

Abstract
Background
Pyrazinamide (PZA) is crucial for tuberculosis (TB) treatment, given its unique ability to eradicate persister bacilli. The worldwide burden of PZA resistance remains poorly described.
Methods
Systematic PubMed, Science Direct and Scopus searches for articles reporting phenotypic (liquid culture drug susceptibility testing or pyrazinamidase activity assays) and/or genotypic (polymerase chain reaction or DNA sequencing) PZA resistance. Global and regional summary estimates were obtained from random-effects meta-analysis, stratified by presence or risk of multidrug resistant TB (MDR-TB). Regional summary estimates were combined with regional WHO TB incidence estimates to determine the annual burden of PZA resistance. Information on single nucleotide polymorphisms (SNPs) in the pncA gene was aggregated to obtain a global summary.
Results
Pooled PZA resistance prevalence estimate was 16.2% (95% CI 11.2-21.2) among all TB cases, 41.3% (29.0-53.7) among patients at high MDR-TB risk, and 60.5% (52.3-68.6) among MDR-TB cases. The estimated global burden is 1.4 million new PZA resistant TB cases annually, about 270,000 in MDR-TB patients. Among 1,815 phenotypically resistant isolates, 608 unique SNPs occurred at 397 distinct positions throughout the pncA gene.
Interpretation
PZA resistance is ubiquitous, with an estimated one in six incident TB cases and more than half of all MDR-TB cases resistant to PZA globally. The diversity of SNPs across the pncA gene complicates the development of rapid molecular diagnostics. These findings caution against relying on PZA in current and future TB drug regimens, especially in MDR-TB patients.
Introduction
The global burden of tuberculosis (TB) remains a major concern for health authorities worldwide. In 2013, there were an estimated 9.0 million new cases and 1.5 million deaths from TB [1]. Treatment regimens for drug-susceptible TB consist of rifampicin (RIF), isoniazid (INH), pyrazinamide (PZA) and ethambutol (EMB). PZA forms a critical cornerstone of this regimen given its unique ability to eradicate persister bacilli, which allowed treatment shortening from 9–12 months to 6 months [2,3]. PZA will likely remain an important component of treatment regimens for drug-susceptible and multidrug-resistant TB (MDR-TB) because of its distinctive mode of action (interference with ATP production) [4,5] and its synergistic pharmacokinetic properties with two of the new anti-TB drugs: the diarylquinoline Bedaquiline (affects F1F0 proton ATP synthase) and the nitroimidazole PA-824 (enhances PZA activity by altering the cell wall integrity) [6–12].
PZase is only active at low pH (pH 5.00–6.00) as experienced in the phagosomal compartment. Down-regulation of efflux pumps in the persister Mycobacterium tuberculosis results in intracellular accumulation of POA, which leads to the depletion of membrane potential [13–17], and inhibits trans-translation [5]. The decreasing membrane potential is detrimental to non-replicating persisters whose energy requirements are finely balanced [9]. Trans-translation plays a role for stress survival and pathogenesis as it aids the management of stalled ribosomes, damaged mRNA and proteins during stressful conditions [14, 18–20].
Even though PZA is a crucial component of TB treatment, little is known about the prevalence of PZA resistance, particularly on a global scale. PZA drug susceptibility testing (DST) is technically challenging and rarely performed as part of routine care or routine drug surveillance in resource-limited settings. Two phenotypic PZA DSTs, BACTEC 460TB and BACTEC MGIT 960 (Becton Dickinson, Sparks, MD) exist; only BACTEC MGIT 960 is currently commercially available. Neither of these assays has been approved by the World Health Organization (WHO), likely due to their complexity and inconsistency, with frequent false positive results [21,22]. Classic and modified Wayne’s PZase methods, which assess the function of the PZase enzyme based on a colorimetric change at critical concentrations of 100μg/ml to 400μg/ml, respectively [23], are also not endorsed by the WHO. More recently, genotypic PZA assays have been developed based on observations that mutations in the pncA gene are the primary mechanism of PZA resistance [15,24–27]. The pncA gene encodes the pyrazinamidase (PZase) enzyme, which converts PZA, a pro-drug, into the active pyrazinoic acid (POA) [14,24]. These molecular techniques, albeit not approved by WHO, are the most commonly used techniques in PZA drug resistance studies.
Understanding regional differences in PZA resistance and its causal mutations is important for policy decisions regarding treatment regimens for drug-resistant TB and development of sequence-based diagnostics [26]. The aims of this review were to summarize the prevalence of PZA resistance globally and by WHO geographic regions, and to estimate the annual burden of PZA resistance, both stratified by MDR-TB status. We also summarize the global frequency and distribution of single nucleotide polymorphisms (SNPs) in the pncA gene in PZA resistant isolates.
Materials and Methods
Search Strategy and Selection Criteria
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.[28] We searched PubMed, ScienceDirect and Scopus on July 14, 2014 for relevant articles published in the English language between 1998 and 2014 using an a priori protocol. The search terms “tuberculosis AND (pyrazinamide OR PZA) AND (phenotype OR genotype OR PZase OR pyrazinamidase OR pncA OR BACTEC OR mutations OR resistance OR resistant OR susceptibility OR sequence analysis OR microbial sensitivity tests OR molecular typing)” were used to identify articles reporting on PZA resistance using any of the methods of interest: phenotypic PZA DST, PZase activity assays, and/or genotypic PZA assays. Additional articles were identified from reference lists and review articles.
Studies were eligible for inclusion in the meta-analysis of prevalence of PZA resistance if (1) PZA DST was assessed using at least one the following phenotypic tests: BACTEC liquid-based DST 460 or 960, considered the reference standard for PZA DST, or PZase activity assays using classic or modified Wayne’s methods [24]. If both BACTEC 960 and BACTEC 460 results were reported, only the BACTEC 960 results were included. BACTEC 960 results were preferred to the BACTEC 460 due to the BACTEC 460 no longer being commercially available. If results from BACTEC 460 using both a PZA concentration of 100μg/mL and 50μg/mL were reported, the results using 100μg/mL were included. If results from both classical and modified Wayne’s PZase assays were reported, the classical Wayne’s results were included. Authors were contacted if no clear method of PZA DST is described in the article. To be eligible for inclusion in the analysis, studies had to provide information on the MDR-TB risk status (patients diagnosed with MDR-TB, patients at high-risk of MDR-TB, or inclusion of any TB case), reporting on a single subgroup or stratifying results by subgroup. High-risk of MDR-TB was defined as an isolate being resistant to at least one anti-TB drug. Any TB was defined as the inclusion of patients independent of drug resistance profile.
Studies were eligible for inclusion in the descriptive SNP analysis if they performed genotypic testing using polymerase chain reaction (PCR) and DNA sequencing and characterized the found SNPs.
For both the PZA prevalence and pncA SNP analysis, studies including samples from multiple countries were only included if the results were stratified by country. In studies collecting multiple samples from a single patient, only the first sample result was used. Where a study performed repeat testing on a sample, only the first result was retained in the review. No additional exclusion criteria were imposed.
Data Extraction
MGW and RMW independently reviewed titles and abstracts of original studies retrieved by the search. MGW and TY reviewed full-text and references of selected articles. MGW and HMS abstracted study data from full reports.
The following information, if available, was abstracted from each article: first author surname; publication year; WHO region (Africa, Americas, Eastern Mediterranean, Europe, South East Asia, or Western Pacific); study dates; study design; study setting; sample size; MDR risk subgroup; age; gender; HIV status; exclusion criteria; specimen type; phenotypic DST method; PZase activity assay; genotypic method; and whether the up and down stream regions of pncA were sequenced. The number of patients with PZA resistance according to liquid DST, the lack of PZase activity, or genotypic mutations in the pncA gene was also recorded. As Taiwan was not defined by the WHO, it was grouped in the Western Pacific region.
Statistical Analysis
Summary estimates for the prevalence of PZA resistance, calculated using random-effects meta-analytic methods in STATA 13 (StataCorp LP, College Station, TX), were determined globally and for each WHO region, stratified according to whether the subgroup of patients had MDR-TB, were at high-risk of MDR-TB, or had any TB.
Estimation of the burden of PZA resistant TB, stratified by region and by presence of MDR-TB were obtained by multiplying the regional point estimates obtained by the random-effects meta-analysis by the most recent (2011) regional WHO estimates for incident TB and MDR-TB cases [1].
