

Abstract
Effective interventions targeting comorbid obesity and depression are critical given the increasing prevalence and worsened outcomes for patients with both conditions. RAINBOW is a type 1 hybrid design randomized controlled trial. The objective is to evaluate the clinical and cost effectiveness and implementation potential of an integrated, technology-enhanced, collaborative care model for treating comorbid obesity and depression in primary care. Obese and depressed adults (n=404) will be randomized to usual care enhanced with the provision of a pedometer and information about the health system’s services for mood or weight management (control) or with the Integrated Coaching for Better Mood and Weight (I-CARE) program (intervention). The 12-month I-CARE program synergistically integrates two proven behavioral interventions: problem-solving therapy with as-needed intensification of pharmacotherapy for depression (PEARLS) and standardized behavioral treatment for obesity (Group Lifestyle Balance™). It utilizes traditional (e.g., office visits and phone consults) and emerging care delivery modalities (e.g., patient web portal and mobile applications). Follow-up assessments will occur at 6, 12, 18, and 24 months. We hypothesize that compared with controls, I-CARE participants will have greater improvements in weight and depression severity measured by the 20-item Depression Symptom Checklist at 12 months, which will be sustained at 24 months. We will also assess I-CARE’s cost-effectiveness and use mixed methods to examine its potential for reach, adoption, implementation, and maintenance. This study offers the potential to change how obese and depressed adults are treated—through a new model of accessible and integrative lifestyle medicine and mental health expertise—in primary care.
Keywords: Depression, obesity, randomized controlled trial, problem solving therapy, standard behavioral treatment, lifestyle change
1. Introduction
Effective interventions targeting comorbid obesity and depression are critical given the increasing prevalence and worsened outcomes for patients with both conditions.1 Obesity affects 36% of women and men in the United States (US)2 and is an independent risk factor for major chronic diseases such as type 2 diabetes mellitus and cardiovascular disease.3,4 Similarly, depression is associated with increased risks of these chronic diseases5 and is a leading cause of disability worldwide.6,7 Lifetime risk of major depressive disorder (MDD) is 20% in US women and 13% in men, and the 12-month prevalence is 8.6% and 4.9%, respectively.8,9 Moreover, over their lifetime, 4% of the US general adult population meets the criteria for a chronic depressive disorder.10 Mounting epidemiologic evidence1,11 has shown a bidirectional relationship between obesity and depression, especially in women. Prospective studies also reveal that the obesity-depression relationship is temporally reciprocal, i.e., baseline obesity predicting later depression and vice versa.12–14 Not only are obesity and depression associated with the same health complications (e.g., type 2 diabetes mellitus and cardiovascular disease), but their coexistence exerts synergistic adverse effects on treatment adherence and response for both conditions.15–17
Thus, adults who are both obese and depressed are a growing population of great public health concern and should be a prime target for clinical interventions to prevent type 2 diabetes mellitus and cardiovascular disease. Some studies suggested the potential benefits of behavioral interventions in obese and depressed adults.18–21 Although proven treatments exist for obesity and depression separately, there is currently a limited evidence base about how to treat them in concert in ways that are effective and practical in primary care settings, where most people seek and receive care.
The RAINBOW (Research Aimed at Improving Both Mood and Weight) trial was designed to evaluate the clinical and cost effectiveness and implementation potential of an integrated, technology-enhanced, collaborative care model for treating obese and depressed adults in primary care. This paper describes the study design and methodology.
2. Methods
2.1. Study Design
RAINBOW is a 2-arm randomized controlled trial in which patients ≥18 years of age with comorbid depression and obesity will be randomized to receive usual care alone or combined with an integrated treatment for the two coexisting disorders, the “Integrated coaching for better mood and weight (I-CARE)” intervention. All study procedures and materials have been approved by the Institutional Review Board for the Palo Alto Medical Foundation (PAMF). The study uses an effectiveness-and-preliminary-implementation (Type 1 hybrid) design, aimed at testing intervention effectiveness while gathering information on its potential for implementation in real-world settings.22 Framed within the Reach, Effectiveness, Adoption, Implementation, and Maintenance (RE-AIM) model, the specific aims focus on outcome and process evaluations.
Aim 1. Determine the clinical and cost effectiveness of I-CARE vs. usual care
Hypothesis 1. Compared with controls, I-CARE participants will achieve greater mean reductions in body mass index (BMI) and Depression Symptom Checklist-20 (SCL-20) score at 12 months, which are the study’s co-primary endpoints.
Hypothesis 2. Mean BMI and SCL-20 scores will remain significantly lower (improved) at 24 months (i.e., 12 months post-treatment) in I-CARE participants compared to controls.
Hypothesis 3. The I-CARE intervention will be cost-effective within 2 years and over a projected longer term compared to usual care, based on the ratio of incremental direct medical and nonmedical costs (estimated from health system and societal perspectives) to incremental benefits (measured by quality-adjusted life years gained).
Aim 2. Examine I-CARE’s potential for reach, adoption, implementation, and maintenance
A mixed methods approach utilizing detailed process data will be used to examine RE-AIM attributes other than effectiveness: reach (e.g., patient participation rate and reasons for refusal), adoption (e.g., characteristics of participating clinics and providers), implementation (e.g., fidelity of a multi-faceted strategy to support intervention delivery within the trial: standard coach training, co-located psychiatric-medical supervision, structured audit and feedback, and external and internal expert facilitation), and maintenance (e.g., expected setting-level sustainability based on post-trial surveys and interviews with stakeholders).
2.2. Eligibility Criteria
Participants will be recruited from multiple medical centers of PAMF, which is a large community-based multispecialty group practice in Northern California. Patients ≥18 years of age who are obese and depressed will be eligible to participate (Table 1). Those with significant medical (e.g., type 2 diabetes mellitus or cardiovascular disease) or psychiatric comorbidities (e.g., psychotic or bipolar disorders) or special lifestyle circumstances (e.g., pregnancy or planned relocation) will be excluded. Women and men of any racial or ethnic background who speak English, meet the inclusion criteria, and have no exclusion criteria will be enrolled.
Table 1.
Inclusion and exclusion criteria
| Pre-screening (Electronic health record data) |
PCP Clearance | Screening (Patient reports by phone or online) |
Baseline Visit (In-person interview, physical exam and, if clinically indicated, study physician clearance) |
|
|---|---|---|---|---|
| Inclusion Criteria: (patients will be included if meeting all of the following) | ||||
| Ethnicity: All ethnic groups | √ | |||
| Gender: Both men and women | √ | |||
| Age: ≥18 years | √ | |||
| Body mass index ≥30.0 kg/m2 (non-Asians) or ≥27.0 kg/m2 (Asians) | √ | √ | ||
| Clinically significant depression PHQ-9 ≥10 | √ | |||
| PAMF patient for ≥1 year and seen in primary care at least once in the preceding 24 months | √ | |||
| Able and willing to enroll and provide written, informed consent, i.e., to: meet the time and data collection requirements of the study; be randomized to one of two intervention arms; participate in follow-up for 24 months; and allow extraction of relevant information from their medical records. | √ | |||
| Exclusion Criteria: (patients will be excluded if meeting any of the following) | ||||
| Active suicidal ideation per PHQ-9 interview that includes active plan and/or intent (item #9 ≥2) | √ | √ | ||
| Any Axis I disorder other than Minor or Major Depressive Disorder and/or Dysthymia, with the exception of any comorbid Anxiety Disorder | √ | √ | ||
| Active Bulimia Nervosa within the past 3 months (however Binge Eating Disorder without purging is not an exclusionary condition) | √ | √ | ||
| Active alcohol or substance use disorder (including prescription drugs) | √ | √ | √ | |
| Ongoing psychiatric care with a provider outside of PAMF | √ | |||
| Had bariatric surgery within the past 12 months or plan to undergo bariatric surgery during the study period | √ | √ | √ | |
| Pre-existing diabetes (other than during pregnancy) | √ | √ | √ | √ |
| Pre-existing cardiovascular disease: e.g., coronary heart disease (myocardial infarction, angina pectoris, percutaneous coronary intervention, and coronary artery bypass graft surgery), cerebrovascular disease (stroke, transient ischemic attack), peripheral vascular disease, heart failure, or aortic aneurysm. | √ | √ | √ | √ |
| Diagnosis of cancer (other than non-melanoma skin cancer) that is/was active or treated with radiation or chemotherapy within the past year | √ | √ | √ | |
| Severe medical comorbidities that require aggressive treatment, e.g., stage 4 or greater renal disease, liver failure | √ | √ | √ | |
| Diagnosis of a terminal illness and/or residence in a long-term care facility | √ | √ | ||
| Cognitive impairment based on the Callahan 6-item screener | √ | |||
| Inability to speak, read or understand English | √ | √ | √ | √ |
| Having no reliable telephone service, or no regular Internet access via a computer and/or mobile device (e.g., smartphone)* | √ | |||
| Plan to move out of the area or transfer care outside PAMF during the study period | √ | |||
| Currently pregnant, lactating, or planning to become pregnant during the study period | √ | √ | √ | √ |
| Already enrolled, or planning to enroll, in a research study that would limit full participation in the study or confound the observation and interpretation of the study’s findings | √ | |||
| Family/household member of another participant or of a staff member | √ | √ | ||
| Investigator discretion for clinical safety or protocol adherence reasons | √ |
We do not employ a behavioral run-in for technology use (typical in efficacy trials) as an inclusion criterion because of the importance of balancing scientific rigor and generalizability in this type 1 hybrid design RCT. It is an integral part of the intervention curriculum that the coach instructs on, and helps troubleshoot issues with, technologies (e.g., MyFitnessPal and Fitbit websites and mobile applications) used in the intervention, as would be expected if the intervention were delivered in routine practice.
2.3. Recruitment and Screening
The target sample size of 404 eligible and consenting participants will be enrolled over a 2-year period. Recruitment and screening will proceed in 5 steps (Table 1). First, PAMF patient electronic health records (EHRs) will be pre-screened to identify potential participants meeting basic eligibility criteria (e.g., age, BMI, time with PAMF, and absence of exclusionary medical or psychiatric comorbidities). Second, primary care providers (PCPs) will review lists of potentially eligible patients, exclude those they deem inappropriate for the study because of medical reasons, and authorize study contact for the rest. Third, patients will be mailed or emailed study invitations that contain a web link for the study screening form that patients can complete on their own or with research staff over the phone. Research staff will begin calling patients 2 weeks after the invitations are sent. Fourth, patients who screen eligible must complete the baseline assessment consisting of a self-administered online questionnaire and an in-person examination visit. Finally, a study physician will review patients’ EHRs to confirm final eligibility before randomization. Based on the demographics of obese and depressed patients seen in primary care at PAMF, the gender and minority racial/ethnic composition of the target enrollment population is estimated to be 64% female, 10% non-Hispanic black, 18% Hispanic/Latino, and 44% Asian.
2.4. Randomization and Blinding
A staff person not involved in outcome assessments or data analysis will perform randomization using a web-based system23 that we developed and have used successfully in several trials.24,25 Participants will be randomly assigned in a 1:1 ratio to the usual care control group or the I-CARE intervention group. The web-based randomization program uses Pocock’s minimization, a covariate-adaptive method,26,27 to achieve better than chance marginal balance between study arms across multiple baseline characteristics: clinic, gender, age, race/ethnicity, education, BMI, SCL-20 score, therapeutic class of antidepressant medication taken, and number of hospitalization. The system’s computational algorithm automatically adjusts the randomization probability based on the characteristics of all the previously randomized participants, thus minimizing the total covariate imbalance between arms after each new patient is randomized. Efron’s biased-coin method28 is applied to protect allocation concealment with the use of non-extreme randomization probabilities (2/3:1/3). Specifically, for each patient about to be randomized, the system automatically calculates an imbalance score for each of the above-mentioned baseline covariates, and then a total imbalance score, S, by summing across the covariates. If S = 0, the randomization probability for receiving the intervention for that patient will be set to ½, and if S < 0 (S > 0), the randomization probability will be set to 2/3 (1/3).
By design, treatment assignments are identifiable to participants and the lifestyle coach, but the investigators, data and safety monitoring board members, outcome assessors, and data analyst will be blinded throughout the trial. Further, the lifestyle coach will be masked to all outcome measures obtained by outcome assessors during blind assessments.
2.5. Continuation of Usual Care
We will recruit from patients who have used PAMF for routine care for at least 1 year and thus have a higher likelihood of an established relationship with their PCP. During informed consent, patients will be clearly instructed that they should continue to receive any medical care (e.g., depression and weight control care) as usual. For patient safety and generalizability, no standard care will be withheld at any time from participants once enrolled, regardless of treatment assignment. They will be advised to consult with their PCP about their conditions. PCPs will be free to prescribe medications or refer patients for mental health and/or obesity consultation, and patients will be free to seek care in the community. All participants will receive information on PAMF health and wellness classes and programs relating to mood and weight, as well as a Fitbit ZIP™ wireless activity tracker.
To retain the integrity of usual care, PCPs will not be told which of their patients are enrolled in the study and in which treatment group if enrolled. They will only identify which of their patients are in the I-CARE intervention if and when they are contacted by the study care team to make antidepressant medication changes. We anticipate the number of I-CARE participants per PCP to be small considering we will be recruiting at multiple large PAMF primary care clinics.
Based on our prior primary care-based trials, we anticipate low rates of changes in concomitant therapy for depression or obesity in usual care within the 12-month intervention period. In the TEAMcare study,29 the number of antidepressant medication initiations and/or adjustments in the TEAMcare intervention (3.37; 95% CI, 2.92–3.89) was 6.2 times (P <.001) that of usual care (0.53; 0.34–0.82) over 12 months. In the 15-month E-LITE trial,24 no one had drug or surgical treatment for obesity; 15 of the 81 (19%) usual care controls used a nonstudy weight-loss program (13 in a commercial program and 2 in a routine class at the clinic), compared to 5 of the 79 (6%) coach-led and 3 of the 81 (4%) self-directed participants (all used a commercial program) (P = 0.003).
