An official website of the United States government
Here's how you know
Official websites use .gov
A
.gov website belongs to an official
government organization in the United States.
Secure .gov websites use HTTPS
A lock (
) or https:// means you've safely
connected to the .gov website. Share sensitive
information only on official, secure websites.
As a library, NLM provides access to scientific literature. Inclusion in an NLM database does not imply endorsement of, or agreement with,
the contents by NLM or the National Institutes of Health.
Learn more:
PMC Disclaimer
|
PMC Copyright Notice
[1].Lodge JPA, Ammori BJ, Prasad KR, Bellamy MC. Ex-vivo and in situ resection of inferior vena cava with hepatectomy for colorectal metastases. Ann Surg. 2000;231:471–9. doi: 10.1097/00000658-200004000-00004. [DOI] [PMC free article] [PubMed] [Google Scholar]
[2].Makuuchi M, Hasegawa H, Yamazaki S, Takayasu K. Four new hepatectomy procedures for resection of the right hepatic vein and preservation of the inferior right hepatic vein. Surg Gynecol Obstet. 1987;164:69–72. [PubMed] [Google Scholar]
[3].Ozeki Y, Uchiyama T, Katayama M, et al. Extended left hepatic trisegmentectomy with resection of main right hepatic vein and preservation of middle and inferior right hepatic veins. Surgery. 1995;117:715–7. doi: 10.1016/S0039-6060(95)80018-2. [DOI] [PubMed] [Google Scholar]
[4].Belghiti J, Noun R, Zante E, et al. Portal triad clamping or hepatic vascular exclusion for major liver resection: a controlled study. Ann Surg. 1996;224:155–61. doi: 10.1097/00000658-199608000-00007. [DOI] [PMC free article] [PubMed] [Google Scholar]
[5].Delva E, Camus Y, Nordlinger B, et al. Vascular occlusions for liver resections — operative management and tolerance to hepatic ischemia: 142 cases. Ann Surg. 1989;209:211–8. doi: 10.1097/00000658-198902000-00012. [DOI] [PMC free article] [PubMed] [Google Scholar]
[6].Evans PM, Vogt DP, Mayes JT, et al. Liver resection using total vascular exclusion. Surgery. 1998;124:807–15. doi: 10.1067/msy.1998.91225. [DOI] [PubMed] [Google Scholar]
[7].Hannoun L, Borie D, Delva E, et al. Liver resection with normothermic ischaemia exceeding 1 h. Br J Surg. 1993;80:1161–5. doi: 10.1002/bjs.1800800933. [DOI] [PubMed] [Google Scholar]
[8].Huguet C, Gallot D, Offenstadt G. Normothermic complete hepatic vascular exclusion for extensive resection of the liver. N Engl J Med. 1976;294:51–2. doi: 10.1056/NEJM197601012940118. [DOI] [PubMed] [Google Scholar]
[9].Pringle JH. Notes on the arrest of hepatic hemorrhage due to trauma. Ann Surg. 1908;48:541–9. doi: 10.1097/00000658-190810000-00005. [DOI] [PMC free article] [PubMed] [Google Scholar]
[11].Delrivière L, Hannoun L. In situ and ex situ in vivo procedure for complex major liver resections requiring prolonged hepatic vascular exclusion in normal and diseased livers. J Am Coll Surg. 1995;181:272–6. [PubMed] [Google Scholar]
[12].Pichlmayr R, Grosse H, Hauss J, et al. Technique and preliminary results of extracorporeal liver surgery (bench procedure) and of surgery on the in situ perfused liver. Br J Surg. 1990;77:21–6. doi: 10.1002/bjs.1800770107. [DOI] [PubMed] [Google Scholar]
[13].Yagyu T, Shimizu R, Nishida M, et al. Reconstruction of the hepatic vein to the prosthetic inferior vena cava in right extended hemihepatectomy with ex situ procedure. Surgery. 1994;115:740–4. [PubMed] [Google Scholar]
[14].Fortner JG, Shiu MH, Kinne D, et al. Major hepatic resection using vascular isolation and hypothermic perfusion. Ann Surg. 1974;180:644–52. doi: 10.1097/00000658-197410000-00030. [DOI] [PMC free article] [PubMed] [Google Scholar]
[15].Hamazaki K, Yagi T, Tanaka N, et al. Hepatectomy under extracorporeal circulation. Surgery. 1995;118:98–102. doi: 10.1016/S0039-6060(05)80015-7. [DOI] [PubMed] [Google Scholar]
References
[1].Craig JR, Peters RL, Edmondson HA. Tumours of the liver and extrahepatic bile ducts. In: AFIP Atlas of tumour Pathology, Second series fascicle 26, 1989.