The analysis of SNPs in the pncA gene was descriptive. We present results according to nucleotide position in order to identify regions of SNP clustering within the pncA gene. In addition, we present a detailed description of all SNPs reported, including the location and type of polymorphism and countries where this SNP has been isolated, as well as whether this SNPs has been linked to a resistant phenotype only or has been observed in both resistant and susceptible isolates, with phenotypic resistance defined by BACTEC DST results or the PZase enzyme assay results if BACTEC DST result was not available.
Role of the funding source: The funders of the study (NIH and NRF) had no role in study design, data collection, data analysis, data interpretation, or writing of the report. The corresponding author had full access to all data in the study and had final responsibility for the decision to submit for publication.
Results
Selected Studies
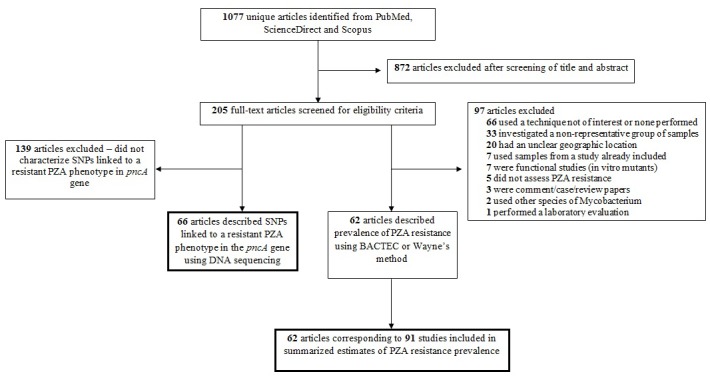
The literature search resulted in 1077 abstracts identified. Of these, 205 full-text articles were selected for review. In total, 62 [29–90] articles met the eligibility criteria for reporting PZA resistance, resulting in 91 datasets due to articles having isolates from multiple WHO regions as well as isolates which met different cohort type criteria (Fig 1). Of the 205 full-text articles reviewed, 66 [27,59–123] articles were eligible for inclusion in the analysis of SNP frequency and distribution.
Fig 1. Flow diagram describing article selection.
Phenotypic PZA Resistance: Study and Population Characteristics
The 62 [29–90] final studies provided phenotypic PZA resistance data on 35,950 M. tuberculosis clinical isolates. According to WHO regions, 8 [39,59,60,68,69,78] studies were from African region, 20 [29,30,38,40,41,43–47,59,70–72,79–83] from the Americas, 3 [31,48,80] from the Eastern Mediterranean, 20 [32,33,49–54,59,61,62,84–86] from European, 17 [34–36,47,55,56,59,63,73,80] from South East Asia, and 23 [37,42,57,58,64–67,74–77,80,86–90] from the Western Pacific region (Fig 2). Most (53/91) [30,35,36,39–61,63,64,78–90] estimates of PZA prevalence were provided for studies including any TB patient, independent of drug resistance profile; 25 [29–37,42,59–67] studies reported PZA resistance among individuals with confirmed MDR-TB, and 13 [33,34,38,68–77] estimates were available for individuals at high-risk of MDR-TB. Study and population characteristics are displayed in S1 Table.
Fig 2. Global distribution of included studies.

Countries are shaded if a study was included in this review.
Phenotypic PZA Resistance: Regional and Pooled Prevalences and Annual Burden
PZA resistance is prevalent across the entire globe and has been reported in all six WHO-defined regions (Fig 3). The pooled summarized prevalence estimate of PZA resistance was 60.5% (95% CI 52.3–68.6%) in MDR-TB patients, 41.3% (95% CI 29.0–53.7%) in TB patients at high-risk of MDR-TB, and 16.2% (95% CI 11.2–21.2%) in studies including any TB patient irrespective of resistance profile. In all six WHO regions, the prevalence of PZA resistance was two to six times higher in MDR-TB patients compared to the population of all TB patients.
Fig 3. Forest plot for the summary estimates of pyrazinamide prevalence by WHO region and presence or risk of MDR-TB.
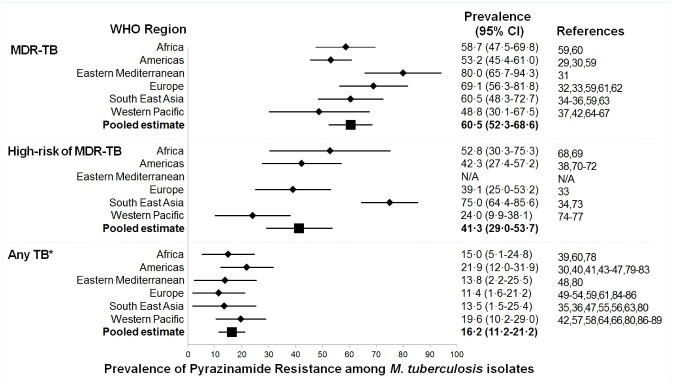
Abbreviations: CI, confidence interval; DST, drug susceptibility test; MDR-TB, multi-drug resistant tuberculosis; N/A, not applicable; WHO, world health organization. MDR-TB was defined as an isolate being resistant to RIF and INH. High risk of MDR-TB was defined as an isolate being resistant to at least one anti-TB drug. *Any TB was defined as the inclusion of patients independent of drug resistance profile.
PZA resistance prevalence among cases of MDR-TB ranged from 48.8% (95% CI 30.1–67.5%) in the Western Pacific to 80.0% (95% CI 65.7–94.3%) in the Eastern Mediterranean, but the latter estimate was based on a single study [31]. The estimated PZA prevalence among those at high risk of MDR-TB varied greatly, from 24.0% (95% CI 9.9–38.1%) in the Western Pacific region to 75.0% (95% CI 64.4–85.6%) in South East Asian region. In the general TB population, PZA prevalence estimated ranged from 11.4% (95% CI 1.6–21.2) in the European region to 21.9% (95% CI 12.0–31.9%) in the Americas.
Multiplying the regional WHO estimates for the annual number of new TB cases and incident MDR-TB cases by the pooled summarized prevalence estimates of PZA resistance, we estimated that about 1.4 million PZA resistant TB cases occur annually, corresponding to 16.2% of the 9.0 million incident TB cases in 2013 (Table 1). Of these, an estimated 270,000 occur in people also resistant to at least isoniazid and rifampicin, representing 60% of all incident cases of MDR-TB estimated in 2013.
Table 1. Estimated annual burden of new PZA resistant tuberculosis cases, overall and among MDR-TB patients, globally and by WHO region.
| WHO region | Incident TB cases* | Incident PZA resistant cases | Incident MDR-TB cases* | Incident PZA resistant MDR-TB cases |
|---|---|---|---|---|
| African | 2,600 000 | 416,000 | 78,000 | 45,800 |
| Americas | 280,000 | 44,800 | 8,400 | 4,468 |
| Eastern Mediterranean | 750,000 | 120,000 | 27,000 | 21,600 |
| European | 360,000 | 57,600 | 91,000 | 62,881 |
| South East Asian | 3,400 000 | 544,000 | 135,000 | 81,675 |
| Western Pacific | 1,600 000 | 256,000 | 125,000 | 61,000 |
| GLOBAL | 9,000 000 | 1,438 000 | 464,400 | 277,424 |
Abbreviations: MDR-TB, multi-drug resistant tuberculosis; PZA, pyrazinamide; TB, tuberculosis; WHO, World Health Organization.
* Incidence of TB cases from the World Health Organization Global Tuberculosis Report 2014.
Single Nucleotide Polymorphism Distribution in pncA Gene
The 66 [27,59–123] articles provided SNP data from 8,651 M. tuberculosis clinical isolates. According to WHO region, five [60,68,69,78,102] articles were from Africa, 14 [27,70–72,79,81–83,97,100,105,107,114,120] from the Americas, two [80,92] from the Eastern Mediterranean, 17 [61,62,84–86,93,96,103,104,106,108–110,115–117,119] from Europe, six [59,63,73,118,121,123] from South East Asia, and 22 [64–67,74–77,87–91,94,95,98,99,101,111–113,122] from the Western Pacific. A SNP in the pncA region was detected in the 1,815 of the 8,651 isolates, with 608 unique polymorphisms in 397 positions in the gene (S2 Table). SNPs were found throughout the entire pncA gene and flanking region with no particular clustering or hot spots (Fig 4). There are however, a few SNPs which were found to be more frequently than others such as -11 and 195, but even the 20 most frequent SNPs only represented one third of all isolates with phenotypic PZA resistance.
Fig 4. Distribution of reported single nucleotide polymorphisms (SNPs) throughout the pncA gene.