As we have done in those trials, from the EHR we will determine PCP orders and referrals throughout the trial period for intervention and control participants. We will also survey participants about any programs or products that they may have used on their own to treat depression or obesity during the trial. We will conduct secondary analyses using data on out-of-study treatments to elucidate their potential confounding effects on the primary intention-to-treat findings.
2.6. Intervention
Participants in the control group will receive no intervention from the study. Participants in the I-CARE group will complete a 12-month integrated intervention for comorbid obesity and depression.
2.6.1. Integrated collaborative care
The I-CARE intervention integrates the essential components of the Diabetes Prevention Program-based Group Lifestyle Balance™ (GLB) program for weight loss and cardiometabolic risk reduction24,30,31 with the PEARLS program32,33 for collaborative stepped depression care, which uses Problem Solving Therapy (PST) combined with behavioral activation as first-line, intensified with stepwise increases in doses and number of antidepressant medications as needed. Both programs are nationally recognized and provide standard coach training and support.34,35 We have shown the effectiveness of both programs separately in our previous trials.24,31–33,36–38 In this study, we innovatively integrate them for the treatment of adults with comorbid obesity and depression in primary care.
2.6.2. Synergistic conceptual models for behavior change
The GLB program is based on Social Cognitive Theory,39 which emphasizes a triadic, reciprocally deterministic relationship between the individual, environment, and behavior. Social Cognitive Theory recognizes that behavior change is a dynamic process that moves at variable speed through stages of readiness to change. Positive outcome expectancies through realistic goal setting and guided action planning are associated with initiation of behavior change, and self-efficacy developed for specific behaviors (e.g., self-weighing, dietary change and physical activity) predict establishment and maintenance of behavior change. Social Cognitive Theory suggests that self-efficacy is enhanced through social support and gradual mastery of self-regulation skills (e.g., self-monitoring, action planning, and problem solving).39
The PST for depression has important overlap with the GLB as follows: both (1) are based on cognitive and behavioral models of behavioral change; (2) involve goal setting and action planning; (3) require monitoring of specific targets from week to week; (4) assign home activities to be done between sessions; (5) incorporate problem solving and relapse prevention; (6) are interactive treatment methods that actively engage participants; and (7) recognize the value of engaging with support from a lifestyle coach to accomplish these goals. Because both interventions share common cognitive and behavioral principles, it is expected that patients can focus on applying familiar skills to behavior change for both improved depression and weight loss simultaneously. Thus, participants are likely to transition between the PST and GLB programs smoothly. The sequential, overlapping combination of PST and GLB programs is also expected to be synergistic in that patients who have gained new behavior change skills using PST will probably be more likely to benefit from the GLB program and vice versa, thereby reinforcing improved outcomes for both disorders.
2.6.3. Intervention format, structure and content
The 12-month I-CARE intervention has an intensive phase and a maintenance phase.
2.6.3.1. Format
Delivered by a trained lifestyle coach, I-CARE begins with a 6-month intensive phase including 9 one-on-one clinic visits of 60 minutes each, and 11 home-viewed 20–30 minute GLB videos and self-study activities, followed by phone calls at least once a month for 15–30 minutes during the 6-month maintenance phase (Table 2). The I-CARE trained lifestyle coach will conduct the visits and phone calls, and additionally can communicate with patients via the secure EHR patient portal throughout the intervention. Throughout the intervention, participants will be asked to wear a study-provided Fitbit pedometer, log their weight on Fitbit website or mobile application (“app”), and log minutes of physical activity and dietary intake using MyFitnessPal website or app. Each participant will set up an online user account for Fitbit and one for MyFitnessPal, and share them with the lifestyle coach as a “friend.” Fitbit pedometers interface with the personal computer or Fitbit app on a mobile device to automatically and wirelessly upload a participant’s daily steps into the person’s Fitbit account. Participants will manually enter their weights, minutes of physical activity, and foods consumed into their accounts on a computer or through the mobile apps. Once friended the lifestyle coach will be able to view participant’s self-tracked data, monitor their progress, and use it to facilitate individualized coaching.
Table 2.
| Week | Visitc | Minutes | Content |
|---|---|---|---|
| 1 | 1 | 60 |
|
| 2 | 2 | 60 |
|
| 3 | 3 | 60 |
|
| 4 | 4 | 60 |
|
| 6 | 5 | 60 |
|
| 8 | 6 | 60 |
|
| 12 | 7 | 60 |
|
| 16 | 8 | 60 |
|
| 20 | 9 | 60 |
|
| 21–52 | Phone | 15–30 |
|
In-between session support as needed via EHR secure email, between weeks 1–52.
Co-located psychiatric and medical supervision during weekly intervention management team meeting, between weeks 1–52.
The 9 one-on-one I-CARE sessions will occur primarily in the clinic, but video conferences (as the second option) or phone sessions (as the last option and for visits 1–5, phone session is only an option upon PI and intervention manager approval) throughout the intensive phase will be an option for participants with considerable constraints.
I-CARE Mood is the PEARLS program; I-CARE Lifestyle is the GLB program.
Participants receive Fitbit, MyFitnessPal, and My Health Online instructions via mail or e-mail prior to first session.
2.6.3.2. Structure, content, and curriculum
The PEARLS intervention for depression begins with PST at the first one-on-one visit and the GLB program is introduced in the fifth visit during week 6 (Table 2). PST teaches participants problem-solving skills using a structured 7-step method and workbook-style paper materials. Within the first 3–4 sessions, participants are typically able to begin utilizing the method by themselves to form action plans for behavior change. Over the remaining sessions, problem-solving skills are augmented and reinforced but no new content is delivered. During the first 5 visits, the lifestyle coach will also instruct participants on, and help troubleshoot issues with, the use of secure email via the EHR-integrated patient portal, MyFitnessPal, and Fitbit, all of which are accessible online or via Android- and iPhone-compatible apps.
During the fifth I-CARE visit (week 6), participants will receive the in-home GLB core program materials, including self-directed videos and a workbook. The lifestyle coach will review the content from 11 out of the 12 core GLB video sessions (excluding the problem solving session due to overlap with PST) during visits 6 through 9. During the maintenance phase, post-core GLB print materials (which are included in the workbook) will be discussed during each phone encounter.
Throughout the 12-month intervention, the coach will practice problem solving skills with participants and provide between-session support via EHR-embedded secure email. The coach will provide lifestyle counseling following the GLB program on weight management, healthy eating, and physical activity after GLB is introduced. The coach and participant will develop a maintenance plan once targeted depression and weight loss goals (or a personal maximum achievable level of improvement) are reached for at least 1 month, and a relapse prevention plan when the participant is nearing the end of the 12-month intervention. Coach contact will cease after 12 months, although participants will be followed through 24 months in order to assess intervention durability and cost-effectiveness.
2.6.4. Psychiatric and medical supervision of lifestyle coach and medication management support for PCPs
Rather than a separate care manager providing care for each illness in primary care systems, which may be prohibitively expensive, a lifestyle coach who is cross-trained using the standardized GLB34 and PEARLS35 training protocols will provide integrated coaching for comorbid obesity and depression, under the supervision of a study psychiatrist and a study physician who are identified from among local PAMF providers. After each one-on-one visit, the coach will document patient progress on key intervention tracking parameters (e.g., date and content; most current Patient Health Questionnaire-9 [PHQ-9] score; pedometer steps; self-reported weight and minutes of physical activity) in the EHR—viewable by all providers on the patient’s care team to facilitate care coordination. Working together as a study care team, the coach will meet for 2 hours each week with the study psychiatrist, study physician, and intervention manager. They use an online tracking database to view each participant’s progress for ongoing case management. The form will include a flag for cases not meeting pre-defined progress milestones for depression (e.g., compared to visit 1, PHQ-9 score <25% decrease by week 4; another <25% decrease by week 8; or PHQ-9 score >5 or <50% decrease by week 12), weight loss (e.g., <3% decrease by week 12; <5% decrease by week 20), and for physical activity (e.g., <150 minutes/week of moderate-intensity physical activity or <8000 steps per day by week 12). Each week the coach and supervisors will discuss new and flagged cases (5–10 minutes of discussion per case). The study psychiatrist and physician will provide psychiatric and medical advice to the coach during case review meetings, but they will not directly interact with intervention participants. Consistent with stepped care strategies, for patients with unremitting depression symptoms the supervising psychiatrist will recommend antidepressant medication changes, according to the study medication protocol (Appendix A), taking into account potential medical or substance abuse etiologies. The psychiatrist communicates her recommendations via secure EHR staff messaging to PCPs who, as treating physicians, will be responsible for prescribing the recommended antidepressant medications. PCPs may consult the study psychiatrist if they have questions about any recommended medication changes. The coach will monitor condition status, coordinate communication between the supervising psychiatrist and the patient’s PCP regarding medication changes, and help problem solve barriers to medication adherence during scheduled visits.
2.7. Participant Safety
Participants will be carefully screened using a multistep enrollment process, and individuals for whom the intervention is deemed medically inappropriate or unsafe will be excluded. The study physician will review medical charts of all the participants after baseline assessments and before randomization. During screening women who are pregnant, lactating, or planning to become pregnant during the study period will be excluded. If a participant becomes pregnant during the study, she will be excluded from further participation in all study activities, and her PCP will be notified. Participants who are diagnosed with any other exclusionary condition (e.g., coronary heart disease, stroke, diabetes, and cancer) following randomization may continue in the trial with approval of the study physician. Established alert levels (e.g., for high blood pressure) and alert conditions (e.g., suicidality, angina, and peripheral vascular disease) will help ensure that participants are referred for further evaluation and therapy when clinically indicated. The PHQ-9 and the SCL-20 will be used to assess suicidal risk. Study staff will follow the self-harm protection protocol (Appendix B) if a participant responds “2” (“more than half the days”) or “3” (“nearly every day”) to item 9 of the PHQ-9 or responds “3” (‘quite a bit”) or “4” (“extremely”) to item 2 of the SCL-20.
To ensure unbiased ascertainment between the intervention and control group, outcome assessors will systematically screen all participants for adverse events during in-person assessments at baseline, 6, 12, 18, and 24 months using a standard interview and reporting form as done in our previous trials.25,30,40 Positive response will be recorded and then reviewed by the study safety officer for seriousness, study relatedness, and expectedness. An adverse event is defined as any untoward medical or psychological event experienced by a patient during or as a result of his/her participation in the study that represents a new symptom or an exacerbation of an existing condition, whether or not considered study related based on appropriate medical judgment. Documentation in EHR will be used to verify patient self-reports. Adverse events discovered outside these planned evaluations (e.g., during intervention encounters) will be duly noted and followed up with, as needed, to assure participant safety. We will report adverse events according to the data and safety monitoring plan (Appendix C).
2.8. Retention
As we have done in our previous trials,24,25,30,40 we will implement a series of strategies to minimize loss to follow-up: (1) careful staff selection and standardized training in trial-specific protocols, rapport building, motivational interviewing, and problem solving as appropriate to their study roles; (2) legally adequate, effective informed consent; (3) education of participants about the importance of follow-up assessments regardless of treatment adherence; (4) prudent participant incentives (e.g., pedometer, cash incentives of $20) and flexible scheduling (outside of work hours, multiple locations); (5) promotion of study “brand” identity with a logo and a website; (6) ongoing monitoring of recruitment and retention; (7) up-to-date participant contact information and two emergency contacts; (8) diligent efforts to re-engage inactive participants; and (9) alternative means of obtaining measurements.
2.9. Study measures and data collection schedule (Table 3)
Table 3.
List of measures and data collection schedule.
| Study Measures | Instrument | Collection Method | Month
|
|||||
|---|---|---|---|---|---|---|---|---|
| Screening | 0 | 6 | 12 | 18 | 24 | |||
| Eligibility Screening | ||||||||
| Depression severity | Patient Health Questionnaire-9 (PHQ-9 and Dysthymia questions) | Self-report | x | |||||
| Suicidal ideation | PHQ-9 (item #9 ≥2) | Self-report | x | |||||
| Bulimia nervosa | PHQ eating disorder module | Self-report | x | |||||
| Alcohol/substance abuse | CAGE Adapted to Include Drugs (CAGE-AID) | Self-report | x | |||||
| Cognitive Impairment | 6-item Screener | Interview | x | |||||
| Primary/Secondary Outcomes | ||||||||
| BMI (height) | Height | Biophysical | x | |||||
| BMI (weight) | Weight | Biophysical | x | x | x | x | x | |
| Depression severity treatment response, and remission | Depression symptom Checklist-20 (SCL-20) | Self-report | x | x | x | x | x | |
| Cardiovascular risk factors | Blood pressure, waist circumference | Biophysical | x | x | x | x | x | |
| Obesity-specific health related questions | Obesity-related Problem Scale | Self-report | x | x | x | x | x | |
| Anxiety | Generalized Anxiety Disorder Scale (GAD-7); Panic Disorder module of the Mini-International Neuropsychiatric Interview (MINI) | Self-report | x | x | x | x | x | |
| Disability | Sheehan Disability Scale | Self-report | x | x | x | x | x | |
| Generic health related quality of life | SF-8 Health Survey | Self-report | x | x | x | x | x | |
| Utility based quality of life | EuroQOL-5D-5L | Self-report | x | x | x | x | x | |
| Direct medical costs, direct nonmedical costs | Health care utilization: from electronic health record (EHR); intervention cost: coach time, survey lifestyle coach for Intervention process accounting, intervention-related patient “out-of-pocket” costs. | EHR; process documentation; self-report | x | x | x | x | x | |
| Absenteeism-Presenteeism questionnaire | Self-report | x | x | x | x | x | ||
| Participant Expense Survey | Self-report | x | x | x | x | x | ||
| Medication use, general wellness services, and out of network health care utilization questionnaire | Interview | x | x | x | x | x | ||
| Potential effect modifiers | ||||||||
| Sociodemographics | Age, gender, education, race/ethnicity | Self-report | x | |||||
| Posttraumatic stress disorder (PTSD) | 17-item PTSD checklist – Civilian Version (PCL-C) | Self-report | x | |||||
| Potential effect mediators | ||||||||
| Dietary intake | 24-hr diet recalls | Interview | x | x | x | x | x | |
| Physical activity | 7-day Physical Activity Recall | Interview | x | x | x | x | x | |
| Problem solving | Social Problem-Solving Inventory-Revised: Short Form | Self-report | x | x | x | x | x | |
| Sleep habits and quality | PROMIS Sleep Disturbance and Sleep Impairment Scales | Self-report | x | x | x | x | x | |
| Safety | ||||||||
| Activity | Rose Angina and Peripheral Vascular Disease Questionnaires | Self-report | x | x | x | x | x | |
| Severe high or low blood pressure | Blood pressure | Biophysical | x | x | x | x | x | |
| Adverse Events (AE) | AE form | Interview | x | x | x | x | x | |
| Self-harm risk | SCL-20 suicidality item | Self-report | x | x | x | x | x | |
2.9.1. Primary outcomes
The co-primary outcomes are changes in BMI and SCL-20 score at 12 months. BMI will be calculated based on height and weight measured per standard protocols.41 The SCL-20 is a valid, reliable measure of depression severity.42,43 It has been used in numerous depression treatment trials in primary care and community settings,32,33,37,38 making it particularly useful for cross-study comparisons and data synthesis in meta-analyses.