[2].Anthony SP, et al. Tumour and tumour-like lesions of the liver and biliary tract. In: MacSween RNM, et al., editors. Pathology of the Liver. 3. Edinburgh: Churchill Livingstone; 1994. pp. 635–711. [Google Scholar]
[4].Schele J, Stang R, Altendorf-Hofmann A, Paul M. Resection of colorectal metastasis. World J Surg. 1995;19:59–71. doi: 10.1007/BF00316981. [DOI] [PubMed] [Google Scholar]
[5].Yoon SS, Tanebe KK. Multidisciplinary management of metastatic colorectal cancer. Surg Oncol. 1998;7:197–207. doi: 10.1016/S0960-7404(99)00022-5. [DOI] [PubMed] [Google Scholar]
References
[1].Blomley M, Cosgrove D. Contrast agents in ultrasound. Br J Hosp Med. 1996;55:6–7. [PubMed] [Google Scholar]
[2].Leen E, McArdle CS. Ultrasound contrast agents in liver imaging. Clin Radiol. 1996;51(Suppl1):35–9. [PubMed] [Google Scholar]
[3].Blomley M, et al. Stimulated acoustic emission imaging (‘sonoscintigraphy’) with the ultrasound contrast agent Levovist: a reproducible Doppler ultrasound effect with potential clinical utility. Acad Radiol. 1998;5(Suppl1):S236–9. doi: 10.1016/S1076-6332(98)80116-5. [DOI] [PubMed] [Google Scholar]
[4].Eckersley R. Functional Imaging with ultrasound contrast agents. Ultrasound Med Biol 1999 (in press).
[5].Blomley MJ, et al. Liver vascular transit time analyzed with dynamic hepatic venography with bolus injections of an US contrast agent: early experience in seven patients with metastases. Radiology. 1998;209:862–6. doi: 10.1148/radiology.209.3.9844688. [DOI] [PubMed] [Google Scholar]
References
[1].Willis RA. The spread of Tumours in the Human Body. 3. London: Butterworths; 1973. Secondary tumours of the liver; pp. 175–83. [Google Scholar]
[2].Cameron GR. The liver as a site and source of cancer. Br Med J 1954; Feb: 347–52. [DOI] [PMC free article] [PubMed]
[3].Ozarda A, Pickren J. The topographic distribution of liver metastases, its relation to surgical and isotope diagnosis. J Nucl Med. 1962;3:149–52. [Google Scholar]
[4].Goligher JC. The operability of carcinoma of the rectum. Br Med J. 1941;ii:393–7. doi: 10.1136/bmj.2.4211.393. [DOI] [PMC free article] [PubMed] [Google Scholar]
[6].Ward J, Naik KS, Guthrie JA, Wilson D, Robinson PJ. Hepatic lesion detection: comparison of MR imaging after the administration of superparamagnetic iron oxide with dualphase CT by using alternative-free response receiver operating characteristic analysis. Radiology. 1999;210:459–66. doi: 10.1148/radiology.210.2.r99fe05459. [DOI] [PubMed] [Google Scholar]
[7].Hagspiel KD, Neidl KFW, Eichenberger AC, et al. Detection of liver metastases: comparison of superparamagnetic iron oxide-enhanced and unenhanced MR imaging at 1.5 T with dynamic CT, intraoperative US and percutaneous US. Radiology. 1995;196:471–8. doi: 10.1148/radiology.196.2.7617863. [DOI] [PubMed] [Google Scholar]
[8].Nelson RC, Chezmar JL, Sugarbaker PH, Bernardino ME. Hepatic tumours: comparison of CT during arterial portography, delayed CT, and MR imaging for preoperative evaluation. Radiology. 1989;172:27–34. doi: 10.1148/radiology.172.1.2662254. [DOI] [PubMed] [Google Scholar]