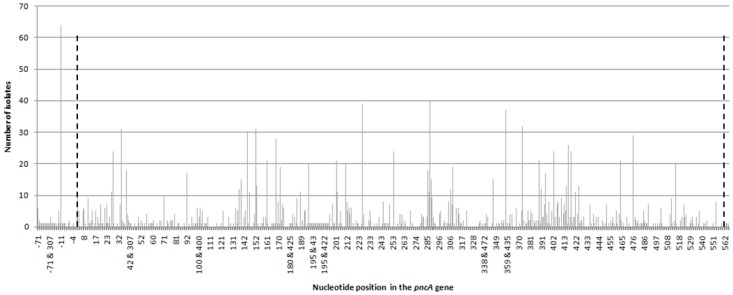
Dashed lines indicate the open reading frame for the pncA gene.
Discussion
M. tuberculosis resistance to rifampicin and isoniazid is well described and monitored, either through continuous surveillance or periodic surveys of a representative sample of patients [124]. In contrast, resistance to ethambutol and PZA, the other two front line drugs, is not routinely monitored and thus poorly described. In this systematic review and meta-analysis, we found that PZA resistance is ubiquitous and increases in prevalence as risk of resistance to other drugs increases, with pooled summary estimates for the prevalence of PZA resistance of 16.2% in the total population of TB patients, 41.3% among TB patients at high risk of MDR-TB, and 60.5% in patients with confirmed MDR-TB. The high prevalence of PZA resistance results in an annual estimated burden of 1.4 million new cases of PZA resistant TB, of which about 270,000 occur in patients with MDR-TB [1]. This high prevalence of PZA resistance observed in all regions of the world and across different TB patient groups is an important finding as PZA is not only a key component of all current regimens for both drug susceptible and drug resistant TB but is also included in all novel drug regimens currently undergoing evaluation in clinical phase II or III trials for treatment of drug-susceptible or drug-resistant TB [125].
While our review aimed to comprehensively summarize information on PZA as a global public health problem, a different systematic review by Chang et al aimed to summarize the performance of molecular and PZase assays compared to culture-based phenotypic DST [126]. In that review, the median (range) of PZA resistance was 5% (0% to 9%) in non-MDR isolates and 51% (31% to 89%) in MDR M. tuberculosis isolates [126]. Our pooled prevalence estimates were higher than the median prevalence reported by Chang et al., especially in the overall TB patient population (16.2%). The summary estimate in our review may have overestimated the overall prevalence of PZA resistance among TB patients if the proportion of patients with drug resistance included in the studies was higher than that observed in the general population of the country where the studies took place.
The high prevalence of PZA resistance and its inclusion in both standard and novel drug regimens highlights the need for routine PZA resistance testing. Others have suggested that molecular assays may be the way forward for detecting PZA resistance, based on findings that molecular assays targeting pncA can detect PZA resistance in MDR-TB isolates with high positive predictive values and rule out PZA resistance in non-MDR isolates with high negative predictive values [126,127]. However, DNA sequencing studies have revealed that mutations and/or polymorphisms occur across the entire length of the pncA gene, suggesting that sequencing the entire pncA gene would be essential to capture all possible mutations [109,117,127–129]. In this review, we confirmed that on a global scale, SNPs are distributed throughout the entire pncA gene. Whereas the tbdream database [14,26] previously reported on 278 unique polymorphisms prior to 2009, our systematic review provides an updated overview, with information on more than 600 unique polymorphisms in approximately 400 positions in pncA (including the upstream flanking region). A few SNPs occurred more frequently than others, possibly because these SNPs are rooted in ancestral strains. Consequently, developing a molecular assay to detect PZA resistance will be much more challenging compared to other genes (rpoB, gyrA, embB) which have been found to have clear resistance-causing hot spots [130]. The identification of causal PZA mutations is further complicated by the fact that not all non-synonymous mutations cause phenotypic resistance [80] and that mutations in the pncA gene can be absent in a small percentage of phenotypically PZA resistant isolates, [66,102] suggesting that PZA resistance could be conferred via an alternative mechanisms such as mutations in the rpsA gene [81]. Whereas development of simplified micro-array systems for simultaneous detection of rifampicin, isoniazid and ethambutol resistance may be possible, [131] inclusion of assessment of PZA resistance may thus require a different approach such as targeted DNA sequencing or next generation sequencing [127,132].
A major strength of our study was the comprehensive inclusion of studies from across the globe and stratification of estimates by region and TB patient category. Insight into PZA prevalence by region and TB patient category provides essential information for the development and clinical use of future PZA resistance tests. Our study adds to the review by Chang et al, which was aimed at summarizing PZA resistance assay performance, not PZA resistance prevalence. Our review also complements the recent study by Miotto et al, which presented pncA sequence results of 1950 clinical isolates obtained from multiple laboratories, but did not stratify results by regions or MDR-TB status [127]. Our review was however limited by the data quality of the original studies [126]. Misclassification of PZA resistance may have occurred in the studies included, and due to false positive results, may have resulted in an overestimate of the true prevalence of PZA resistance. Phenotypic PZA drug susceptibility testing has not been endorsed by the WHO perhaps due to concerns surrounding false positivity related to the acidity of the media, inoculum size and critical concentration used [17,133,134]. Alternative techniques, the PZase activity assays, [23,135] have been used in the hope of identifying PZA resistance more accurately, but the interpretation of colourmetric change for these assays is highly subjective [56]. It is uncertain whether all mutations observed in the pncA region are associated with resistance. Similar to the tbdream database approach, [26] we chose not to make a priori decisions as to whether mutations described actually confer resistance and report any mutation found in a PZA-resistant isolate. Another limitation was the restricted number of studies for certain regions (especially Eastern Mediterranean, where all strains included came from a single study in Pakistan) and the lack of adequate representation of countries within certain regions (especially for Africa, where almost all isolates included came from South Africa, and the Americas). This not only resulted in uncertainty of the accuracy of the point estimates and wide confidence intervals but also highlights the lack of information on PZA resistance in several regions of the world. Finally, many studies did not provide clinical information and we were therefore unable to stratify our analysis by new versus re-treatment status.
The ubiquitous presence of PZA resistance is of global interest and should signal a call to action. Development of rapid diagnostics to detect PZA resistance will be essential to maximize the efficacy of novel treatment regimens and minimize the risk of development of resistance to novel drugs. In addition, the high prevalence of PZA resistance, especially among MDR-TB patients, highlights the need for development of treatment regimens that can be effectively used in patients with PZA-resistant MDR-TB.
Supporting Information
(PDF)
Abbreviations: MDR-TB, multi-drug resistant tuberculosis; PZA, pyrazinamide; TB, tuberculosis; WHO, World Health Organization; lab, laboratory; N/A, not applicable; N/S, not stated; HR-MDR, high-risk multi-drug resistant tuberculosis; MTB, Mycobacterium tuberculosis; PCR, polymerase chain reaction, East Med, Eastern Mediterranean.
(PDF)
Abbreviations: A, adenine; bp, base pair; C, cytosine; del, deletion; G, guanine; R, resistant; SNP, single-nucleotide polymorphism; T, thymine. * Article found one isolate sensitive and one isolate resistant.
(PDF)
Acknowledgments
Research reported in this publication was supported by the National Institute of Allergy and Infectious Diseases of the National Institutes of Health under the award number R01AI099026. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Data Availability
All relevant data are within the paper and its Supporting Information files.