2.9.2. Secondary outcomes
BMI and SCL-20 score at 24 months will be secondary outcomes. Additional secondary outcome measures will include depression treatment response (>50% decline in SCL-20 score from baseline) and remission (SCL-20 score <0.5), waist circumference and resting blood pressure according to standardized protocols,41 and the following measures at 12 and 24 months:
Obesity-specific problems
The Obesity-Related Problem Scale specifically measures the impact of obesity on psychosocial functioning. The 8-item scale has high internal reliability and sound test–retest reliability, correlates strongly with a wide range of theoretically related constructs, and is responsive to weight loss intervention.44
Anxiety
Anxiety will be measured with the Generalized Anxiety Disorder Scale (GAD-7) and the Panic Disorder module of the Mini-International Neuropsychiatric Interview (MINI). GAD-7 is a valid and reliable 7-question scale for screening generalized anxiety disorder and strongly associated with multiple domains of functional impairment.45 The MINI has high validity and reliability scores;46 and in the present study we will specifically use module E to screen for panic disorder.
Disability
The Sheehan Disability Scale is a validated questionnaire that measures functional disability and is sensitive to treatment effects in clinical trials.47 Patients rate the extent to which they symptoms impair work/school, social, and family life on a visual analog scale from 0 to 10 and answer the number of days when their symptoms cause them to miss work/school and be unproductive at work/school.
Quality of life
Quality of life will be measured with the Short Form-8 Health Survey (SF-8) and Euro-QoL 5D. The SF-8 is an 8-item version of the SF-36 that measures overall health-related quality of life.48 Euro-QoL 5D (EQ-5D-5L) include 5 domains (mobility, self-care, usual activities, pain and discomfort, and depression and anxiety) scored on 5 levels (no, slight, moderate, severe, or extreme problems) and current health rated on a visual analogue scale from 0 to 100. It has been shown to be a valid and reliable tool to measure utility based quality of life.49 Values from the EQ-5D-5L instrument will be used to calculate quality-adjusted life years that are used to inform incremental benefits of the I-CARE intervention relative to control.
Costs
These include direct medical costs and direct nonmedical costs. Direct medical costs will include the costs of identifying eligible patients, providing the intervention, addressing side effects, and health care utilization. Direct nonmedical costs will include intervention-related “out-of-pocket” costs (e.g., value of participant time spent on intervention activities). We will obtain authorization from patients for extraction of EHR data on health care utilization (e.g., office visits, in-patient stays, procedures, medications, laboratory tests). We will also interview participants about their medication use (with the aid of containers of regularly-taken medication brought by participants to the visits), general wellness service use, and out of network health care utilization. Also, we will survey the coach and patients using adapted resource utilization and cost capture instruments based on the Diabetes Prevention Program and Diabetes Prevention Program translation trials.50,51
2.9.3. Potential effect modifiers and mediators
To complement the primary and secondary findings, we will explore for whom and under what condition (effect modifiers) and how (mediators) treatment effects occur. Data will be collected on measures of potential moderators (e.g., gender, age, race/ethnicity, education, posttraumatic stress disorder) and mediators (e.g. dietary intake, physical activity, problem solving, and sleep quality) responses to the intervention. Posttraumatic stress disorder (PTSD) will be measured with the 17-item PTSD checklist – Civilian Version that has high reliability and validity.52 Participants’ dietary intake will be assessed by multiple-pass 24-hour diet recalls,53 the gold-standard dietary assessment method. Physical activity will be measured using Stanford 7-day Physical Activity Recall, which is a reliable measure that is sensitive to change in physical activity.54 Participants’ problem solving skills will be assessed using the reliable and valid Social Problem-Solving Inventory-Revised: Short Form that contains 25 items in the following five scales: positive problem orientation, rational problem solving, negative problem orientation, impulsive/careless style, and avoidance style.55 Sleep quality will be measured with the 8-item PROMIS sleep disturbance and sleep impairment scales short forms.56
2.9.4. Process measures
As in an effectiveness-and-preliminary-implementation (Type 1 hybrid) design, we will use mixed methods to collect process measures that will provide a nuanced understanding of why the intervention is (or is not) more effective than usual care, whether high intervention fidelity is achieved, what barriers and enablers there are, how these may translate into real-world implementation, and what modifications can be made to maximize implementation success.22 We will frame the process evaluation around the RE-AIM framework (Table 4). In addition to focusing on effectiveness, RE-AIM examines the reach, adoption, implementation, and maintenance of the program, and any barriers or enablers in each of these domains.57,58 We will conduct survey and interview different stakeholders, including participants, recruitment staff, study care team, internal experts (study physician advisors), PCPs, and medical and administrative leaders at participating clinics, at multiple time points throughout the trial period.
Table 4.
Summary of Quantitative and Qualitative Measures for the Process Evaluation
| RE-AIM Domains | Example Questions, Data Sources, and Methods | |
|---|---|---|
| Quantitative | Qualitative | |
| Reach | Using patient survey and recruitment tracking data we will assess the percentage and characteristics of participants compared to non-participants, e.g., by soliciting demographic information from potential participants and reasons for screening refusal or ineligibility. | We will ask study staff at the beginning, mid-point, and end of the 2-year recruitment period: What were the barriers to and enablers of recruiting participants? Was there variability in these factors related to demographics or other characteristics? How were the barriers addressed? Were the solutions successful? What could be changed to maximize reach? |
|
| ||
| Adoption | Using administrative data we will describe the characteristics of participating clinics, and the percentage and characteristics of PCPs approached that participated (e.g., PCPs referring patients for screening or making recommended antidepressant medication changes). | Via interviews with internal experts, PCPs, and medical and administrative leaders we will ask: What were the barriers to and enablers of clinic and PCP participation? Why did the barriers exist? What recommendations do they have for addressing barriers and maximizing adoption? |
|
| ||
| Implementation (staff perspective) | Using intervention tracking data we will assess time and resources required for coach training, intervention delivery, coach supervision, and fidelity assurance. | Via interviews with study care team, internal experts, PCPs, and medical and administrative leaders we will ask: What were the barriers to and enablers of delivering the intervention, and were they different across participating clinics? How might these factors translate or not to real-world implementation? Were certain components more challenging to deliver than others? What modifications could be made to maximize real-world implementation? |
|
| ||
| Implementation (patient perspective) | Using intervention tracking data we will assess participants’ receipt of and adherence to the intervention, e.g., by monitoring the number of in-person sessions, phone calls and DVD sessions completed, reasons for missed sessions, secure email and self-monitoring frequency, and consistency of adherence across participant subgroups. | Via interviews with a 10% random sample of intervention participants we will ask: How relevant and acceptable were the knowledge and skills gained? How often did they practice the intervention strategies? What were the perceived benefits? What problems did they encounter? How satisfied were they with program format, materials, and coach performance? |
|
| ||
| Maintenance | Using follow-up data through 24 months we will assess attrition rates and adverse events by participant characteristics and treatment condition; the durability of intervention effects on depression, obesity, and health-related quality of life; and simulation model-based projections of cost-effectiveness within trial and long term. | Via interviews with study care team, internal experts, PCPs, and medical and administrative leaders we will ask: How could the intervention be integrated into regular care and sustained after the study ended? What resources, policies, and care process redesigns would be needed to maximize sustainability? |
In addition to qualitative evaluation through surveys and interviews, we will also collect data on the screening process, e.g., the proportion and representativeness of the patients who are eligible at initial and subsequent screenings, reasons for exclusion, and demographics of patients who screen ineligible or decline participation. We also will assess the proportion and representativeness of physicians willing to approve screening of their potentially eligible patients, patient retention rates, and the representatives of patients who complete follow-up assessments and reasons for dropout.
Intervention exposure and adherence measures will include attendance at one-on-one visits, reasons for missed visits, frequency of self-monitoring records and secure emails, self-reported completion of in-home videos, and number of completed counselling phone calls. Self-monitoring data obtained during intervention program will be used for adherence monitoring and for the coach to use in tailoring feedback for individual participants.
2.10. Statistical Analysis
2.10.1. Analytic plan
Repeated-measures mixed-effects linear (for continuous outcomes) or logistic models (for categorical outcomes) using intention-to-treat tests of group by time interactions will evaluate between-group differences in primary (Aim 1, Hypotheses 1 and 2) and secondary outcomes. The fixed effects of each model will include the baseline value of the outcome of interest, randomization balancing factors, group, time point, and group-by-time interaction indicators. The models will account for the non-independence of repeated measures using a covariance structure within participants to be determined by the least Bayesian Information Criterion and clustering of patients within primary care providers. Maximum likelihood estimation in mixed modeling will be used for missing data. We will document the extent and pattern of missing data and the reasons, and will conduct sensitivity analyses of the impact of missing data (e.g., with multiple imputation,59–61 on stability of the primary results). Models will be adjusted for nonlinearity and/or unequal variances based on residuals from a model using residual plots. Polynomial terms may be included if indicated. Appropriate transformation of the outcome variable (e.g., logarithmic) will be considered as a remedy for unequal variances. Also, the model could be altered to a heterogeneous variance model if participants in different intervention arms are found to have different variances. We will verify that mixed model-based results are not sensitive to violations of model assumptions with permutation and bootstrap resampling tests.62,63
Mediation analyses will explore changes in potential putative mediators (e.g. problem solving, antidepressant medication change, physical activity, dietary intake, sleep quality) and their effects on treatment response. Using MacKinnon’s product of coefficients test (αβ)64 we will examine longitudinal and contemporaneous mediation separately. Longitudinal mediation refers to changes in mediators from baseline to 6 months followed by change in BMI and/or SCL-20. Contemporaneous mediation refers to changes in mediators and change in BMI and/or SCL-20 from baseline to 12 months. Asymmetric confidence limits will be constructed based on the distribution of the product with the PRODCLIN program. Because multicollinearity may be present in a multiple mediator model, we first will test each mediator separately in a single-mediator model. Next, multiple-mediator models will be used to test for independent and suppression effects when all variables found to be at least marginally significant in the single-mediator models are entered simultaneously. To determine the extent of mediated effect, the percentage of total effect mediated will be calculated for each significant mediator as αβ/(αβ + γ), where γ is the direct intervention effect on outcome.
Moderation analyses will explore differences in intervention effect by potential subgroups (e.g., according to gender, age, race/ethnicity, and education). These analyses will follow the same general analytic approach as described above for primary and secondary outcomes, with the inclusion of appropriate moderator main effects and moderator-by-group interaction terms.