[9].Matsui O, Takashima T, Kadoya L, et al. Liver metastases from colorectal cancers: detection with CT during arterial portography. Radiology. 1987;165:65–9. doi: 10.1148/radiology.165.1.2819942. [DOI] [PubMed] [Google Scholar]
[10].Soyer P, Lacheheb D, Levesque M. False positive diagnosis based on CT portography:correlation with pathological findings. Am J Roentgenol. 1992;160:285–9. doi: 10.2214/ajr.160.2.8424337. [DOI] [PubMed] [Google Scholar]
[11].Valls C, Lopez E, Guma A, Gil M, Sanchez A, Andia E, Serra J, Moreno V, Figueras J. Helical CT versus CT arterial portography in the detection of hepatic metastases from colorectal carcinoma. Am J Roentgenol. 1998;70:1341–7. doi: 10.2214/ajr.170.5.9574613. [DOI] [PubMed] [Google Scholar]
[12].Young N, Sing T, Wong KP, Hollands M, Tait N. Use of spiral and non-spiral computed tomography arterial portography in the detection of potentially malignant liver masses. J Gastroenterol Hepatol. 1997;12:385–91. doi: 10.1111/j.1440-1746.1997.tb00448.x. [DOI] [PubMed] [Google Scholar]
[13].Seneterre E, Taourel P, Bouvier Y, et al. Detection of hepatic metastases: ferumoxides-enhanced MR imaging versus unenhanced MR imaging and CT during arterial portography. Radiology. 1996;200:785–92. doi: 10.1148/radiology.200.3.8756932. [DOI] [PubMed] [Google Scholar]
[14].Oudkerk M, van den Heuvel AG, Wielpolski PA, et al. Hepatic lesions: detection with ferumoxide-enhanced T1-weighted MR imaging. Radiology. 1997;203:449–56. doi: 10.1148/radiology.203.2.9114103. [DOI] [PubMed] [Google Scholar]
[15].Jones EC, Chezmar JL, Nelson RC, et al. The frequency and significance of small (<15 mm) hepatic lesions detected by CT. Am J Roentgenol. 1992;158:535–9. doi: 10.2214/ajr.158.3.1738990. [DOI] [PubMed] [Google Scholar]
[16].Schwarz LH, Gandras EJ, Colangelo SM, Ercolani MC, Panicek DM. Prevalence and importance of small hepatic lesions found at CT in patients with cancer. Radiology. 1999;210:71–4. doi: 10.1148/radiology.210.1.r99ja0371. [DOI] [PubMed] [Google Scholar]
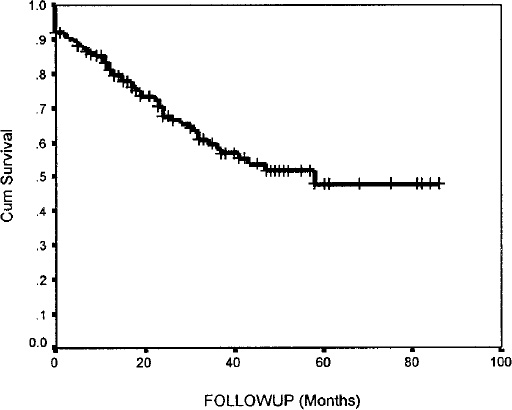
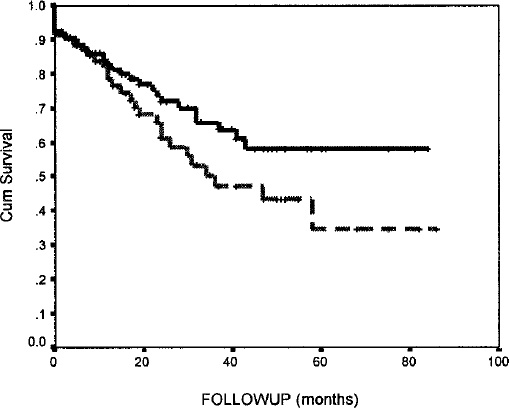
Patients with hepatic metastases from colorectal cancer have a poor prognosis, with a median survival of less than 12 months. Although chemotherapy may have a beneficial effect on the natural history of unresected liver metastases, 5-year survival is difficult to achieve by chemotherapy alone. Hepatic resection can achieve prolonged survival with an acceptable mortality risk in selected patients, but this approach has classically been reserved for a very select group of patients, usually those with a solitary metastasis discovered some time after the primary colorectal resection. This author’s practices in surgery for hepatic metastases from colorectal cancer have been more radical than most other surgeons[1]. A careful follow-up protocol with the use of adjuvant chemotherapy and redo resection have enabled this author to achieve satisfactory results (Figs 1 and 2).