Funding Statement
AVR and MGW are partially funded by the National Institute of Allergy and Infectious Diseases (NIAID), National Institutes of Health (NIH), grant R01AI099026. HMS was partially supported by the NIH training grant 2T32AI070114. SLS is funded by the South African Research Chairs Initiative of the Department of Science and Technology and National Research Foundation (NRF) of South Africa, award number UID 86539. MGW funded by the NRF of South Africa and the Medical Research Council of South Africa, grant UID 89519. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
References
- 1. World Health Organization. Global Tuberculosis Report. Geneva, Switzerland: WHO press; 2014. [Google Scholar]
- 2. McDermott W, Tompsett R. Activation of pyrazinamide and nicotinamide in acidic environments in vitro. American review of tuberculosis. 1954;70(4):748–54. [DOI] [PubMed] [Google Scholar]
- 3. Mitchison DA. The Action Of Antituberculosis Drugs In Short-Course Chemotherapy. Tubercle. 1985;66(3):219–25. [DOI] [PubMed] [Google Scholar]
- 4. Shi W, Chen J, Feng J, Cui P, Zhang S, Weng X, et al. Aspartate decarboxylase (PanD) as a new target of pyrazinamide in Mycobacterium tuberculosis . Emerging Microbes & Infections. 2014;3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Shi W, Zhang X, Jiang X, Yuan H, Lee JS, Barry CE III, et al. Pyrazinamide Inhibits Trans-Translation in Mycobacterium tuberculosis . Science. 2011;333(6049):1630–2. 10.1126/science.1208813 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Ibrahim M, Andries K, Lounis N, Chauffour A, Truffot-Pernot C, Jarlier V, et al. Synergistic activity of R207910 combined with pyrazinamide against murine tuberculosis. Antimicrobial Agents and Chemotherapy. 2007;51(3):1011–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Tasneen R, Tyagi S, Williams K, Grosset J, Nuermberger E. Enhanced bactericidal activity of rifampin and/or pyrazinamide when combined with PA-824 in a murine model of tuberculosis. Antimicrob Agents Chemother. 2008;52(10):3664–8. 10.1128/AAC.00686-08 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Diacon AH, Donald PR, Pym A, Grobusch M, Patientia RF, Mahanyele R, et al. Randomized Pilot Trial of Eight Weeks of Bedaquiline (TMC207) Treatment for Multidrug-Resistant Tuberculosis: Long-Term Outcome, Tolerability, and Effect on Emergence of Drug Resistance. Antimicrobial Agents and Chemotherapy. 2012;56(6):3271–6. 10.1128/AAC.06126-11 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Zhang Y TA. Genetics of drug resistance in Mycobacterium tuberculosis In: Hatfull GF, Jacobs WR, eds. Molecular genetics of mycobacteria. Washington DC: ASM Press; 2000:235–54. [Google Scholar]
- 10. Andries K, Verhasselt P, Guillemont J, Gohlmann HWH, Neefs JM, Winkler H, et al. A diarylquinoline drug active on the ATP synthase of Mycobacterium tuberculosis . Science. 2005;307(5707):223–7. [DOI] [PubMed] [Google Scholar]
- 11. Zhang Y, Wade MM, Scorpio A, Zhang H, Sun ZH. Mode of action of pyrazinamide: disruption of Mycobacterium tuberculosis membrane transport and energetics by pyrazinoic acid. Journal of Antimicrobial Chemotherapy. 2003;52(5):790–5. [DOI] [PubMed] [Google Scholar]
- 12. Shi R, Sugawara I. Development of New Anti-tuberculosis Drug Candidates. Tohoku Journal of Experimental Medicine. 2010;221(2):97–106. [DOI] [PubMed] [Google Scholar]
- 13. Stover CK, Warrener P, VanDevanter DR, Sherman DR, Arain TM, Langhorne MH, et al. A small-molecule nitroimidazopyran drug candidate for the treatment of tuberculosis. Nature. 2000;405(6789):962–6. [DOI] [PubMed] [Google Scholar]
- 14. Zhang Y, Shi W, Zhang W, Mitchison D. Mechanisms of Pyrazinamide Action and Resistance. Microbiology Spectrum. 2014;2(4). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Somoskovi A, Parsons LM, Salfinger M. The molecular basis of resistance to isoniazid, rifampin, and pyrazinamide in Mycobacterium tuberculosis . Respiratory Research. 2001;2(3):164–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Zimhony O, Vilcheze C, Jacobs WR. Characterization of Mycobacterium smegmatis expressing the Mycobacterium tuberculosis fatty acid synthase I (fas1) gene. Journal of Bacteriology. 2004;186(13):4051–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Zhang Y, Mitchison D. The curious characteristics of pyrazinamide: a review. International Journal of Tuberculosis and Lung Disease. 2003;7(1):6–21. [PubMed] [Google Scholar]
- 18. Muto A, Fujihara A, Ito K, Matsuno J, Ushida C, Himeno H. Requirement of transfer-messenger RNA for the growth of Bacillus subtilis under stresses. Genes to Cells. 2000;5(8):627–35. [DOI] [PubMed] [Google Scholar]
- 19. Thibonnier M, Thiberge J-M, De Reuse H. Trans-Translation in Helicobacter pylori: Essentiality of Ribosome Rescue and Requirement of Protein Tagging for Stress Resistance and Competence. Plos One. 2008;3(11). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Keiler KC. Biology of trans-Translation. Annual Review of Microbiology. Annual Review of Microbiology. 622008 p. 133–51. [DOI] [PubMed] [Google Scholar]
- 21. World Health Organization. Global Tuberculosis Report. Geneva, Switzerland: WHO press; 2012. [Google Scholar]
- 22. World Health Organization. Guidelines for the programmatic management of drug-resistant tuberculosis: emergency update 2008. Geneva, Switzerland: WHO press; 2008. [Google Scholar]
- 23. Wayne LG. Simple Pyrazinamidase And Urease Tests For Routine Identification Of Mycobacteria . American Review of Respiratory Disease. 1974;109(1):147–51. [DOI] [PubMed] [Google Scholar]
- 24. Scorpio A, Zhang Y. Mutations in pncA, a gene encoding pyrazinamidase/nicotinamidase, cause resistance to the antituberculous drug pyrazinamide in tubercle bacillus. Nature Medicine. 1996;2(6):662–7. [DOI] [PubMed] [Google Scholar]
- 25. Scorpio A, LindholmLevy P, Heifets L, Gilman R, Siddiqi S, Cynamon M, et al. Characterization of pncA mutations in pyrazinamide-resistant Mycobacterium tuberculosis . Antimicrobial Agents and Chemotherapy. 1997;41(3):540–3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Sandgren A, Strong M, Muthukrishnan P, Weiner BK, Church GM, Murray MB. Tuberculosis Drug Resistance Mutation Database. Plos Medicine. 2009;6(2):132–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Cheng SJ, Thibert L, Sanchez T, Heifets L, Zhang Y. pncA mutations as a major mechanism of pyrazinamide resistance in Mycobacterium tuberculosis: Spread of a monoresistant strain in Quebec, Canada. Antimicrobial Agents and Chemotherapy. 2000;44(3):528–32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Moher D, Liberati A, Tetzlaff J, Altman DG, Grp P. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Plos Medicine. 2009;6(7). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Becerra MC, Freeman J, Bayona J, Shin SS, Kim JY, Furin JJ, et al. Using treatment failure under effective directly observed short-course chemotherapy programs to identify patients with multidrug-resistant tuberculosis. International Journal of Tuberculosis and Lung Disease. 2000;4(2):108–14. [PubMed] [Google Scholar]
- 30. LaBombardi VJ. Comparison of the ESP and BACTEC systems for testing susceptibilities of Mycobacterium tuberculosis complex isolates to pyrazinamide. Journal of Clinical Microbiology. 2002;40(6):2238–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Khurram M, Khaar HTB, Fahim M. Multidrug-resistant tuberculosis in Rawalpindi, Pakistan. Journal of Infection in Developing Countries. 2012;6(1):29–32. [DOI] [PubMed] [Google Scholar]
- 32. Pardini M, Varaine F, Hewison C, Iona E, Pataracchia M, Orefici G, et al. Pyrazinamide resistance in multidrug-resistant strains of Mycobacterium tuberculosis isolated in Abkhazia. Journal of Chemotherapy. 2007;19(1):106–7. [DOI] [PubMed] [Google Scholar]