Cost-effectiveness analyses (Aim 1, Hypothesis 3) will extend and combine existing models for obesity and depression that we and others have developed.65–70 We will compare incremental costs, estimated from the perspectives of health systems (direct medical costs only) and society (direct medical and non-medical costs), to incremental benefits, expressed as quality-adjusted life years gained. We will also consider the number needed to treat as an important and clinically-relevant outcome and estimate the intervention cost per number needed to treat. The use of quality-adjusted life years allows for comparisons of both changes in morbidity and health status as well as mortality effects based on change in the risk of death and, among survivors, reduction in quality of life due to nonfatal events, given the probabilities of disease progression in the target population.68,71 We will convert Cohen’s d effect sizes to estimates of the number needed to treat to have one more patient with better outcomes in the intervention arm vs. usual care.72 We will exclude from all analyses research-related costs, such as costs of recruitment, screening, and outcome surveillance that are beyond those recommended for routine clinical practice. Intervention start-up costs, fixed costs of sustaining the intervention, and marginal costs of adding additional participants to the intervention will be differentiated because they are relevant for different decisions: whether to implement the intervention in the first place and whether to sustain or expand it over time. We will use simulation models, similar to those in Diabetes Prevention Program and Sequenced Treatment Alternatives to Relieve Depression,68,73,74 to analyze incremental cost-effectiveness ratios during the trial and projected into 5-, 10-, 20-, 30-year, and lifetime horizons. Cost-utility estimates with different time horizons will be useful for stakeholders deciding on program implementation. Sensitivity analyses will be performed and results will be interpreted according to standard guidelines.75–77
We will analyze quantitative process data using standard tests, e.g., Student’s t-tests and χ2 tests for continuous and categorical variables, respectively (Aim 2). We will use NVivo to analyze all qualitative data.78 Two independent and trained researchers will code all qualitative data separately by stakeholder group (e.g., participants, recruitment staff, study care team, internal experts, PCPs, and medical and administrative leaders) using principles of content analysis.79 Codes will be developed based on the RE-AIM domains assessed. Quantitative process data and qualitative data will be combined to draw conclusions about reach, adoption, implementation, and maintenance of the intervention.80
2.10.2. Sample size and data interpretation
The trial with 202 participants per arm has 90% power to detect a standardized mean difference of 0.35 (Cohen’s d) in the primary endpoints of BMI and SCL-20 scores at 12 months between the intervention and usual care group at α=5% (2-sided), assuming at least 85% retention at 12 months based on prior trial experiences.32,33,38,81,82 We used a t-test with simplified assumptions to estimate power, whereas actual power likely will be greater due to increased efficiency associated with repeated-measures mixed models with baseline and covariate adjustments.83 Because treatment success will be judged on both (not either) primary outcomes, multiplicity adjustment is unnecessary.84 No multiplicity adjustment will be made for secondary analyses, which are intended to complement the primary findings and to inform future research. They will be interpreted within that context, considering the totality of evidence available.84,85
We chose a d of 0.35 as the minimum important between-group difference based on our prior studies and other available literature. Previously, we observed a standardized mean difference of 0.46 between usual care and the GLB weight loss intervention being tested in the current trial. This corresponded to a mean of 5.0% vs. 2.6% weight loss over 15 months.24 Weight loss of ≥5% is widely regarded clinically significant,86 while a weight change of <3% defines weight maintenance.87 Hence, the net BMI lowering effect of the intervention relates to the minimal clinically important difference in weight reduction. A meta-analysis of behavioral weight-loss studies reported effect sizes of 0.61–0.67 for improvements in depression and self-esteem.88 The d effect sizes in the PEARLS trials ranged from 0.35–0.74.32,33 Further, the National Institute for Clinical Excellence in the U.K. defines a threshold of clinical significance for depression treatment as a standardized effect size of 0.50.89
2.11. Quality Control
2.11.1. Data management
Study data will be entered into computerized databases including the following: (1) Microsoft Access for recruitment and intervention tracking data; (2) REDCap90 hosted at the PAMF Research Institute for self- and interviewer-administered questionnaire data and physical measurements; and (3) the Nutrition Data System for Research (NDS-R) (Minneapolis, MN) licensed for data collection and nutrient analysis based on multiple-pass 24-hour diet recalls.91,92 These databases employ automatic, real-time range, logic, and missing value checks, as applicable. Also, the outcome assessors are trained on data collection protocols (e.g., multiple-pass 24-hour diet recall using NDS-R and 7-day physical activity recall), and their performance is continuously monitored. All datasets will be cleaned, verified and archived, and then read into SAS (version 9.2; SAS Institute Inc, Cary, NC) datasets, which also will be archived. One official copy of all study data and a master data dictionary will be maintained and updated regularly. All analytic and tracking databases will be stored in a password-protected, encrypted network drive with continuous backups. For the protection of participant confidentiality, unique anonymous study IDs will be used for data storing, tracking and reporting. Protected health information will be stored separately from all other study data, and will be used and disclosed in accordance with the Health Insurance Portability and Accountability Act regulations. Regular reports will be produced on (1) patient accrual and follow-up completion/retention in relation to goals and timeline; (2) the randomization process and group comparability on the balancing variables; (3) key baseline characteristics of the sample, by (blinded) group, related to the primary and secondary outcome variables and proposed effect modifiers and mediators; (4) intervention exposure and adherence; and (5) protocol violations. Any observed delays in these processes or data irregularities will be followed up and resolved in a timely manner.
2.11.2. Intervention fidelity
Following recommendations for behavioral intervention studies,93 we will standardize intervention materials and provide rigorous coach training and oversight to ensure intervention fidelity. All one-on-one sessions and phone calls will be audiotaped, and a random sample of at least 10% will be reviewed and rated for protocol adherence using a structured rating scale. The lifestyle coach will follow a structured framework for composing secure emails, which will be sampled for periodic review as part of routine quality control efforts. The coach will complete a checklist of critical intervention behaviors and materials delivered during one-on-one sessions, and document the frequency, duration, and purpose of phone and email communications. These records will be subject to periodic reviews using standardized evaluation forms. If a coach scores below an a priori performance standard, she will receive more frequent audit and feedback and “booster” training if necessary.
To monitor and support participants’ receipt of and adherence to the intervention, the coach will review and give feedback on homework and self-monitoring records and document participants’ mastery of protocol-specific, achievement-based objectives. The coach will routinely inquire about barriers to treatment receipt and adherence, recommend problem-solving strategies, and provide ongoing support using motivational interviewing techniques.94
3. Discussion
Research on integrated therapy in comorbid obesity and depression is lacking. One randomized controlled trial by Linde and Simon et al. tested the efficacy of an intensive intervention with 203 obese and depressed women in a primary care setting that combined behavioral weight-loss and cognitive-behavioral depression treatments into 26 group visits over 1 year, compared with behavioral weight-loss treatment alone for the same number of sessions.20 There were no significant differences between groups at 12 months for weight or depression symptoms measured by SCL-20.20 Pagoto et al. completed an efficacy trial in 161 obese women with major depressive disorder who were treated sequentially with behavioral activation therapy for depression followed by behavioral weight-loss treatment, or received behavioral weight-loss treatment only. Both study arms involved 26 weekly individual and group sessions during a 6-month intensive phase, and 6 group and 10 phone sessions during 18 months of maintenance.95 At 12 months (primary endpoint), the two groups did not differ in weight loss, but sequential treatment led to greater improvement in Beck Depression Inventory-II scores.21 Participants with better depression treatment response and remission lost greater weight regardless of random assignment. Simon’s and Pagoto’s efficacy trials tested high-intensity behavioral interventions (≥26 in-person visits in 1 year), included women only, and neither used team-based multicondition collaborative care involving as-needed stepped treatment intensification with antidepressant medications.38,96,97 The findings of these trials reinforce a critical need for alternative comorbidity treatment models that can be integrated within primary care and better engage obese and depressed patients, thereby enhancing effectiveness and generalizability.
The current study uniquely adapts and integrates the GLB video program for weight loss with the PEARLS program for collaborative stepped depression care. The intervention incorporates conventional clinic- and home-based modes of care delivery (e.g., office visits plus phone consults and in-home video), and leverages low-cost, wide-reach health information technologies (e.g., web, secure email, and mobile apps). Using an effectiveness-and-preliminary-implementation (Type 1 hybrid) design,22 this is the first study to test the clinical and cost effectiveness and implementation potential of combining these two proven, nationally recognized programs to treat obese and depressed adults in primary care. The in-depth process evaluation data collected from different stakeholders will not only strengthen the interpretation of primary findings, but also provide important contextual and experiential information to inform researchers, policy makers, health system administrators, clinicians, and patients about the potential for future dissemination and implementation. Furthermore, our study psychiatrist and physician are practicing clinicians in the health system where this study is being conducted. Although a lifestyle coach is to be hired and paid by the study to conduct the intervention, we will purposely select candidates in health professions that are typical in the primary care workforce (e.g., health educators and registered dietitians). Coach training for the study can be readily scaled in future dissemination and implementation of the intervention if warranted by findings from this study. Both GLB and PEARLS programs are nationally recognized and provide standard coach training and support.
This study leverages two proven behavioral interventions in ways that are practical and likely to have a synergistic therapeutic effect on two prevalent and commonly coexisting chronic conditions, obesity and depression. In turn, this could help prevent long-term complications of these conditions, such as type 2 diabetes mellitus, cardiovascular disease, and dementia.3,15,17,98 If successful, this study will offer the potential to change how obese and depressed adults are treated using an integrated multicondition collaborative care model in primary care.
Acknowledgments
The project described is supported by Award Number R01HL119453 from the National Heart, Lung and Blood Institute and internal funding from the Palo Alto Medical Foundation Research Institute. JGF is supported in part by NIH/NIA K01AG037593-01A1. VY is supported in part by NIDDK K23DK097308. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Heart, Lung and Blood Institute or the National Institutes of Health. No sponsor or funding source has a role in the design or conduct of the study; collection, management, analysis or interpretation of the data; or preparation, review or approval of the manuscript.
The authors dedicate this work to the deceased Wayne Katon, MD, who contributed significantly to the conception and design of the RAINBOW study. The authors extend special thanks to RAINBOW participants and their families who make this study possible. The authors also thank the study physician advisors (Meg Durbin, MD, Ed Yu, MD, and Bahar Aghighi, MD), the study Data and Safety Monitoring Board members (William Haskell, PhD, Mickey Trockel, MD, Sandra Tsai, MD, and Manisha Desai, PhD), and the study team members who have made substantial contributions to the conduct of the study (Veronica Luna, BS, Andrea Blonstein, MBA, RD, Elizabeth Jameiro, MD, Nancy Wittels, MS, Elizabeth Ward, MD, and Lenard Lesser, MD, MSHS).
Investigators at Palo Alto Medical Foundation Research Institute, the University of Washington, and the University of Pittsburgh collaborated to create the RAINBOW I-CARE intervention, which integrates adaptations of the Program to Encourage Active, Rewarding Lives for Seniors and the Group Lifestyle Balance™ Program. The University of Washington and the University of Pittsburgh provided training and support for RAINBOW study staff at Palo Alto Medical Foundation Research Institute.
Appendix A. Study Medication Protocol
I-CARE Treatment of Depression with Medications
A. Initiating Antidepressants
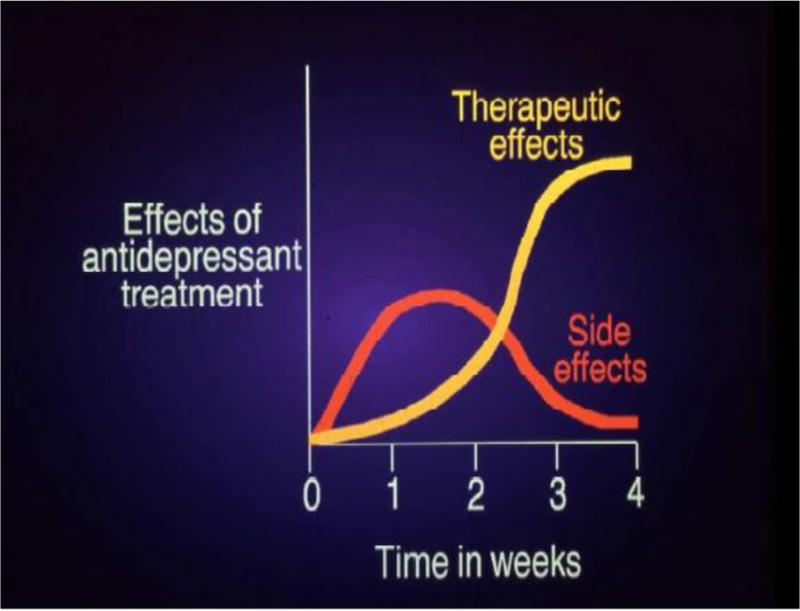
When starting patients on antidepressants, they need to understand that side effects can occur before the medication’s therapeutic effects help them to feel better. It is helpful to draw the figure below for patients, illustrating that side effects peak in the first 1–2 weeks and then subside, whereas therapeutic effects often peak at 3–4 weeks. This figure can prevent patients from getting discouraged prematurely and discontinuing medications.
B. Antidepressant Side Effects
Short-Term Side Effects
These occur within the first several weeks and include jitteriness, insomnia, headache, and nausea, and other side effects that may be idiosyncratic to the individual patient. These symptoms are usually lessened by starting antidepressants at a low dose and increasing the dose weekly. Short-term side effects usually disappear within 2–3 weeks.
Long-Term Side Effects
-
▪
Diarrhea is particularly common with sertraline (Zoloft), but can occur with other SSRIs or with bupropion (Wellbutrin). Changing to a low dosage of paroxetine (Paxil) at 5–10 mg and titrating upward by 5–10 mg every 7–10 days to a dosage of 20–50 mg may help because paroxetine (Paxil) has slight anticholinergic effects.
-
▪
Sexual dysfunction can occur in up to one third of patients receiving selective serotonin reuptake inhibitors (SSRIs), such as fluoxetine. It is important to ask about sexual function, since many patients with diabetes already have problematic sexual functioning. The most common sexual side effect is delayed orgasm or inability to experience orgasm. Patients can be switched or cross-tapered to bupropion SR if they experience this side effect on an SSRI. The addition of bupropion SR 100 mg twice a day or buspirone 15 mg twice a day to an SSRI regimen also often alleviates sexual dysfunction.
-
▪
Sleep problems continue to occur in approximately 25–33% of patients despite effective SSRI treatment. For people bothered by insomnia, trazodone could be prescribed, starting at 25 mg at bedtime and increasing the dose by 25 mg increments every 5 days until insomnia is successfully treated.
-
▪
Weight gain, a significant problem for many people with type 2 diabetes, is worsened for 5–10% of SSRI-treated patients. Paroxetine is the SSRI that has the most weight gain associated with it. Because bupropion and fluoxetine are not associated with weight gain, these antidepressants are good first choices for overweight people.
C. Choice of Antidepressant
For patients already taking an anti-depressant at a sub-therapeutic dose, the first treatment action step is to titrate up the antidepressant dosage. All titrations should be done slowly, on a weekly basis, until PHQ-9 score goals are achieved: either < 5 or a decrease of half the baseline total score.