58% for bilateral resection (n=97); 35% for unilobar disease (n=64) at 5 years (p> 0.05). This demonstrates that patients with advanced disease can do well.
Thus, these days it seems that virtually no liver tumour should be considered to be unresectable, even though the majority of patients continue to present at a late stage in their disease. Some experts have challenged the old dogma relating to hepatic resection and candidates with multiple and bilobar tumours, as well as patients with limited extrahepatic infiltration, are now considered for resection. In addition, metastases from tumours other than colorectal cancer are also regularly undergoing liver resection.
Radiology assessment
MRI is the imaging method of choice for the liver in our centre, although other groups routinely use CT arterioportography with similar results. Three-dimensional CT and MRI imaging technology continues to improve and may be of value in planning the surgical approach. Hepatic angiography with portal venography may also be useful. For example, small neuroendocrine metastases not detected by other methods will rule out some candidates and knowledge of variations in hepatic arterial anatomy can be helpful in some cases. Venography to examine the inferior vena cava and hepatic veins is occasionally useful if all three major hepatic veins are involved with tumour as an adequate inferior or middle right hepatic vein may obviate the need for ex-vivo venous reconstruction[2,3]. It is our current practice to use CT scanning of the chest, abdomen and pelvis to exclude extrahepatic disease for all tumour types. Screening for primary site recurrence (e.g. colonoscopy) is also clearly important and an isotope bone scan may be useful.
Intraoperative ultrasound
This author introduced the routine use of intraoperative ultrasound for liver resection at our centre, both in terms of assessment of resectability and as an aid to extending hepatic resection beyond the described segmental boundaries in difficult cases. An initial study on intra-operative ultrasound suggested that this simple tool could alter the course of surgery in approximately 40% of liver operations by accurate definition of small tumours and by a close examination of their relationship to intrahepatic vascular structures. However, recent improvements in magnetic resonance imaging technology and contrast media mean that intra-operative studies have a lesser role now.
Anaesthesia and surgical techniques
Improvements in anaesthesia have been integral to the success of hepatic surgery, primarily through the use of low central venous pressure techniques for liver resection. In this author’s centre only 20% of cases require blood transfusion. This is despite the fact that 85% of this author’s current resection practice is hemihepatectomy or more and the majority is extended hepatectomy and bilateral resection work. The use of low frequency ultrasonic dissection is partly responsible for this improvement.
In the majority of hepatobiliary centres, Pringle’s manoeuvre (temporary occlusion of the hepatic artery and portal vein) and/or total vascular isolation (by additional clamping of the inferior vena cava above and below the liver to provide hepatic vascular exclusion) are used routinely, and this short-term warm ischaemia is reported to be well-tolerated[4–10]. However, it has been our preference in recent years to avoid ischaemia whenever possible as we had noticed an increased postoperative morbidity and longer hospital stay in those patients in whom vascular isolation techniques had been used for prolonged periods.
In our experience, the use of hepatic ischaemia techniques and blood transfusion are more often necessary for the more complex resections. Whereas right and left hepatectomy and right hepatic trisegmentectomy (extended right hepatectomy — resection of hepatic segments 4–8 ± 1) should be regarded as routine and rarely require transfusion, left hepatic trisegmentectomy (extended left hepatectomy — resection of hepatic segments 2, 3, 4, 5, 8 ± 1), for example, is more challenging. Recent internal audit of the last 22 left hepatic trisegmentectomies carried out by this author has shown that 11 required Pringle’s manoeuvre and five needed a period of total vascular isolation. In 14 cases the caudate lobe (segment 1) was also resected. Eleven of the 22 patients required blood transfusion, although the median requirement was only 1.5 units. In this group of 22 patients, six of the seven patients with major post-operative morbidity had required either Pringle’s manoeuvre or total vascular isolation, confirming our previous observation.