- 33. Fattorini L, Iona E, Ricci ML, Thoresen OF, Orru G, Oggioni MR, et al. Activity of 16 antimicrobial agents against drug-resistant strains of Mycobacterium tuberculosis . Microbial Drug Resistance-Mechanisms Epidemiology and Disease. 1999;5(4):265–70. [DOI] [PubMed] [Google Scholar]
- 34. Kelly PM, Lumb R, Pinto A, da Costa G, Sarmento J, Bastian I. Analysis of Mycobacterium tuberculosis isolates from treatment failure patients living in East Timor. International Journal of Tuberculosis and Lung Disease. 2005;9(1):81–6. [PubMed] [Google Scholar]
- 35. Kelly PM, Ardian M, Waramori G, Anstey NM, Syahrial H, Tijtra E, et al. A community-based TB drug susceptibility study in Mimika district, Papua province, Indonesia. International Journal of Tuberculosis and Lung Disease. 2006;10(2):167–71. [PubMed] [Google Scholar]
- 36. Arora J, Sidiq Z, Visalakshi P, Bhalla M, Behera D, Myneedu VP. Pyrazinamide resistance among drug-resistant Mycobacterium tuberculosis isolates at a referral hospital. Diagnostic Microbiology and Infectious Disease. 2013;77(4):380–1. 10.1016/j.diagmicrobio.2013.08.014 [DOI] [PubMed] [Google Scholar]
- 37. Simpson G, Coulter C, Weston J, Knight T, Carter R, Vincent S, et al. Resistance patterns of multidrug-resistant tuberculosis in Western Province, Papua New Guinea. International Journal of Tuberculosis and Lung Disease. 2011;15(4):551–2. 10.5588/ijtld.10.0347 [DOI] [PubMed] [Google Scholar]
- 38. Saravia JC, Appleton SC, Rich ML, Sarria M, Bayona J, Becerra MC. Retreatment management strategies when first-line tuberculosis therapy fails. International Journal of Tuberculosis and Lung Disease. 2005;9(4):421–9. [PubMed] [Google Scholar]
- 39. Ndung'u PW, Kariuki S, Ng'ang'a Z, Revathi G. Resistance patterns of Mycobacterium tuberculosis isolates from pulmonary tuberculosis patients in Nairobi. Journal of Infection in Developing Countries. 2012;6(1):33–9. [DOI] [PubMed] [Google Scholar]
- 40. Barreto AMW, Araujo JBM, Medeiros RFD, Caldas PCD. Direct sensitivity test of the MB/BacT system. Memorias Do Instituto Oswaldo Cruz. 2002;97(2):263–4. [DOI] [PubMed] [Google Scholar]
- 41. Ribeiro LB, Magalhaes V, Magalhaes M. Primary and acquired pyrazinamide resistance in patients with pulmonary tuberculosis treated at a referral hospital in the city of Recife, Brazil. Jornal Brasileiro De Pneumologia. 2012;38(6):740–7. [DOI] [PubMed] [Google Scholar]
- 42. Huang W-C, Chen C-H, Huang C-C, Wu K-M, Chiou C-S, Lin C-F, et al. A Reduction in Anti-Tuberculosis Drug Resistance after the Implementation of the National "STOP TB" Program in Central Taiwan, 2003–2007. Japanese Journal of Infectious Diseases. 2013;66(2):89–95. [DOI] [PubMed] [Google Scholar]
- 43. Chedore P, Bertucci L, Wolfe J, Sharma M, Jamieson F. Potential for Erroneous Results Indicating Resistance When Using the Bactec MGIT 960 System for Testing Susceptibility of Mycobacterium tuberculosis to Pyrazinamide. Journal of Clinical Microbiology. 2010;48(1):300–1. 10.1128/JCM.01775-09 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. Granich RM, Balandrano S, Santaella AJ, Binkin NJ, Castro KG, Marquez-Fiol A, et al. Survey of drug resistance of Mycobacterium tuberculosis in 3 Mexican states, 1997. Archives of Internal Medicine. 2000;160(5):639–44. [DOI] [PubMed] [Google Scholar]
- 45. Sachais BS, Nachamkin I, Mills JK, Leonard DGB. Novel pncA mutations in pyrazinamide-resistant isolates of Mycobacterium tuberculosis . Molecular Diagnosis. 1998;3(4):229–32. [DOI] [PubMed] [Google Scholar]
- 46. Fredricks BA, DeCoster DJ, Kim Y, Sparks N, Callister SM, Schell RF. Rapid pyrazinamide susceptibility testing of Mycobacterium tuberculosis by flow cytometry. Journal of Microbiological Methods. 2006;67(2):266–72. [DOI] [PubMed] [Google Scholar]
- 47. Duque A, Lin SYG, Desmond E, Rienthong S, Rienthong D, Boonin C. Evaluation of the BD Bactec MGIT 320 System for Detection of Mycobacteria and Drug Susceptibility Testing of Mycobacterium tuberculosis . Journal of Clinical Microbiology. 2013;51(10):3403–5. 10.1128/JCM.01357-13 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Khan MY, Kinsara AJ, Osoba AO, Wali S, Samman Y, Memish Z. Increasing resistance of M-tuberculosis to anti-TB drugs in Saudi Arabia. International Journal of Antimicrobial Agents. 2001;17(5):415–8. [DOI] [PubMed] [Google Scholar]
- 49. Kontos F, Nicolaou S, Kostopoulos C, Gitti Z, Petinaki E, Maniati M, et al. Multicenter evaluation of the fully automated Bactec MGIT 960 system for susceptibility testing of Mycobacterium tuberculosis to pyrazinamide: comparison with the radiometric Bactec 460TB system. Journal of Microbiological Methods. 2003;55(1):331–3. [DOI] [PubMed] [Google Scholar]
- 50. Nutini S, Tortoli E, Corrado A. Multidrug-resistant tuberculosis in the Florence province from 1992 to 1995. International Journal of Tuberculosis and Lung Disease. 1998;2(6):484–9. [PubMed] [Google Scholar]
- 51. Scarparo C, Ricordi P, Ruggiero G, Piccoli P. Evaluation of the fully automated BACTEC MGIT 960 system for testing susceptibility of Mycobacterium tuberculosis to pyrazinamide, streptomycin, isoniazid, rifampin, and ethambutol and comparison with the radiometric BACTEC 460TB method. Journal of Clinical Microbiology. 2004;42(3):1109–14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52. Napiorkowska A, Augustynowicz-Kopec E, Zwolska Z. Phenotypic characterization of pyrazinamide-resistant Mycobacterium tuberculosis isolated in Poland. Pneumonologia i alergologia polska. 2010;78(4):256–62. [PubMed] [Google Scholar]
- 53. Espasa M, Salvado M, Vicente E, Tudo G, Alcaide F, Coll P, et al. Evaluation of the VersaTREK System Compared to the Bactec MGIT 960 System for First-Line Drug Susceptibility Testing of Mycobacterium tuberculosis . Journal of Clinical Microbiology. 2012;50(2):488–91. 10.1128/JCM.06432-11 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54. Djuretic T, Herbert J, Drobniewski F, Yates M, Smith EG, Magee JG, et al. Antibiotic resistant tuberculosis in the United Kingdom: 1993–1999. Thorax. 2002;57(6):477–82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55. Krishnamurthy A, Almeida D, Rodrigues C, Mehta A. Comparison of pyrazinamide drug susceptibility of M. tuberculosis by radiometric BACTEC and enzymatic pyrazinamidase assay. Indian journal of medical microbiology. 2004;22(3):166–8. [PubMed] [Google Scholar]
- 56. Sharma B, Pal N, Malhotra B, Vyas L, Rishi S. Comparison of MGIT 960 & pyrazinamidase activity assay for pyrazinamide susceptibility testing of Mycobacterium tuberculosis . Indian Journal of Medical Research. 2010;132(1):72–6. [PubMed] [Google Scholar]
- 57. Su W-J, Feng J-Y, Huang C-C, Perng R-P. Increasing drug resistance of Mycobacterium tuberculosis isolates in a medical center in northern Taiwan. Journal of the Formosan Medical Association. 2008;107(3):259–64. 10.1016/S0929-6646(08)60145-X [DOI] [PubMed] [Google Scholar]
