CT of nonmucinous minimally invasive adenocarcinoma. Axial 2-mm CT section shows a peripheral, predominantly ground-glass, part-solid nodule in the right upper lobe that includes a 4 × 3 mm solid component (arrow), which corresponded to invasion by pathology. CT, computed tomography.
Radiology Recommendation 1
When an opacity in the lung adenocarcinoma spectrum is either a pure GGN or part-solid nodule with a predominant ground-glass component, we recommend that the term BAC no longer be used. These tumors should be classified by the new terms: AIS, MIA, and LPA (strong recommendation, low-quality evidence).
Invasive adenocarcinoma is usually a solid nodule (Figure 15) but may also be part solid (Figure 16) and occasionally a GGN.23,58,103,125,129 –134,367,370–372 A lobar pattern of ground-glass opacity (GGO) may occur (Figure 17). Bubble-like or cystic lucencies in stage IA adenocarcinoma have been described as correlating with well-differentiated tumors131,132,370,371,373,374 and slow growth.132,374 Thick (≥2 mm) coarse spiculation has been associated with lymph node metastasis, vascular invasion, and decreased survival post resection.23,375 For stage IA adenocarcinoma presenting as a part-solid nodule, an extensive ground-glass component suggests a favorable prognosis.18,20,23,103,105,376–388 Histologically, the ground-glass component typically corresponds to a lepidic pattern and the solid component to invasive patterns. An intratumoral air bronchogram usually indicates a well-differentiated tumor.132,370,375,387 Absence of pleural retraction for stage IA adenocarcinoma is also a favorable prognostic sign.375,389 In solid adenocarcinomas, the presence of notches, or concave cuts on thin section CT, has been associated with poor differentiation on histology and adverse outcome.390
Figure 15.

CT and FDG-PET of invasive adenocarcinoma. A, Axial CT image and (B) FDG-PET images show a 2-cm spiculated hypermetabolic solid nodule in the left lower lobe. CT, computed tomography; FDG-PET, fluorodeoxyglucose positron emission tomography.
Figure 16.

Invasive adenocarcinoma. A, Axial CT image shows a part-solid nodule in the left upper lobe. B, Corresponding sagittal CT images show automated estimation of the volume of (B) the solid component (1.188 cm3) and (C) the entire lesion (8.312 cm3). In this case, if tumor size were measured only by the invasive component, the size T factor would change from T2a (3.2 cm) to T1a (1.8 cm). Recording of total and invasive sizes are suggested until it is known whether invasive size predicts prognosis better than total size. CT, computed tomography.
Figure 17.

CT of nonmucinous lepidic predominant adenocarcinoma. CT images show (A) predominantly GGO in the right upper lobe and (B) multiple GGN in the right lower lobe. CT, computed tomography; GGN, ground-glass nodule.
Invasive mucinous adenocarcinoma, formerly called mucinous BAC, characteristically presents in imaging studies as a range of nodules to lobar replacement by a spectrum of patterns including GGO, mixed GGO/solid foci, or consolidation,126,128 but intraalveolar mucus may make the CT appearance solid or nearly solid (Figs. 18 and 19).125,391 The mucoid component may appear as homogeneous consolidation with soft-tissue attenuation that is lower than that of muscle. After administration of an intravenous iodinated contrast agent, vessels are well shown traversing these regions (CT angiogram sign).126,125,133,391 Overlap does occur between imaging features of mucinous and nonmucinous invasive adenocarcinomas.
Figure 18.

CT of invasive mucinous adenocarcinoma. A, Axial and (B) coronal CT images show multilobar consolidation and nodules mixed with GGO. Air bronchograms are present. CT, computed tomography; GGO, ground-glass opacity.
Figure 19.

CT and FDG PET of invasive mucinous adenocarcinoma. A, Coronal CT and (B) FDG-PET images show a hypermetabolic hypodense solid 4 cm mass in the right lower lobe. CT, computed tomography; FDG-PET, fluorodeoxyglucose positron emission tomography.
Radiology Recommendation 2
For overtly invasive adenocarcinomas previously classified as mucinous BAC, we recommend they be separated from nonmucinous adenocarcinomas and be classified as invasive mucinous adenocarcinoma (strong recommendation, moderate quality evidence).
Remark: At CT, this entity is usually solid or mostly solid, has frequent air bronchograms, shows a lobar or multilobar distribution, and frequently consists of multiple nodular or consolidative opacities (former term multicentric BAC).
Size and Growth Rate of Lesions
AAH characteristically is ≤5 mm but in a minority of cases may be up to 12 mm.19,276,129,363,364,368 Growth is very slow. Although it has been suggested that a pure GGN less than 5 mm is so unlikely to become a cancer that it needs no follow-up,359 optimal frequency and duration of CT follow-up of a GGN of any size are as yet unclear.
AIS is variable in size, but most are 2 cm or less. Growth is very slow. Suspicious GGNs, i.e., ≥5 mm diameter, are usually followed by at least annual follow-up CT examination, and an increase in size or attenuation is regarded as a sign of probable progression to invasive disease.359 For sizes more than 10 mm, closer follow-up is indicated with CT every 6 months to 1 year. Nevertheless, all recommendations for following suspicious GGNs to date have been based on data from small observational studies and need further evaluation.131,361,368,372,387,392–394
MIA has not yet been well defined in terms of imaging findings, in part, because the histopathologic definition is difficult, and little is known about size and growth rates, but most MIA are less than 2 cm.58 Invasive adenocarcinomas of the lung are variable in size and growth rates. For adenocarcinoma less than 2 cm, the smaller the tumor, the less likely there is to be vascular invasion.373 Size of an adenocarcinoma does predict metastatic disease to the central nervous system: for a node-negative adenocarcinoma of 2 to 6 cm, the probability of metastatic disease to the central nervous system has been reported as 0.14 for a 2 cm tumor, increasing linearly to 0.72 for a 6 cm tumor.395,396
For small solid nodules suspicious for lung cancer at CT, the recommendations for follow-up per Fleischner Society guidelines are currently widely recognized.397–399 Nevertheless, these guidelines do not specifically address GGNs and part-solid nodules, as discussed by Godoy and Naidich.359
Because the sizes of many of the clinically problematic nodular lesions at CT are small, how size is measured is especially important. Differences in CT scanners, window settings, and inter- and intraobserver performance are common and may impact critically on assessments of size, especially in the CT follow-up of nodular lesions.400–405
Multiple Primary Lung Cancers
Multifocal lung adenocarcinomas are not uncommon, being found in up to 8 to 22% in surgically resected adenocarcinomas406,407 and 18% of adenocarcinomas detected in screening programs.64 Multiple lung adenocarcinomas can occur in the setting of multiple AAH, AIS, and invasive adenocarcinoma (Figure 20).365 Similarities or differences in attenuation may provide clues regarding the relative percentage of lepidic versus solid histologic components.359 Subsolid nodules are very rarely metastatic.408
Figure 20.

CT of multicentric GGNs of AIS/AAH. A and B, Multiple subsolid nodules (arrows) on axial 3-mm CT images show differing sizes and attenuation. These were presumed to represent preinvasive lesions (AAH and AIS). Because the dominant nodule in the right upper lobe posteriorly near the fissure in part A (large arrowhead) appears somewhat dense, it was excised surgically and found to be nonmucinous AIS. AAH, atypical adenomatous hyperplasia; AIS, adenocarcinoma in situ; CT, computed tomography; GGN, ground-glass nodule.
Positron Emission Tomography (Scanning)
Elevated standard uptake values (SUVs) on fluorodeoxyglucose positron emission tomography (PET) correlate with cellular proliferation and aggressiveness of the primary cancer (Figures 15 and 19).369,409–417 Sensitivity of PET for AIS is usually very low.410,414 PET is commonly used for staging and follow-up of invasive adenocarcinoma, and for lesions of 7 mm or larger, SUV for adenocarcinoma of the lung tends to be lower than for other histologic types of lung cancer and correlate inversely with survival.416,418,419 PET may be more accurate than CT for assessing response to chemotherapy, although more studies are needed.420,421 For mucinous versus nonmucinous adenocarcinoma, after adjusting for size of the lesion, no significant difference in SUV has been found.125 For a small, well-differentiated adenocarcinoma of low fluorodeoxyglucose avidity (e.g., maximum SUV <2.5), follow-up PET to assess change in SUV as a diagnostic tool unfortunately seems to be of only limited value.422
Magnetic Resonance
Magnetic resonance has been investigated as a method for differentiating among small AIS, mixed invasive adenocarcinoma/ AIS, and invasive adenocarcinoma.285,423 In the studies by Ohno et al. and Tanaka et al.,285,423 for the distinction of AIS/lepidic predominant (former BAC) from invasive adenocarcinoma, sensitivity was 86% and 97%, and specificity was 100% and 77%, respectively.
Imaging-Guided Percutaneous Needle Biopsy for Molecular and Immunohistochemical Correlations
Percutaneous imaging-guided needle biopsy, whether obtained by aspiration or as a core, allows molecular characterization from even minimal samples.200,201,203
Radiology Recommendations
When an opacity in the lung adenocarcinoma spectrum is either a pure GGN or part-solid nodule with a predominant ground-glass component, we recommend that the term BAC no longer be used. These tumors should be classified by the new terms: AIS, MIA, and LPA (strong recommendation, low-quality evidence).
For overtly invasive adenocarcinomas previously classified as mucinous BAC, we recommend they be separated from nonmucinous adenocarcinomas and be classified as invasive mucinous adenocarcinoma (strong recommendation, moderate quality evidence).
Remark: At CT, this entity is usually solid or mostly solid, has frequent air bronchograms, shows a lobar or multilobar distribution, and frequently consists of multiple nodular or consolidative opacities (former term multicentric BAC).
Radiology Considerations for Good Practice
Radiologists performing biopsies should obtain sufficient tissue not only for traditional microscopic analysis but also for immunohistochemical and molecular analysis.
Thin-section CT technique should be used for part-solid lesions, to record the size of (a) the solid component and (b) total tumor size, including both solid and ground-glass components (Figure 16).
Changes in shape, size, and attenuation help determine follow-up and when intervention is appropriate.
Radiology Research Recommendations
What is the natural history of single and multiple GGNs? The frequency of invasive transformation of these lesions is unknown.
How should tumor size be measured: single largest diameter, bidimensional, volume? For part-solid lesions, size of both the entire lesion and solid component should be mentioned, because prognosis as a function of size is not yet well established in terms of the dimensions of the solid component. Correlation of the measurement of the solid component of part-solid lesions and size of the invasive component at histopathologic assessment is also needed. Careful attention to thin-section CT technique to assess changes over time in sizes of small adenocarcinomas of the lung is warranted. Inter- and intraobserver differences among radiologists for measurements of the size of a nodule remain an important arena for inquiry.400,402 Volumetric measurements also offer promise for assessing changes in size of indeterminate nodules, but error—both human and computer—remains an issue for small GGN, including identifying a possible solid component (Figures 17B, C).405,424,425
What is the CT attenuation according to the newly proposed lung adenocarcinoma histologic subtypes? CT histogram analysis suggests that attenuation characteristics may differ among AAH, AIS, and MIA.366 Further investigations of these lesions using quantitative analysis are in order.
In the setting of multiple adenocarcinomas, can careful description of the attenuation (e.g., relative extent of ground glass versus solid components) for each nodule assist in the determination whether the nodules are metastases versus synchronous or metachronous primary carcinomas, similar to the way comprehensive histologic subtyping is helpful pathologically?102
How can this new classification impact CT screening? Screening may reveal small cancers early in their natural history,64,372,426–434 and cost/benefit issues, both medical and economic, remain an arena of active current research.424,435–439
What molecular correlations can be made with the spectrum of radiologic patterns of lung adenocarcinoma? Not many studies have attempted correlation of imaging and molecular findings. EGFR mutations have been described as correlating with more than 50% GGO,271,440,441 with size less than 3.5 cm440,442 and with a high SUV level at PET of advanced-stage disease.440,443 Ki-67 has been described as associated with high SUV levels at PET444,445 and with dedifferentiation of the tumor.445
SURGICAL FEATURES
The newly proposed adenocarcinoma classification, particularly introduction of the concepts of AIS and MIA, raises surgical issues to which no definite answer is available yet. This relates to sublobar resection for early-stage lung cancer, role of chest CT in selecting patients for sublobar resection, specific surgical approach for these lesions, extent of lymph node dissection, the role of frozen section analysis, and the treatment of multiple small lung cancers.
Is Sublobar (Limited) Resection Adequate Oncologic Treatment for Some Early Adenocarcinomas?
One of the main reasons for defining the concepts of AIS and MIA in this classification is to raise the question whether these diagnoses can be anticipated by a GGO appearance on CT when presenting as a small, solitary lesion and whether limited resection may be effective therapy for such lesions. Lobectomy is still considered standard surgical treatment for tumors 2 cm or less in size, which have a solid appearance on CT, because such tumors are invasive carcinomas. Whether there can be any change in this standard care for lesions that present with a GGO appearance on CT awaits the results of two randomized trials (Japan Clinical Oncology Group, JCOG 0802 in Japan and CALGB 140503 in North America) that randomize such patients to either lobectomy or sublobar resection. Recently, there have been numerous retrospective studies that have suggested that sublobar (limited) resection for early lung cancers may be adequate surgical treatment; however, these are not randomized trials.24–26 Most reports showed no difference in survival or in locoregional recurrence between lobectomy and sublobar resection for tumors 2 cm or less in size. Tumors with a GGN (GGO) appearance on CT are reported to have 100% disease-free survival at 5 years after complete resection.18–21
Can CT be Used to Select Patients for Sublobar Resection?
In performing sublobar resections, several important factors affect the appropriateness of this intervention. These include the location (peripheral versus central), appearance (ground glass versus solid), and size (T1a versus T1b versus T2) of the tumor. CT images, especially obtained by high-resolution CT scan with thin slices, are indispensable to evaluate these factors, and recent studies show rather good image-pathological correlations.359 In recent studies correlating CT findings of GGOs with histopathology, many of these lesions, though not all, correspond to preinvasive, noninvasive, or early forms of neoplastic growth, especially those of adenocarcinoma lineage.18–23,359,424
Is There a Difference in Outcome between Video-Assisted Thoracoscopic surgery versus Thoracotomy in the Treatment of Early-Stage Lung Adenocarcinoma?
Several series suggest that there is no difference in overall survival between patients who have lobectomies performed by video-assisted thoracoscopic surgery (VATS) versus those performed by thoracotomy for clinical stage I non-small cell lung cancer.446,447 Morbidity seems to be lower with the VATS approach. VATS is a standard approach for peripheral wedge resections; VATS segmentectomy is much less widely performed and requires further evaluation.448
What can be Expected of Pathologists at Frozen Section?
For a limited resection to be adequate oncologically, a precise pre- and intraoperative diagnosis is critical. The accuracy of intraoperative frozen section analysis in determining whether small lung adenocarcinomas have an invasive component still needs to be defined. The predictive value of frozen section ranges from 93 to 100% but not all articles clearly report the accuracy of frozen section analysis.65–67,449
Evaluation of margins by frozen section may be problematic, especially when stapler cartridges have been used on both sides. Scraping or washing of staple lines with subsequent cytological analysis has been attempted.450,451 When a sublobar resection is performed, frozen section analysis of an interlobar, hilar, or any suspicious lymph node is a useful staging evaluation, and when positive nodes are found, a lobectomy is indicated when there is no functional cardiopulmonary limitation.
Should a Systematic Lymph Node Dissection be Performed in Every Early-Stage Adenocarcinoma?
The necessity of systematic hilar and mediastinal lymph node dissection is based on the fact that approximately 20% of pulmonary adenocarcinomas ≤20 mm and 5% of cases ≤10 mm in size are reported to have nodal metastases.452–454 Lobe-specific nodal dissection, which limits dissection to the primary nodal regions draining the involved lobe, has been shown to be a potentially adequate alternative to complete systematic nodal dissection.26,455,456 A recently reported multicenter prospective clinical trial randomizing patients with intraoperatively staged T1–2N0 nonhilar N1 NSCLC to lymph node sampling versus systematic nodal dissection showed that systematic nodal dissection identified occult disease in 3.8% of patients but was not associated with a benefit in overall survival.457 These results should not be generalized to higher stage tumors. Recent studies also show that in some specific subsets of very early-stage adenocarcinoma, especially GGO lesions, systematic lymph node dissection is not always required.458
Multiple Lesions
In the setting of multifocal lung adenocarcinomas, when there is no evidence of mediastinal lymph node invasion, multiple nodules are not a contraindication for surgical exploration.64,459 A standard treatment algorithm for multiple lesions has not yet been established. Several factors have to be taken into consideration: number and size of the different nodules, synchronous versus metachronous lesions, ipsilateral versus contralateral, primary versus metastatic lesions, and specific nature (AAH, AIS, and MIA).
Surgery Research Recommendations
The precise role of limited resection has not been determined yet because of a lack of randomized prospective trials.
The extent of lymph node dissection remains controversial.
The accuracy of frozen section in assessing the presence of invasive adenocarcinoma and the accuracy of frozen section or cytology of resection margins in sublobar resections need to be investigated further, and specific guidelines for frozen section analysis should be developed to guide intraoperative decisions.
Treatment of multiple lesions has not been standardized.
CLASSIFICATION IN A LOW-RESOURCE SETTING
Although this lung adenocarcinoma classification is written to incorporate special stains and molecular techniques, it is understood that some patients will need to be managed without immunohistochemical or molecular data. This may occur in parts of the world where resources are limited, or it may happen in academic centers where the additional tissue required for special studies is not available. This section briefly outlines how this classification can be applied in such situations.
Pathologic Classification
In the absence of molecular, immunohistochemical, or histochemical testing, the diagnosis and subclassification of lung adenocarcinoma are based purely on light microscopic evaluation of pathologic material.
Resection Specimens
For resection specimens, the two situations where special stains may be useful include solid adenocarcinoma, for which mucin stains can help in the distinction from large cell carcinoma, and for which NE markers can help diagnose LCNEC. In the former situation, if an adenocarcinoma shows a pure solid pattern without acinar, papillary, or lepidic patterns, sometimes intracytoplasmic mucin can be seen on H&E stains. If this cannot be detected, the tumor should be classified as large cell carcinoma, mentioning that it was not possible to perform special stains. If a non-small cell carcinoma shows NE morphology and NE immunohistochemical markers cannot be performed, the tumor should be classified as large cell carcinoma with NE morphology and a specific comment should be made that the tumor could be LCNEC but that material was not available to confirm this immunohistochemically.
Small Biopsies and Cytology
For small biopsies, if clear glandular or squamous differentiation is seen morphologically, the tumor can be classified as adenocarcinoma or squamous cell carcinoma, respectively. If there is some level of uncertainty, this can be reflected by the phrase: poorly differentiated non-small cell carcinoma, favor adenocarcinoma (or squamous cell carcinoma), mentioning in a comment that special stains were not available, and this diagnosis is based purely on light microscopic morphology. If no morphologic features of glandular or squamous differentiation are seen, the tumor should be classified as poorly differentiated NSCLC-NOS.
Clinical, Radiologic, and Surgical Approach to Aid Management of Patients in the Absence of Molecular or Immunohistochemical Data
Evaluation of patients with lung adenocarcinoma should be no different if the diagnosis is established in the absence of special techniques.
Whenever possible, a chest CT extending to adrenals and liver should be used for radiologic evaluation of such patients. In a low resource setting, chest radiography may reveal the primary lung cancer, pleural effusions, and involvement of lymph nodes or bones; however, given the much lower resolution with radiographs compared with CT, an attempt to obtain a chest CT examination should be made for accurate diagnosis and staging of tumor when possible.
If patients diagnosed in low resource settings may subsequently have tissue tested with molecular or immunohistochemical studies, tissue should be managed appropriately to make this possible.
Clinical management of lung adenocarcinoma patients without information about molecular status such as EGFR or KRAS mutations consists of standard surgical and chemotherapeutic approaches based on tumor, node, and metastasis (TNM) staging.
IMPLICATIONS OF THIS CLASSIFICATION FOR TNM STAGING
There are several important implications of this new adenocarcinoma classification for staging that need to be considered for the next revision of the TNM classification. The changes relating to the concepts of AIS, MIA, and LPA parallel classification criteria and terminology currently used in breast cancer,460 but they would not be applicable to other histologic types of lung cancer. In addition, the comprehensive histologic subtyping approach to assessing invasive adenocarcinomas in this classification provides a useful approach to staging multiple adenocarcinomas.