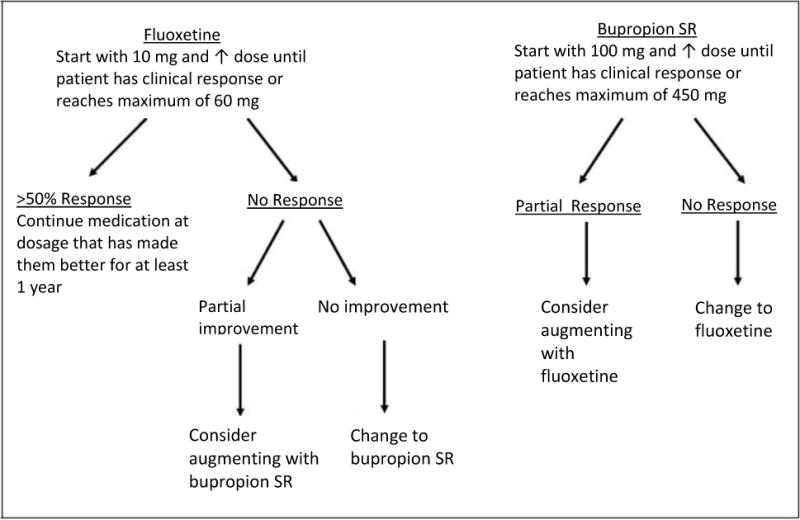
For patients who have never taken antidepressants, fluoxetine or bupropion SR are good first-line antidepressant choices due to lack of weight gain with these medications. Initiation and titration are shown in the schematic below.
Patients who have tried one SSRI unsuccessfully in the past can be switched to either a second SSRI, bupropion SR, or venlafaxine XR.
Patients with coexisting anxiety can usually be effectively treated by starting on citalopram or sertraline.
Patients with moderate to severe neuropathy may be treated with either venlafaxine XR, duloxetine, or bupropion SR. These medications have been shown in randomized controlled trials in non-depressed individuals to reduce neuropathic pain.
Patients with pre-existing sexual dysfunction can usually be successfully treated with bupropion SR. While other antidepressants are likely to worsen problems with sexual response, initiating treatment with bupropion SR may improve function. Adding an antidepressant such as bupropion SR or an anti-anxiety agent such as buspirone to an SSRI can also help sexual function in patients with diabetes and may be viewed very positively. The TCM should work with the consulting psychiatrist when carrying out antidepressant augmentation strategies.
D. Strategies for Overcoming Common Issues with Taking Antidepressants
A variety of strategies may help patients take antidepressants, including:
-
▪
Provide rationale for use.
-
▪
Pay vigorous attention to side-effects.
-
▪
Counter demoralization, fear of dependence, and loss of control.
-
▪
Enlist family/spousal support.
-
▪
Elicit resistance and relationship to prior experience with medication.
-
▪
Identify relevant illness aspects (phobic, paranoid).
-
▪
Increase contact with brief phone check-ins.
-
▪
Give specific instructions (take regardless of symptom change, don’t stop on own).
-
▪
Use symptom scale PHQ-9 to chart progress.
Depression Goal: PHQ-9 < 5 OR at least 50% decrease from baseline in PHQ-9
TCM to encourage patient to fill out PHQ-9 weekly until reaches a “steady state”, then prn.
TCM to discuss behavioral activation methods, medication adherence strategies, rationale for initial and long-term maintenance therapy with antidepressants (e.g., don’t decrease dose or stop without checking with TCM or PCP; take regardless of symptoms), and side effects (most disappear at 2 weeks).
TCM to contact PCP and team psychiatrist if patient has: acute suicidal symptoms, psychotic symptoms, manic symptoms, severe lack of appetite with insufficient oral intake or weight loss, suspected alcohol or drug misuse, or severe medication side effects.
Create My Better Health Plan initially and update at each visit.
ANTIDEPRESSANT MEDICATION
_____ Fluoxetine 10 mg/day × 1 week; then 20mg/day × 1 week. If PHQ-9 hasn’t decreased by 50% or more, increase to 30mg/day. At week 4, if PHQ-9 hasn’t decreased by 50% or more, increase to 40mg/day. Can increase fluoxetine up to a maximum of 60 mg/day as needed/tolerated.
_____ If two or more negative SSRI trials or for those patients with preexisting diabetes-related sexual dysfunction, start Bupropion SR 100mg/day for 1 week; then 100mg 2×/day for a week; then 200mg in am & 100mg in pm. If PHQ-9 at 4 weeks isn’t decreased by 50%, increase dose to 200mg BID.
_____ If patient doesn’t fit above criteria, or has significant medical or psychiatric symptoms, antidepressant medications to be suggested by CAREteam consulting psychiatrist or PCP.
| Antidepressant Medications | ||||
|---|---|---|---|---|
| Drug | Starting dose | Usual Dose | Indications | Side Effects |
| Starting antidepressants: improvement often seen in first two weeks. If not seen by 8 weeks, likely needs new agent or second agent. Check in at least weekly when starting antidepressants. 3/3 of people with depression will improve with antidepressants. | ||||
| Stopping antidepressants: Recurrence of depression is common. 64% of patients with depression had a recurrence 10 years after stopping their antidepressants. If patients do decide to stop their antidepressants, encourage them to talk with their PCP prior to stopping and help them understand that there are fewer problems when antidepressant dosages are tapered over a two week period. | ||||
| Selective serotonin reuptake inhibitors (SSRIs) | ||||
| Citalopram (Celexa) | 10 | 20–40 | Max FDA daily recommended dose for patients >60 yrs old is 20 mg | Jitteriness, restlessness, agitation, GI distress, nausea, diarrhea, insomnia usually improve in 2 weeks. Weight gain for some patients. |
| Fluoxetine (Prozac) | 10 | 20–60 | First line (weight gain less likely) | |
| Fluvoxamine (Luvox) | 50 | 50–300 | ||
| Paroxetine (Paxil) | 20 | 20–60 | Worst for sexual dysfunction, weight gain, sedation; mild anticholinergic effects (helps diarrhea) | Same as above. |
| Paroxetine CR (Paxil CR) | 25 | 25–75 | Same as above. | |
| Sertraline (Zoloft) | 50 | 50–200 | Same as above. | |
| Dopamine-norepinephrine reuptake inhibitors | ||||
| Bupropion SR (Wellbutrin SR) **When dose > 100 mg give bid. |
100 | 300–400 | Weight gain rare. May improve sexual functioning. Useful for lethargic patients. | Contraindicated in patients with seizure history or eating disorders. |
| Serotonin-norepinephrine reuptake inhibitors (SNRIs) | ||||
| Venlafaxine XR (Effexor XR)— **When dose > 75 mg, give bid. |
37.5, 75 & 100 | 75–300 | Effective for diabetic neuropathy, fibromyalgia, chronic pain. | |
| Duloxetine (Cymbalta)— | 30 | 60–120 | Effective for diabetic neuropathy, fibromyalgia, chronic pain. | |
| Serotonin modulators | ||||
| Trazodone (Desyrel) | 25–50 | 50–300 | Useful for insomnia associated with depression/anxiety. | Doses > 50 mg can cause orthostatic hypotension or (rarely) priapism. |
| Tricyclics and tetracyclics | ||||
| Amitriptyline (Elavil) | 25–50 | 100–300 | Anticholinergic side effects and weight gain. Elders particularly susceptible to memory change, confusion, hallucinations, sedation and orthostatic hypotension. Contraindicated in patients with recent MI, cardiac conduction problems |
|
| Amoxapine (Asendin) | 50 | 100–400 | ||
| Clomipramine (Anafranil) | 25 | 100–250 | ||
| Maprotiline (Ludiomil) | 50 | 100–225 | ||
| Doxepin (Adapin, Sinequan) | 25–50 | 100–300 | ||
| Imipramine (Tofranil) | 25–50 | 100–300 | ||
| Desipramine (Norpramin) | 50 | 100–300 | ||
| Nortriptyline (Pamelor) | 25 | 50–200 | ||
| Protriptyline (Vivactil) | 10 | 15–60 | ||
| Noradrenergic and specific serotonergic antidepressant | ||||
| Mirtazapine (Remeron) | 15 | 15–45 | Causes weight gain in 50% of patients. Helpful for anxious patients with insomnia and no appetite. | |
Appendix B. RAINBOW Self-harm Protection Protocol
Rationale
The Patient Health Questionnaire-9 (PHQ-9) has a question regarding self-harm risk. If a participant reports frequently contemplating suicidal ideation (“more than half the days” or “nearly every day” over the last 2 weeks), a clinical response is indicated. The Symptom Checklist (SCL-20) questionnaire also has a question regarding self-harm risk. If a participant reports frequently contemplating suicidal ideation (“quite a bit” or “extremely” over the past 2 weeks), a clinical response is indicated.
This protocol includes two self-harm protection procedures: one for participants self-screening online and the other for research staff conducting the telephone (e.g., during phone screening or intervention phone consult) or in-person (e.g., during a baseline or follow-up assessment or intervention visit) interviews.
The research staff conducting the telephone or in-person interviews are non-clinicians.
Current suicidal ideation is the only interview finding that clearly requires further clinical assessment and possible intervention.
- This protocol refers to self-harm risk responded to an online self-screening (PHQ-9 only), telephone or in-person interview (PHQ-9 or SCL-20) as follows:
-
-Responding “2” (“more than half the days”) or “3” (“nearly every day”) to the PHQ-9 question – “Over the last 2 weeks, how often have you been bothered by thoughts that you would be better off dead or thoughts of hurting yourself in some way?”
-
-Responding “3” (‘quite a bit”) or “4” (“extremely”) to the (SCL-20) question – “Overall in the past 2 weeks how much were you distressed by thoughts of ending your life?”
-
-
Either question can be endorsed at several different time points. The PHQ-9 is administered during online self-screening or phone screening by a research associate, and during every in-person or phone intervention sessions. The SCL-20 is completed at the clinic during baseline and follow-up assessments (6, 12, 18, and 24 months).
Procedures
A. For participants self-screening online
- During the online self-screening, if a participant responds “2” (“more than half the days”) or “3” (“nearly every day”) to the PHQ-9 question “Over the last 2 weeks, how often have you been bothered by thoughts that you would be better off dead or thoughts of hurting yourself in some way?” the participant will be shown the following instructions:
- “Please note: we do not monitor this screener in real time; if this is an emergency call 911.
- For more immediate attention, because you have been bothered by thoughts that you would be better off dead or of hurting yourself in some way in the last 2 weeks, you should call your physician or other healthcare professional right away, or go to the emergency room.
- You may also call the National Suicide Hotline at 800-SUICIDE/800-784-2433 or the National Suicide Prevention Lifeline at 800-273-TALK/800-273-8255. The helplines are available 24 hours every day.
- We will have a study clinician contact you within 1–2 days. In the meantime, do not delay seeking medical attention.”
The research staff will generate daily reports (except for weekends and holidays) on any positive suicidality responses from the newly completed PHQ-9s since the last report. The research staff will follow the following procedural steps based on the participant’s answers to screening questions and should not attempt to perform any independent assessment of self-harm risk.
If positive suicidality responses are identified, the research staff will contact the study psychiatrist via a high priority staff message in EPIC. The study psychiatrist is licensed and has clinical privileges at PAMF. The study psychiatrist will notify the research staff of receipt of message within 24 hours; otherwise staff will call to confirm receipt. The assessment request and study psychiatrist’s follow-up attempts and actions will be documented in the study Safety Monitoring Database.
If the study psychiatrist is not available, the research staff will send a high priority staff message in EPIC to the participant’s PCP or covering physician (using the dot phrase *) requesting that he/she contact the patient and enter an urgent mental health referral into EPIC as deemed appropriate. The PCP or covering physician may in addition schedule a follow up appointment with the patient as deemed appropriate.
The study psychiatrist will attempt to contact the participant as soon as possible (within 1–2 days) to conduct a PHONE assessment of current suicidal ideation for level of lethality and need for further referral. This assessment will be based on characteristics of suicidal patients (low-, moderate-, or high-risk) and clinical strategies for managing suicidal patients at these different thresholds. These strategies could include prompt emergency intervention by a licensed mental health professional when the immediate suicide risk is high and the participant has refused other interventions.
-
If there is an IMMINENT/HIGH risk of harm, including but not limited to: an active plan to harm oneself or another person, grave disability impacting the participant’s ability to care for him/herself or severely impairing participant’s judgment and/or without reasonable supportive resources, then the study psychiatrist will ask for participant’s location and advise the participant that she is obligated to take immediate action to get help for the participant. The study psychiatrist will call 911, giving participant’s name, date of birth, location, medical conditions and current risk factors and notify any immediate family member or emergency contact if relevant.
The study psychiatrist will check study database to see whether patient is an I-CARE participant.- For enrolled I-CARE participants, the study psychiatrist will contact the study health coach via phone or confidential email, who will contact the participant weekly thereafter (unless currently hospitalized) to complete the PHQ-9 (until patient’s PHQ-9 score <5, or score decreases by 50%), assess progress, and coordinate patient’s follow up care with the study psychiatrist. The study psychiatrist will also send a staff message to inform patient’s PCP of this action (dot phrase **).
- For patients excluded from enrollment, or enrolled control participants, the study psychiatrist will send a high priority staff message in Epic (dot phrase**) to inform participant’s PCP or covering physician of the action of calling 911 and give potential resources for follow up following hospitalization. The PCP may in addition choose to call or schedule a follow up appointment with the patient as deemed appropriate.
- If there is MODERATE RISK of harm, with the participant having significant symptoms, but able to tend to basic needs, expressing willingness to get help, possibly having suicidal thoughts but denying an active suicidal plan:
- For enrolled I-CARE participants, the study psychiatrist will contact the study health coach, via phone or confidential email, who will contact the participant weekly thereafter by phone to complete the PHQ-9 (until patient’s PHQ-9 score <5, or score decreases by 50%), assess progress, and assist participant with follow-up. The study psychiatrist will send a staff message to inform patient’s PCP of this action. The study psychiatrist will be available as needed to consult with the health coach and the participant’s PCP.
- For patients excluded from enrollment, or enrolled control participants, The study psychiatrist will send a high priority staff message in Epic (using the dot phrase ***) to inform participant’s PCP or covering physician of follow up plan.
- If there is LOW RISK of harm, with participant denying suicidal or homicidal thoughts, able to carry out basic activities of daily living, with reasonable social supports and agreeable to getting help:
- For enrolled I-CARE participants, the study psychiatrist will staff message the study health coach who will contact the participant weekly thereafter to complete the PHQ-9 (until patient’s PHQ-9 score <5, or score decreases by 50%), assess progress, and coordinate the patient’s follow up care with the study psychiatrist. The study psychiatrist will send a staff message to inform patient’s PCP of this action.