- 58. Hung NV, Ando H, Thuy TT-B, Kuwahara T, Hang NT-L, Sakurada S, et al. Clonal expansion of Mycobacterium tuberculosis isolates and coexisting drug resistance in patients newly diagnosed with pulmonary tuberculosis in Hanoi, Vietnam. BMC research notes. 2013;6:444-. 10.1186/1756-0500-6-444 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59. Mestdagh M, Fonteyne PA, Realini L, Rossau R, Jannes G, Mijs W, et al. Relationship between pyrazinamide resistance, loss of pyrazinamidase activity, and mutations in the pncA locus in multidrug-resistant clinical isolates of Mycobacterium tuberculosis . Antimicrobial Agents and Chemotherapy. 1999;43(9):2317–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60. Mphahlele M, Syre H, Valvatne H, Stavrum R, Mannsaker T, Muthivhi T, et al. Pyrazinamide resistance among South African multidrug-resistant Mycobacterium tuberculosis isolates. Journal of Clinical Microbiology. 2008;46(10):3459–64. 10.1128/JCM.00973-08 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61. Piersimoni C, Mustazzolu A, Giannoni F, Bornigia S, Gherardi G, Fattorini L. Prevention of False Resistance Results Obtained in Testing the Susceptibility of Mycobacterium tuberculosis to Pyrazinamide with the Bactec MGIT 960 System Using a Reduced Inoculum. Journal of Clinical Microbiology. 2013;51(1):291–4. 10.1128/JCM.01838-12 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62. Perdigao J, Macedo R, Joao I, Fernandes E, Brum L, Portugal I. Multidrug-resistant tuberculosis in Lisbon, Portugal: A molecular epidemiological perspective. Microbial Drug Resistance. 2008;14(2):133–43. 10.1089/mdr.2008.0798 [DOI] [PubMed] [Google Scholar]
- 63. Jonmalung J, Prammananan T, Leechawengwongs M, Chaiprasert A. Surveillance of pyrazinamide susceptibility among multidrug-resistant Mycobacterium tuberculosis isolates from Siriraj Hospital, Thailand. BMC Microbiol. 2010;10:223 10.1186/1471-2180-10-223 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64. Tan Y, Hu Z, Zhang T, Cai X, Kuang H, Liu Y, et al. Role of pncA and rpsA Gene Sequencing in Detection of Pyrazinamide Resistance in Mycobacterium tuberculosis Isolates from Southern China. Journal of Clinical Microbiology. 2014;52(1):291–7. 10.1128/JCM.01903-13 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65. Ando H, Mitarai S, Kondo Y, Suetake T, Sekiguchi JI, Kato S, et al. Pyrazinamide resistance in multidrug-resistant Mycobacterium tuberculosis isolates in Japan. Clinical microbiology and infection: the official publication of the European Society of Clinical Microbiology and Infectious Diseases. 2010;16(8):1164–8. [DOI] [PubMed] [Google Scholar]
- 66. Huang TS, Lee SSJ, Tu HZ, Huang WK, Chen YS, Huang CK, et al. Correlation between pyrazinamide activity and pncA mutations in Mycobacterium tuberculosis isolates in Taiwan. Antimicrobial Agents and Chemotherapy. 2003;47(11):3672–3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67. Chiu Y-C, Huang S-F, Yu K-W, Lee Y-C, Feng J-Y, Su W-J. Characteristics of pncA mutations in multidrug-resistant tuberculosis in Taiwan. Bmc Infectious Diseases. 2011;11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68. Davies AP, Billington OJ, McHugh TD, Mitchison DA, Gillespie SH. Comparison of phenotypic and genotypic methods for pyrazinamide susceptibility testing with Mycobacterium tuberculosis . Journal of Clinical Microbiology. 2000;38(10):3686–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69. Louw GE, Warren RM, Donald PR, Murray MB, Bosman M, Van Heiden PD, et al. Frequency and implications of pyrazinamide resistance in managing previously treated tuberculosis patients. International Journal of Tuberculosis and Lung Disease. 2006;10(7):802–7. [PubMed] [Google Scholar]
- 70. Clemente WT, Soares Lima SS, Palaci M, Silva MSN, Sumnienski Rodrigues VF, Dalla Costa ER, et al. Phenotypic and genotypic characterization of drug-resistant Mycobacterium tuberculosis strains. Diagnostic Microbiology and Infectious Disease. 2008;62(2):199–204. 10.1016/j.diagmicrobio.2008.06.013 [DOI] [PubMed] [Google Scholar]
- 71. Cuevas-Cordoba B, Oyuki Xochihua-Gonzalez S, Cuellar A, Fuentes-Dominguez J, Zenteno-Cuevas R. Characterization of pncA gene mutations in pyrazinamide-resistant Mycobacterium tuberculosis isolates from Mexico. Infection Genetics and Evolution. 2013;19:330–4. [DOI] [PubMed] [Google Scholar]
- 72. Escalante P, Ramaswamy S, Sanabria H, Soini H, Pan X, Valiente-Castillo O, et al. Genotypic characterization of drug-resistant Mycobacterium tuberculosis isolates from Peru. Tubercle and lung disease: the official journal of the International Union against Tuberculosis and Lung Disease. 1998;79(2):111–8. [DOI] [PubMed] [Google Scholar]
- 73. Muthaiah M, Jagadeesan S, Ayalusamy N, Sreenivasan M, Prabhu SS, Muthuraj U, et al. Molecular Epidemiological Study of Pyrazinamide-Resistance in Clinical Isolates of Mycobacterium tuberculosis from South India. International Journal of Molecular Sciences. 2010;11(7):2670–80. 10.3390/ijms11072670 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74. Chan RCY, Hui M, Chan EWC, Au TK, Chin ML, Yip CK, et al. Genetic and phenotypic characterization of drug-resistant Mycobacterium tuberculosis isolates in Hong Kong. Journal of Antimicrobial Chemotherapy. 2007;59(5):866–73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75. Aono A, Hirano K, Hamasaki S, Abe C. Evaluation of BACTEC MGIT 960 PZA medium for susceptibility testing of Mycobacterium tuberculosis to pyrazinamide (PZA): compared with the results of pyrazinamidase assay and Kyokuto PZA test. Diagnostic Microbiology and Infectious Disease. 2002;44(4):347–52. [DOI] [PubMed] [Google Scholar]
- 76. Lee ASG, Tang LLH, Lim IHK, Wong SY. Characterization of pyrazinamide and ofloxacin resistance among drug resistant Mycobacterium tuberculosis isolates from Singapore. International journal of infectious diseases: IJID: official publication of the International Society for Infectious Diseases. 2002;6(1):48–51. [DOI] [PubMed] [Google Scholar]
- 77. Choi J-H, Lee KW, Kang H-R, Hwang YI, Jang S, Kim D-G, et al. Clinical Efficacy of Direct DNA Sequencing Analysis on Sputum Specimens for Early Detection of Drug-Resistant Mycobacterium tuberculosis in a Clinical Setting. Chest. 2010;137(2):393–400. 10.1378/chest.09-0150 [DOI] [PubMed] [Google Scholar]
- 78. Daum LT, Rodriguez JD, Worthy SA, Ismail NA, Omar SV, Dreyer AW, et al. Next-Generation Ion Torrent Sequencing of Drug Resistance Mutations in Mycobacterium tuberculosis Strains. Journal of Clinical Microbiology. 2012;50(12):3831–7. 10.1128/JCM.01893-12 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79. Bhuju S, Fonseca LdS, Marsico AG, de Oliveira Vieira GB, Sobral LF, Stehr M, et al. Mycobacterium tuberculosis isolates from Rio de Janeiro reveal unusually low correlation between pyrazinamide resistance and mutations in the pncA gene. Infection Genetics and Evolution. 2013;19:1–6. [DOI] [PubMed] [Google Scholar]
- 80. Hirano K, Takahashi M, Kazumi Y, Fukasawa Y, Abe C. Mutation in pncA is a major mechanism of pyrazinamide resistance in Mycobacterium tuberculosis . Tubercle and Lung Disease. 1998;78(2):117–22. [DOI] [PubMed] [Google Scholar]
- 81. Alexander DC, Ma JH, Guthrie JL, Blair J, Chedore P, Jamieson FB. Gene Sequencing for Routine Verification of Pyrazinamide Resistance in Mycobacterium tuberculosis: a Role for pncA but Not rpsA . Journal of Clinical Microbiology. 2012;50(11):3726–8. 10.1128/JCM.00620-12 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82. Mirabal NC, Yzquierdo SL, Lemus D, Madruga M, Milian Y, Echemendia M, et al. Evaluation of Colorimetric Methods Using Nicotinamide for Rapid Detection of Pyrazinamide Resistance in Mycobacterium tuberculosis . Journal of Clinical Microbiology. 2010;48(8):2729–33. 10.1128/JCM.00311-10 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83. Sheen P, Mendez M, Gilman RH, Pena L, Caviedes L, Zimic MJ, et al. Sputum PCR-Single-Strand Conformational Polymorphism Test for Same-Day Detection of Pyrazinamide Resistance in Tuberculosis Patients. Journal of Clinical Microbiology. 2009;47(9):2937–43. 10.1128/JCM.01594-08 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84. Lemaitre N, Sougakoff W, Truffot-Pernot C, Jarlier V. Characterization of new mutations in pyrazinamide-resistant strains of Mycobacterium tuberculosis and identification of conserved regions important for the catalytic activity of the pyrazinamidase PncA . Antimicrobial Agents and Chemotherapy. 