AIS would be classified as Tis. Nevertheless, because carcinoma in situ (CIS) can occur with both lung squamous cell carcinoma and adenocarcinoma, these should be specified as Tis (squamous) or Tis (adenocarcinoma), similar to breast cancer where there is Tis for ductal CIS and Tis for lobular CIS.
MIA would be classified as T1mi, similar to microinvasive breast cancer, which defined as an invasive carcinoma with no focus measuring greater than 1 mm; however, the size for MIA is not greater than 5 mm.
Also, similar to breast cancer, the size T factor for adenocarcinomas with an in situ or lepidic component may best predict prognosis according only to the size of the invasive component rather than the way it is currently done including total tumor size including both the invasive and the lepidic or in situ components. In early-stage tumors, the tumor size T factor may need to be adjusted from total tumor size to only the size of the invasive component. This needs to be tested radiologically and pathologically by comparing survival according to total tumor size (GGO plus solid components by CT versus invasive versus in situ/lepidic components pathologically) compared with analysis only by the size of the solid or invasive component by CT and pathology examinations, respectively.
For multiple lung adenocarcinomas, comprehensive histologic subtyping can help in distinguishing intrapulmonary metastasis versus synchronous or metachronous primaries.102 The role of molecular testing in this setting is promising but needs further study.331
Many of these concepts need to be tested vigorously in the next 5 years in both early- and advanced-stage lung adenocarcinoma to determine whether they are robust enough to warrant changes in the 8th Edition TNM classification.
ACKNOWLEDGMENTS
The authors thank Isabel Sulimanoff, MSKCC Senior Reference Librarian, for expert assistance with developing the search strategy and literature search and Drs. Holger Schunemann of the ATS Documents Development and Implementation Committee for advice about the systematic review and Thomas Barker, for administrative assistance.
Writing Committee: William D. Travis, Elisabeth Brambilla, Masayuki Noguchi, Andrew G. Nicholson, Kim R. Geisinger, Yasushi Yatabe, David G. Beer, Charles A. Powell, Gregory J. Riely, Paul E. Van Schil, Kavita Garg, John H. M. Austin, Hisao Asamura, Valerie W. Rusch, Fred R. Hirsch, Giorgio Scagliotti, Tetsuya Mitsudomi, Rudolf M. Huber, Yuichi Ishikawa, James Jett, Montserrat Sanchez-Cespedes, Jean-Paul Sculier, Takashi Takahashi, Masahiro Tsuboi, Johan Vansteenkiste, Ignacio Wistuba, and Pan-Chyr Yang.
Some of these, which are owned by Cornell Research Foundation (CRF) are non-exclusively licensed to General Electric. As an inventor of these patents, Dr. Yankelevitz is entitled to a share of any compensation which CRF may receive from its commercialization of these patents.
Footnotes
Disclosure: The other authors declare no conflicts of interest.
REFERENCES
- 1.Boyle P, Levin B. World Cancer Report 2008. Lyon: International Agency for Research on Cancer; 2008. [Google Scholar]
- 2.Parkin DM, Bray F, Ferlay J, et al. Global cancer statistics 2002. CA Cancer J Clin. 2005;55:74–108. doi: 10.3322/canjclin.55.2.74. [DOI] [PubMed] [Google Scholar]
- 3.Curado MP, Edwards B, Shin HR, et al. Cancer Incidence in Five Continents. IX. Lyon: IARC Scientific Publications; 2007. [Google Scholar]
- 4.Travis WD, Brambilla E, Muller-Hermelink HK, et al. Tumours of the Lung, Pleura, Thymus and Heart. Lyon, France: IARC Press; 2004. Pathology and Genetics. [Google Scholar]
- 5.Travis WD, Colby TV, Corrin B, et al. Histological Typing of Lung and Pleural Tumors. Berlin: Springer; 1999. [Google Scholar]
- 6.WHO. Histological Typing of Lung Tumours. Geneva: World Health Organization (WHO); 1967. [Google Scholar]
- 7.WHO. Histological Typing of Lung Tumors. Geneva: World Health Organization (WHO); 1981. [Google Scholar]
- 8.Mok TS, Wu YL, Thongprasert S, et al. Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma. N Engl J Med. 2009;361:947–957. doi: 10.1056/NEJMoa0810699. [DOI] [PubMed] [Google Scholar]
- 9.Mitsudomi T, Morita S, Yatabe Y, et al. Gefitinib versus cisplatin plus docetaxel in patients with non-small-cell lung cancer harbouring mutations of the epidermal growth factor receptor (WJTOG3405): an open label, randomised phase 3 trial. Lancet Oncol. 2010;11:121–128. doi: 10.1016/S1470-2045(09)70364-X. [DOI] [PubMed] [Google Scholar]
- 10.Maemondo M, Inoue A, Kobayashi K, et al. Gefitinib or chemotherapy for non-small-cell lung cancer with mutated EGFR. N Engl J Med. 2010;362:2380–2388. doi: 10.1056/NEJMoa0909530. [DOI] [PubMed] [Google Scholar]
- 11.Zhou C, Wu Y-L, Chen G, et al. Efficacy results from the randomized phase III OPTIMAL (CTONG 0802) study comparing first-line erlotinib versus carboplatin (CBDCA) plus gemcitabine (GEM) in Chinese advanced non-small cell lung cancer (NSCLC) patients (PTS) with EGFR activating mutations. Ann Oncol. 2010;21(Suppl. 8):viii1–viii12. [Google Scholar]
- 12.Scagliotti GV, Park K, Patil S, et al. Survival without toxicity for cisplatin plus pemetrexed versus cisplatin plus gemcitabine in chemonaive patients with advanced non-small cell lung cancer: a risk-benefit analysis of a large phase III study. Eur J Cancer. 2009;45:2298–2303. doi: 10.1016/j.ejca.2009.04.033. [DOI] [PubMed] [Google Scholar]
- 13.Scagliotti GV, Parikh P, von Pawel J, et al. Phase III study comparing cisplatin plus gemcitabine with cisplatin plus pemetrexed in chemotherapy-naive patients with advanced-stage non-small-cell lung cancer. J Clin Oncol. 2008;26:3543–3551. doi: 10.1200/JCO.2007.15.0375. [DOI] [PubMed] [Google Scholar]
- 14.Ciuleanu T, Brodowicz T, Zielinski C, et al. Maintenance pemetrexed plus best supportive care versus placebo plus best supportive care for non-small-cell lung cancer: a randomised, double-blind, phase 3 study. Lancet. 2009;374:1432–1440. doi: 10.1016/S0140-6736(09)61497-5. [DOI] [PubMed] [Google Scholar]
- 15.Scagliotti G, Hanna N, Fossella F, et al. The differential efficacy of pemetrexed according to NSCLC histology: a review of two phase III studies. Oncologist. 2009;14:253–263. doi: 10.1634/theoncologist.2008-0232. [DOI] [PubMed] [Google Scholar]
- 16.Johnson DH, Fehrenbacher L, Novotny WF, et al. Randomized phase II trial comparing bevacizumab plus carboplatin and paclitaxel with carboplatin and paclitaxel alone in previously untreated locally advanced or metastatic non-small-cell lung cancer. J Clin Oncol. 2004;22:2184–2191. doi: 10.1200/JCO.2004.11.022. [DOI] [PubMed] [Google Scholar]
- 17.Cohen MH, Gootenberg J, Keegan P, et al. FDA drug approval summary: bevacizumab (Avastin) plus Carboplatin and Paclitaxel as first-line treatment of advanced/metastatic recurrent nonsquamous non-small cell lung cancer. Oncologist. 2007;12:713–718. doi: 10.1634/theoncologist.12-6-713. [DOI] [PubMed] [Google Scholar]
- 18.Kodama K, Higashiyama M, Yokouchi H, et al. Prognostic value of ground-glass opacity found in small lung adenocarcinoma on high-resolution CT scanning. Lung Cancer. 2001;33:17–25. doi: 10.1016/s0169-5002(01)00185-4. [DOI] [PubMed] [Google Scholar]
- 19.Suzuki K, Asamura H, Kusumoto M, et al. “Early” peripheral lung cancer: prognostic significance of ground glass opacity on thin-section computed tomographic scan. Ann Thorac Surg. 2002;74:1635–1639. doi: 10.1016/s0003-4975(02)03895-x. [DOI] [PubMed] [Google Scholar]
- 20.Takamochi K, Nagai K, Yoshida J, et al. Pathologic N0 status in pulmonary adenocarcinoma is predictable by combining serum carcinoembryonic antigen level and computed tomographic findings. J Thorac Cardiovasc Surg. 2001;122:325–330. doi: 10.1067/mtc.2001.114355. [DOI] [PubMed] [Google Scholar]
- 21.Sakurai H, Maeshima A, Watanabe S, et al. Grade of stromal invasion in small adenocarcinoma of the lung: histopathological minimal invasion and prognosis. Am J Surg Pathol. 2004;28:198–206. doi: 10.1097/00000478-200402000-00007. [DOI] [PubMed] [Google Scholar]
- 22.Adler B, Padley S, Miller RR, et al. High-resolution CT of bronchioloalveolar carcinoma. AJR Am J Roentgenol. 1992;159:275–277. doi: 10.2214/ajr.159.2.1321558. [DOI] [PubMed] [Google Scholar]
- 23.Aoki T, Tomoda Y, Watanabe H, et al. Peripheral lung adenocarcinoma: correlation of thin-section CT findings with histologic prognostic factors and survival. Radiology. 2001;220:803–809. doi: 10.1148/radiol.2203001701. [DOI] [PubMed] [Google Scholar]
- 24.El-Sherif A, Gooding WE, Santos R, et al. Outcomes of sublobar resection versus lobectomy for stage I non-small cell lung cancer: a 13-year analysis. Ann Thorac Surg. 2006;82:408–415. doi: 10.1016/j.athoracsur.2006.02.029. [DOI] [PubMed] [Google Scholar]
- 25.Nakamura H, Kawasaki N, Taguchi M, et al. Survival following lobectomy vs limited resection for stage I lung cancer: a meta-analysis. Br J Cancer. 2005;92:1033–1037. doi: 10.1038/sj.bjc.6602414. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Okada M, Koike T, Higashiyama M, et al. Radical sublobar resection for small-sized non-small cell lung cancer: a multicenter study. J Thorac Cardiovasc Surg. 2006;132:769–775. doi: 10.1016/j.jtcvs.2006.02.063. [DOI] [PubMed] [Google Scholar]
- 27.Shah PL, Singh S, Bower M, et al. The role of transbronchial fine needle aspiration in an integrated care pathway for the assessment of patients with suspected lung cancer. J Thorac Oncol. 2006;1:324–327. [PubMed] [Google Scholar]
- 28.Edwards SL, Roberts C, McKean ME, et al. Preoperative histological classification of primary lung cancer: accuracy of diagnosis and use of the non-small cell category. J Clin Pathol. 2000;53:537–540. doi: 10.1136/jcp.53.7.537. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Cataluna JJ, Perpina M, Greses JV, et al. Cell type accuracy of bronchial biopsy specimens in primary lung cancer. Chest. 1996;109:1199–1203. doi: 10.1378/chest.109.5.1199. [DOI] [PubMed] [Google Scholar]
- 30.Travis WD, Rekhtman N, Riley GJ, et al. Pathologic diagnosis of advanced lung cancer based on small biopsies and cytology: a paradigm shift. J Thorac Oncol. 2010;5:411–414. doi: 10.1097/JTO.0b013e3181d57f6e. [DOI] [PubMed] [Google Scholar]
- 31.Survey Monkey. 2010 Available at: www.surveymonkey.com. [Google Scholar]
- 32.Schunemann HJ, Jaeschke R, Cook DJ, et al. An official ATS statement: grading the quality of evidence and strength of recommendations in ATS guidelines and recommendations. Am J Respir Crit Care Med. 2006;174:605–614. doi: 10.1164/rccm.200602-197ST. [DOI] [PubMed] [Google Scholar]
- 33.Schunemann HJ, Oxman AD, Brozek J, et al. GRADE: assessing the quality of evidence for diagnostic recommendations. ACP J Club. 2008;149:2–3. [PubMed] [Google Scholar]
- 34.Schunemann HJ, Oxman AD, Brozek J, et al. Grading quality of evidence and strength of recommendations for diagnostic tests and strategies. BMJ. 2008;336:1106–1110. doi: 10.1136/bmj.39500.677199.AE. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Guyatt GH, Oxman AD, Kunz R, et al. Going from evidence to recommendations. BMJ. 2008;336:1049–1051. doi: 10.1136/bmj.39493.646875.AE. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Guyatt GH, Oxman AD, Kunz R, et al. What is “quality of evidence” and why is it important to clinicians? BMJ. 2008;336:995–998. doi: 10.1136/bmj.39490.551019.BE. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Guyatt GH, Oxman AD, Vist GE, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336:924–926. doi: 10.1136/bmj.39489.470347.AD. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Guyatt G, Oxman AD, Kunz R, et al. GRADE guidelines: 1. Introduction—GRADE evidence profiles and summary of findings tables. J Clin Epidemiol. 2010 Dec 30; doi: 10.1016/j.jclinepi.2010.04.026. (Epub ahead of print). [DOI] [PubMed] [Google Scholar]
- 39.Loo PS, Thomas SC, Nicolson MC, et al. Subtyping of undifferentiated non-small cell carcinomas in bronchial biopsy specimens. J Thorac Oncol. 2010;5:442–447. doi: 10.1097/JTO.0b013e3181d40fac. [DOI] [PubMed] [Google Scholar]
- 40.Nicholson AG, Gonzalez D, Shah P, et al. Refining the diagnosis and EGFR status of non-small cell lung carcinoma in biopsy and cytologic material, using a panel of mucin staining, TTF-1, cytokeratin 5/6, and P63, and EGFR mutation analysis. J Thorac Oncol. 2010;5:436–441. doi: 10.1097/JTO.0b013e3181c6ed9b. [DOI] [PubMed] [Google Scholar]
- 41.Barletta JA, Perner S, Iafrate AJ, et al. Clinical significance of TTF-1 protein expression and TTF-1 gene amplification in lung adenocarcinoma. J Cell Mol Med. 2009;13:1977–1986. doi: 10.1111/j.1582-4934.2008.00594.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Deshpande CG, Geisinger K, Petersen I, et al. Grading of lung adenocarcinoma: architectural versus nuclear approach. Mod Pathol. 2009;22(Suppl 1):1596. [Google Scholar]
- 43.Sica G, Yoshizawa A, Sima CS, et al. A grading system of lung adenocarcinomas based on histologic pattern is predictive of disease recurrence in stage I tumors. Am J Surg Pathol. 2010;34:1155–1162. doi: 10.1097/PAS.0b013e3181e4ee32. [DOI] [PubMed] [Google Scholar]
- 44.Yoshizawa A, Motoi N, Riely GJ, et al. Prognostic significance of the proposed IASLC/ATS/ERS revised classification of lung adenocarcinoma in 514 stage I lung adenocarcinomas. Mod Pathol. 2011:24. doi: 10.1038/modpathol.2010.232. In press. [DOI] [PubMed] [Google Scholar]
- 45.Thunnissen FB, Beasley MB, Borczuk A, et al. Reproducibility of histopathological subtypes in pulmonary adenocarcinoma. Mod Pathol. 2010;23:415A. doi: 10.1038/modpathol.2012.106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Noguchi M, Morikawa A, Kawasaki M, et al. Small adenocarcinoma of the lung. Histologic characteristics and prognosis. Cancer. 1995;75:2844–2852. doi: 10.1002/1097-0142(19950615)75:12<2844::aid-cncr2820751209>3.0.co;2-#. [DOI] [PubMed] [Google Scholar]
- 47.Borczuk AC, Qian F, Kazeros A, et al. Invasive size is an independent predictor of survival in pulmonary adenocarcinoma. Am J Surg Pathol. 2009;33:462–469. doi: 10.1097/PAS.0b013e318190157c. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Yim J, Zhu LC, Chiriboga L, et al. Histologic features are important prognostic indicators in early stages lung adenocarcinomas. Mod Pathol. 2007;20:233–241. doi: 10.1038/modpathol.3800734. [DOI] [PubMed] [Google Scholar]
- 49.Goldstein NS, Mani A, Chmielewski G, et al. Prognostic factors in T1 NO MO adenocarcinomas and bronchioloalveolar carcinomas of the lung. Am J Clin Pathol. 1999;112:391–402. doi: 10.1093/ajcp/112.3.391. [DOI] [PubMed] [Google Scholar]
- 50.Clayton F. Bronchioloalveolar carcinomas. Cell types, patterns of growth, and prognostic correlates. Cancer. 1986;57:1555–1564. doi: 10.1002/1097-0142(19860415)57:8<1555::aid-cncr2820570820>3.0.co;2-n. [DOI] [PubMed] [Google Scholar]
- 51.Daly RC, Trastek VF, Pairolero PC, et al. Bronchoalveolar carcinoma: factors affecting survival. Ann Thorac Surg. 1991;51:368–376. doi: 10.1016/0003-4975(91)90847-j. discussion 76–77. [DOI] [PubMed] [Google Scholar]
- 52.Manning JT, Jr, Spjut HJ, Tschen JA. Bronchioloalveolar carcinoma: the significance of two histopathologic types. Cancer. 1984;54:525–534. doi: 10.1002/1097-0142(19840801)54:3<525::aid-cncr2820540324>3.0.co;2-x. [DOI] [PubMed] [Google Scholar]
- 53.Riquet M, Foucault C, Berna P, et al. Prognostic value of histology in resected lung cancer with emphasis on the relevance of the adenocarcinoma subtyping. Ann Thorac Surg. 2006;81:1988–1995. doi: 10.1016/j.athoracsur.2006.01.021. [DOI] [PubMed] [Google Scholar]
- 54.Goldstein NS, Thomas M. Mucinous and nonmucinous bronchioloalveolar adenocarcinomas have distinct staining patterns with thyroid transcription factor and cytokeratin 20 antibodies. Am J Clin Pathol. 2001;116:319–325. doi: 10.1309/550P-QLJX-D84W-F6DN. [DOI] [PubMed] [Google Scholar]
- 55.Garfield DH, Cadranel J, West HL. Bronchioloalveolar carcinoma: the case for two diseases. Clin Lung Cancer. 2008;9:24–29. doi: 10.3816/CLC.2008.n.004. [DOI] [PubMed] [Google Scholar]
- 56.Garfield DH, Cadranel J. The importance of distinguishing mucinous and nonmucinous bronchioloalveolar carcinomas. Lung. 2009;187:207–208. doi: 10.1007/s00408-009-9149-3. [DOI] [PubMed] [Google Scholar]
- 57.Garfield DH, Franklin WA. A comparison of survival and disease-specific survival in surgically resected, lymph node-positive bronchioloalveolar carcinoma versus nonsmall cell lung cancer: implications for adjuvant therapy. Cancer. 2008;113:1107–1108. doi: 10.1002/cncr.23662. [DOI] [PubMed] [Google Scholar]
- 58.Travis WD, Garg K, Franklin WA, et al. Evolving concepts in the pathology and computed tomography imaging of lung adenocarcinoma and bronchioloalveolar carcinoma. J Clin Oncol. 2005;23:3279–3287. doi: 10.1200/JCO.2005.15.776. [DOI] [PubMed] [Google Scholar]
- 59.West HL, Garfield DH. Bronchioloalveolar carcinoma: not as easy as “BAC”. J Thorac Oncol. 2009;4:1047–1048. doi: 10.1097/JTO.0b013e3181b6ebda. [DOI] [PubMed] [Google Scholar]
- 60.Raz DJ, He B, Rosell R, et al. Bronchioloalveolar carcinoma: a review. Clin Lung Cancer. 2006;7:313–322. doi: 10.3816/CLC.2006.n.012. [DOI] [PubMed] [Google Scholar]
- 61.Gandara DR. Bronchioloalveolar carcinoma: the “changing face of lung cancer”. Clin Lung Cancer. 2006;7:299. [PubMed] [Google Scholar]