- For patients excluded from enrollment, or enrolled control participants, the study psychiatrist will send a staff message in Epic (using the dot phrase ****) to inform participant’s PCP of follow up plan.
The study psychiatrist in scenarios 6–8 above will complete a study Self-Harm Risk Clinician Assessment Form that is part of the study Safety Monitoring Database.
B. PROCEDURES for telephone or in-person interviews with research staff
During telephone or in-person interviews with research staff, if a participant’s response suggests suicidal ideation on PHQ-9 or SCL-20 per definition in Rationale #5, the interviewer will ask “Do you have a plan for how you would commit suicide?”
If yes, the interviewer stop the interview, get the participant’s location (if phone interview), let the participant know that you are concerned for his/her safety and therefore need to call for help, and call 911 immediately. You do NOT need participant’s consent to call 911 if you feel there is a possibility of immediate risk of harm to self or others.
If no, the interviewer will tell the participant that the study psychiatrist will contact him/her within 24–48 hours and give the participant the Resource Contact Information Form or verbally give the participant the resource contact phone numbers if interviewing participant by phone. The interviewer will then offer to continue with the interview. Before moving on, it may be helpful to acknowledge to the patient that we will continue to monitor suicidal thoughts throughout the study, as they are a fairly common symptom of depression, and part of the depressive illness itself. Also helpful to instill hope: “We will work together to get you feeling better.”
Dot Phrases for use in EPIC
RESEARCH STAFF high priority dot phrases to alert PCP or covering physician via Epic if the study psychiatrist is unavailable
*This message is to inform you that your patient recently endorsed suicidal thoughts on the PHQ-9 and/or SCL-20 while participating in the RAINBOW study.
As the study psychiatrist is not immediately available, we urge you to contact your patient and initiate an Urgent Mental Health referral in Epic if deemed appropriate.
In addition, you may choose to schedule a follow up appointment with the patient at your discretion.
-For enrolled I-CARE participants: Our health coach will contact your patient within one week and weekly thereafter to complete PHQ-9 and assess progress, consulting with the study psychiatrist as needed.
Study psychiatrist dot phrases to alert PCPs via Epic
For HIGH RISK PATIENTS
**This message is to inform you that your patient was recently assessed by the RAINBOW study psychiatrist to be at high risk for self harm based on responses to PHQ-9 and/or SCL-20. As a result, 911 has already been contacted and patient is en route to being evaluated in an emergency room setting for possible psychiatric and/or medical admission to the hospital. Appropriate family member/emergency contact has already been contacted.
-For enrolled I-CARE participants, our health coach will contact your patient within one week and weekly thereafter to complete PHQ-9 and assess progress, consulting with the study psychiatrist as needed.
For MODERATE RISK PATIENTS
***This message is to inform you that your patient recently endorsed having suicidal thoughts over the past two weeks on the PHQ-9 and/or SCL-20 and has been contacted and assessed by the RAINBOW study psychiatrist by phone.
We urge you to contact your patient and initiate an Urgent or Routine Mental Health referral in Epic as deemed appropriate.
In addition, you may choose to schedule a follow up appointment with the patient at your discretion.
-For enrolled I-CARE participants: Our health coach will contact your patient within one week and weekly thereafter to complete PHQ-9 and assess progress, consulting with the study psychiatrist as needed.
For LOW RISK PATIENTS
****This message is to inform you that your patient recently endorsed having significant depressive and/or anxiety symptoms over the past two weeks on the PHQ-9 and/or SCL-20.
For enrolled I-CARE participants, our study health coach will contact the participant within one week and weekly thereafter to complete the PHQ-9 and assess progress, consulting with the study psychiatrist as needed.
For patients excluded from enrollment, or enrolled control participants, we recommend you advise your participant who is in network to contact PA (650-853-4726) or Fremont (510-498-2942) Behavioral Health intake referral line to schedule a routine appointment with a mental health provider. If participant is out of network, we recommend that you advise he/she to contact their insurance provider for an in-network mental health provider. If neither of the above options are available, the patient should be advised to schedule an appointment with their PCP or covering physician within the next 1–2 weeks to discuss treatment options.
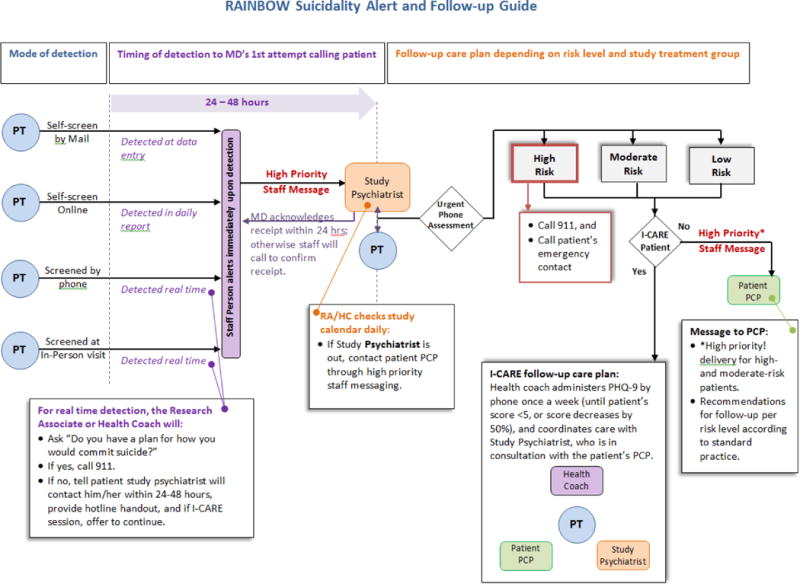
Appendix C. RAINBOW Data and Safety Monitoring Plan
The following procedures will be followed to ensure the safety of study participants and the validity and integrity of data in compliance with NIH requirements.
Functions of the Data and Safety Monitoring Board (DSMB)
We will empanel a DSMB prior to enrollment of the first study participant. A DSMB in the context of this investigator-initiated randomized controlled trial exists for the purpose of providing the investigators, the cognizant IRB(s) and the sponsor with objective, scientific monitoring of the conduct of the study from the standpoint of ensuring (1) the protection and safety of human subjects and (2) the validity and integrity of the trial. The DSMB will be an independent, advisory body to the investigators and funding agency. To fulfill its functions, the DSMB will review the original protocol and any subsequent amendments, perform expedited monitoring of serious adverse events (SAEs) that are unexpected and at least possibly related to the study, perform ongoing monitoring of drop-outs and non-SAEs, determine whether study procedures should be changed or the study should be halted because of serious safety concerns and/or major problems with the study conduct, and perform periodic review of the completeness and validity of data to be used for analysis of effectiveness and safety. The DSMB will also monitor implementation of procedures to ensure research participant privacy and data confidentiality.
As in any clinical trial, it is not possible to anticipate all possible adverse events (AEs). We will conduct extensive training with our staff in ascertaining, monitoring, and documenting AEs—serious or not. The study investigators have extensive experience in clinical trial organization and management, including data and safety monitoring for single site and multi-site trials. We have established procedures for rendering first aid and life threatening emergencies. Study physicians will oversee these procedures.
Membership of the DSMB
The DSMB will consist of 3–5 outside members (not part of the investigative team) with expertise in a variety of disciplines including mental health, biobehavioral medicine, preventive medicine, nutrition, physical activity, biostatistics, clinical trial designs, and bioethics of research conduct. In the event of an award, we will work with NIH-designated Project Official to appoint an appropriate DSMB. The expertise of the members will include the disciplines and skills needed to initially review the protocol and then to monitor trial progress, data quality, and participant safety. The voting members must have no personal stake in the scientific outcomes of the study. They will not be included as authors of publications from the study, but will be acknowledged for their contribution. The PI and Reporting Investigator (Ma) will be responsible for overseeing the preparation of AEs and SAEs and all statistical reports to the DSMB.
Functional Organization of the DSMB
One individual will serve as Chairperson of the DSMB and will communicate by e-mail and telephone conference with the other members on an as-needed basis. Communication pertaining to expedited review of unexpected and possibly study-related SAEs will occur within a week of receiving the report of such events from Dr. Ma. Reporting and communication about routine trial monitoring will occur during DSMB meetings throughout the study.
DSMB Meetings and Recommendations
The DSMB will convene every 4–6 months, in person or by conference call, with the investigators to review summaries of patient accrual, data collection, the timeliness of data transfer to analysis files, group balance and data concerning the execution of the randomization process, analysis plans and results, and the numbers and characteristics of any SAEs, and the numbers and rates of non-SAEs. At the end of each meeting, DSMB members will make a recommendation regarding the continuation of the trial and the time interval and format of the next meeting. In addition, there will be an evaluative statement regarding SAEs, protocol exceptions, and other matters of data quality, integrity of the trial, and timeliness. The DSMB’s findings and recommendations will be documented in the meeting minutes and transmitted to the investigators and sponsor for their information and action. A draft of the meeting minutes will be made available to the DSMB Chair for approval prior to distribution of a final version to other DSMB members, the funding agency, and the investigators.
Monitoring of Safety Data by the DSMB
Blinded Reporting
Safety information for this study will be reported to the DSMB by group but with the true identity of the treatment groups masked. This will maintain proper blinding of the investigators, outcome assessors, and the DSMB. However, if there are extraordinary concerns regarding patient safety, the DSMB may request unblinded data, e.g., on unexpected SAEs or unanticipated problems, in order to determine the nature and extent of toxicity of the intervention under study or the integrity of the trial conduct. When this occurs, the unblinded results will not be released to the investigators unless warranted for safety protection of the research participants.
No formal interim analyses are proposed of study outcomes by study group before primary data analyses. Follow-up data will be reported for all participants, irrespective of random assignment, during the course of the study. For purposes of study monitoring, including review of planned primary outcome analyses, the DSMB may wish to review results with permuted group assignments to test the analysis programs.
SAEs
For ongoing monitoring of this study, all SAEs will be reported to the DSMB during its regularly scheduled meetings, regardless of any judgment of their expectedness or relatedness to the study. Expedited reviews will occur for all unexpected and possibly study-related events meeting the NIH definition of SAEs, i.e., any fatal event, immediately life-threatening event, permanently or substantially disabling event, event requiring or prolonging inpatient hospitalization, or any congenital anomaly. Dr. Ma will concurrently notify the DSMB and the IRB by email within 72 business hours of the detection of an SAE requiring expedited review and will submit all relevant information about the event and a proposed corrective and preventive action plan (CAPA). The relevant information may include, but is not limited to, that about the event and its outcome, dosing history of a suspect medication/treatment, concomitant medications, the subject’s medical history and current conditions, and all relevant laboratory data. Within one week of receiving the notification, the DSMB will render their determination of the event and recommendations about the CAPA in a letter signed by the chair and transmitted by email to Dr. Ma and the IRB.
Non-SAEs
At periodic intervals, the DSMB will be provided with summaries of the numbers and rates of all AEs by blinded treatment group. “Blinded treatment group” means an arbitrary labeling (e.g., 1 and 2) that does not reveal the true identity of the groups. These reports will include types of events, affected body system(s), severity, expectedness, study relatedness, and treatment phase. Data on individual non-SAEs is not expected to be needed for this review. At the discretion of the DSMB, however, the Chair may request unblinded and/or individual-level results to determine the nature and extent of adverse consequences.
Other Safety-Related Reports
It is considered necessary for the purpose of monitoring the safety of the study that the DSMB review not only AEs and SAEs, but other data that may reflect differences in safety between treatment groups. For example, these may include treatment retention rates and reasons for drop-outs. In addition, mean (SD) changes in SCL-20 score, weight, BMI, and cardiovascular risk factors from baseline to follow-up will be reported for all participants, irrespective of random assignment, because as noted above, interim outcome analyses by group are not planned in this trial.
Study Stopping Rules
Formal stopping rules for safety, efficacy, and futility are not proposed as part of this application but may be established per recommendations of the DSMB following the funding of the grant. If at any time during the course of the study, the DSMB judges that risk to participants may significantly outweighs the potential benefit, the DSMB shall have the discretion and responsibility to request all necessary information for detailed analyses, and if warranted, recommend that the study be terminated. Stopping rules for the trial could include stopping because of a significant number of injuries or illnesses that can reasonably be attributed to participation in the study, inability to recruit and measure the required number of participants to conduct the primary outcome analyses, poor intervention quality and delivery, serious deviation from study protocols, or other circumstances that would render the study unlikely to produce scientifically valid findings. The DSMB will carefully weigh the risk of completing the trial as planned against the risk of prematurely stopping the trial for safety or futility.
Monitoring of Data Quality by the DSMB
For each DSMB meeting, Dr. Ma will submit a detailed report on data quality and completeness. At a minimum, this will include the following: (1) patient accrual and follow-up completion/retention in relation to goals and timeline; (2) the randomization process and group comparability on the balancing variables; (3) key baseline characteristics of the sample, by blinded group, related to the primary and secondary outcome variables and proposed effect modifiers and mediators; (4) indices of intervention adherence; and (5) protocol violations.
Annual Report to the sponsor
As part of each annual progress report to the NIH, Dr. Ma will include a summary of findings regarding safety and quality based on data received to that point in the study and any new DSMB recommendations about patient safety, protocol adherence, and data quality.
Protection against Depression-related Risks
Protection against risks of worsening depression and self-harm
Some of the questions about depression, thoughts of death and other psychiatric symptoms and conditions as a part of the screening may be distressing to some patients. However, in general the questions will not be particularly intrusive or distressing, and stress will likely be transient. In addition, participants are free to choose not to any questions. It is widely accepted that asking questions about thoughts of death or suicide does not lead to increased risk of suicide. Nevertheless, in the event that a patient is identified as being suicidal in the screening or follow-up phase of the study (not because of being asked questions), we have a self-harm protection protocol (below) in place that will alert the study supervising psychiatrist to assess the patient’s suicidal thoughts by telephone, followed by notification of the patient’s primary care provider and appropriate clinical action if necessary.