1999;43(7):1761–3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85. Simons SO, van Ingen J, van der Laan T, Mulder A, Dekhuijzen PNR, Boeree MJ, et al. Validation of pncA Gene Sequencing in Combination with the Mycobacterial Growth Indicator Tube Method To Test Susceptibility of Mycobacterium tuberculosis to Pyrazinamide. Journal of Clinical Microbiology. 2012;50(2):428–34. 10.1128/JCM.05435-11 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86. Sekiguchi J-i, Miyoshi-Akiyama T, Augustynowicz-Kopec E, Zwolska Z, Kirikae F, Toyota E, et al. Detection of multidrug resistance in Mycobacterium tuberculosis . Journal of Clinical Microbiology. 2007;45(1):179–92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87. Zhou M, Geng X, Chen J, Wang X, Wang D, Deng J, et al. Rapid Colorimetric Testing for Pyrazinamide Susceptibility of M. tuberculosis by a PCR-Based In-Vitro Synthesized Pyrazinamidase Method. Plos One. 2011;6(11). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88. Cui Z, Wang J, Lu J, Huang X, Zheng R, Hu Z. Evaluation of Methods for Testing the Susceptibility of Clinical Mycobacterium tuberculosis Isolates to Pyrazinamide. Journal of Clinical Microbiology. 2013;51(5):1374–80. 10.1128/JCM.03197-12 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89. Endoh T, Yagihashi A, Uehara N, Kobayashi D, Tsuji N, Nakamura M, et al. Pyrazinamide resistance associated with pncA gene mutation in Mycobacterium tuberculosis in Japan. Epidemiology and Infection. 2002;128(2):337–42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90. Huang Z-k, Luo Q, Jiang B-x, Li W-t, Xu X-m, Xiong G-l, et al. Performance of the microscopic observation drug susceptibility assay in pyrazinamide susceptibility testing for Mycobacterium tuberculosis . Chinese Medical Journal. 2013;126(22):4334–9. [PubMed] [Google Scholar]
- 91. Kim HJ, Kwak HK, Lee J, Yun YJ, Lee JS, Lee MS, et al. Patterns of pncA mutations in drug-resistant Mycobacterium tuberculosis isolated from patients in South Korea. International Journal of Tuberculosis and Lung Disease. 2012;16(1):98–103. 10.5588/ijtld.10.0739 [DOI] [PubMed] [Google Scholar]
- 92. Doustdar F, Khosravi AD, Farnia P. Mycobacterium tuberculosis Genotypic Diversity in Pyrazinamide-Resistant Isolates of Iran. Microbial Drug Resistance. 2009;15(4):251–6. 10.1089/mdr.2009.0066 [DOI] [PubMed] [Google Scholar]
- 93. Marttila HJ, Marjamaki M, Vyshnevskaya E, Vyshnevskiy BI, Otten TF, Vasilyef AV, et al. pncA mutations in pyrazinamide-resistant Mycobacterium tuberculosis isolates from northwestern Russia. Antimicrobial Agents and Chemotherapy. 1999;43(7):1764–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94. Lee KW, Lee JM, Jung KS. Characterization of pncA mutations of pyrazinamide-resistant Mycobacterium tuberculosis in Korea. Journal of Korean Medical Science. 2001;16(5):537–43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95. Park SK, Lee JY, Chang CL, Lee MK, Son HC, Kim CM, et al. pncA mutations in clinical Mycobacterium tuberculosis isolates from Korea. Bmc Infectious Diseases. 2001;1:art. no.-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96. Portugal I, Barreiro L, Moniz-Pereira J, Brum L. pncA mutations in pyrazinamide-resistant Mycobacterium tuberculosis isolates in Portugal. Antimicrobial Agents and Chemotherapy. 2004;48(7):2736–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97. Barco P, Cardoso RF, Hirata RDC, Leite CQF, Pandolfi JR, Sato DN, et al. pncA mutations in pyrazinamide-resistant Mycobacterium tuberculosis clinical isolates from the southeast region of Brazil. Journal of Antimicrobial Chemotherapy. 2006;58(5):930–5. [DOI] [PubMed] [Google Scholar]
- 98. Hou L, Osei-Hyiaman D, Zhang Z, Wang B, Yang A, Kano K. Molecular characterization of pncA gene mutations in Mycobacterium tuberculosis clinical isolates from China. Epidemiology and Infection. 2000;124(2):227–32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99. Miyagi C, Yamane N, Yogesh B, Ano H, Takashima T. Genetic and phenotypic characterization of pyrazinamide-resistant Mycobacterium tuberculosis complex isolates in Japan. Diagnostic Microbiology and Infectious Disease. 2004;48(2):111–6. [DOI] [PubMed] [Google Scholar]
- 100. Rodrigues V, Telles MA, Ribeiro MO, Cafrune PU, Rossetti MLR, Zaha A. Characterization of pncA mutations in pyrazinamide-resistant Mycobacterium tuberculosis in Brazil. Antimicrobial Agents and Chemotherapy. 2005;49(1):444–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101. Jnawali HN, Hwang SC, Park YK, Kim H, Lee YS, Chung GT, et al. Characterization of mutations in multi- and extensive drug resistance among strains of Mycobacterium tuberculosis clinical isolates in Republic of Korea. Diagnostic Microbiology and Infectious Disease. 2013;76(2):187–96. 10.1016/j.diagmicrobio.2013.02.035 [DOI] [PubMed] [Google Scholar]
- 102. Bishop KS, Blumberg L, Trollip AP, Smith AN, Roux L, York DF, et al. Characterisation of the pncA gene in Mycobacterium tuberculosis isolates from Gauteng, South Africa. International Journal of Tuberculosis and Lung Disease. 2001;5(10):952–7. [PubMed] [Google Scholar]
- 103. Tracevska T, Jansone I, Baumanis V, Nodieva A, Marga O, Skenders G. Spectrum of pncA mutations in multidrug-resistant Mycobacterium tuberculosis isolates obtained in Latvia. Antimicrobial Agents and Chemotherapy. 2004;48(8):3209–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104. Yuksel P, Tansel O. Characterization of pncA mutations of pyrazinamide-resistant Mycobacterium tuberculosis in Turkey. New Microbiologica. 2009;32(2):153–8. [PubMed] [Google Scholar]
- 105. Morlock GP, Crawford JT, Butler WR, Brim SE, Sikes D, Mazurek GH, et al. Phenotypic characterization of pncA mutants of Mycobacterium tuberculosis . Antimicrobial Agents and Chemotherapy. 2000;44(9):2291–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106. Jureen P, Werngren J, Toro J-C, Hoffner S. Pyrazinamide resistance and pncA gene mutations in Mycobacterium tuberculosis . Antimicrobial Agents and Chemotherapy. 2008;52(5):1852–4. 10.1128/AAC.00110-08 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107. Denkin S, Volokhov D, Chizhikov V, Zhang Y. Microarray-based pncA genotyping of pyrazinamide-resistant strains of Mycobacterium tuberculosis . Journal of Medical Microbiology. 2005;54(12):1127–31. [DOI] [PubMed] [Google Scholar]
- 108. Zhdanova S, Heysell SK, Ogarkov O, Boyarinova G, Alexeeva G, Pholwat S, et al. Primary Multidrug-Resistant Mycobacterium tuberculosis in 2 Regions, Eastern Siberia, Russian Federation. Emerging Infectious Diseases. 2013;19(10):1649–52. 10.3201/eid1910.121108 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109. Stoffels K, Mathys V, Fauville-Dufaux M, Wintjens R, Bifani P. Systematic Analysis of Pyrazinamide-Resistant Spontaneous Mutants and Clinical Isolates of Mycobacterium tuberculosis . Antimicrobial Agents and Chemotherapy. 2012;56(10):5186–93. 10.1128/AAC.05385-11 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110. Brown TJ, Tansel O, French GL. Simultaneous identification and typing of multi-drug-resistant Mycobacterium tuberculosis isolates by analysis of pncA and rpoB . Journal of Medical Microbiology. 2000;49(7):651–6. [DOI] [PubMed] [Google Scholar]
- 111. Pandey S, Newton S, Upton A, Roberts S, Drinkovic D. Characterisation of pncA mutations in clinical Mycobacterium tuberculosis isolates in New Zealand. Pathology. 2009;41(6):582–4. [DOI] [PubMed] [Google Scholar]
- 112. Suzuki Y, Suzuki A, Tamaru A, Katsukawa C, Oda H. Rapid detection of pyrazinamide-resistant Mycobacterium tuberculosis by a PCR-based in vitro system. Journal of Clinical Microbiology. 2002;40(2):501–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 113. Zhang H, Bi LJ, Li CY, Sun ZG, Deng JY, Zhang XE. Mutations Found in the pncA Gene of Mycobacterium tuberculosis in Clinical Pyrazinamide-resistant Isolates from a Local Region of China. Journal of International Medical Research. 2009;37(5):1430–5. [DOI] [PubMed] [Google Scholar]