- 62.Watanabe S, Watanabe T, Arai K, et al. Results of wedge resection for focal bronchioloalveolar carcinoma showing pure ground-glass attenuation on computed tomography. Ann Thorac Surg. 2002;73:1071–1075. doi: 10.1016/s0003-4975(01)03623-2. [DOI] [PubMed] [Google Scholar]
- 63.Sakurai H, Dobashi Y, Mizutani E, et al. Bronchioloalveolar carcinoma of the lung 3 centimeters or less in diameter: a prognostic assessment. Ann Thorac Surg. 2004;78:1728–1733. doi: 10.1016/j.athoracsur.2004.05.017. [DOI] [PubMed] [Google Scholar]
- 64.Vazquez M, Carter D, Brambilla E, et al. Solitary and multiple resected adenocarcinomas after CT screening for lung cancer: histopathologic features and their prognostic implications. Lung Cancer. 2009;64:148–154. doi: 10.1016/j.lungcan.2008.08.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Yamato Y, Tsuchida M, Watanabe T, et al. Early results of a prospective study of limited resection for bronchioloalveolar adenocarcinoma of the lung. Ann Thorac Surg. 2001;71:971–974. doi: 10.1016/s0003-4975(00)02507-8. [DOI] [PubMed] [Google Scholar]
- 66.Yamada S, Kohno T. Video-assisted thoracic surgery for pure ground-glass opacities 2 cm or less in diameter. Ann Thorac Surg. 2004;77:1911–1915. doi: 10.1016/j.athoracsur.2003.12.040. [DOI] [PubMed] [Google Scholar]
- 67.Yoshida J, Nagai K, Yokose T, et al. Limited resection trial for pulmonary ground-glass opacity nodules: fifty-case experience. J Thorac Cardiovasc Surg. 2005;129:991–996. doi: 10.1016/j.jtcvs.2004.07.038. [DOI] [PubMed] [Google Scholar]
- 68.Koike T, Togashi K, Shirato T, et al. Limited resection for noninvasive bronchioloalveolar carcinoma diagnosed by intraoperative pathologic examination. Ann Thorac Surg. 2009;88:1106–1111. doi: 10.1016/j.athoracsur.2009.06.051. [DOI] [PubMed] [Google Scholar]
- 69.Motoi N, Szoke J, Riely GJ, et al. Lung adenocarcinoma: modification of the 2004 WHO mixed subtype to include the major histologic subtype suggests correlations between papillary and micropapillary adenocarcinoma subtypes EGFR mutations and gene expression analysis. Am J Surg Pathol. 2008;32:810–827. doi: 10.1097/PAS.0b013e31815cb162. [DOI] [PubMed] [Google Scholar]
- 70.Carey FA, Wallace WA, Fergusson RJ, et al. Alveolar atypical hyperplasia in association with primary pulmonary adenocarcinoma: a clinicopathological study of 10 cases. Thorax. 1992;47:1041–1043. doi: 10.1136/thx.47.12.1041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Weng S, Tsuchiya E, Satoh Y, et al. Multiple atypical adenomatous hyperplasia of type II pneumonocytes and bronchio-alveolar carcinoma. Histopathology. 1990;16:101–103. doi: 10.1111/j.1365-2559.1990.tb01073.x. [DOI] [PubMed] [Google Scholar]
- 72.Nakanishi K. Alveolar epithelial hyperplasia and adenocarcinoma of the lung. Arch Pathol Lab Med. 1990;114:363–368. [PubMed] [Google Scholar]
- 73.Nakahara R, Yokose T, Nagai K, et al. Atypical adenomatous hyperplasia of the lung: a clinicopathological study of 118 cases including cases with multiple atypical adenomatous hyperplasia. Thorax. 2001;56:302–305. doi: 10.1136/thorax.56.4.302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Miller RR. Bronchioloalveolar cell adenomas. Am J Surg Pathol. 1990;14:904–912. doi: 10.1097/00000478-199010000-00002. [DOI] [PubMed] [Google Scholar]
- 75.Nakayama H, Noguchi M, Tsuchiya R, et al. Clonal growth of atypical adenomatous hyperplasia of the lung: cytofluorometric analysis of nuclear DNA content. Mod Pathol. 1990;3:314–320. [PubMed] [Google Scholar]
- 76.Niho S, Yokose T, Suzuki K, et al. Monoclonality of atypical adenomatous hyperplasia of the lung. Am J Pathol. 1999;154:249–254. doi: 10.1016/S0002-9440(10)65271-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Sakamoto H, Shimizu J, Horio Y, et al. Disproportionate representation of KRAS gene mutation in atypical adenomatous hyperplasia, but even distribution of EGFR gene mutation from preinvasive to invasive adenocarcinomas. J Pathol. 2007;212:287–294. doi: 10.1002/path.2165. [DOI] [PubMed] [Google Scholar]
- 78.Westra WH, Baas IO, Hruban RH, et al. K-ras oncogene activation in atypical alveolar hyperplasias of the human lung. Cancer Res. 1996;56:2224–2228. [PubMed] [Google Scholar]
- 79.Kohno T, Kunitoh H, Suzuki K, et al. Association of KRAS polymorphisms with risk for lung adenocarcinoma accompanied by atypical adenomatous hyperplasias. Carcinogenesis. 2008;29:957–963. doi: 10.1093/carcin/bgn048. [DOI] [PubMed] [Google Scholar]
- 80.Yoshida Y, Shibata T, Kokubu A, et al. Mutations of the epidermal growth factor receptor gene in atypical adenomatous hyperplasia and bronchioloalveolar carcinoma of the lung. Lung Cancer. 2005;50:1–8. doi: 10.1016/j.lungcan.2005.04.012. [DOI] [PubMed] [Google Scholar]
- 81.Kitamura H, Kameda Y, Nakamura N, et al. Atypical adenomatous hyperplasia and bronchoalveolar lung carcinoma. Analysis by morphometry and the expressions of p53 and carcinoembryonic antigen. Am J Surg Pathol. 1996;20:553–562. doi: 10.1097/00000478-199605000-00002. [DOI] [PubMed] [Google Scholar]
- 82.Takamochi K, Ogura T, Suzuki K, et al. Loss of heterozygosity on chromosomes 9q and 16p in atypical adenomatous hyperplasia concomitant with adenocarcinoma of the lung. Am J Pathol. 2001;159:1941–1948. doi: 10.1016/S0002-9440(10)63041-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Licchesi JD, Westra WH, Hooker CM, et al. Promoter hypermethylation of hallmark cancer genes in atypical adenomatous hyperplasia of the lung. Clin Cancer Res. 2008;14:2570–2578. doi: 10.1158/1078-0432.CCR-07-2033. [DOI] [PubMed] [Google Scholar]
- 84.Nakanishi K, Kawai T, Kumaki F, et al. Expression of human telomerase RNA component and telomerase reverse transcriptase mRNA in atypical adenomatous hyperplasia of the lung. Hum Pathol. 2002;33:697–702. doi: 10.1053/hupa.2002.125775. [DOI] [PubMed] [Google Scholar]
- 85.Seki N, Takasu T, Mandai K, et al. Expression of eukaryotic initiation factor 4E in atypical adenomatous hyperplasia and adenocarcinoma of the human peripheral lung. Clin Cancer Res. 2002;8:3046–3053. [PubMed] [Google Scholar]
- 86.Licchesi JD, Westra WH, Hooker CM, et al. Epigenetic alteration of Wnt pathway antagonists in progressive glandular neoplasia of the lung. Carcinogenesis. 2008;29:895–904. doi: 10.1093/carcin/bgn017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Kerr KM, MacKenzie SJ, Ramasami S, et al. Expression of Fhit, cell adhesion molecules and matrix metalloproteinases in atypical adenomatous hyperplasia and pulmonary adenocarcinoma. J Pathol. 2004;203:638–644. doi: 10.1002/path.1557. [DOI] [PubMed] [Google Scholar]
- 88.Maeshima AM, Tochigi N, Yoshida A, et al. Clinicopathologic analysis of multiple (five or more) atypical adenomatous hyperplasias (AAHs) of the lung: evidence for the AAH-adenocarcinoma sequence. J Thorac Oncol. 2010;5:466–471. doi: 10.1097/JTO.0b013e3181ce3b73. [DOI] [PubMed] [Google Scholar]
- 89.Mori M, Rao SK, Popper HH, et al. Atypical adenomatous hyperplasia of the lung: a probable forerunner in the development of adenocarcinoma of the lung. Mod Pathol. 2001;14:72–84. doi: 10.1038/modpathol.3880259. [DOI] [PubMed] [Google Scholar]
- 90.Kitamura H, Kameda Y, Ito T, et al. Atypical adenomatous hyperplasia of the lung. Implications for the pathogenesis of peripheral lung adenocarcinoma. Am J Clin Pathol. 1999;111:610–622. doi: 10.1093/ajcp/111.5.610. [DOI] [PubMed] [Google Scholar]
- 91.Koga T, Hashimoto S, Sugio K, et al. Lung adenocarcinoma with bronchioloalveolar carcinoma component is frequently associated with foci of high-grade atypical adenomatous hyperplasia. Am J Clin Pathol. 2002;117:464–470. doi: 10.1309/CHXA-3MH0-B7FD-JGUL. [DOI] [PubMed] [Google Scholar]
- 92.Maeshima AM, Tochigi N, Yoshida A, et al. Histological scoring for small lung adenocarcinomas 2 cm or less in diameter: a reliable prognostic indicator. J Thorac Oncol. 2010;5:333–339. doi: 10.1097/JTO.0b013e3181c8cb95. [DOI] [PubMed] [Google Scholar]
- 93.Sawada E, Nambu A, Motosugi U, et al. Localized mucinous bronchioloalveolar carcinoma of the lung: thin-section computed tomography and fluorodeoxyglucose positron emission tomography findings. Jpn J Radiol. 2010;28:251–258. doi: 10.1007/s11604-009-0414-4. [DOI] [PubMed] [Google Scholar]
- 94.Oka S, Hanagiri T, Uramoto H, et al. Surgical resection for patients with mucinous bronchioloalveolar carcinoma. Asian J Surg. 2010;33:89–93. doi: 10.1016/S1015-9584(10)60015-2. [DOI] [PubMed] [Google Scholar]
- 95.De Oliveira Duarte Achcar R, Nikiforova MN, Yousem SA. Micropapillary lung adenocarcinoma: EGFR, K-ras and BRAF mutational profile. Am J Clin Pathol. 2009;131:694–700. doi: 10.1309/AJCPBS85VJEOBPDO. [DOI] [PubMed] [Google Scholar]
- 96.Nakamura Y, Niki T, Goto A, et al. c-Met activation in lung adenocarcinoma tissues: an immunohistochemical analysis. Cancer Sci. 2007;98:1006–1013. doi: 10.1111/j.1349-7006.2007.00493.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Kim YH, Ishii G, Goto K, et al. Dominant papillary subtype is a significant predictor of the response to gefitinib in adenocarcinoma of the lung. Clin Cancer Res. 2004;10:7311–7317. doi: 10.1158/1078-0432.CCR-04-0811. [DOI] [PubMed] [Google Scholar]
- 98.Ding L, Getz G, Wheeler DA, et al. Somatic mutations affect key pathways in lung adenocarcinoma. Nature. 2008;455:1069–1075. doi: 10.1038/nature07423. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99.Shedden K, Taylor JM, Enkemann SA, et al. Gene expression-based survival prediction in lung adenocarcinoma: a multi-site, blinded validation study. Nat Med. 2008;14:822–827. doi: 10.1038/nm.1790. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100.Sholl LM, Yeap BY, Iafrate AJ, et al. Lung adenocarcinoma with EGFR amplification has distinct clinicopathologic and molecular features in never-smokers. Cancer Res. 2009;69:8341–8348. doi: 10.1158/0008-5472.CAN-09-2477. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101.Dacic S, Shuai Y, Yousem S, et al. Clinicopathological predictors of EGFR/KRAS mutational status in primary lung adenocarcinomas. Mod Pathol. 2010;23:159–168. doi: 10.1038/modpathol.2009.154. [DOI] [PubMed] [Google Scholar]
- 102.Girard N, Deshpande C, Lau C, et al. Comprehensive histologic assessment helps to differentiate multiple lung primary nonsmall cell carcinomas from metastases. Am J Surg Pathol. 2009;33:1752–1764. doi: 10.1097/PAS.0b013e3181b8cf03. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103.Lee HY, Han J, Lee KS, et al. Lung adenocarcinoma as a solitary pulmonary nodule: prognostic determinants of CT, PET, and histopathologic findings. Lung Cancer. 2009;66:379–385. doi: 10.1016/j.lungcan.2009.02.011. [DOI] [PubMed] [Google Scholar]
- 104.Yokose T, Suzuki K, Nagai K, et al. Favorable and unfavorable morphological prognostic factors in peripheral adenocarcinoma of the lung 3 cm or less in diameter. Lung Cancer. 2000;29:179–188. doi: 10.1016/s0169-5002(00)00103-3. [DOI] [PubMed] [Google Scholar]
- 105.Lin DM, Ma Y, Zheng S, et al. Prognostic value of bronchioloalveolar carcinoma component in lung adenocarcinoma. Histol Histopathol. 2006;21:627–632. doi: 10.14670/HH-21.627. [DOI] [PubMed] [Google Scholar]
- 106.Okudela K, Woo T, Mitsui H, et al. Proposal of an improved histological sub-typing system for lung adenocarcinoma—significant prognostic values for stage I disease. Int J Clin Exp Pathol. 2010;3:348–366. [PMC free article] [PubMed] [Google Scholar]
- 107.Silver SA, Askin FB. True papillary carcinoma of the lung: a distinct clinicopathologic entity. Am J Surg Pathol. 1997;21:43–51. doi: 10.1097/00000478-199701000-00005. [DOI] [PubMed] [Google Scholar]
- 108.Amin MB, Tamboli P, Merchant SH, et al. Micropapillary component in lung adenocarcinoma: a distinctive histologic feature with possible prognostic significance. Am J Surg Pathol. 2002;26:358–364. doi: 10.1097/00000478-200203000-00010. [DOI] [PubMed] [Google Scholar]
- 109.Miyoshi T, Satoh Y, Okumura S, et al. Early-stage lung adenocarcinomas with a micropapillary pattern, a distinct pathologic marker for a significantly poor prognosis. Am J Surg Pathol. 2003;27:101–109. doi: 10.1097/00000478-200301000-00011. [DOI] [PubMed] [Google Scholar]
- 110.Kamiya K, Hayashi Y, Douguchi J, et al. Histopathological features and prognostic significance of the micropapillary pattern in lung adenocarcinoma. Mod Pathol. 2008;21:992–1001. doi: 10.1038/modpathol.2008.79. [DOI] [PubMed] [Google Scholar]
- 111.Kawakami T, Nabeshima K, Makimoto Y, et al. Micropapillary pattern and grade of stromal invasion in pT1 adenocarcinoma of the lung: usefulness as prognostic factors. Mod Pathol. 2007;20:514–521. doi: 10.1038/modpathol.3800765. [DOI] [PubMed] [Google Scholar]
- 112.Kuroda N, Hamaguchi N, Takeuchi E, et al. Lung adenocarcinoma with a micropapillary pattern: a clinicopathological study of 25 cases. APMIS. 2006;114:381–385. doi: 10.1111/j.1600-0463.2006.apm_340.x. [DOI] [PubMed] [Google Scholar]
- 113.Kuroda N, Hamauzu T, Toi M, et al. Pulmonary adenocarcinoma with micropapillary component: an immunohistochemical study. Case report. APMIS. 2005;113:550–554. doi: 10.1111/j.1600-0463.2005.apm_151.x. [DOI] [PubMed] [Google Scholar]
- 114.Maeda R, Isowa N, Onuma H, et al. Lung adenocarcinomas with micropapillary components. Gen Thorac Cardiovasc Surg. 2009;57:534–539. doi: 10.1007/s11748-009-0436-y. [DOI] [PubMed] [Google Scholar]
- 115.Makimoto Y, Nabeshima K, Iwasaki H, et al. Micropapillary pattern: a distinct pathological marker to subclassify tumours with a significantly poor prognosis within small peripheral lung adenocarcinoma (</=20 mm) with mixed bronchioloalveolar and invasive subtypes (Noguchi’s type C tumours) Histopathology. 2005;46:677–684. doi: 10.1111/j.1365-2559.2005.02126.x. [DOI] [PubMed] [Google Scholar]
- 116.Miyoshi T, Shirakusa T, Ishikawa Y, et al. Possible mechanism of metastasis in lung adenocarcinomas with a micropapillary pattern. Pathol Int. 2005;55:419–424. doi: 10.1111/j.1440-1827.2005.01847.x. [DOI] [PubMed] [Google Scholar]
- 117.Roh MS, Lee JI, Choi PJ, et al. Relationship between micropapillary component and micrometastasis in the regional lymph nodes of patients with stage I lung adenocarcinoma. Histopathology. 2004;45:580–586. doi: 10.1111/j.1365-2559.2004.01953.x. [DOI] [PubMed] [Google Scholar]
- 118.Sanchez-Mora N, Presmanes MC, Monroy V, et al. Micropapillary lung adenocarcinoma: a distinctive histologic subtype with prognostic significance. Case series. Hum Pathol. 2008;39:324–330. doi: 10.1016/j.humpath.2007.05.029. [DOI] [PubMed] [Google Scholar]
- 119.Tsutsumida H, Nomoto M, Goto M, et al. A micropapillary pattern is predictive of a poor prognosis in lung adenocarcinoma, and reduced surfactant apoprotein A expression in the micropapillary pattern is an excellent indicator of a poor prognosis. Mod Pathol. 2007;20:638–647. doi: 10.1038/modpathol.3800780. [DOI] [PubMed] [Google Scholar]
- 120.Wislez M, Antoine M, Baudrin L, et al. Non-mucinous and mucinous subtypes of adenocarcinoma with bronchioloalveolar carcinoma features differ by biomarker expression and in the response to gefitinib. Lung Cancer. 2010;68:185–191. doi: 10.1016/j.lungcan.2009.05.021. [DOI] [PubMed] [Google Scholar]
- 121.Hata A, Katakami N, Fujita S, et al. Frequency of EGFR and KRAS mutations in Japanese patients with lung adenocarcinoma with features of the mucinous subtype of bronchioloalveolar carcinoma. J Thorac Oncol. 2010;5:1197–1200. doi: 10.1097/JTO.0b013e3181e2a2bc. [DOI] [PubMed] [Google Scholar]
- 122.Yatabe Y, Mitsudomi T. Epidermal growth factor receptor mutations in lung cancers. Pathol Int. 2007;57:233–244. doi: 10.1111/j.1440-1827.2007.02098.x. [DOI] [PubMed] [Google Scholar]
- 123.Holst VA, Finkelstein S, Yousem SA. Bronchioloalveolar adenocarcinoma of lung: monoclonal origin for multifocal disease. Am J Surg Pathol. 1998;22:1343–1350. doi: 10.1097/00000478-199811000-00004. [DOI] [PubMed] [Google Scholar]
- 124.Furak J, Trojan I, Szoke T, et al. Bronchioloalveolar lung cancer: occurrence, surgical treatment and survival. Eur J Cardiothorac Surg. 2003;23:818–823. doi: 10.1016/s1010-7940(03)00084-8. [DOI] [PubMed] [Google Scholar]
- 125.Lee HY, Lee KS, Han J, et al. Mucinous versus nonmucinous solitary pulmonary nodular bronchioloalveolar carcinoma: CT and FDG PET findings and pathologic comparisons. Lung Cancer. 2009;65:170–175. doi: 10.1016/j.lungcan.2008.11.009. [DOI] [PubMed] [Google Scholar]
- 126.Miyake H, Matsumoto A, Terada A, et al. Mucin-producing tumor of the lung: CT findings. J Thorac Imaging. 1995;10:96–98. doi: 10.1097/00005382-199521000-00003. [DOI] [PubMed] [Google Scholar]
- 127.Casali C, Rossi G, Marchioni A, et al. A single institution-based retrospective study of surgically treated bronchioloalveolar adenocarcinoma of the lung: clinicopathologic analysis, molecular features, and possible pitfalls in routine practice. J Thorac Oncol. 2010;5:830–836. doi: 10.1097/jto.0b013e3181d60ff5. [DOI] [PubMed] [Google Scholar]
- 128.Akira M, Atagi S, Kawahara M, et al. High-resolution CT findings of diffuse bronchioloalveolar carcinoma in 38 patients. AJR Am J Roentgenol. 1999;173:1623–1629. doi: 10.2214/ajr.173.6.10584811. [DOI] [PubMed] [Google Scholar]
- 129.Kodama K, Higashiyama M, Yokouchi H, et al. Natural history of pure ground-glass opacity after long-term follow-up of more than 2 years. Ann Thorac Surg. 2002;73:386–392. doi: 10.1016/s0003-4975(01)03410-5. [DOI] [PubMed] [Google Scholar]