Protection against risk of worsening anxiety
The Generalized Anxiety Disorder 7-Item (GAD-7) Scale is a screening tool that has been developed to screen for 4 anxiety disorders: Post Traumatic Stress Disorder, Panic Disorder, Generalized Anxiety Disorder, and Social Phobia. A score of ≥10 indicates a high probability of 1 or more of these disorders. Patients with coexisting anxiety who meet all inclusion and exclusion criteria will be eligible to participate. They can usually be effectively treated by starting on citalopram or sertraline. Patients carrying a diagnosis of bipolar or psychotic disorder will not be eligible to participate. However, patients with undiagnosed anxiety disorders or panic attacks can have an exacerbation of anxiety symptoms if an antidepressant is started at therapeutic dose or if an antidepressant like buproprion is used. Patients screening positive on the GAD-7 will be asked follow-up questions to screen for panic disorder. Patients with suspected panic disorder should be discussed with a psychiatrist before starting or increasing the dosage of a patient’s planned antidepressant. SSRIs are effective treatments for both panic disorder and depression, but patients with comorbid panic should be started on lower dosages initially.
Protection against adverse reactions to antidepressant medications (ADMs)
Consistent with the stepped depression care strategies, the study supervising psychiatrist will contact PCPs of intervention participants with unremitting symptoms (e.g., PHQ-9 score remains >50% of baseline by week 10 of PST) to recommend initiating or adjusting ADMs. Health coaches will support and educate intervention participants regarding ADM management in preparation for potential recommendations by the study psychiatrist and action by their PCP.
Footnotes
Trial registration: ClinicalTrials.gov #NCT02246413
Authors’ Contribution
JM conceived the study, obtained funding, has the overall responsibility for its design and conduct, and drafted the manuscript. VY, JGF, MAL, MKK, and MBS participated in the design of the study. LX contributed to planning the statistical analyses. NL contributed to drafting the manuscript. All authors participated in critical revisions for important intellectual content.
Competing Interests
The authors declare that they have no financial, research, organizational, or other interests to disclose that are relevant to the execution of this research or this publication.
These materials were adapted with permission from Dr. Wayne Katon, Principal Investigator for the TEAMcare trial (http://www.teamcarehealth.org).
References
- 1.Faith MS, Butryn M, Wadden TA, Fabricatore A, Nguyen AM, Heymsfield SB. Evidence for prospective associations among depression and obesity in population-based studies. Obes Rev. 2011 May;12(5):e438–453. doi: 10.1111/j.1467-789X.2010.00843.x. [DOI] [PubMed] [Google Scholar]
- 2.Flegal KM, Carroll MD, Kit BK, Ogden CL. Prevalence of obesity and trends in the distribution of body mass index among US adults, 1999–2010. JAMA. 2012 Feb 1;307(5):491–497. doi: 10.1001/jama.2012.39. [DOI] [PubMed] [Google Scholar]
- 3.Nguyen NT, Nguyen XM, Lane J, Wang P. Relationship between obesity and diabetes in a US adult population: findings from the National Health and Nutrition Examination Survey, 1999–2006. Obes Surg. 2011 Mar;21(3):351–355. doi: 10.1007/s11695-010-0335-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Jokinen E. Obesity and cardiovascular disease. Minerva pediatrica. 2015 Mar;67(1):25–32. [PubMed] [Google Scholar]
- 5.Chapman DP, Perry GS, Strine TW. The vital link between chronic disease and depressive disorders. Prev Chronic Dis 2005. 2005 http://www.cdc.gov/pcd/issues/2005/jan/pdf/04_0066.pdf. Accessed June 16, 2008. [PMC free article] [PubMed]
- 6.World Health Organization. The World Health Report 2002: Reducing Risks, Promoting Healthy Life. Geneva, Switzerland: World Health Organization; 2002. [Google Scholar]
- 7.Murray JL, Lopez AD, editors. Summary: the global burden of disease. Boston, MA: Harvard School of Public Health; 1996. [Google Scholar]
- 8.Inter-university Consortium for Political and Social Research. National Comorbidity Survey Replication (NCS-R) Lifetime and Twelve-month Prevalence estimates. 2007 http://www.hcp.med.harvard.edu/ncs/index.php. Accessed June 16, 2008.
- 9.Gonzalez HM, Tarraf W, Whitfield KE, Vega WA. The epidemiology of major depression and ethnicity in the United States. J Psychiatr Res. 2010 Nov;44(15):1043–1051. doi: 10.1016/j.jpsychires.2010.03.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Blanco C, Okuda M, Markowitz JC, Liu SM, Grant BF, Hasin DS. The epidemiology of chronic major depressive disorder and dysthymic disorder: results from the National Epidemiologic Survey on Alcohol and Related Conditions. J Clin Psychiatry. 2010 Dec;71(12):1645–1656. doi: 10.4088/JCP.09m05663gry. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Preiss K, Brennan L, Clarke D. A systematic review of variables associated with the relationship between obesity and depression. Obes Rev. 2013 Nov;14(11):906–918. doi: 10.1111/obr.12052. [DOI] [PubMed] [Google Scholar]
- 12.Bjerkeset O, Romundstad P, Evans J, Gunnell D. Association of adult body mass index and height with anxiety, depression, and suicide in the general population: the HUNT study. Am J Epidemiol. 2008 Jan 15;167(2):193–202. doi: 10.1093/aje/kwm280. [DOI] [PubMed] [Google Scholar]
- 13.Herva A, Laitinen J, Miettunen J, et al. Obesity and depression: results from the longitudinal Northern Finland 1966 Birth Cohort Study. Int J Obes (Lond) 2006 Mar;30(3):520–527. doi: 10.1038/sj.ijo.0803174. [DOI] [PubMed] [Google Scholar]
- 14.Blaine B. Does depression cause obesity?: A meta-analysis of longitudinal studies of depression and weight control. J Health Psychol. 2008 Nov;13(8):1190–1197. doi: 10.1177/1359105308095977. [DOI] [PubMed] [Google Scholar]
- 15.Ladwig KH, Marten-Mittag B, Lowel H, Doring A, Wichmann HE. Synergistic effects of depressed mood and obesity on long-term cardiovascular risks in 1510 obese men and women: results from the MONICA-KORA Augsburg Cohort Study 1984–1998. Int J Obes (Lond) 2006 Sep;30(9):1408–1414. doi: 10.1038/sj.ijo.0803285. [DOI] [PubMed] [Google Scholar]
- 16.Werrij MQ, Mulkens S, Hospers HJ, Jansen A. Overweight and obesity: the significance of a depressed mood. Patient Educ Couns. 2006 Jul;62(1):126–131. doi: 10.1016/j.pec.2005.06.016. [DOI] [PubMed] [Google Scholar]
- 17.Katon WJ. Epidemiology and treatment of depression in patients with chronic medical illness. Dialogues in clinical neuroscience. 2011;13(1):7–23. doi: 10.31887/DCNS.2011.13.1/wkaton. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Faulconbridge LF, Wadden TA, Rubin RR, et al. One-year changes in symptoms of depression and weight in overweight/obese individuals with type 2 diabetes in the Look AHEAD study. Obesity (Silver Spring) 2012 Apr;20(4):783–793. doi: 10.1038/oby.2011.315. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Rubin RR, Wadden TA, Bahnson JL, et al. Impact of intensive lifestyle intervention on depression and health-related quality of life in type 2 diabetes: the Look AHEAD Trial. Diabetes Care. 2014 Jun;37(6):1544–1553. doi: 10.2337/dc13-1928. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Linde JA, Simon GE, Ludman EJ, et al. A randomized controlled trial of behavioral weight loss treatment versus combined weight loss/depression treatment among women with comorbid obesity and depression. Ann Behav Med. 2011 Feb;41(1):119–130. doi: 10.1007/s12160-010-9232-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Pagoto S, Schneider KL, Whited MC, et al. Randomized controlled trial of behavioral treatment for comorbid obesity and depression in women: the Be Active Trial. Int J Obes (Lond) 2013 Mar 5; doi: 10.1038/ijo.2013.25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Curran GM, Bauer M, Mittman B, Pyne JM, Stetler C. Effectiveness-implementation hybrid designs: combining elements of clinical effectiveness and implementation research to enhance public health impact. Med Care. 2012 Mar;50(3):217–226. doi: 10.1097/MLR.0b013e3182408812. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Xiao L, Huang Q, Yank V, Ma J. An easily accessed web-based minimization random allocation system for clinical trials. JMIR. 2013;15(7):e139. doi: 10.2196/jmir.2392. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Ma J, Yank V, Xiao L, et al. Translating the Diabetes Prevention Program lifestyle intervention for weight loss into primary care: a randomized trial. JAMA Intern Med. 2013 Jan 28;173(2):113–121. doi: 10.1001/2013.jamainternmed.987. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Ma J, Strub P, Lavori PW, et al. DASH for asthma: A pilot study of the DASH diet in not-well-controlled adult asthma. Contemp Clin Trials. 2013 Jul;35(2):55–67. doi: 10.1016/j.cct.2013.04.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Pocock SJ. Clinical Trials, A Practical Approach. Chichester: John Wiley and Sons; 1991. pp. 84–86. [Google Scholar]
- 27.Pocock SJ, Simon R. Sequential treatment assignment with balancing for prognostic factors in the controlled clinical trial. Biometrics. 1975 Mar;31(1):103–115. [PubMed] [Google Scholar]
- 28.Efron B. Forcing sequential experiment to be balanced. Biometrika. 1971;58:403–417. [Google Scholar]
- 29.Lin EH, Von Korff M, Ciechanowski P, et al. Treatment adjustment and medication adherence for complex patients with diabetes, heart disease, and depression: a randomized controlled trial. Ann Fam Med. 2012 Jan-Feb;10(1):6–14. doi: 10.1370/afm.1343. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Ma J, King AC, Wilson SR, Xiao L, Stafford RS. Evaluation of lifestyle interventions to treat elevated cardiometabolic risk in primary care (E-LITE): a randomized controlled trial. BMC Fam Pract. 2009;10:71. doi: 10.1186/1471-2296-10-71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Kramer MK, Kriska AM, Venditti EM, et al. Translating the Diabetes Prevention Program: a comprehensive model for prevention training and program delivery. Am J Prev Med. 2009 Dec;37(6):505–511. doi: 10.1016/j.amepre.2009.07.020. [DOI] [PubMed] [Google Scholar]
- 32.Ciechanowski P, Wagner E, Schmaling K, et al. Community-integrated home-based depression treatment in older adults: a randomized controlled trial. JAMA. 2004 Apr 7;291(13):1569–1577. doi: 10.1001/jama.291.13.1569. [DOI] [PubMed] [Google Scholar]
- 33.Ciechanowski P, Chaytor N, Miller J, et al. PEARLS depression treatment for individuals with epilepsy: a randomized controlled trial. Epilepsy & behavior: E&B. 2010 Nov;19(3):225–231. doi: 10.1016/j.yebeh.2010.06.003. [DOI] [PubMed] [Google Scholar]
- 34.University of Pittsburge Diabetes Prevention Support Center. GLB Lifestyle Coach Training. 2015 http://www.diabetesprevention.pitt.edu/index.php/training/glb-lifestyle-coach-training/. Accessed March 13, 2015.
- 35.University of Washington. PEARLS Program. http://www.pearlsprogram.org/Training.aspx. Accessed June 28, 2012.
- 36.Kramer MK, Kriska AM, Venditti EM, et al. A novel approach to diabetes prevention: evaluation of the Group Lifestyle Balance program delivered via DVD. Diabetes Res Clin Pract. 2010 Dec;90(3):e60–63. doi: 10.1016/j.diabres.2010.08.013. [DOI] [PubMed] [Google Scholar]
- 37.Chaytor N, Ciechanowski P, Miller JW, et al. Long-term outcomes from the PEARLS randomized trial for the treatment of depression in patients with epilepsy. Epilepsy & behavior: E&B. 2011 Mar;20(3):545–549. doi: 10.1016/j.yebeh.2011.01.017. [DOI] [PubMed] [Google Scholar]
- 38.Katon WJ, Lin EH, Von Korff M, et al. Collaborative care for patients with depression and chronic illnesses. N Engl J Med. 2010 Dec 30;363(27):2611–2620. doi: 10.1056/NEJMoa1003955. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Bandura A. Social Foundations of Thought and Action: A Social Cognitive Theory. Englewood Cliffs, N.J: Prentice Hall; 1986. [Google Scholar]
- 40.Ma J, Strub P, Camargo CA, Jr, et al. The Breathe Easier through Weight Loss Lifestyle (BE WELL) Intervention: a randomized controlled trial. BMC Pulm Med. 2010;10:16. doi: 10.1186/1471-2466-10-16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. (PhenX (consensus measures of Phenotypes and eXposures) is supported by NHGRI award No. U01 HG004597).Measures from the PhenX Toolkit version February 4 2011, Ver 4.2. www.phenxtoolkit.org. Accessed January 15, 2015.