- 114. Hannan MM, Desmond EP, Morlock GP, Mazurek GH, Crawford JT. Pyrazinamide-monoresistant Mycobacterium tuberculosis in the United States. Journal of Clinical Microbiology. 2001;39(2):647–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115. Hoffner S, Angeby K, Sturegard E, Jonsson B, Johansson A, Sellin M, et al. Proficiency of drug susceptibility testing of Mycobacterium tuberculosis against pyrazinamide: the Swedish experience. International Journal of Tuberculosis and Lung Disease. 2013;17(11):1486–90. 10.5588/ijtld.13.0195 [DOI] [PubMed] [Google Scholar]
- 116. Aragon LM, Garrigo M, Moreno C, Espanol M, Coll P. Evaluation of the BacT/ALERT PZA kit in comparison with the BACTEC 460TB PZA for testing Mycobacterium tuberculosis susceptibility to pyrazinamide. Journal of Antimicrobial Chemotherapy. 2007;60(3):655–7. [DOI] [PubMed] [Google Scholar]
- 117. Werngren J, Sturegard E, Jureen P, Angeby K, Hoffner S, Schon T. Reevaluation of the Critical Concentration for Drug Susceptibility Testing of Mycobacterium tuberculosis against Pyrazinamide Using Wild-Type MIC Distributions and pncA Gene Sequencing. Antimicrobial Agents and Chemotherapy. 2012;56(3):1253–7. 10.1128/AAC.05894-11 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118. Watcharasamphankul W, Houpt ER, Foongladda S. Rapid detection of pyrazinamide resistant Mycobacterium tuberculosis by high resolution melting curve analysis. Journal of the Medical Association of Thailand = Chotmaihet thangphaet. 2013;96(9):1218–23. [PubMed] [Google Scholar]
- 119. Napiorkowska A, Ruesch-Gerdes S, Hillemann D, Richter E, Augustynowicz-Kopec E. Characterisation of pyrazinamide-resistant Mycobacterium tuberculosis strains isolated in Poland and Germany. International Journal of Tuberculosis and Lung Disease. 2014;18(4):454–60. 10.5588/ijtld.13.0457 [DOI] [PubMed] [Google Scholar]
- 120. Ghiraldi LD, Campanerut PAZ, Spositto FLE, Sato DN, Leite CQF, Hirata M, et al. Evaluation of the microscopic observation drug susceptibility assay for detection of Mycobacterium tuberculosis resistance to pyrazinamide. Clinical Microbiology and Infection. 2011;17(12):1792–7. 10.1111/j.1469-0691.2011.03508.x [DOI] [PubMed] [Google Scholar]
- 121. Shenai S, Rodrigues C, Sadani M, Sukhadia N, Mehta A. Comparison of phenotypic and genotypic methods for pyrazinamide susceptibility testing. The Indian journal of tuberculosis. 2009;56(2):82–90. [PubMed] [Google Scholar]
- 122. Li H, Chen J, Zhou M, Geng X, Yu J, Wang W, et al. Rapid Detection of Mycobacterium tuberculosis and Pyrazinamide Susceptibility Related to pncA Mutations in Sputum Specimens through an Integrated Gene-to-Protein Function Approach. Journal of Clinical Microbiology. 2014;52(1):260–7. 10.1128/JCM.02285-13 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 123. Pholwat S, Stroup S, Gratz J, Trangan V, Foongladda S, Kumburu H, et al. Pyrazinamide susceptibility testing of Mycobacterium tuberculosis by high resolution melt analysis. Tuberculosis. 2014;94(1):20–5. 10.1016/j.tube.2013.10.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 124. World Health Organization; Multidrug and extensively drug-resistant TB (M/XDR-TB): 2010 global report on surveillance and response. Geneva, Switzerland: WHO press; 2010. [Google Scholar]
- 125. Zumla A, Memish ZA, Maeurer M, Bates M, Mwaba P, Al-Tawfiq JA, et al. Emerging novel and antimicrobial-resistant respiratory tract infections: new drug development and therapeutic options. The Lancet Infectious Diseases. 2014(0). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 126. Chang KC, Yew WW, Zhang Y. Pyrazinamide Susceptibility Testing in Mycobacterium tuberculosis: a Systematic Review with Meta-Analyses. Antimicrobial Agents and Chemotherapy. 2011;55(10):4499–505. 10.1128/AAC.00630-11 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 127. Miotto P, Cabibbe AM, Feuerriegel S, Casali N, Drobniewski F, Rodionova Y, et al. Mycobacterium tuberculosis pyrazinamide resistance determinants: a multicenter study. MBio. 2014;5(5):e01819–14. 10.1128/mBio.01819-14 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 128. Zimic M, Sheen P, Quiliano M, Gutierrez A, Gilman RH. Peruvian and globally reported amino acid substitutions on the Mycobacterium tuberculosis pyrazinamidase suggest a conserved pattern of mutations associated to pyrazinamide resistance. Infection Genetics and Evolution. 2010;10(2):346–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 129. Somoskovi A, Dormandy J, Parsons LM, Kaswa M, Goh KS, Rastogi N, et al. Sequencing of the pncA gene in members of the Mycobacterium tuberculosis complex has important diagnostic applications: Identification of a species-specific pncA mutation in "Mycobacterium canettii" and the reliable and rapid predictor of pyrazinamide resistance. Journal of Clinical Microbiology. 2007;45(2):595–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 130. Almeida Da Silva PE, Palomino JC. Molecular basis and mechanisms of drug resistance in Mycobacterium tuberculosis: classical and new drugs. Journal of Antimicrobial Chemotherapy. 2011;66(7):1417–30. 10.1093/jac/dkr173 [DOI] [PubMed] [Google Scholar]
- 131. Linger Y, Kukhtin A, Golova J, Perov A, Lambarqui A, Bryant L, et al. Simplified Microarray System for Simultaneously Detecting Rifampin, Isoniazid, Ethambutol, and Streptomycin Resistance Markers in Mycobacterium tuberculosis . Journal of Clinical Microbiology. 2014;52(6):2100–7. 10.1128/JCM.00238-14 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 132. Streicher EM, Maharaj K, York T, Van Heerden C, Barnard M, Diacon A, et al. Rapid Sequencing of the Mycobacterium tuberculosis pncA Gene for Detection of Pyrazinamide Susceptibility. Journal of clinical microbiology. 2014;52(11):4056–7. 10.1128/JCM.02438-14 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 133. Zhang Y, Permar S, Sun ZH. Conditions that may affect the results of susceptibility testing of Mycobacterium tuberculosis to pyrazinamide. Journal of Medical Microbiology. 2002;51(1):42–9. [DOI] [PubMed] [Google Scholar]
- 134. Fonseca LdS, Marsico AG, Vieira GB, Duarte RdS, Saad MH, Mello FdC. Correlation between resistance to pyrazinamide and resistance to other antituberculosis drugs in Mycobacterium tuberculosis strains isolated at a referral hospital. Jornal brasileiro de pneumologia: publicacao oficial da Sociedade Brasileira de Pneumologia e Tisilogia. 2012;38(5):630–3. [DOI] [PubMed] [Google Scholar]
- 135. Singh P, Wesley C, Jadaun GPS, Malonia SK, Das R, Upadhyay P, et al. Comparative evaluation of Lowenstein-Jensen proportion method, BacT/ALERT 3D system, and enzymatic pyrazinamidase assay for pyrazinamide susceptibility testing of Mycobacterium tuberculosis . Journal of Clinical Microbiology. 2007;45(1):76–80. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
(PDF)
Abbreviations: MDR-TB, multi-drug resistant tuberculosis; PZA, pyrazinamide; TB, tuberculosis; WHO, World Health Organization; lab, laboratory; N/A, not applicable; N/S, not stated; HR-MDR, high-risk multi-drug resistant tuberculosis; MTB, Mycobacterium tuberculosis; PCR, polymerase chain reaction, East Med, Eastern Mediterranean.
(PDF)
Abbreviations: A, adenine; bp, base pair; C, cytosine; del, deletion; G, guanine; R, resistant; SNP, single-nucleotide polymorphism; T, thymine. * Article found one isolate sensitive and one isolate resistant.
(PDF)
Data Availability Statement
All relevant data are within the paper and its Supporting Information files.