- 130.Nagao M, Murase K, Yasuhara Y, et al. Measurement of localized ground-glass attenuation on thin-section computed tomography images: correlation with the progression of bronchioloalveolar carcinoma of the lung. Invest Radiol. 2002;37:692–697. doi: 10.1097/00004424-200212000-00009. [DOI] [PubMed] [Google Scholar]
- 131.Saito H, Yamada K, Hamanaka N, et al. Initial findings and progression of lung adenocarcinoma on serial computed tomography scans. J Comput Assist Tomogr. 2009;33:42–48. doi: 10.1097/RCT.0b013e3181633509. [DOI] [PubMed] [Google Scholar]
- 132.Yabuuchi H, Murayama S, Murakami J, et al. High-resolution CT characteristics of poorly differentiated adenocarcinoma of the peripheral lung: comparison with well differentiated adenocarcinoma. Radiat Med. 2000;18:343–347. [PubMed] [Google Scholar]
- 133.Im JG, Han MC, Yu EJ, et al. Lobar bronchioloalveolar carcinoma: ‘Angiogram sign’ on CT scans. Radiology. 1990;176:749–753. doi: 10.1148/radiology.176.3.2167502. [DOI] [PubMed] [Google Scholar]
- 134.Tateishi U, Muller NL, Johkoh T, et al. Mucin-producing adenocarcinoma of the lung: thin-section computed tomography findings in 48 patients and their effect on prognosis. J Comput Assist Tomogr. 2005;29:361–368. doi: 10.1097/01.rct.0000162820.08909.e1. [DOI] [PubMed] [Google Scholar]
- 135.Clayton F. The spectrum and significance of bronchioloalveolar carcinomas. Pathol Annu. 1988;23:361–394. [PubMed] [Google Scholar]
- 136.Shah RN, Badve S, Papreddy K, et al. Expression of cytokeratin 20 in mucinous bronchioloalveolar carcinoma. Hum Pathol. 2002;33:915–920. doi: 10.1053/hupa.2002.126876. [DOI] [PubMed] [Google Scholar]
- 137.Lau SK, Desrochers MJ, Luthringer DJ. Expression of thyroid transcription factor-1, cytokeratin 7, and cytokeratin 20 in bronchioloalveolar carcinomas: an immunohistochemical evaluation of 67 cases. Mod Pathol. 2002;15:538–542. doi: 10.1038/modpathol.3880560. [DOI] [PubMed] [Google Scholar]
- 138.Sarantopoulos GP, Gui D, Shintaku P, et al. Immunohistochemical analysis of lung carcinomas with pure or partial bronchioloalveolar differentiation. Arch Pathol Lab Med. 2004;128:406–414. doi: 10.5858/2004-128-406-IAOLCW. [DOI] [PubMed] [Google Scholar]
- 139.Simsir A, Wei XJ, Yee H, et al. Differential expression of cytokeratins 7 and 20 and thyroid transcription factor-1 in bronchioloalveolar carcinoma: an immunohistochemical study in fine-needle aspiration biopsy specimens. Am J Clin Pathol. 2004;121:350–357. doi: 10.1309/CM20-WA20-RW3T-600L. [DOI] [PubMed] [Google Scholar]
- 140.Finberg KE, Sequist LV, Joshi VA, et al. Mucinous differentiation correlates with absence of EGFR mutation and presence of KRAS mutation in lung adenocarcinomas with bronchioloalveolar features. J Mol Diagn. 2007;9:320–326. doi: 10.2353/jmoldx.2007.060182. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 141.Sakuma Y, Matsukuma S, Yoshihara M, et al. Distinctive evaluation of nonmucinous and mucinous subtypes of bronchioloalveolar carcinomas in EGFR and K-ras gene-mutation analyses for Japanese lung adenocarcinomas: confirmation of the correlations with histologic subtypes and gene mutations. Am J Clin Pathol. 2007;128:100–108. doi: 10.1309/WVXFGAFLAUX48DU6. [DOI] [PubMed] [Google Scholar]
- 142.Marchetti A, Buttitta F, Pellegrini S, et al. Bronchioloalveolar lung carcinomas: K-ras mutations are constant events in the mucinous subtype. J Pathol. 1996;179:254–259. doi: 10.1002/(SICI)1096-9896(199607)179:3<254::AID-PATH589>3.0.CO;2-J. [DOI] [PubMed] [Google Scholar]
- 143.Maeshima A, Sakamoto M, Hirohashi S. Mixed mucinous-type and non-mucinous-type adenocarcinoma of the lung: immunohistochemical examination and K-ras gene mutation. Virchows Arch. 2002;440:598–603. doi: 10.1007/s00428-002-0629-6. [DOI] [PubMed] [Google Scholar]
- 144.Tam IY, Chung LP, Suen WS, et al. Distinct epidermal growth factor receptor and KRAS mutation patterns in non-small cell lung cancer patients with different tobacco exposure and clinicopathologic features. Clin Cancer Res. 2006;12:1647–1653. doi: 10.1158/1078-0432.CCR-05-1981. [DOI] [PubMed] [Google Scholar]
- 145.Copin MC, Buisine MP, Leteurtre E, et al. Mucinous bronchioloalveolar carcinomas display a specific pattern of mucin gene expression among primary lung adenocarcinomas. HumPathol. 2001;32:274–281. doi: 10.1053/hupa.2001.22752. [DOI] [PubMed] [Google Scholar]
- 146.Awaya H, Takeshima Y, Yamasaki M, et al. Expression of MUC1, MUC2, MUC5AC, and MUC6 in atypical adenomatous hyperplasia, bronchioloalveolar carcinoma, adenocarcinoma with mixed subtypes, and mucinous bronchioloalveolar carcinoma of the lung. Am J Clin Pathol. 2004;121:644–653. doi: 10.1309/U4WG-E9EB-FJN6-CM8R. [DOI] [PubMed] [Google Scholar]
- 147.Sato K, Ueda Y, Shikata H, et al. Bronchioloalveolar carcinoma of mixed mucinous and nonmucinous type: immunohistochemical studies and mutation analysis of the p53 gene. Pathol Res Pract. 2006;202:751–756. doi: 10.1016/j.prp.2006.07.002. [DOI] [PubMed] [Google Scholar]
- 148.Tsuta K, Ishii G, Nitadori J, et al. Comparison of the immunophenotypes of signet-ring cell carcinoma, solid adenocarcinoma with mucin production, and mucinous bronchioloalveolar carcinoma of the lung characterized by the presence of cytoplasmic mucin. J Pathol. 2006;209:78–87. doi: 10.1002/path.1947. [DOI] [PubMed] [Google Scholar]
- 149.Sica GL, Yoshizawa AK, Downey RJ, et al. Reassessment of the histologic spectrum of mucinous bronchioloalveolar carcinoma (mBAC) Mod Pathol. 2008;21:351A. [Google Scholar]
- 150.Gaeta M, Blandino A, Scribano E, et al. Mucinous cystadenocarcinoma of the lung: CT-pathologic correlation in three cases. J Comput Assist Tomogr. 1999;23:641–643. doi: 10.1097/00004728-199907000-00028. [DOI] [PubMed] [Google Scholar]
- 151.Deshpande CG, Yoshizawa A, Motoi N, et al. Clear cell change in lung adenocarcinoma: a cytologic change rather than a histologic variant. Mod Pathol. 2009;22(Suppl 1):1595. [Google Scholar]
- 152.Cohen PR, Yoshizawa A, Motoi N, et al. Signet ring cell features (SRCF) in lung adenocarcinoma: a cytologic feature or a histologic subtype? Mod Pathol. 2010;23:404A. [Google Scholar]
- 153.Rodig SJ, Mino-Kenudson M, Dacic S, et al. Unique clinicopathologic features characterize ALK-rearranged lung adenocarcinoma in the western population. Clin Cancer Res. 2009;15:5216–5223. doi: 10.1158/1078-0432.CCR-09-0802. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 154.Inamura K, Satoh Y, Okumura S, et al. Pulmonary adenocarcinomas with enteric differentiation: histologic and immunohistochemical characteristics compared with metastatic colorectal cancers and usual pulmonary adenocarcinomas. Am J Surg Pathol. 2005;29:660–665. doi: 10.1097/01.pas.0000160438.00652.8b. [DOI] [PubMed] [Google Scholar]
- 155.Moran CA, Hochholzer L, Fishback N, et al. Mucinous (so-called colloid) carcinomas of lung. Mod Pathol. 1992;5:634–638. [PubMed] [Google Scholar]
- 156.Rossi G, Murer B, Cavazza A, et al. Primary mucinous (so-called colloid) carcinomas of the lung: a clinicopathologic and immunohistochemical study with special reference to CDX-2 homeobox gene and MUC2 expression. Am J Surg Pathol. 2004;28:442–452. doi: 10.1097/00000478-200404000-00003. [DOI] [PubMed] [Google Scholar]
- 157.Gao ZH, Urbanski SJ. The spectrum of pulmonary mucinous cystic neoplasia: a clinicopathologic and immunohistochemical study of ten cases and review of literature. Am J Clin Pathol. 2005;124:62–70. doi: 10.1309/52XXR6E6U0J2JX0F. [DOI] [PubMed] [Google Scholar]
- 158.Nakatani Y, Kitamura H, Inayama Y, et al. Pulmonary adenocarcinomas of the fetal lung type: a clinicopathologic study indicating differences in histology, epidemiology, and natural history of low-grade and high-grade forms. Am J Surg Pathol. 1998;22:399–411. doi: 10.1097/00000478-199804000-00003. [DOI] [PubMed] [Google Scholar]
- 159.Nakatani Y, Masudo K, Miyagi Y, et al. Aberrant nuclear localization and gene mutation of beta-catenin in low-grade adenocarcinoma of fetal lung type: up-regulation of the Wnt signaling pathway may be a common denominator for the development of tumors that form morules. Mod Pathol. 2002;15:617–624. doi: 10.1038/modpathol.3880575. [DOI] [PubMed] [Google Scholar]
- 160.Sekine S, Shibata T, Matsuno Y, et al. Beta-catenin mutations in pulmonary blastomas: association with morule formation. J Pathol. 2003;200:214–221. doi: 10.1002/path.1352. [DOI] [PubMed] [Google Scholar]
- 161.Li HC, Schmidt L, Greenson JK, et al. Primary pulmonary adenocarcinoma with intestinal differentiation mimicking metastatic colorectal carcinoma: case report and review of literature. Am J Clin Pathol. 2009;131:129–133. doi: 10.1309/AJCPB04XWICTFERL. [DOI] [PubMed] [Google Scholar]
- 162.Hatanaka K, Tsuta K, Watanabe K, et al. Primary pulmonary adenocarcinoma with enteric differentiation resembling metastatic colorectal carcinoma: a report of the second case negative for cytokeratin 7. Pathol Res Pract. doi: 10.1016/j.prp.2010.07.005. In press. [DOI] [PubMed] [Google Scholar]
- 163.Yousem SA. Pulmonary intestinal-type adenocarcinoma does not show enteric differentiation by immunohistochemical study. Mod Pathol. 2005;18:816–821. doi: 10.1038/modpathol.3800358. [DOI] [PubMed] [Google Scholar]
- 164.Rossi G, Pelosi G, Graziano P, et al. A reevaluation of the clinical significance of histological subtyping of non–small-cell lung carcinoma: diagnostic algorithms in the era of personalized treatments. Int J Surg Pathol. 2009;17:206–218. doi: 10.1177/1066896909336178. [DOI] [PubMed] [Google Scholar]
- 165.Rossi G, Papotti M, Barbareschi M, et al. Morphology and a limited number of immunohistochemical markers may efficiently subtype non-small-cell lung cancer. J Clin Oncol. 2009;27:e141–e142. doi: 10.1200/JCO.2009.24.0515. author reply e3–e4. [DOI] [PubMed] [Google Scholar]
- 166.Suh J, Rekhtman N, Ladanyi M, et al. Testing of new IASLC/ATS/ERS criteria for diagnosis of lung adenocarcinoma (AD) in small biopsies: minimize immunohistochemistry (IHC) to maximize tissue for molecular studies. Mod Pathol. 2011;24(Supplement 1) In press. [Google Scholar]
- 167.Hanna N, Shepherd FA, Fossella FV, et al. Randomized phase III trial of pemetrexed versus docetaxel in patients with non-small-cell lung cancer previously treated with chemotherapy. J Clin Oncol. 2004;22:1589–1597. doi: 10.1200/JCO.2004.08.163. [DOI] [PubMed] [Google Scholar]
- 168.Yatabe Y, Mitsudomi T, Takahashi T. TTF-1 expression in pulmonary adenocarcinomas. Am J Surg Pathol. 2002;26:767–773. doi: 10.1097/00000478-200206000-00010. [DOI] [PubMed] [Google Scholar]
- 169.Lau SK, Luthringer DJ, Eisen RN. Thyroid transcription factor-1: a review. Appl Immunohistochem Mol Morphol. 2002;10:97–102. doi: 10.1097/00129039-200206000-00001. [DOI] [PubMed] [Google Scholar]
- 170.Camilo R, Capelozzi VL, Siqueira SA, et al. Expression of p63, keratin 5/6, keratin 7, and surfactant-A in non-small cell lung carcinomas. Hum Pathol. 2006;37:542–546. doi: 10.1016/j.humpath.2005.12.019. [DOI] [PubMed] [Google Scholar]
- 171.Wu M, Wang B, Gil J, et al. p63 and TTF-1 immunostaining. A useful marker panel for distinguishing small cell carcinoma of lung from poorly differentiated squamous cell carcinoma of lung. Am J Clin Pathol. 2003;119:696–702. doi: 10.1309/P5AB-R5KQ-89RN-JTFH. [DOI] [PubMed] [Google Scholar]
- 172.Chu PG, Weiss LM. Expression of cytokeratin 5/6 in epithelial neoplasms: an immunohistochemical study of 509 cases. Mod Pathol. 2002;15:6–10. doi: 10.1038/modpathol.3880483. [DOI] [PubMed] [Google Scholar]
- 173.Ordonez NG. Value of thyroid transcription factor-1, E-cadherin, BG8, WT1, and CD44S immunostaining in distinguishing epithelial pleural mesothelioma from pulmonary and nonpulmonary adenocarcinoma. Am J Surg Pathol. 2000;24:598–606. doi: 10.1097/00000478-200004000-00016. [DOI] [PubMed] [Google Scholar]
- 174.Kaufmann O, Dietel M. Thyroid transcription factor-1 is the superior immunohistochemical marker for pulmonary adenocarcinomas and large cell carcinomas compared to surfactant proteins A and B. Histopathology. 2000;36:8–16. doi: 10.1046/j.1365-2559.2000.00801.x. [DOI] [PubMed] [Google Scholar]
- 175.Kargi A, Gurel D, Tuna B. The diagnostic value of TTF-1, CK 5/6, and p63 immunostaining in classification of lung carcinomas. Appl Immunohistochem Mol Morphol. 2007;15:415–420. doi: 10.1097/PAI.0b013e31802fab75. [DOI] [PubMed] [Google Scholar]
- 176.Khayyata S, Yun S, Pasha T, et al. Value of P63 and CK5/6 in distinguishing squamous cell carcinoma from adenocarcinoma in lung fine-needle aspiration specimens. Diagn Cytopathol. 2009;37:178–183. doi: 10.1002/dc.20975. [DOI] [PubMed] [Google Scholar]
- 177.Chu P, Wu E, Weiss LM. Cytokeratin 7 and cytokeratin 20 expression in epithelial neoplasms: a survey of 435 cases. Mod Pathol. 2000;13:962–972. doi: 10.1038/modpathol.3880175. [DOI] [PubMed] [Google Scholar]
- 178.Rivera MP, Mehta AC. Initial diagnosis of lung cancer: ACCP evidence-based clinical practice guidelines (2nd edition) Chest. 2007;132:131S–148S. doi: 10.1378/chest.07-1357. [DOI] [PubMed] [Google Scholar]
- 179.Rekhtman N, Brandt SM, Sigel CS, et al. Suitability of thoracic cytology for new therapeutic paradigms in non-small cell lung carcinoma: high accuracy of tumor subtyping and feasibility of EGFR and KRAS molecular testing. J Thorac Oncol. doi: 10.1097/JTO.0b013e31820517a3. In press. [DOI] [PubMed] [Google Scholar]
- 180.Sigel CS, Friedlander MA, Zakowski MF, et al. Subtyping of non-small cell lung carcinoma (NSCLC): comparison of cytology and small biopsy specimens. Mod Pathol. 2010;23:414A. [Google Scholar]
- 181.Zhang X, Zhao Y, Wang M, et al. Detection and comparison of epidermal growth factor receptor mutations in cells and fluid of malignant pleural effusion in non-small cell lung cancer. Lung Cancer. 2008;60:175–182. doi: 10.1016/j.lungcan.2007.10.011. [DOI] [PubMed] [Google Scholar]
- 182.Zakowski MF, Hussain S, Pao W, et al. Morphologic features of adenocarcinoma of the lung predictive of response to the epidermal growth factor receptor kinase inhibitors erlotinib and gefitinib. Arch Pathol Lab Med. 2009;133:470–477. doi: 10.1043/1543-2165-133.3.470. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 183.Wu SG, Gow CH, Yu CJ, et al. Frequent EGFR mutations in malignant pleural effusion of lung adenocarcinoma. Eur Respir J. 2008;32:924–930. doi: 10.1183/09031936.00167407. [DOI] [PubMed] [Google Scholar]
- 184.Au NH, Gown AM, Cheang M, et al. P63 expression in lung carcinoma: a tissue microarray study of 408 cases. Appl Immunohistochem Mol Morphol. 2004;12:240–247. doi: 10.1097/00129039-200409000-00010. [DOI] [PubMed] [Google Scholar]
- 185.Ang DC, Ghaffar H, Zakowski MF, et al. Expression of squamous markers in lung adenocarcinoma (AD): clinicopathologic and molecular correlates, and implications for differentiation from squamous cell carcinoma (SqCC) Mod Pathol. 2010;23:397A. [Google Scholar]
- 186.Ionescu DN, Treaba D, Gilks CB, et al. Nonsmall cell lung carcinoma with neuroendocrine differentiation–an entity of no clinical or prognostic significance. Am J Surg Pathol. 2007;31:26–32. doi: 10.1097/01.pas.0000213319.04919.97. [DOI] [PubMed] [Google Scholar]
- 187.Sterlacci W, Fiegl M, Hilbe W, et al. Clinical relevance of neuroendocrine differentiation in non-small cell lung cancer assessed by immunohistochemistry: a retrospective study on 405 surgically resected cases. Virchows Arch. 2009;455:125–132. doi: 10.1007/s00428-009-0812-0. [DOI] [PubMed] [Google Scholar]
- 188.Chung CK, Zaino R, Stryker JA, et al. Carcinoma of the lung: evaluation of histological grade and factors influencing prognosis. Ann Thorac Surg. 1982;33:599–604. doi: 10.1016/s0003-4975(10)60819-3. [DOI] [PubMed] [Google Scholar]
- 189.Kobayashi N, Toyooka S, Soh J, et al. Risk factors for recurrence and unfavorable prognosis in patients with stage I non-small cell lung cancer and a tumor diameter of 20 mm or less. J Thorac Oncol. 2007;2:808–812. doi: 10.1097/JTO.0b013e31814617c7. [DOI] [PubMed] [Google Scholar]
- 190.Nakazato Y, Minami Y, Kobayashi H, et al. Nuclear grading of primary pulmonary adenocarcinomas—correlation between nuclear size and prognosis. J Thorac Oncol. 2009;4:S495. doi: 10.1002/cncr.24948. [DOI] [PubMed] [Google Scholar]
- 191.Petersen I, Kotb WF, Friedrich KH, et al. Core classification of lung cancer: correlating nuclear size and mitoses with ploidy and clinicopathological parameters. Lung Cancer. 2009;65:312–318. doi: 10.1016/j.lungcan.2008.12.013. [DOI] [PubMed] [Google Scholar]
- 192.Aida S, Shimazaki H, Sato K, et al. Prognostic analysis of pulmonary adenocarcinoma subclassification with special consideration of papillary and bronchioloalveolar types. Histopathology. 2004;45:468–476. doi: 10.1111/j.1365-2559.2004.01946.x. [DOI] [PubMed] [Google Scholar]
- 193.Gleason DF. Histologic grading of prostate cancer: a perspective. Hum Pathol. 1992;23:273–279. doi: 10.1016/0046-8177(92)90108-f. [DOI] [PubMed] [Google Scholar]
- 194.Kadota K, Suzuki K, Rusch VW, et al. Nuclear grading system predicts recurrence in stage I lung adenocarcinoma patients. Mod Pathol. 2011;24(Supplement 1) In press. [Google Scholar]
- 195.Li AR, Chitale D, Riely GJ, et al. EGFR mutations in lung adenocarcinomas: clinical testing experience and relationship to EGFR gene copy number and immunohistochemical expression. J Mol Diagn. 2008;10:242–248. doi: 10.2353/jmoldx.2008.070178. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 196.Lim EH, Zhang SL, Li JL, et al. Using whole genome amplification (WGA) of low-volume biopsies to assess the prognostic role of EGFR, KRAS, p53, and CMET mutations in advanced-stage non-small cell lung cancer (NSCLC) J Thorac Oncol. 2009;4:12–21. doi: 10.1097/JTO.0b013e3181913e28. [DOI] [PubMed] [Google Scholar]