- 42.Goldberg DP, Rickels K, Downing R, Hesbacher P. A comparison of two psychiatric screening tests. Br J Psychiatry. 1976 Jul;129:61–67. doi: 10.1192/bjp.129.1.61. [DOI] [PubMed] [Google Scholar]
- 43.Glass RM, Allan AT, Uhlenhuth EH, Kimball CP, Borinstein DI. Psychiatric screening in a medical clinic. An evaluation of a self-report inventory. Arch Gen Psychiatry. 1978 Oct;35(10):1189–1195. doi: 10.1001/archpsyc.1978.01770340039003. [DOI] [PubMed] [Google Scholar]
- 44.Karlsson J, Taft C, Sjostrom L, Torgerson JS, Sullivan M. Psychosocial functioning in the obese before and after weight reduction: construct validity and responsiveness of the Obesity-related Problems scale. Int J Obes Relat Metab Disord. 2003 May;27(5):617–630. doi: 10.1038/sj.ijo.0802272. [DOI] [PubMed] [Google Scholar]
- 45.Spitzer RL, Kroenke K, Williams JB, Lowe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006 May 22;166(10):1092–1097. doi: 10.1001/archinte.166.10.1092. [DOI] [PubMed] [Google Scholar]
- 46.Sheehan DV, Lecrubier Y, Sheehan KH, et al. The Mini-International Neuropsychiatric Interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry. 1998;59(Suppl 20):22–33. quiz 34–57. [PubMed] [Google Scholar]
- 47.Sheehan KH, Sheehan DV. Assessing treatment effects in clinical trials with the discan metric of the Sheehan Disability Scale. International clinical psychopharmacology. 2008 Mar;23(2):70–83. doi: 10.1097/YIC.0b013e3282f2b4d6. [DOI] [PubMed] [Google Scholar]
- 48.Ware JE, Kosinski M, Dewey JE, Gandek B. How to Score and Interpret Single-Item Health Status Measures: A Manual for Users of the SF-8 Health Survey. Lincoln RI: QualityMetric Incorporated; 2001. [Google Scholar]
- 49.Badia X, Schiaffino A, Alonso J, Herdman M. Using the EuroQoI 5-D in the Catalan general population: feasibility and construct validity. Qual Life Res. 1998 May;7(4):311–322. doi: 10.1023/a:1024933913698. [DOI] [PubMed] [Google Scholar]
- 50.Schafer GL, Songer TJ, Kramer MK, Miller RG, Vanderwood KK, Kriska A. Do Food Costs Increase for Participants in a Diabetes Prevention Program?; Paper presented at: American Diabetes Association 73rd Scientific Sessions2013; Chicago, IL. [Google Scholar]
- 51.Hernan WH, Brandle M, Zhang P, et al. Costs associated with the primary prevention of type 2 diabetes mellitus in the Diabetes Prevention Program (DPP) Diabetes Care. 2003 Jan;26(1):36–47. doi: 10.2337/diacare.26.1.36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Weathers FW, Litz BT, Herman DS, Huska JA, Keane TM. The PTSD checklist: Reliability, validity, and diagnostic utility; Paper presented at the Annual Meeting of the International Society for Traumatic Stress Studies; 1993; San Antonio, TX. [Google Scholar]
- 53.Moshfegh AJ, Goldman J, Lacomb R, Perloff B, Cleveland L. Research results using the new USDA Automated Multiple-Pass Method. FASEB J. 2001;15(4):A278. (abstr) [Google Scholar]
- 54.Blair SN, Haskell WL, Ho P, et al. Assessment of habitual physical activity by a seven-day recall in a community survey and controlled experiments. Am J Epidemiol. 1985 Nov;122(5):794–804. doi: 10.1093/oxfordjournals.aje.a114163. [DOI] [PubMed] [Google Scholar]
- 55.D’Zurilla TJ, Chang EC, Nottingham EJt, Faccini L. Social problem-solving deficits and hopelessness, depression, and suicidal risk in college students and psychiatric inpatients. J Clin Psychol. 1998 Dec;54(8):1091–1107. doi: 10.1002/(sici)1097-4679(199812)54:8<1091::aid-jclp9>3.0.co;2-j. [DOI] [PubMed] [Google Scholar]
- 56.Yu L, Buysse DJ, Germain A, et al. Development of short forms from the PROMIS sleep disturbance and Sleep-Related Impairment item banks. Behavioral sleep medicine. 2011 Dec 28;10(1):6–24. doi: 10.1080/15402002.2012.636266. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Glasgow RE, Vogt TM, Boles SM. Evaluating the public health impact of health promotion interventions: the RE-AIM framework. Am J Public Health. 1999 Sep;89(9):1322–1327. doi: 10.2105/ajph.89.9.1322. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Kessler RS, Purcell EP, Glasgow RE, Klesges LM, Benkeser RM, Peek CJ. What does it mean to “employ” the RE-AIM model? Eval Health Prof. 2013 Mar;36(1):44–66. doi: 10.1177/0163278712446066. [DOI] [PubMed] [Google Scholar]
- 59.Robin DB. Multiple Imputation for Nonresponse in Surveys. New York: John Wiley & Sons, Inc; 1987. [Google Scholar]
- 60.Lavori PW, Dawson R, Shera D. A multiple imputation strategy for clinical trials with truncation of patient data. Stat Med. 1995 Sep 15;14(17):1913–1925. doi: 10.1002/sim.4780141707. [DOI] [PubMed] [Google Scholar]
- 61.Schafer JL. Analysis of Incomplete Multivariate Data. New York: Chapman and Hall; 1997. [Google Scholar]
- 62.Tang L, Duan N, Klap R, Asarnow JR, Belin TR. Applying permutation tests with adjustment for covariates and attrition weights to randomized trials of health-services interventions. Stat Med. 2009 Jan 15;28(1):65–74. doi: 10.1002/sim.3453. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.DiCiccio TJ, Efron B. Bootstrap confidence intervals. Statistic Sci. 1996;11(3):189–228. [Google Scholar]
- 64.MacKinnon DP, Fritz MS, Williams J, Lockwood CM. Distribution of the product confidence limits for the indirect effect: program PRODCLIN. Behav Res Methods. 2007 Aug;39(3):384–389. doi: 10.3758/bf03193007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Goldhaber-Fiebert JD, Rubinfeld RE, Bhattacharya J, Robinson TN, Wise PH. The utility of childhood and adolescent obesity assessment in relation to adult health. Med Decis Making. 2012 doi: 10.1177/0272989X12447240. Epub ahead of print. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Hall KD, Jordan PN. Modeling weight-loss maintenance to help prevent body weight regain. Am J Clin Nutr. 2008 Dec;88(6):1495–1503. doi: 10.3945/ajcn.2008.26333. [DOI] [PubMed] [Google Scholar]
- 67.Hall KD. Predicting metabolic adaptation, body weight change, and energy intake in humans. American journal of physiology. Endocrinology and metabolism. 2010 Mar;298(3):E449–466. doi: 10.1152/ajpendo.00559.2009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Herman WH, Hoerger TJ, Brandle M, et al. The cost-effectiveness of lifestyle modification or metformin in preventing type 2 diabetes in adults with impaired glucose tolerance. Ann Intern Med. 2005 Mar 1;142(5):323–332. doi: 10.7326/0003-4819-142-5-200503010-00007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Haji Ali Afzali H, Karnon J, Gray J. A critical review of model-based economic studies of depression: modelling techniques, model structure and data sources. Pharmacoeconomics. 2012 Jun 1;30(6):461–482. doi: 10.2165/11590500-000000000-00000. [DOI] [PubMed] [Google Scholar]
- 70.Wein LM, Yang Y, Goldhaber-Fiebert JD. Assessing screening policies for childhood obesity. Obesity (Silver Spring) 2012 Jul;20(7):1437–1443. doi: 10.1038/oby.2011.373. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Gold MR, Siegel JE, Russell LB, Weinstein MC, editors. Cost-Effectiveness in Health and Medicine. New York: Oxford University Press; 1996. [Google Scholar]
- 72.Kraemer HC, Kupfer DJ. Size of treatment effects and their importance to clinical research and practice. Biol Psychiatry. 2006 Jun 1;59(11):990–996. doi: 10.1016/j.biopsych.2005.09.014. [DOI] [PubMed] [Google Scholar]
- 73.The STAR*D Investigative Team. Sequenced Treatment Alternatives to Relieve Depression (STAR*D) Protocol and Analytic Plan. 2002 http://www.madinamerica.com/MADINAMERICA.COM/STARD%20Documents_files/STAR-D%20Protocol%20with%20Analytic%20Plan.pdf. Accessed April 19, 2011.
- 74.Within-trial cost-effectiveness of lifestyle intervention or metformin for the primary prevention of type 2 diabetes. Diabetes Care. 2003 Sep;26(9):2518–2523. doi: 10.2337/diacare.26.9.2518. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Laupacis A, Feeny D, Detsky AS, Tugwell PX. How attractive does a new technology have to be to warrant adoption and utilization? Tentative guidelines for using clinical and economic evaluations. CMAJ. 1992 Feb 15;146(4):473–481. [PMC free article] [PubMed] [Google Scholar]
- 76.Guidelines for the economic evaluation of health technologies. 3rd. Ottawa, Canada: Canadian Agency for Drugs and Technologies in Health; 2006. [Google Scholar]
- 77.Weinstein MC, Siegel JE, Gold MR, Kamlet MS, Russell LB. Recommendations of the Panel on Cost-effectiveness in Health and Medicine. JAMA. 1996 Oct 16;276(15):1253–1258. [PubMed] [Google Scholar]
- 78.QSR NVivo [computer program] Victoria, Australia: QSR International; [Google Scholar]
- 79.Elo S, Kyngas H. The qualitative content analysis process. Journal of advanced nursing. 2008 Apr;62(1):107–115. doi: 10.1111/j.1365-2648.2007.04569.x. [DOI] [PubMed] [Google Scholar]
- 80.Patton MQ. Qualitative research and evaluation methods. San Francisco: Sage Publications; 2002. [Google Scholar]
- 81.Ma J, Yank V, Xiao L, et al. Translating the Diabetes Prevention Program lifestyle intervention for weight loss into primary care: A randomized trial. Arch Intern Med. 2012 doi: 10.1001/2013.jamainternmed.987. accepted for publication. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Ma J, Berra K, Haskell WL, et al. Case management to reduce risk of cardiovascular disease in a county health care system. Arch Intern Med. 2009 Nov 23;169(21):1988–1995. doi: 10.1001/archinternmed.2009.381. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Kraemer HC. To increase power in randomized clinical trials without increasing sample size. Psychopharmacol Bull. 1991;27(3):217–224. [PubMed] [Google Scholar]
- 84.ICH Harmonised Tripartite Guideline. Statistical principles for clinical trials. International Conference on Harmonisation E9 Expert Working Group. Stat Med. 1999 Aug 15;18(15):1905–1942. [PubMed] [Google Scholar]
- 85.Bender R, Lange S. Adjusting for multiple testing–when and how? J Clin Epidemiol. 2001 Apr;54(4):343–349. doi: 10.1016/s0895-4356(00)00314-0. [DOI] [PubMed] [Google Scholar]
- 86.Thomas PR. Weighing the Options: Criteria for Evaluating Weight-Management Programs. Washington, DC: Committee to Develop Criteria for Evaluating the Outcomes of Approaches to Prevent and Treat Obesity, Institute of Medicine; 1995. [PubMed] [Google Scholar]
- 87.Stevens J, Truesdale KP, McClain JE, Cai J. The definition of weight maintenance. Int J Obes (Lond) 2006 Mar;30(3):391–399. doi: 10.1038/sj.ijo.0803175. [DOI] [PubMed] [Google Scholar]
- 88.Blaine BE, Rodman J, Newman JM. Weight loss treatment and psychological well-being: a review and meta-analysis. J Health Psychol. 2007 Jan;12(1):66–82. doi: 10.1177/1359105307071741. [DOI] [PubMed] [Google Scholar]
- 89.National Institute for Clinical Excellence. Depression: Management of Depression in Primary and Secondary Care. London, England: National Health Service; 2004. [Google Scholar]
- 90.Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)–a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009 Apr;42(2):377–381. doi: 10.1016/j.jbi.2008.08.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Conway JM, Ingwersen LA, Vinyard BT, Moshfegh AJ. Effectiveness of the US Department of Agriculture 5-step multiple-pass method in assessing food intake in obese and nonobese women. Am J Clin Nutr. 2003 May;77(5):1171–1178. doi: 10.1093/ajcn/77.5.1171. [DOI] [PubMed] [Google Scholar]
- 92.Conway JM, Ingwersen LA, Moshfegh AJ. Accuracy of dietary recall using the USDA five-step multiple-pass method in men: an observational validation study. J Am Diet Assoc. 2004 Apr;104(4):595–603. doi: 10.1016/j.jada.2004.01.007. [DOI] [PubMed] [Google Scholar]
- 93.Bellg AJ, Borrelli B, Resnick B, et al. Enhancing treatment fidelity in health behavior change studies: best practices and recommendations from the NIH Behavior Change Consortium. Health Psychol. 2004 Sep;23(5):443–451. doi: 10.1037/0278-6133.23.5.443. [DOI] [PubMed] [Google Scholar]
- 94.Miller WR, Rollnick S. Motivational Interviewing: Preparing People for Change. 2nd. New York: Guilford Press; 2002. [Google Scholar]
- 95.Schneider KL, Bodenlos JS, Ma Y, et al. Design and methods for a randomized clinical trial treating comorbid obesity and major depressive disorder. BMC Psychiatry. 2008;8:77. doi: 10.1186/1471-244X-8-77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Katon WJ, Von Korff M, Lin EH, et al. The Pathways Study: a randomized trial of collaborative care in patients with diabetes and depression. Arch Gen Psychiatry. 2004 Oct;61(10):1042–1049. doi: 10.1001/archpsyc.61.10.1042. [DOI] [PubMed] [Google Scholar]
- 97.Unutzer J, Katon W, Callahan CM, et al. Collaborative care management of late-life depression in the primary care setting: a randomized controlled trial. JAMA. 2002 Dec 11;288(22):2836–2845. doi: 10.1001/jama.288.22.2836. [DOI] [PubMed] [Google Scholar]
- 98.Katon W, Pedersen HS, Ribe AR, et al. Effect of Depression and Diabetes Mellitus on the Risk for Dementia: A National Population-Based Cohort Study. JAMA psychiatry. 2015 Apr 15; doi: 10.1001/jamapsychiatry.2015.0082. [DOI] [PMC free article] [PubMed] [Google Scholar]