- 197.Savic S, Tapia C, Grilli B, et al. Comprehensive epidermal growth factor receptor gene analysis from cytological specimens of non-small-cell lung cancers. Br J Cancer. 2008;98:154–160. doi: 10.1038/sj.bjc.6604142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 198.Miller VA, Riely GJ, Zakowski MF, et al. Molecular characteristics of bronchioloalveolar carcinoma and adenocarcinoma, bronchioloalveolar carcinoma subtype, predict response to erlotinib. J Clin Oncol. 2008;26:1472–1478. doi: 10.1200/JCO.2007.13.0062. [DOI] [PubMed] [Google Scholar]
- 199.Kimura H, Fujiwara Y, Sone T, et al. EGFR mutation status in tumour-derived DNA from pleural effusion fluid is a practical basis for predicting the response to gefitinib. Br J Cancer. 2006;95:1390–1395. doi: 10.1038/sj.bjc.6603428. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 200.Borczuk AC, Shah L, Pearson GD, et al. Molecular signatures in biopsy specimens of lung cancer. Am J Respir Crit Care Med. 2004;170:167–174. doi: 10.1164/rccm.200401-066OC. [DOI] [PubMed] [Google Scholar]
- 201.Zudaire I, Lozano MD, Vazquez MF, et al. Molecular characterization of small peripheral lung tumors based on the analysis of fine needle aspirates. Histol Histopathol. 2008;23:33–40. doi: 10.14670/HH-23.33. [DOI] [PubMed] [Google Scholar]
- 202.Gordon GJ, Richards WG, Sugarbaker DJ, et al. A prognostic test for adenocarcinoma of the lung from gene expression profiling data. Cancer Epidemiol Biomarkers Prev. 2003;12:905–910. [PubMed] [Google Scholar]
- 203.Solomon SB, Zakowski MF, Pao W, et al. Core needle lung biopsy specimens: adequacy for EGFR and KRAS mutational analysis. AJR Am J Roentgenol. 2010;194:266–269. doi: 10.2214/AJR.09.2858. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 204.Asano H, Toyooka S, Tokumo M, et al. Detection of EGFR gene mutation in lung cancer by mutant-enriched polymerase chain reaction assay. Clin Cancer Res. 2006;12:43–48. doi: 10.1158/1078-0432.CCR-05-0934. [DOI] [PubMed] [Google Scholar]
- 205.Otani H, Toyooka S, Soh J, et al. Detection of EGFR gene mutations using the wash fluid of CT-guided biopsy needle in NSCLC patients. J Thorac Oncol. 2008;3:472–476. doi: 10.1097/JTO.0b013e31816de2cd. [DOI] [PubMed] [Google Scholar]
- 206.Bepler G, Kusmartseva I, Sharma S, et al. RRM1 modulated in vitro and in vivo efficacy of gemcitabine and platinum in non-small-cell lung cancer. J Clin Oncol. 2006;24:4731–4737. doi: 10.1200/JCO.2006.06.1101. [DOI] [PubMed] [Google Scholar]
- 207.Olaussen KA, Dunant A, Fouret P, et al. DNA repair by ERCC1 in non-small-cell lung cancer and cisplatin-based adjuvant chemotherapy. N Engl J Med. 2006;355:983–991. doi: 10.1056/NEJMoa060570. [DOI] [PubMed] [Google Scholar]
- 208.Chang MH, Ahn JS, Lee J, et al. The efficacy of pemetrexed as a third- or fourth-line therapy and the significance of thymidylate synthase expression in patients with advanced non-small cell lung cancer. Lung Cancer. 2010;69:323–329. doi: 10.1016/j.lungcan.2009.12.002. [DOI] [PubMed] [Google Scholar]
- 209.Monica V, Scagliotti GV, Ceppi P, et al. Differential thymidylate synthase expression in different variants of large-cell carcinoma of the lung. Clin Cancer Res. 2009;15:7547–7552. doi: 10.1158/1078-0432.CCR-09-1641. [DOI] [PubMed] [Google Scholar]
- 210.Kang CH, Jang BG, Kim DW, et al. The prognostic significance of ERCC1, BRCA1, XRCC1, and betaIII-tubulin expression in patients with non-small cell lung cancer treated by platinum- and taxane-based neoadjuvant chemotherapy and surgical resection. Lung Cancer. 2010;68:478–483. doi: 10.1016/j.lungcan.2009.07.004. [DOI] [PubMed] [Google Scholar]
- 211.Rosell R, Perez-Roca L, Sanchez JJ, et al. Customized treatment in non-small-cell lung cancer based on EGFR mutations and BRCA1 mRNA expression. PLoS One. 2009;4:e5133. doi: 10.1371/journal.pone.0005133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 212.Savci-Heijink CD, Kosari F, Aubry MC, et al. The role of desmoglein-3 in the diagnosis of squamous cell carcinoma of the lung. Am J Pathol. 2009;174:1629–1637. doi: 10.2353/ajpath.2009.080778. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 213.Monica V, Ceppi P, Righi L, et al. Desmocollin-3: a new marker of squamous differentiation in undifferentiated large-cell carcinoma of the lung. Mod Pathol. 2009;22:709–717. doi: 10.1038/modpathol.2009.30. [DOI] [PubMed] [Google Scholar]
- 214.Bishop JA, Sharma R, Illei PB. Napsin A and thyroid transcription factor-1 expression in carcinomas of the lung, breast, pancreas, colon, kidney, thyroid, and malignant mesothelioma. Hum Pathol. 2010;41:20–25. doi: 10.1016/j.humpath.2009.06.014. [DOI] [PubMed] [Google Scholar]
- 215.Paez JG, Janne PA, Lee JC, et al. EGFR mutations in lung cancer: correlation with clinical response to gefitinib therapy. Science. 2004;304:1497–1500. doi: 10.1126/science.1099314. [DOI] [PubMed] [Google Scholar]
- 216.Lynch TJ, Bell DW, Sordella R, et al. Activating mutations in the epidermal growth factor receptor underlying responsiveness of non-small-cell lung cancer to gefitinib. N Engl J Med. 2004;350:2129–2139. doi: 10.1056/NEJMoa040938. [DOI] [PubMed] [Google Scholar]
- 217.Pao W, Miller V, Zakowski M, et al. EGF receptor gene mutations are common in lung cancers from “never smokers” and are associated with sensitivity of tumors to gefitinib and erlotinib. Proc Natl Acad Sci USA. 2004;101:13306–13311. doi: 10.1073/pnas.0405220101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 218.Azzoli CG, Baker S, Jr, Temin S, et al. American Society of Clinical Oncology Clinical Practice Guideline update on chemotherapy for stage IV non-small-cell lung cancer. J Clin Oncol. 2009;27:6251–6266. doi: 10.1200/JCO.2009.23.5622. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 219.Pao W, Kris MG, Iafrate AJ, et al. Integration of molecular profiling into the lung cancer clinic. Clin Cancer Res. 2009;15:5317–5322. doi: 10.1158/1078-0432.CCR-09-0913. [DOI] [PubMed] [Google Scholar]
- 220.Shaw AT, Yeap BY, Mino-Kenudson M, et al. Clinical features and outcome of patients with non-small-cell lung cancer who harbor EML4-ALK. J Clin Oncol. 2009;27:4247–4253. doi: 10.1200/JCO.2009.22.6993. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 221.Detterbeck FC, Jantz MA, Wallace M, et al. Invasive mediastinal staging of lung cancer: ACCP evidence-based clinical practice guidelines (2nd edition) Chest. 2007;132:202S–220S. doi: 10.1378/chest.07-1362. [DOI] [PubMed] [Google Scholar]
- 222.Schrump DS, Giaccone G, Kelsey CR, et al. Non-small cell lung cancer. In: DeVita VT, Lawrence TS, Rosenberg SA, editors. Cancer, Princiiples and Practice of Oncology. 7th Ed. Philadelphia: Wolters Kluwer; Lippincott, Williams & Wilkins; 2008. pp. 887–895. [Google Scholar]
- 223.Sculier JP, Chansky K, Crowley JJ, et al. The impact of additional prognostic factors on survival and their relationship with the anatomical extent of disease expressed by the 6th Edition of the TNM Classification of Malignant Tumors and the proposals for the 7th Edition. J Thorac Oncol. 2008;3:457–466. doi: 10.1097/JTO.0b013e31816de2b8. [DOI] [PubMed] [Google Scholar]
- 224.Chansky K, Sculier JP, Crowley JJ, et al. The International Association for the Study of Lung Cancer Staging Project: prognostic factors and pathologic TNM stage in surgically managed non-small cell lung cancer. J Thorac Oncol. 2009;4:792–801. doi: 10.1097/JTO.0b013e3181a7716e. [DOI] [PubMed] [Google Scholar]
- 225.Janjigian YY, McDonnell K, Kris MG, et al. Pack-years of cigarette smoking as a prognostic factor in patients with stage IIIB/IV Nonsmall cell lung cancer. Cancer. 2010;116:670–675. doi: 10.1002/cncr.24813. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 226.Miller VA, Kris MG, Shah N, et al. Bronchioloalveolar pathologic subtype and smoking history predict sensitivity to gefitinib in advanced non-small-cell lung cancer. J Clin Oncol. 2004;22:1103–1109. doi: 10.1200/JCO.2004.08.158. [DOI] [PubMed] [Google Scholar]
- 227.West HL, Franklin WA, McCoy J, et al. Gefitinib therapy in advanced bronchioloalveolar carcinoma: Southwest Oncology Group Study S0126. J Clin Oncol. 2006;24:1807–1813. doi: 10.1200/JCO.2005.04.9890. [DOI] [PubMed] [Google Scholar]
- 228.Sequist LV, Bell DW, Lynch TJ, et al. Molecular predictors of response to epidermal growth factor receptor antagonists in non-small-cell lung cancer. J Clin Oncol. 2007;25:587–595. doi: 10.1200/JCO.2006.07.3585. [DOI] [PubMed] [Google Scholar]
- 229.Sutani A, Nagai Y, Udagawa K, et al. Gefitinib for non-small-cell lung cancer patients with epidermal growth factor receptor gene mutations screened by peptide nucleic acid-locked nucleic acid PCR clamp. Br J Cancer. 2006;95:1483–1489. doi: 10.1038/sj.bjc.6603466. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 230.Inoue A, Suzuki T, Fukuhara T, et al. Prospective phase II study of gefitinib for chemotherapy-naive patients with advanced non-small-cell lung cancer with epidermal growth factor receptor gene mutations. J Clin Oncol. 2006;24:3340–3346. doi: 10.1200/JCO.2005.05.4692. [DOI] [PubMed] [Google Scholar]
- 231.Inoue A, Kobayashi K, Usui K, et al. First-line gefitinib for patients with advanced non-small-cell lung cancer harboring epidermal growth factor receptor mutations without indication for chemotherapy. J Clin Oncol. 2009;27:1394–1400. doi: 10.1200/JCO.2008.18.7658. [DOI] [PubMed] [Google Scholar]
- 232.Tamura K, Okamoto I, Kashii T, et al. Multicentre prospective phase II trial of gefitinib for advanced non-small cell lung cancer with epidermal growth factor receptor mutations: results of the West Japan Thoracic Oncology Group trial (WJTOG0403) Br J Cancer. 2008;98:907–914. doi: 10.1038/sj.bjc.6604249. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 233.Yoshida K, Yatabe Y, Park JY, et al. Prospective validation for prediction of gefitinib sensitivity by epidermal growth factor receptor gene mutation in patients with non-small cell lung cancer. J Thorac Oncol. 2007;2:22–28. [PubMed] [Google Scholar]
- 234.Douillard JY, Shepherd FA, Hirsh V, et al. Molecular predictors of outcome with gefitinib and docetaxel in previously treated non-small-cell lung cancer: data from the randomized phase III INTEREST trial. J Clin Oncol. 2010;28:744–752. doi: 10.1200/JCO.2009.24.3030. [DOI] [PubMed] [Google Scholar]
- 235.Hirsch FR, Varella-Garcia M, Bunn PA, Jr, et al. Molecular predictors of outcome with gefitinib in a phase III placebo-controlled study in advanced non-small-cell lung cancer. J Clin Oncol. 2006;24:5034–5042. doi: 10.1200/JCO.2006.06.3958. [DOI] [PubMed] [Google Scholar]
- 236.Zhu CQ, da Cunha Santos G, Ding K, et al. Role of KRAS and EGFR as biomarkers of response to erlotinib in National Cancer Institute of Canada Clinical Trials Group Study BR. 21. J Clin Oncol. 2008;26:4268–4275. doi: 10.1200/JCO.2007.14.8924. [DOI] [PubMed] [Google Scholar]
- 237.Sholl LM, Xiao Y, Joshi V, et al. EGFR mutation is a better predictor of response to tyrosine kinase inhibitors in non-small cell lung carcinoma than FISH, CISH, and immunohistochemistry. Am J Clin Pathol. 2010;133:922–934. doi: 10.1309/AJCPST1CTHZS3PSZ. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 238.Kawahara A, Yamamoto C, Nakashima K, et al. Molecular diagnosis of activating EGFR mutations in non-small cell lung cancer using mutation specific antibodies for immunohistochemical analysis. Clin Cancer Res. 2010;16:3163–3170. doi: 10.1158/1078-0432.CCR-09-3239. [DOI] [PubMed] [Google Scholar]
- 239.Brevet M, Arcila M, Ladanyi M. Assessment of EGFR mutation status in lung adenocarcinoma by immunohistochemistry using antibodies specific to the two major forms of mutant EGFR. J Mol Diagn. 2010;12:169–176. doi: 10.2353/jmoldx.2010.090140. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 240.Yu J, Kane S, Wu J, et al. Mutation-specific antibodies for the detection of EGFR mutations in non-small-cell lung cancer. Clin Cancer Res. 2009;15:3023–3028. doi: 10.1158/1078-0432.CCR-08-2739. [DOI] [PubMed] [Google Scholar]
- 241.Fukuoka M, Wu Y, Thongprasert S, et al. Biomarker analyses from a phase III, randomized, open-label, first-line study of gefitinib (G) versus carboblatin/paclitaxel (C/P) in clinically selected patients (pts) with advanced non-small-cell lung cancer (NSCLC) in Asia (IPASS) J Clin Oncol. 2009;27:521S. doi: 10.1200/JCO.2010.33.4235. [DOI] [PubMed] [Google Scholar]
- 242.Kubota K, Niho S, Enatsu S, et al. Efficacy differences of pemetrexed by histology in pretreated patients with stage IIIB/IV non-small cell lung cancer: review of results from an open-label randomized phase II study. J Thorac Oncol. 2009;4:1530–1536. doi: 10.1097/JTO.0b013e3181b9e608. [DOI] [PubMed] [Google Scholar]
- 243.Zinner RG, Novello S, Peng G, et al. Comparison of patient outcomes according to histology among pemetrexed-treated patients with stage IIIB/IV non-small-cell lung cancer in two phase II trials. Clin Lung Cancer. 2010;11:126–131. doi: 10.3816/CLC.2010.n.017. [DOI] [PubMed] [Google Scholar]
- 244.Gronberg BH, Bremnes RM, Flotten O, et al. Phase III study by the Norwegian lung cancer study group: pemetrexed plus carboplatin compared with gemcitabine plus carboplatin as first-line chemotherapy in advanced non-small-cell lung cancer. J Clin Oncol. 2009;27:3217–3224. doi: 10.1200/JCO.2008.20.9114. [DOI] [PubMed] [Google Scholar]
- 245.Sandler A, Gray R, Perry MC, et al. Paclitaxel-carboplatin alone or with bevacizumab for non-small-cell lung cancer. N Engl J Med. 2006;355:2542–2550. doi: 10.1056/NEJMoa061884. [DOI] [PubMed] [Google Scholar]
- 246.Soda M, Choi YL, Enomoto M, et al. Identification of the transforming EML4-ALK fusion gene in non-small-cell lung cancer. Nature. 2007;448:561–566. doi: 10.1038/nature05945. [DOI] [PubMed] [Google Scholar]
- 247.Wong DW, Leung EL, So KK, et al. The EML4-ALK fusion gene is involved in various histologic types of lung cancers from nonsmokers with wild-type EGFR and KRAS. Cancer. 2009;115:1723–1733. doi: 10.1002/cncr.24181. [DOI] [PubMed] [Google Scholar]
- 248.Kwak EL, Bang YJ, Camidge DR, et al. Anaplastic lymphoma kinase inhibition in non-small-cell lung cancer. N Engl J Med. 2010;363:1693–1703. doi: 10.1056/NEJMoa1006448. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 249.Choi YL, Soda M, Yamashita Y, et al. EML4-ALK mutations in lung cancer that confer resistance to ALK inhibitors. N Engl J Med. 2010;363:1734–1739. doi: 10.1056/NEJMoa1007478. [DOI] [PubMed] [Google Scholar]
- 250.Mao C, Qiu LX, Liao RY, et al. KRAS mutations and resistance to EGFR-TKIs treatment in patients with non-small cell lung cancer: a meta-analysis of 22 studies. Lung Cancer. 2010;69:272–278. doi: 10.1016/j.lungcan.2009.11.020. [DOI] [PubMed] [Google Scholar]
- 251.Linardou H, Dahabreh IJ, Kanaloupiti D, et al. Assessment of somatic k-RAS mutations as a mechanism associated with resistance to EGFR-targeted agents: a systematic review and meta-analysis of studies in advanced non-small-cell lung cancer and metastatic colorectal cancer. Lancet Oncol. 2008;9:962–972. doi: 10.1016/S1470-2045(08)70206-7. [DOI] [PubMed] [Google Scholar]
- 252.Goldstraw P. IASLC Staging Manual in Thoracic Oncology. Orange Park, FL: International Association for the Study of Lung Cancer, Editorial Rx Press; 2009. [Google Scholar]
- 253.Goldstraw P, Crowley J, Chansky K, et al. The IASLC Lung Cancer Staging Project: proposals for the revision of the TNM stage groupings in the forthcoming (seventh) edition of the TNM Classification of malignant tumours. J Thorac Oncol. 2007;2:706–714. doi: 10.1097/JTO.0b013e31812f3c1a. [DOI] [PubMed] [Google Scholar]
- 254.Pignon JP, Tribodet H, Scagliotti GV, et al. Lung adjuvant cisplatin evaluation: a pooled analysis by the LACE Collaborative Group. J Clin Oncol. 2008;26:3552–3559. doi: 10.1200/JCO.2007.13.9030. [DOI] [PubMed] [Google Scholar]
- 255.Pao W, Wang TY, Riely GJ, et al. KRAS mutations and primary resistance of lung adenocarcinomas to gefitinib or erlotinib. PLoS Med. 2005;2:e17. doi: 10.1371/journal.pmed.0020017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 256.Kim CF, Jackson EL, Woolfenden AE, et al. Identification of bronchioalveolar stem cells in normal lung and lung cancer. Cell. 2005;121:823–835. doi: 10.1016/j.cell.2005.03.032. [DOI] [PubMed] [Google Scholar]
- 257.Weir BA, Woo MS, Getz G, et al. Characterizing the cancer genome in lung adenocarcinoma. Nature. 2007;450:893–898. doi: 10.1038/nature06358. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 258.Tanaka H, Yanagisawa K, Shinjo K, et al. Lineage-specific dependency of lung adenocarcinomas on the lung development regulator TTF-1. Cancer Res. 2007;67:6007–6011. doi: 10.1158/0008-5472.CAN-06-4774. [DOI] [PubMed] [Google Scholar]
- 259.Colby TV, Leslie KO, Yousem SA. Lungs. In: Mills SE, editor. Histology for Pathologists. 3rd ed. Philadelphia: Lippincott Williams & Wilkins; 2007. pp. 473–504. [Google Scholar]
- 260.Wang BY, Gil J, Kaufman D, et al. P63 in pulmonary epithelium, pulmonary squamous neoplasms, and other pulmonary tumors. Hum Pathol. 2002;33:921–926. doi: 10.1053/hupa.2002.126878. [DOI] [PubMed] [Google Scholar]
- 261.Takeuchi T, Tomida S, Yatabe Y, et al. Expression profile-defined classification of lung adenocarcinoma shows close relationship with underlying major genetic changes and clinicopathologic behaviors. J Clin Oncol. 2006;24:1679–1688. doi: 10.1200/JCO.2005.03.8224. [DOI] [PubMed] [Google Scholar]
- 262.Colby TV, Wistuba II, Gazdar A. Precursors to pulmonary neoplasia. Adv Anat Pathol. 1998;5:205–215. doi: 10.1097/00125480-199807000-00001. [DOI] [PubMed] [Google Scholar]
- 263.Westra WH. Early glandular neoplasia of the lung. Respir Res. 2000;1:163–169. doi: 10.1186/rr28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 264.Tang X, Varella-Garcia M, Xavier AC, et al. Epidermal growth factor receptor abnormalities in the pathogenesis and progression of lung adenocarcinomas. Cancer Prev Res (Phila Pa) 2008;1:192–200. doi: 10.1158/1940-6207.CAPR-08-0032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 265.Tang X, Shigematsu H, Bekele BN, et al. EGFR tyrosine kinase domain mutations are detected in histologically normal respiratory epithelium in lung cancer patients. Cancer Res. 2005;65:7568–7572. doi: 10.1158/0008-5472.CAN-05-1705. [DOI] [PubMed] [Google Scholar]
- 266.Soh J, Toyooka S, Ichihara S, et al. Sequential molecular changes during multistage pathogenesis of small peripheral adenocarcinomas of the lung. J Thorac Oncol. 2008;3:340–347. doi: 10.1097/JTO.0b013e318168d20a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 267.Yatabe Y, Takahashi T, Mitsudomi T. Epidermal growth factor receptor gene amplification is acquired in association with tumor progression of EGFR-mutated lung cancer. Cancer Res. 2008;68:2106–2111. doi: 10.1158/0008-5472.CAN-07-5211. [DOI] [PubMed] [Google Scholar]
- 268.Tang ZQ, Han LY, Lin HH, et al. Derivation of stable microarray cancer-differentiating signatures using consensus scoring of multiple random sampling and gene-ranking consistency evaluation. Cancer Res. 2007;67:9996–10003. doi: 10.1158/0008-5472.CAN-07-1601. [DOI] [PubMed] [Google Scholar]
- 269.Koga T, Hashimoto S, Sugio K, et al. Clinicopathological and molecular evidence indicating the independence of bronchioloalveolar components from other subtypes of human peripheral lung adenocarcinoma. Clin Cancer Res. 2001;7:1730–1738. [PubMed] [Google Scholar]
- 270.Marchetti A, Pellegrini S, Bertacca G, et al. FHIT and p53 gene abnormalities in bronchioloalveolar carcinomas. Correlations with clinicopathological data and K-ras mutations. J Pathol. 1998;184:240–246. doi: 10.1002/(SICI)1096-9896(199803)184:3<240::AID-PATH20>3.0.CO;2-B. [DOI] [PubMed] [Google Scholar]
- 271.Yoshida Y, Kokubu A, Suzuki K, et al. Molecular markers and changes of computed tomography appearance in lung adenocarcinoma with ground-glass opacity. Jpn J Clin Oncol. 2007;37:907–912. doi: 10.1093/jjco/hym139. [DOI] [PubMed] [Google Scholar]
- 272.Terasaki H, Niki T, Matsuno Y, et al. Lung adenocarcinoma with mixed bronchioloalveolar and invasive components: clinicopathological features, subclassification by extent of invasive foci, and immunohistochemical characterization. Am J Surg Pathol. 2003;27:937–951. doi: 10.1097/00000478-200307000-00009. [DOI] [PubMed] [Google Scholar]
- 273.Huang CL, Taki T, Adachi M, et al. Mutations of p53 and K-ras genes as prognostic factors for non-small cell lung cancer. Int J Oncol. 1998;12:553–563. doi: 10.3892/ijo.12.3.553. [DOI] [PubMed] [Google Scholar]
- 274.Shigematsu H, Lin L, Takahashi T, et al. Clinical and biological features associated with epidermal growth factor receptor gene mutations in lung cancers. J Natl Cancer Inst. 2005;97:339–346. doi: 10.1093/jnci/dji055. [DOI] [PubMed] [Google Scholar]
- 275.Marchetti A, Martella C, Felicioni L, et al. EGFR mutations in non-small-cell lung cancer: analysis of a large series of cases and development of a rapid and sensitive method for diagnostic screening with potential implications on pharmacologic treatment. J Clin Oncol. 2005;23:857–865. doi: 10.1200/JCO.2005.08.043. [DOI] [PubMed] [Google Scholar]
- 276.Ohtsuka T, Watanabe K, Kaji M, et al. A clinicopathological study of resected pulmonary nodules with focal pure ground-glass opacity. Eur J Cardiothorac Surg. 2006;30:160–163. doi: 10.1016/j.ejcts.2006.03.058. [DOI] [PubMed] [Google Scholar]
- 277.Sonobe M, Manabe T, Wada H, et al. Mutations in the epidermal growth factor receptor gene are linked to smoking-independent, lung adenocarcinoma. Br J Cancer. 2005;93:355–363. doi: 10.1038/sj.bjc.6602707. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 278.Bryant CM, Albertus DL, Kim S, et al. Clinically relevant characterization of lung adenocarcinoma subtypes based on cellular pathways: an international validation study. PLoS One. 2010;5:e11712. doi: 10.1371/journal.pone.0011712. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 279.Yousem SA, Nikiforova M, Nikiforov Y. The histopathology of BRAF-V600E-mutated lung adenocarcinoma. Am J Surg Pathol. 2008;32:1317–1321. doi: 10.1097/PAS.0b013e31816597ca. [DOI] [PubMed] [Google Scholar]
- 280.Conde E, Angulo B, Tang M, et al. Molecular context of the EGFR mutations: evidence for the activation of mTOR/S6K signaling. Clin Cancer Res. 2006;12:710–717. doi: 10.1158/1078-0432.CCR-05-1362. [DOI] [PubMed] [Google Scholar]
- 281.Ohtsuka K, Ohnishi H, Furuyashiki G, et al. Clinico-pathological and biological significance of tyrosine kinase domain gene mutations and overexpression of epidermal growth factor receptor for lung adenocarcinoma. J Thorac Oncol. 2006;1:787–795. [PubMed] [Google Scholar]
- 282.Sonobe M, Manabe T, Wada H, et al. Lung adenocarcinoma harboring mutations in the ERBB2 kinase domain. J Mol Diagn. 2006;8:351–356. doi: 10.2353/jmoldx.2006.050132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 283.Ninomiya H, Hiramatsu M, Inamura K, et al. Correlation between morphology and EGFR mutations in lung adenocarcinomas Significance of the micropapillary pattern and the hobnail cell type. Lung Cancer. 2009;63:235–240. doi: 10.1016/j.lungcan.2008.04.017. [DOI] [PubMed] [Google Scholar]
- 284.Hirsch FR, Varella-Garcia M, McCoy J, et al. Increased epidermal growth factor receptor gene copy number detected by fluorescence in situ hybridization associates with increased sensitivity to gefitinib in patients with bronchioloalveolar carcinoma subtypes: a southwest oncology group study. J Clin Oncol. 2005;23:6838–6845. doi: 10.1200/JCO.2005.01.2823. [DOI] [PubMed] [Google Scholar]
- 285.Tanaka R, Horikoshi H, Nakazato Y, et al. Magnetic resonance imaging in peripheral lung adenocarcinoma: correlation with histopathologic features. J Thorac Imaging. 2009;24:4–9. doi: 10.1097/RTI.0b013e31818703b7. [DOI] [PubMed] [Google Scholar]
- 286.Stenhouse G, Fyfe N, King G, et al. Thyroid transcription factor 1 in pulmonary adenocarcinoma. J Clin Pathol. 2004;57:383–387. doi: 10.1136/jcp.2003.007138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 287.Kim YT, Kim TY, Lee DS, et al. Molecular changes of epidermal growth factor receptor (EGFR) and KRAS and their impact on the clinical outcomes in surgically resected adenocarcinoma of the lung. Lung Cancer. 2008;59:111–118. doi: 10.1016/j.lungcan.2007.08.008. [DOI] [PubMed] [Google Scholar]
- 288.Ang DC, Zakowski MF, Ladanyi M, et al. Characteristic morphology and immunoprofile of lung adenocarcinoma with KRAS mutations: propensity for solid growth pattern and correlation with TTF-1 expression. Mod Pathol. 2010;23(Suppl):396A. [Google Scholar]
- 289.Saad RS, Cho P, Silverman JF, et al. Usefulness of Cdx2 in separating mucinous bronchioloalveolar adenocarcinoma of the lung from metastatic mucinous colorectal adenocarcinoma. Am J Clin Pathol. 2004;122:421–427. doi: 10.1309/UMF7-15KR-G2V1-98YD. [DOI] [PubMed] [Google Scholar]
- 290.Shrestha B, Ebihara Y, Osakabe Y, et al. Immunohistochemical, ultrastructural and molecular study of well differentiated adenocarcinomas of the lung predominantly composed of goblet cells. Lung Cancer. 1998;22:103–117. doi: 10.1016/s0169-5002(98)00052-x. [DOI] [PubMed] [Google Scholar]
- 291.Yatabe Y, Koga T, Mitsudomi T, et al. CK20 expression, CDX2 expression, K-ras mutation, and goblet cell morphology in a subset of lung adenocarcinomas. J Pathol. 2004;203:645–652. doi: 10.1002/path.1566. [DOI] [PubMed] [Google Scholar]
- 292.Sasaki H, Kawano O, Endo K, et al. Uncommon V599E BRAF mutations in Japanese patients with lung cancer. J Surg Res. 2006;133:203–206. doi: 10.1016/j.jss.2005.10.022. [DOI] [PubMed] [Google Scholar]
- 293.Naoki K, Chen TH, Richards WG, et al. Missense mutations of the BRAF gene in human lung adenocarcinoma. Cancer Res. 2002;62:7001–7003. [PubMed] [Google Scholar]
- 294.Tang Z, Du R, Jiang S, et al. Dual MET-EGFR combinatorial inhibition against T790M-EGFR-mediated erlotinib-resistant lung cancer. Br J Cancer. 2008;99:911–922. doi: 10.1038/sj.bjc.6604559. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 295.Cappuzzo F, Janne PA, Skokan M, et al. MET increased gene copy number and primary resistance to gefitinib therapy in non-small-cell lung cancer patients. Ann Oncol. 2009;20:298–304. doi: 10.1093/annonc/mdn635. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 296.Engelman JA, Zejnullahu K, Mitsudomi T, et al. MET amplification leads to gefitinib resistance in lung cancer by activating ERBB3 signaling. Science. 2007;316:1039–1043. doi: 10.1126/science.1141478. [DOI] [PubMed] [Google Scholar]
- 297.Pao W, Miller VA, Politi KA, et al. Acquired resistance of lung adenocarcinomas to gefitinib or erlotinib is associated with a second mutation in the EGFR kinase domain. PLoS Med. 2005;2:e73. doi: 10.1371/journal.pmed.0020073. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 298.Sequist LV, Martins RG, Spigel D, et al. First-line gefitinib in patients with advanced non-small-cell lung cancer harboring somatic EGFR mutations. J Clin Oncol. 2008;26:2442–2449. doi: 10.1200/JCO.2007.14.8494. [DOI] [PubMed] [Google Scholar]
- 299.Nguyen KS, Kobayashi S, Costa DB. Acquired resistance to epidermal growth factor receptor tyrosine kinase inhibitors in non-small-cell lung cancers dependent on the epidermal growth factor receptor pathway. Clin Lung Cancer. 2009;10:281–289. doi: 10.3816/CLC.2009.n.039. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 300.Takahashi T, Sonobe M, Kobayashi M, et al. Clinicopathologic features of non-small-cell lung cancer with EML4-ALK fusion gene. Ann Surg Oncol. 2010;17:889–897. doi: 10.1245/s10434-009-0808-7. [DOI] [PubMed] [Google Scholar]
- 301.Inamura K, Takeuchi K, Togashi Y, et al. EML4-ALK lung cancers are characterized by rare other mutations, a TTF-1 cell lineage, an acinar histology, and young onset. Mod Pathol. 2009;22:508–515. doi: 10.1038/modpathol.2009.2. [DOI] [PubMed] [Google Scholar]
- 302.Takeuchi K, Choi YL, Togashi Y, et al. KIF5B-ALK, a novel fusion oncokinase identified by an immunohistochemistry-based diagnostic system for ALK-positive lung cancer. Clin Cancer Res. 2009;15:3143–3149. doi: 10.1158/1078-0432.CCR-08-3248. [DOI] [PubMed] [Google Scholar]
- 303.Yoshida A, Tsuta K, Watanabe SI, et al. Frequent ALK rearrangement and TTF-1/p63 co-expression in lung adenocarcinoma with signet-ring cell component. Lung Cancer. doi: 10.1016/j.lungcan.2010.09.013. In press. [DOI] [PubMed] [Google Scholar]
- 304.Jokoji R, Yamasaki T, Minami S, et al. Combination of morphological feature analysis and immunohistochemistry is useful for screening of EML4-ALK-positive lung adenocarcinoma. J Clin Pathol. 2010;63:1066–1070. doi: 10.1136/jcp.2010.081166. [DOI] [PubMed] [Google Scholar]
- 305.Inamura K, Takeuchi K, Togashi Y, et al. EML4-ALK fusion is linked to histological characteristics in a subset of lung cancers. J Thorac Oncol. 2008;3:13–17. doi: 10.1097/JTO.0b013e31815e8b60. [DOI] [PubMed] [Google Scholar]
- 306.Mino-Kenudson M, Chirieac LR, Law K, et al. A novel, highly sensitive antibody allows for the routine detection of ALK-rearranged lung adenocarcinomas by standard immunohistochemistry. Clin Cancer Res. 2010;16:1561–1571. doi: 10.1158/1078-0432.CCR-09-2845. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 307.Sakairi Y, Nakajima T, Yasufuku K, et al. EML4-ALK fusion gene assessment using metastatic lymph node samples obtained by endobronchial ultrasound-guided transbronchial needle aspiration. Clin Cancer Res. 2010;16:4938–4945. doi: 10.1158/1078-0432.CCR-10-0099. [DOI] [PubMed] [Google Scholar]
- 308.Boland JM, Erdogan S, Vasmatzis G, et al. Anaplastic lymphoma kinase immunoreactivity correlates with ALK gene rearrangement and transcriptional up-regulation in non-small cell lung carcinomas. Hum Pathol. 2009;40:1152–1158. doi: 10.1016/j.humpath.2009.01.012. [DOI] [PubMed] [Google Scholar]
- 309.Beer DG, Kardia SL, Huang CC, et al. Gene-expression profiles predict survival of patients with lung adenocarcinoma. Nat Med. 2002;8:816–824. doi: 10.1038/nm733. [DOI] [PubMed] [Google Scholar]
- 310.Borczuk AC, Kim HK, Yegen HA, et al. Lung adenocarcinoma global profiling identifies type II transforming growth factor-(beta) receptor as a repressor of invasiveness. Am J Respir Crit Care Med. 2005;172:729–737. doi: 10.1164/rccm.200504-615OC. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 311.Shibata T, Hanada S, Kokubu A, et al. Gene expression profiling of epidermal growth factor receptor/KRAS pathway activation in lung adenocarcinoma. Cancer Sci. 2007;98:985–991. doi: 10.1111/j.1349-7006.2007.00483.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 312.Berrar D, Sturgeon B, Bradbury I, et al. Survival trees for analyzing clinical outcome in lung adenocarcinomas based on gene expression profiles: identification of neogenin and diacylglycerol kinase alpha expression as critical factors. J Comput Biol. 2005;12:534–544. doi: 10.1089/cmb.2005.12.534. [DOI] [PubMed] [Google Scholar]
- 313.Bianchi F, Nuciforo P, Vecchi M, et al. Survival prediction of stage I lung adenocarcinomas by expression of 10 genes. J Clin Invest. 2007;117:3436–3444. doi: 10.1172/JCI32007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 314.Endoh H, Tomida S, Yatabe Y, et al. Prognostic model of pulmonary adenocarcinoma by expression profiling of eight genes as determined by quantitative real-time reverse transcriptase polymerase chain reaction. J Clin Oncol. 2004;22:811–819. doi: 10.1200/JCO.2004.04.109. [DOI] [PubMed] [Google Scholar]
- 315.Guo L, Ma Y, Ward R, et al. Constructing molecular classifiers for the accurate prognosis of lung adenocarcinoma. Clin Cancer Res. 2006;12:3344–3354. doi: 10.1158/1078-0432.CCR-05-2336. [DOI] [PubMed] [Google Scholar]
- 316.Hayes DN, Monti S, Parmigiani G, et al. Gene expression profiling reveals reproducible human lung adenocarcinoma subtypes in multiple independent patient cohorts. J Clin Oncol. 2006;24:5079–5090. doi: 10.1200/JCO.2005.05.1748. [DOI] [PubMed] [Google Scholar]
- 317.Inamura K, Shimoji T, Ninomiya H, et al. A metastatic signature in entire lung adenocarcinomas irrespective of morphological heterogeneity. Hum Pathol. 2007;38:702–709. doi: 10.1016/j.humpath.2006.11.019. [DOI] [PubMed] [Google Scholar]
- 318.Larsen JE, Pavey SJ, Passmore LH, et al. Gene expression signature predicts recurrence in lung adenocarcinoma. Clin Cancer Res. 2007;13:2946–2954. doi: 10.1158/1078-0432.CCR-06-2525. [DOI] [PubMed] [Google Scholar]
- 319.Liu H, Kho AT, Kohane IS, et al. Predicting survival within the lung cancer histopathological hierarchy using a multi-scale genomic model of development. PLoS Med. 2006;3:e232. doi: 10.1371/journal.pmed.0030232. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 320.Sun Z, Wigle DA, Yang P. Non-overlapping and non-cell-type-specific gene expression signatures predict lung cancer survival. J Clin Oncol. 2008;26:877–883. doi: 10.1200/JCO.2007.13.1516. [DOI] [PubMed] [Google Scholar]
- 321.Xi L, Lyons-Weiler J, Coello MC, et al. Prediction of lymph node metastasis by analysis of gene expression profiles in primary lung adenocarcinomas. Clin Cancer Res. 2005;11:4128–4135. doi: 10.1158/1078-0432.CCR-04-2525. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 322.Potti A, Mukherjee S, Petersen R, et al. A genomic strategy to refine prognosis in early-stage non-small-cell lung cancer. N Engl J Med. 2006;355:570–580. doi: 10.1056/NEJMoa060467. [DOI] [PubMed] [Google Scholar]
- 323.Chen HY, Yu SL, Chen CH, et al. A five-gene signature and clinical outcome in non-small-cell lung cancer. N Engl J Med. 2007;356:11–20. doi: 10.1056/NEJMoa060096. [DOI] [PubMed] [Google Scholar]
- 324.Chitale D, Gong Y, Taylor BS, et al. An integrated genomic analysis of lung cancer reveals loss of DUSP4 in EGFR-mutant tumors. Oncogene. 2009;28:2773–2783. doi: 10.1038/onc.2009.135. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 325.Tonon G, Brennan C, Protopopov A, et al. Common and contrasting genomic profiles among the major human lung cancer subtypes. Cold Spring Harb Symp Quant Biol. 2005;70:11–24. doi: 10.1101/sqb.2005.70.021. [DOI] [PubMed] [Google Scholar]
- 326.Aviel-Ronen S, Coe BP, Lau SK, et al. Genomic markers for malignant progression in pulmonary adenocarcinoma with bronchioloalveolar features. Proc Natl Acad Sci USA. 2008;105:10155–10160. doi: 10.1073/pnas.0709618105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 327.Chang JW, Liu HP, Hsieh MH, et al. Increased epidermal growth factor receptor (EGFR) gene copy number is strongly associated with EGFR mutations and adenocarcinoma in non-small cell lung cancers: a chromogenic in situ hybridization study of 182 patients. Lung Cancer. 2008;61:328–339. doi: 10.1016/j.lungcan.2008.01.009. [DOI] [PubMed] [Google Scholar]
- 328.Cappuzzo F, Hirsch FR, Rossi E, et al. Epidermal growth factor receptor gene and protein and gefitinib sensitivity in non-small-cell lung cancer. J Natl Cancer Inst. 2005;97:643–655. doi: 10.1093/jnci/dji112. [DOI] [PubMed] [Google Scholar]
- 329.Dacic S, Ionescu DN, Finkelstein S, et al. Patterns of allelic loss of synchronous adenocarcinomas of the lung. Am J Surg Pathol. 2005;29:897–902. doi: 10.1097/01.pas.0000164367.96379.66. [DOI] [PubMed] [Google Scholar]
- 330.Wang X, Wang M, MacLennan GT, et al. Evidence for common clonal origin of multifocal lung cancers. J Natl Cancer Inst. 2009;101:560–570. doi: 10.1093/jnci/djp054. [DOI] [PubMed] [Google Scholar]
- 331.Girard N, Ostrovnaya I, Lau C, et al. Genomic and mutational profiling to assess clonal relationships between multiple non-small cell lung cancers. Clin Cancer Res. 2009;15:5184–5190. doi: 10.1158/1078-0432.CCR-09-0594. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 332.van Rens MT, Eijken EJ, Elbers JR, et al. p53 mutation analysis for definite diagnosis of multiple primary lung carcinoma. Cancer. 2002;94:188–196. doi: 10.1002/cncr.10001. [DOI] [PubMed] [Google Scholar]
- 333.Matsuzoe D, Hideshima T, Ohshima K, et al. Discrimination of double primary lung cancer from intrapulmonary metastasis by p53 gene mutation. Br J Cancer. 1999;79:1549–1552. doi: 10.1038/sj.bjc.6690247. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 334.Wang X, Christiani DC, Mark EJ, et al. Carcinogen exposure p53 alteration, and K-ras mutation in synchronous multiple primary lung carcinoma. Cancer. 1999;85:1734–1739. [PubMed] [Google Scholar]
- 335.Lau DH, Yang B, Hu R, et al. Clonal origin of multiple lung cancers: K-ras and p53 mutations determined by nonradioisotopic single-strand conformation polymorphism analysis. Diagn Mol Pathol. 1997;6:179–184. doi: 10.1097/00019606-199708000-00001. [DOI] [PubMed] [Google Scholar]
- 336.Girard N, Deshpande C, Azzoli CG, et al. Use of epidermal growth factor receptor/Kirsten rat sarcoma 2 viral oncogene homolog mutation testing to define clonal relationships among multiple lung adenocarcinomas: comparison with clinical guidelines. Chest. 2010;137:46–52. doi: 10.1378/chest.09-0325. [DOI] [PubMed] [Google Scholar]
- 337.Nonami Y, Ohtuki Y, Sasaguri S. Study of the diagnostic difference between the clinical diagnostic criteria and results of immunohistochemical staining of multiple primary lung cancers. J Cardiovasc Surg (Torino) 2003;44:661–665. [PubMed] [Google Scholar]
- 338.Vansteenkiste JF, De Belie B, Deneffe GJ, et al. Practical approach to patients presenting with multiple synchronous suspect lung lesions: a reflection on the current TNM classification based on 54 cases with complete follow-up. Lung Cancer. 2001;34:169–175. doi: 10.1016/s0169-5002(01)00245-8. [DOI] [PubMed] [Google Scholar]
- 339.Yoshino I, Nakanishi R, Osaki T, et al. Postoperative prognosis in patients with non-small cell lung cancer with synchronous ipsilateral intrapulmonary metastasis. Ann Thorac Surg. 1997;64:809–813. doi: 10.1016/s0003-4975(97)00281-6. [DOI] [PubMed] [Google Scholar]
- 340.Chung JH, Choe G, Jheon S, et al. Epidermal growth factor receptor mutation and pathologic-radiologic correlation between multiple lung nodules with ground-glass opacity differentiates multicentric origin from intrapulmonary spread. J Thorac Oncol. 2009;4:1490–1495. doi: 10.1097/JTO.0b013e3181bc9731. [DOI] [PubMed] [Google Scholar]
- 341.Balak MN, Gong Y, Riely GJ, et al. Novel D761Y and common secondary T790M mutations in epidermal growth factor receptor mutant lung adenocarcinomas with acquired resistance to kinase inhibitors. Clin Cancer Res. 2006;12:6494–6501. doi: 10.1158/1078-0432.CCR-06-1570. [DOI] [PubMed] [Google Scholar]
- 342.Jackman DM, Holmes AJ, Lindeman N, et al. Response and resistance in a non-small-cell lung cancer patient with an epidermal growth factor receptor mutation and leptomeningeal metastases treated with high-dose gefitinib. J Clin Oncol. 2006;24:4517–4520. doi: 10.1200/JCO.2006.06.6126. [DOI] [PubMed] [Google Scholar]
- 343.Schmid K, Oehl N, Wrba F, et al. EGFR/KRAS/BRAF mutations in primary lung adenocarcinomas and corresponding locoregional lymph node metastases. Clin Cancer Res. 2009;15:4554–4560. doi: 10.1158/1078-0432.CCR-09-0089. [DOI] [PubMed] [Google Scholar]
- 344.Monaco SE, Nikiforova MN, Cieply K, et al. A comparison of EGFR and KRAS status in primary lung carcinoma and matched metastases. Hum Pathol. 2010;41:94–102. doi: 10.1016/j.humpath.2009.06.019. [DOI] [PubMed] [Google Scholar]
- 345.Meert AP, Martin B, Delmotte P, et al. The role of EGF-R expression on patient survival in lung cancer: a systematic review with meta-analysis. Eur Respir J. 2002;20:975–981. doi: 10.1183/09031936.02.00296502. [DOI] [PubMed] [Google Scholar]
- 346.Berghmans T, Paesmans M, Mascaux C, et al. Thyroid transcription factor 1—a new prognostic factor in lung cancer: a meta-analysis. Ann Oncol. 2006;17:1673–1676. doi: 10.1093/annonc/mdl287. [DOI] [PubMed] [Google Scholar]
- 347.Mascaux C, Iannino N, Martin B, et al. The role of RAS oncogene in survival of patients with lung cancer: a systematic review of the literature with meta-analysis. Br J Cancer. 2005;92:131–139. doi: 10.1038/sj.bjc.6602258. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 348.Nakamura H, Kawasaki N, Taguchi M, et al. Association of HER-2 overexpression with prognosis in nonsmall cell lung carcinoma: a meta-analysis. Cancer. 2005;103:1865–1873. doi: 10.1002/cncr.20957. [DOI] [PubMed] [Google Scholar]
- 349.Mitsudomi T, Hamajima N, Ogawa M, et al. Prognostic significance of p53 alterations in patients with non-small cell lung cancer: a meta-analysis. Clin Cancer Res. 2000;6:4055–4063. [PubMed] [Google Scholar]
- 350.Steels E, Paesmans M, Berghmans T, et al. Role of p53 as a prognostic factor for survival in lung cancer: a systematic review of the literature with a meta-analysis. Eur Respir J. 2001;18:705–719. doi: 10.1183/09031936.01.00062201. [DOI] [PubMed] [Google Scholar]
- 351.Martin B, Paesmans M, Mascaux C, et al. Ki-67 expression and patients survival in lung cancer: systematic review of the literature with meta-analysis. Br J Cancer. 2004;91:2018–2025. doi: 10.1038/sj.bjc.6602233. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 352.Martin B, Paesmans M, Berghmans T, et al. Role of Bcl-2 as a prognostic factor for survival in lung cancer: a systematic review of the literature with meta-analysis. Br J Cancer. 2003;89:55–64. doi: 10.1038/sj.bjc.6601095. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 353.Mascaux C, Martin B, Paesmans M, et al. Has Cox-2 a prognostic role in non-small-cell lung cancer? A systematic review of the literature with meta-analysis of the survival results. Br J Cancer. 2006;95:139–145. doi: 10.1038/sj.bjc.6603226. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 354.Marks JL, Broderick S, Zhou Q, et al. Prognostic and therapeutic implications of EGFR and KRAS mutations in resected lung adenocarcinoma. J Thorac Oncol. 2008;3:111–116. doi: 10.1097/JTO.0b013e318160c607. [DOI] [PubMed] [Google Scholar]
- 355.Kosaka T, Yatabe Y, Onozato R, et al. Prognostic implication of EGFR, KRAS and TP53 gene mutations in a large cohort of Japanese patients with surgically treated lung adenocarcinoma. J Thorac Oncol. 2009;4:22–29. doi: 10.1097/JTO.0b013e3181914111. [DOI] [PubMed] [Google Scholar]
- 356.Yanaihara N, Caplen N, Bowman E, et al. Unique microRNA molecular profiles in lung cancer diagnosis and prognosis. Cancer Cell. 2006;9:189–198. doi: 10.1016/j.ccr.2006.01.025. [DOI] [PubMed] [Google Scholar]
- 357.Raponi M, Dossey L, Jatkoe T, et al. MicroRNA classifiers for predicting prognosis of squamous cell lung cancer. Cancer Res. 2009;69:5776–5783. doi: 10.1158/0008-5472.CAN-09-0587. [DOI] [PubMed] [Google Scholar]
- 358.Hansell DM, Bankier AA, MacMahon H, et al. Fleischner Society: glossary of terms for thoracic imaging. Radiology. 2008;246:697–722. doi: 10.1148/radiol.2462070712. [DOI] [PubMed] [Google Scholar]
- 359.Godoy MC, Naidich DP. Subsolid pulmonary nodules and the spectrum of peripheral adenocarcinomas of the lung: recommended interim guidelines for assessment and management. Radiology. 2009;253:606–622. doi: 10.1148/radiol.2533090179. [DOI] [PubMed] [Google Scholar]
- 360.Lee HY, Goo JM, Lee HJ, et al. Usefulness of concurrent reading using thin-section and thick-section CT images in subcentimetre solitary pulmonary nodules. Clin Radiol. 2009;64:127–132. doi: 10.1016/j.crad.2008.09.003. [DOI] [PubMed] [Google Scholar]
- 361.Takashima S, Sone S, Li F, et al. Small solitary pulmonary nodules (< or = 1 cm) detected at population-based CT screening for lung cancer: reliable high-resolution CT features of benign lesions. AJR Am J Roentgenol. 2003;180:955–964. doi: 10.2214/ajr.180.4.1800955. [DOI] [PubMed] [Google Scholar]
- 362.Ishikawa H, Koizumi N, Morita T, et al. Ultrasmall pulmonary opacities on multidetector-row high-resolution computed tomography: a prospective radiologic-pathologic examination. J Comput Assist Tomogr. 2005;29:621–625. doi: 10.1097/01.rct.0000172672.09564.8c. [DOI] [PubMed] [Google Scholar]
- 363.Kishi K, Homma S, Kurosaki A, et al. Small lung tumors with the size of 1cm or less in diameter: clinical, radiological, and histopathological characteristics. Lung Cancer. 2004;44:43–51. doi: 10.1016/j.lungcan.2003.09.024. [DOI] [PubMed] [Google Scholar]
- 364.Kim HY, Shim YM, Lee KS, et al. Persistent pulmonary nodular ground-glass opacity at thin-section CT: histopathologic comparisons. Radiology. 2007;245:267–275. doi: 10.1148/radiol.2451061682. [DOI] [PubMed] [Google Scholar]
- 365.Kim TJ, Goo JM, Lee KW, et al. Clinical, pathological and thin-section CT features of persistent multiple ground-glass opacity nodules: comparison with solitary ground-glass opacity nodule. Lung Cancer. 2009;64:171–178. doi: 10.1016/j.lungcan.2008.08.002. [DOI] [PubMed] [Google Scholar]
- 366.Ikeda K, Awai K, Mori T, et al. Differential diagnosis of ground-glass opacity nodules: CT number analysis by three-dimensional computerized quantification. Chest. 2007;132:984–990. doi: 10.1378/chest.07-0793. [DOI] [PubMed] [Google Scholar]
- 367.Choi JA, Kim JH, Hong KT, et al. CT bronchus sign in malignant solitary pulmonary lesions: value in the prediction of cell type. Eur Radiol. 2000;10:1304–1309. doi: 10.1007/s003300000315. [DOI] [PubMed] [Google Scholar]
- 368.Takashima S, Maruyama Y, Hasegawa M, et al. CT findings and progression of small peripheral lung neoplasms having a replacement growth pattern. AJR Am J Roentgenol. 2003;180:817–826. doi: 10.2214/ajr.180.3.1800817. [DOI] [PubMed] [Google Scholar]
- 369.Gould MK, Fletcher J, Iannettoni MD, et al. Evaluation of patients with pulmonary nodules: when is it lung cancer?: ACCP evidence-based clinical practice guidelines (2nd edition) Chest. 2007;132:108S–130S. doi: 10.1378/chest.07-1353. [DOI] [PubMed] [Google Scholar]
- 370.Nakazono T, Sakao Y, Yamaguchi K, et al. Subtypes of peripheral adenocarcinoma of the lung: differentiation by thin-section CT. Eur Radiol. 2005;15:1563–1568. doi: 10.1007/s00330-004-2595-7. [DOI] [PubMed] [Google Scholar]
- 371.Zwirewich CV, Vedal S, Miller RR, et al. Solitary pulmonary nodule: high-resolution CT and radiologic-pathologic correlation. Radiology. 1991;179:469–476. doi: 10.1148/radiology.179.2.2014294. [DOI] [PubMed] [Google Scholar]
- 372.Yang ZG, Sone S, Takashima S, et al. High-resolution CT analysis of small peripheral lung adenocarcinomas revealed on screening helical CT. AJR Am J Roentgenol. 2001;176:1399–1407. doi: 10.2214/ajr.176.6.1761399. [DOI] [PubMed] [Google Scholar]
- 373.Tateishi U, Uno H, Yonemori K, et al. Prediction of lung adenocarcinoma without vessel invasion: a CT scan volumetric analysis. Chest. 2005;128:3276–3283. doi: 10.1378/chest.128.5.3276. [DOI] [PubMed] [Google Scholar]
- 374.Kojima Y, Saito H, Sakuma Y, et al. Correlations of thin-section computed tomographic, histopathological, and clinical findings of adenocarcinoma with a bubblelike appearance. J Comput Assist Tomogr. 2010;34:413–417. doi: 10.1097/RCT.0b013e3181d275b6. [DOI] [PubMed] [Google Scholar]
- 375.Yoshino I, Nakanishi R, Kodate M, et al. Pleural retraction and intra-tumoral air-bronchogram as prognostic factors for stage I pulmonary adenocarcinoma following complete resection. Int Surg. 2000;85:105–112. [PubMed] [Google Scholar]
- 376.Kondo T, Yamada K, Noda K, et al. Radiologic-prognostic correlation in patients with small pulmonary adenocarcinomas. Lung Cancer. 2002;36:49–57. doi: 10.1016/s0169-5002(01)00448-2. [DOI] [PubMed] [Google Scholar]
- 377.Sakao Y, Nakazono T, Sakuragi T, et al. Predictive factors for survival in surgically resected clinical IA peripheral adenocarcinoma of the lung. Ann Thorac Surg. 2004;77:1157–1161. doi: 10.1016/j.athoracsur.2003.09.055. [DOI] [PubMed] [Google Scholar]
- 378.Kuriyama K, Seto M, Kasugai T, et al. Ground-glass opacity on thin-section CT: value in differentiating subtypes of adenocarcinoma of the lung. AJR Am J Roentgenol. 1999;173:465–469. doi: 10.2214/ajr.173.2.10430155. [DOI] [PubMed] [Google Scholar]
- 379.Castro CY, Coffey DM, Medeiros LJ, et al. Prognostic significance of percentage of bronchioloalveolar pattern in adenocarcinomas of the lung. Ann Diagn Pathol. 2001;5:274–284. doi: 10.1053/adpa.2001.27915. [DOI] [PubMed] [Google Scholar]
- 380.Hashizume T, Yamada K, Okamoto N, et al. Prognostic significance of thin-section CT scan findings in small-sized lung adenocarcinoma. Chest. 2008;133:441–447. doi: 10.1378/chest.07-1533. [DOI] [PubMed] [Google Scholar]
- 381.Dong B, Sato M, Sagawa M, et al. Computed tomographic image comparison between mediastinal and lung windows provides possible prognostic information in patients with small peripheral lung adenocarcinoma. J Thorac Cardiovasc Surg. 2002;124:1014–1020. doi: 10.1067/mtc.2002.125647. [DOI] [PubMed] [Google Scholar]
- 382.Matsuguma H, Yokoi K, Anraku M, et al. Proportion of ground-glass opacity on high-resolution computed tomography in clinical T1 N0 M0 adenocarcinoma of the lung: a predictor of lymph node metastasis. J Thorac Cardiovasc Surg. 2002;124:278–284. doi: 10.1067/mtc.2002.122298. [DOI] [PubMed] [Google Scholar]
- 383.Ohde Y, Nagai K, Yoshida J, et al. The proportion of consolidation to ground-glass opacity on high resolution CT is a good predictor for distinguishing the population of non-invasive peripheral adenocarcinoma. Lung Cancer. 2003;42:303–310. doi: 10.1016/j.lungcan.2003.07.001. [DOI] [PubMed] [Google Scholar]
- 384.Okada M, Nishio W, Sakamoto T, et al. Correlation between computed tomographic findings, bronchioloalveolar carcinoma component, and biologic behavior of small-sized lung adenocarcinomas. J Thorac Cardiovasc Surg. 2004;127:857–861. doi: 10.1016/j.jtcvs.2003.08.048. [DOI] [PubMed] [Google Scholar]
- 385.Sakao Y, Nakazono T, Tomimitsu S, et al. Lung adenocarcinoma can be subtyped according to tumor dimension by computed tomography mediastinal-window setting. Additional size criteria for clinical T1 adenocarcinoma. Eur J Cardiothorac Surg. 2004;26:1211–1215. doi: 10.1016/j.ejcts.2004.08.021. [DOI] [PubMed] [Google Scholar]
- 386.Seki N, Sawada S, Nakata M, et al. Lung cancer with localized ground-glass attenuation represents early-stage adenocarcinoma in nonsmokers. J Thorac Oncol. 2008;3:483–490. doi: 10.1097/JTO.0b013e31816a4994. [DOI] [PubMed] [Google Scholar]
- 387.Takashima S, Maruyama Y, Hasegawa M, et al. High-resolution CT features: prognostic significance in peripheral lung adenocarcinoma with bronchioloalveolar carcinoma components. Respiration. 2003;70:36–42. doi: 10.1159/000068410. [DOI] [PubMed] [Google Scholar]
- 388.Nishio R, Akata S, Saito K, et al. The ratio of the maximum high attenuation area dimension to the maximum tumor dimension may be an index of the presence of lymph node metastasis in lung adenocarcinomas 3 cm or smaller on high-resolution computed tomography. J Thorac Oncol. 2007;2:29–33. [PubMed] [Google Scholar]
- 389.Shim HS, Park IK, Lee CY, et al. Prognostic significance of visceral pleural invasion in the forthcoming (seventh) edition of TNM classification for lung cancer. Lung Cancer. 2009;65:161–165. doi: 10.1016/j.lungcan.2008.11.008. [DOI] [PubMed] [Google Scholar]
- 390.Ikehara M, Saito H, Kondo T, et al. Comparison of thin-section CT and pathological findings in small solid-density type pulmonary adenocarcinoma: prognostic factors from CT findings. Eur J Radiol. doi: 10.1016/j.ejrad.2010.09.026. In press. [DOI] [PubMed] [Google Scholar]
- 391.Gaeta M, Vinci S, Minutoli F, et al. CT and MRI findings of mucin-containing tumors and pseudotumors of the thorax: pictorial review. Eur Radiol. 2002;12:181–189. doi: 10.1007/s003300100934. [DOI] [PubMed] [Google Scholar]
- 392.Nakata M, Sawada S, Saeki H, et al. Prospective study of thoracoscopic limited resection for ground-glass opacity selected by computed tomography. Ann Thorac Surg. 2003;75:1601–1605. doi: 10.1016/s0003-4975(02)04815-4. discussion 5–6. [DOI] [PubMed] [Google Scholar]
- 393.Takashima S, Maruyama Y, Hasegawa M, et al. Prognostic significance of high-resolution CT findings in small peripheral adenocarcinoma of the lung: a retrospective study on 64 patients. Lung Cancer. 2002;36:289–295. doi: 10.1016/s0169-5002(01)00489-5. [DOI] [PubMed] [Google Scholar]
- 394.Hiramatsu M, Inagaki T, Matsui Y, et al. Pulmonary ground-glass opacity (GGO) lesions-large size and a history of lung cancer are risk factors for growth. J Thorac Oncol. 2008;3:1245–1250. doi: 10.1097/JTO.0b013e318189f526. [DOI] [PubMed] [Google Scholar]
- 395.Austin JHM, Mujoomdar A, Powell CA, et al. Carcinoma of the lung and metastatic disease of the central nervous system. Am J Respir Crit Care Med. 2008;178:1090. doi: 10.1164/ajrccm.178.10.1090. [DOI] [PubMed] [Google Scholar]
- 396.Mujoomdar A, Austin JHM, Malhotra R, et al. Clinical predictors of metastatic disease to the brain from non-small cell lung carcinoma: primary tumor size, cell type, and lymph node metastases. Radiology. 2007;242:882–888. doi: 10.1148/radiol.2423051707. [DOI] [PubMed] [Google Scholar]
- 397.MacMahon H, Austin JHM, Gamsu G, et al. Guidelines for management of small pulmonary nodules detected on CT scans: a statement from the Fleischner Society. Radiology. 2005;237:395–400. doi: 10.1148/radiol.2372041887. [DOI] [PubMed] [Google Scholar]
- 398.Eisenberg RL, Bankier AA, Boiselle PM. Compliance with Fleischner Society guidelines for management of small lung nodules: a survey of 834 radiologists. Radiology. 2010;255:218–224. doi: 10.1148/radiol.09091556. [DOI] [PubMed] [Google Scholar]
- 399.MacMahon H. Compliance with Fleischner Society guidelines for management of lung nodules: lessons and opportunities. Radiology. 2010;255:14–15. doi: 10.1148/radiol.10092382. [DOI] [PubMed] [Google Scholar]
- 400.Zhao B, James LP, Moskowitz CS, et al. Evaluating variability in tumor measurements from same-day repeat CT scans of patients with non-small cell lung cancer. Radiology. 2009;252:263–272. doi: 10.1148/radiol.2522081593. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 401.Ravenel JG, Leue WM, Nietert PJ, et al. Pulmonary nodule volume: effects of reconstruction parameters on automated measurements—a phantom study. Radiology. 2008;247:400–408. doi: 10.1148/radiol.2472070868. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 402.Jennings SG, Winer-Muram HT, Tarver RD, et al. Lung tumor growth: assessment with CT–comparison of diameter and cross-sectional area with volume measurements. Radiology. 2004;231:866–871. doi: 10.1148/radiol.2313030715. [DOI] [PubMed] [Google Scholar]
- 403.Winer-Muram HT, Jennings SG, Meyer CA, et al. Effect of varying CT section width on volumetric measurement of lung tumors and application of compensatory equations. Radiology. 2003;229:184–194. doi: 10.1148/radiol.2291020859. [DOI] [PubMed] [Google Scholar]
- 404.Yankelevitz DF, Reeves AP, Kostis WJ, et al. Small pulmonary nodules: volumetrically determined growth rates based on CT evaluation. Radiology. 2000;217:251–256. doi: 10.1148/radiology.217.1.r00oc33251. [DOI] [PubMed] [Google Scholar]
- 405.de Hoop B, Gietema H, van de Vorst S, et al. Pulmonary ground-glass nodules: increase in mass as an early indicator of growth. Radiology. 2010;255:199–206. doi: 10.1148/radiol.09090571. [DOI] [PubMed] [Google Scholar]
- 406.Nakata M, Sawada S, Yamashita M, et al. Surgical treatments for multiple primary adenocarcinoma of the lung. Ann Thorac Surg. 2004;78:1194–1199. doi: 10.1016/j.athoracsur.2004.03.102. [DOI] [PubMed] [Google Scholar]
- 407.Zwirewich CV, Miller RR, Muller NL. Multicentric adenocarcinoma of the lung: CT-pathologic correlation. Radiology. 1990;176:185–190. doi: 10.1148/radiology.176.1.2162069. [DOI] [PubMed] [Google Scholar]
- 408.Park CM, Goo JM, Kim TJ, et al. Pulmonary nodular ground-glass opacities in patients with extrapulmonary cancers: what is their clinical significance and how can we determine whether they are malignant or benign lesions? Chest. 2008;133:1402–1409. doi: 10.1378/chest.07-2568. [DOI] [PubMed] [Google Scholar]
- 409.Okada M, Tauchi S, Iwanaga K, et al. Associations among bronchioloalveolar carcinoma components, positron emission tomographic and computed tomographic findings, and malignant behavior in small lung adenocarcinomas. J Thorac Cardiovasc Surg. 2007;133:1448–1454. doi: 10.1016/j.jtcvs.2007.02.023. [DOI] [PubMed] [Google Scholar]
- 410.Higashi K, Ueda Y, Seki H, et al. Fluorine-18-FDG PET imaging is negative in bronchioloalveolar lung carcinoma. J Nucl Med. 1998;39:1016–1020. [PubMed] [Google Scholar]
- 411.Higashi K, Ueda Y, Yagishita M, et al. FDG PET measurement of the proliferative potential of non-small cell lung cancer. J Nucl Med. 2000;41:85–92. [PubMed] [Google Scholar]
- 412.Higashi K, Ueda Y, Ayabe K, et al. FDG PET in the evaluation of the aggressiveness of pulmonary adenocarcinoma: correlation with histopathological features. Nucl Med Commun. 2000;21:707–714. doi: 10.1097/00006231-200008000-00002. [DOI] [PubMed] [Google Scholar]
- 413.Ohtsuka T, Nomori H, Watanabe K, et al. Prognostic significance of [(18)F]fluorodeoxyglucose uptake on positron emission tomography in patients with pathologic stage I lung adenocarcinoma. Cancer. 2006;107:2468–2473. doi: 10.1002/cncr.22268. [DOI] [PubMed] [Google Scholar]
- 414.Raz DJ, Odisho AY, Franc BL, et al. Tumor fluoro-2-deoxy-D-glucose avidity on positron emission tomographic scan predicts mortality in patients with early-stage pure and mixed bronchioloalveolar carcinoma. J Thorac Cardiovasc Surg. 2006;132:1189–1195. doi: 10.1016/j.jtcvs.2006.06.033. [DOI] [PubMed] [Google Scholar]
- 415.Sagawa M, Higashi K, Sugita M, et al. Fluorodeoxyglucose uptake correlates with the growth pattern of small peripheral pulmonary adenocarcinoma. Surg Today. 2006;36:230–234. doi: 10.1007/s00595-005-3123-3. [DOI] [PubMed] [Google Scholar]
- 416.Pastorino U, Landoni C, Marchiano A, et al. Fluorodeoxyglucose uptake measured by positron emission tomography and standardized uptake value predicts long-term survival of CT screening detected lung cancer in heavy smokers. J Thorac Oncol. 2009;4:1352–1356. doi: 10.1097/JTO.0b013e3181bbf1dc. [DOI] [PubMed] [Google Scholar]
- 417.Nakayama H, Okumura S, Daisaki H, et al. Value of integrated positron emission tomography revised using a phantom study to evaluate malignancy grade of lung adenocarcinoma: a multicenter study. Cancer. 2010;116:3170–3177. doi: 10.1002/cncr.25244. [DOI] [PubMed] [Google Scholar]
- 418.Um SW, Kim H, Koh WJ, et al. Prognostic value of 18F-FDG uptake on positron emission tomography in patients with pathologic stage I non-small cell lung cancer. J Thorac Oncol. 2009;4:1331–1336. doi: 10.1097/JTO.0b013e3181b6be3e. [DOI] [PubMed] [Google Scholar]
- 419.Berghmans T, Dusart M, Paesmans M, et al. Primary tumor standardized uptake value (SUVmax) measured on fluorodeoxyglucose positron emission tomography (FDG-PET) is of prognostic value for survival in non-small cell lung cancer (NSCLC): a systematic review and metaanalysis (MA) by the European Lung Cancer Working Party for the IASLC Lung Cancer Staging Project. J Thorac Oncol. 2008;3:6–12. doi: 10.1097/JTO.0b013e31815e6d6b. [DOI] [PubMed] [Google Scholar]
- 420.Birchard KR, Hoang JK, Herndon JE, Jr, et al. Early changes in tumor size in patients treated for advanced stage nonsmall cell lung cancer do not correlate with survival. Cancer. 2009;115:581–586. doi: 10.1002/cncr.24060. [DOI] [PubMed] [Google Scholar]
- 421.Sohn HJ, Yang YJ, Ryu JS, et al. [18F]Fluorothymidine positron emission tomography before and 7 days after gefitinib treatment predicts response in patients with advanced adenocarcinoma of the lung. Clin Cancer Res. 2008;14:7423–7429. doi: 10.1158/1078-0432.CCR-08-0312. [DOI] [PubMed] [Google Scholar]
- 422.Cloran FJ, Banks KP, Song WS, et al. Limitations of dual time point PET in the assessment of lung nodules with low FDG avidity. Lung Cancer. 2010;68:66–71. doi: 10.1016/j.lungcan.2009.05.013. [DOI] [PubMed] [Google Scholar]
- 423.Ohno Y, Hatabu H, Takenaka D, et al. Dynamic MR imaging: value of differentiating subtypes of peripheral small adenocarcinoma of the lung. Eur J Radiol. 2004;52:144–150. doi: 10.1016/j.ejrad.2004.01.015. [DOI] [PubMed] [Google Scholar]
- 424.van Klaveren RJ, Oudkerk M, Prokop M, et al. Management of lung nodules detected by volume CT scanning. N Engl J Med. 2009;361:2221–2229. doi: 10.1056/NEJMoa0906085. [DOI] [PubMed] [Google Scholar]
- 425.Oda S, Awai K, Murao K, et al. Computer-aided volumetry of pulmonary nodules exhibiting ground-glass opacity at MDCT. AJR Am J Roentgenol. 2010;194:398–406. doi: 10.2214/AJR.09.2583. [DOI] [PubMed] [Google Scholar]
- 426.Henschke CI, McCauley DI, Yankelevitz DF, et al. Early Lung Cancer Action Project: overall design and findings from baseline screening. Lancet. 1999;354:99–105. doi: 10.1016/S0140-6736(99)06093-6. [DOI] [PubMed] [Google Scholar]
- 427.Henschke CI, Naidich DP, Yankelevitz DF, et al. Early lung cancer action project: initial findings on repeat screenings. Cancer. 2001;92:153–159. doi: 10.1002/1097-0142(20010701)92:1<153::aid-cncr1303>3.0.co;2-s. [DOI] [PubMed] [Google Scholar]
- 428.Lindell RM, Hartman TE, Swensen SJ, et al. Five-year lung cancer screening experience: CT appearance, growth rate, location, and histologic features of 61 lung cancers. Radiology. 2007;242:555–562. doi: 10.1148/radiol.2422052090. [DOI] [PubMed] [Google Scholar]
- 429.Hasegawa M, Sone S, Takashima S, et al. Growth rate of small lung cancers detected on mass CT screening. Br J Radiol. 2000;73:1252–1259. doi: 10.1259/bjr.73.876.11205667. [DOI] [PubMed] [Google Scholar]
- 430.Henschke CI, Yankelevitz DF, Libby DM, et al. Survival of patients with stage I lung cancer detected on CT screening. N Engl J Med. 2006;355:1763–1771. doi: 10.1056/NEJMoa060476. [DOI] [PubMed] [Google Scholar]
- 431.Kakinuma R, Ohmatsu H, Kaneko M, et al. Progression of focal pure ground-glass opacity detected by low-dose helical computed tomography screening for lung cancer. J Comput Assist Tomogr. 2004;28:17–23. doi: 10.1097/00004728-200401000-00003. [DOI] [PubMed] [Google Scholar]
- 432.Sone S, Nakayama T, Honda T, et al. Long-term follow-up study of a population-based 1996–1998 mass screening programme for lung cancer using mobile low-dose spiral computed tomography. Lung Cancer. 2007;58:329–341. doi: 10.1016/j.lungcan.2007.06.022. [DOI] [PubMed] [Google Scholar]
- 433.Pelosi G, Sonzogni A, Veronesi G, et al. Pathologic and molecular features of screening low-dose computed tomography (LDCT)-detected lung cancer: a baseline and 2-year repeat study. Lung Cancer. 2008;62:202–214. doi: 10.1016/j.lungcan.2008.03.012. [DOI] [PubMed] [Google Scholar]
- 434.Wang JC, Sone S, Feng L, et al. Rapidly growing small peripheral lung cancers detected by screening CT: correlation between radiological appearance and pathological features. Br J Radiol. 2000;73:930–937. doi: 10.1259/bjr.73.873.11064644. [DOI] [PubMed] [Google Scholar]
- 435.Infante M, Cavuto S, Lutman FR, et al. A randomized study of lung cancer screening with spiral computed tomography: three-year results from the DANTE trial. Am J Respir Crit Care Med. 2009;180:445–453. doi: 10.1164/rccm.200901-0076OC. [DOI] [PubMed] [Google Scholar]
- 436.Bepler G. Are we coming full circle for lung cancer screening a second time? Am J Respir Crit Care Med. 2009;180:384–385. doi: 10.1164/rccm.200906-0977ED. [DOI] [PubMed] [Google Scholar]
- 437.McMahon PM, Kong CY, Johnson BE, et al. Estimating long-term effectiveness of lung cancer screening in the Mayo CT screening study. Radiology. 2008;248:278–287. doi: 10.1148/radiol.2481071446. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 438.McMahon PM, Kong CY, Weinstein MC, et al. Adopting helical CT screening for lung cancer: potential health consequences during a 15-year period. Cancer. 2008;113:3440–3449. doi: 10.1002/cncr.23962. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 439.Gatsonis CA. The National Lung Screening Trial: overview and study design. Radiology. 2011;258:243–253. doi: 10.1148/radiol.10091808. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 440.Park EA, Lee HJ, Kim YT, et al. EGFR gene copy number in adenocarcinoma of the lung by FISH analysis: investigation of significantly related factors on CT, FDG-PET, and histopathology. Lung Cancer. 2009;64:179–186. doi: 10.1016/j.lungcan.2008.08.003. [DOI] [PubMed] [Google Scholar]
- 441.Yano M, Sasaki H, Kobayashi Y, et al. Epidermal growth factor receptor gene mutation and computed tomographic findings in peripheral pulmonary adenocarcinoma. J Thorac Oncol. 2006;1:413–416. [PubMed] [Google Scholar]
- 442.Chantranuwat C, Sriuranpong V, Huapai N, et al. Histopathologic characteristics of pulmonary adenocarcinomas with and without EGFR mutation. J Med Assoc Thai. 2005;88(Suppl 4):S322–S329. [PubMed] [Google Scholar]
- 443.Huang CT, Yen RF, Cheng MF, et al. Correlation of F-18 fluorodeoxyglucose-positron emission tomography maximal standardized uptake value and EGFR mutations in advanced lung adenocarcinoma. Med Oncol. 2010;27:9–15. doi: 10.1007/s12032-008-9160-1. [DOI] [PubMed] [Google Scholar]
- 444.Watanabe K, Nomori H, Ohtsuka T, et al. [F-18]Fluorodeoxyglucose positron emission tomography can predict pathological tumor stage and proliferative activity determined by Ki-67 in clinical stage IA lung adenocarcinomas. Jpn J Clin Oncol. 2006;36:403–409. doi: 10.1093/jjco/hyl043. [DOI] [PubMed] [Google Scholar]
- 445.Vesselle H, Salskov A, Turcotte E, et al. Relationship between non-small cell lung cancer FDG uptake at PET, tumor histology, and Ki-67 proliferation index. J Thorac Oncol. 2008;3:971–978. doi: 10.1097/JTO.0b013e31818307a7. [DOI] [PubMed] [Google Scholar]
- 446.Schuchert MJ, Pettiford BL, Keeley S, et al. Anatomic segmentectomy in the treatment of stage I non-small cell lung cancer. Ann Thorac Surg. 2007;84:926–932. doi: 10.1016/j.athoracsur.2007.05.007. [DOI] [PubMed] [Google Scholar]
- 447.Shapiro M, Weiser TS, Wisnivesky JP, et al. Thoracoscopic segmentectomy compares favorably with thoracoscopic lobectomy for patients with small stage I lung cancer. J Thorac Cardiovasc Surg. 2009;137:1388–1393. doi: 10.1016/j.jtcvs.2009.02.009. [DOI] [PubMed] [Google Scholar]
- 448.Yan TD, Black D, Bannon PG, et al. Systematic review and meta-analysis of randomized and nonrandomized trials on safety and efficacy of video-assisted thoracic surgery lobectomy for early-stage non-small-cell lung cancer. J Clin Oncol. 2009;27:2553–2562. doi: 10.1200/JCO.2008.18.2733. [DOI] [PubMed] [Google Scholar]
- 449.Watanabe T, Okada A, Imakiire T, et al. Intentional limited resection for small peripheral lung cancer based on intraoperative pathologic exploration. Jpn J Thorac Cardiovasc Surg. 2005;53:29–35. doi: 10.1007/s11748-005-1005-7. [DOI] [PubMed] [Google Scholar]
- 450.Higashiyama M, Kodama K, Takami K, et al. Intraoperative lavage cytologic analysis of surgical margins in patients undergoing limited surgery for lung cancer. J Thorac Cardiovasc Surg. 2003;125:101–107. doi: 10.1067/mtc.2003.92. [DOI] [PubMed] [Google Scholar]
- 451.Utsumi T, Sawabata N, Inoue M, et al. Optimal sampling methods for margin cytology examination following lung excision. Interact Cardiovasc Thorac Surg. 2010;10:434–436. doi: 10.1510/icvts.2009.212142. [DOI] [PubMed] [Google Scholar]
- 452.Asamura H, Suzuki K, Watanabe S, et al. A clinicopathological study of resected subcentimeter lung cancers: a favorable prognosis for ground glass opacity lesions. Ann Thorac Surg. 2003;76:1016–1022. doi: 10.1016/s0003-4975(03)00835-x. [DOI] [PubMed] [Google Scholar]
- 453.Ginsberg RJ, Rubinstein LV. Randomized trial of lobectomy versus limited resection for T1 N0 non-small cell lung cancer. Lung Cancer Study Group. Ann Thorac Surg. 1995;60:615–622. doi: 10.1016/0003-4975(95)00537-u. [DOI] [PubMed] [Google Scholar]
- 454.Miller DL, Rowland CM, Deschamps C, et al. Surgical treatment of non-small cell lung cancer 1 cm or less in diameter. Ann Thorac Surg. 2002;73:1545–1550. doi: 10.1016/s0003-4975(02)03525-7. discussion 50–51. [DOI] [PubMed] [Google Scholar]
- 455.Rami-Porta R, Wittekind C, Goldstraw P. Complete resection in lung cancer surgery: proposed definition. Lung Cancer. 2005;49:25–33. doi: 10.1016/j.lungcan.2005.01.001. [DOI] [PubMed] [Google Scholar]
- 456.Ishiguro F, Matsuo K, Fukui T, et al. Effect of selective lymph node dissection based on patterns of lobe-specific lymph node metastases on patient outcome in patients with resectable non-small cell lung cancer: a large-scale retrospective cohort study applying a propensity score. J Thorac Cardiovasc Surg. 2010;139:1001–1006. doi: 10.1016/j.jtcvs.2009.07.024. [DOI] [PubMed] [Google Scholar]
- 457.Darling GE, Allen MS, Landreneau RJ, et al. Randomized trial of mediastinal lymph node sampling versus complete lymphadenectomy during pulmonary resection in the patient with N0 or N1 (less than hilar) non-small cell carcinoma: results of the ACOSOG Z0030 Trial. J Thorac Cardiovasc Surg. doi: 10.1016/j.jtcvs.2010.11.008. In press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 458.Nomori H, Iwatani K, Kobayashi H, et al. Omission of mediastinal lymph node dissection in lung cancer: its techniques and diagnostic procedures. Ann Thorac Cardiovasc Surg. 2006;12:83–88. [PubMed] [Google Scholar]
- 459.Finley DJ, Yoshizawa A, Travis W, et al. Predictors of outcomes after surgical treatment of synchronous primary lung cancers. J Thorac Oncol. 2010;5:197–205. doi: 10.1097/JTO.0b013e3181c814c5. [DOI] [PubMed] [Google Scholar]
- 460.Hayes DF, Allred C, Anderson BO, et al. Breast. In: Edge SB, Byrd DR, Compton CC, et al., editors. AJCC Cancer Staging Manual. 7th Ed. New York: Springer; 2009. pp. 347–376. [Google Scholar]