Inferior vena cava (IVC) involvement can often be dealt with by simple venous side-clamping or in more extensive cases by total hepatic vascular isolation with IVC clamping and the selective use of a veno-venous bypass. IVC resection accounts for 4.5% of this author’s metastatic work, and replacement by graft has been necessary in about 40%[1]. Tumours involving all of the major hepatic veins with or without IVC invasion, and particularly tumours involving the hepatocaval confluence and needing IVC replacement, continue to pose a surgical challenge. Ex-vivo resection[1,11–13] offers a potential life-line for this group of patients and this technique deserves discussion, although it accounts for less than 2% of this author’s total hepatic resection experience.
Advanced techniques
In-situ hypothermic perfusion, the ‘anti situm technique’ and ex-vivo liver resection are techniques that may be preferable in some cases where it is anticipated that the parenchymal dissection will be difficult. The aim is to provide a bloodless field combined with hypothermic cellular protection, allowing a prolonged and more precise dissection[11–15]. Many of the techniques have been developed from liver transplantation.
For in-situ hypothermic perfusion, the portal triad structures and the IVC are clamped and cooling is achieved by infusion of a preservation solution into the portal vein or hepatic artery. The IVC is clamped above and below the liver (and also the right suprarenal vein if necessary) and the infrahepatic IVC is incised above the lower clamp. Perfusion is started with a cold hepatic preservation solution and the venous effluent is actively sucked from the IVC to prevent excessive body cooling. Liver cooling can by maintained by continuous slow perfusion during the resection or by repeated cooling by perfusion every 30 min.
The anti situm procedure combines in-situ hypothermic perfusion with separation of the suprahepatic IVC to allow mobilization for dissection of the cranial and posterior parts of the liver under direct vision. It should allow the whole upper part of the liver to be moved onto the abdominal wall in order to allow access to the cranial and posterior aspects of the liver. Veno-venous bypass may be an advantage. Hepatic perfusion is as for the in-situ technique, although the liver can be placed on a heat exchange plate to help keep it cool during the resection[11].
Ex-vivo resection involves totally removing the liver and operation on it to remove the tumours prior to reimplantation. This technique is useful where there is involvement of all three hepatic veins and if the portal triad structures are also involved. The IVC may be replaced by the use of a prosthetic graft[1].
Redo liver resection
About 30% of patients who develop recurrent metastatic disease following hepatic resection will have isolated liver metastases. This is a very worthwhile group to consider for further surgery and results are at least as good as with first-time surgery.
Future work
Future efforts must concentrate on earlier referral and more rapid assessment for liver surgery. Often the window of opportunity for surgery is narrow and unnecessary delays make surgery difficult or impossible. Surgical techniques continue to advance and there are several new technologies that are becoming incorporated into hepatic resection. Improvements in pre-operative staging and better follow-up radiology are required. The use of adjuvant chemotherapies and ablative therapies may also improve results.
Metastatic tumours in the liver are reported to be 18 times more common than primary lesions. Of a series of 95 000 autopsies between 1978 and 1980, 20.4% patients had malignant tumours and 38% of these (7299, 7.7% of total) had metastases in the liver[1]. In this series there were 105 patients (0.1%) with primary hepatic malignancy and 64 (0.07%) with a primary benign tumour (not including haemangiomas and cysts), although this maybe an underestimate due to incomplete reporting of these lesions. The four most common primary sites for liver metastases, in descending order, are lung, large bowel, pancreas and breast. Of these, colorectal carcinomas characteristically form small numbers of large, expansile tumours, with or without satellites, while tumours from other primary sites have an infiltrative pattern, either with multifocal or diffuse involvement of the liver.
Small liver lesions may be detected on imaging the liver in patients being evaluated for surgical resection of metastasis. These may be small additional metastases or incidental benign liver lesions. The list of such lesions is long, but only simple cysts and haemangiomas occur with any frequency[1,2]. Cysts are reported in 1–14% autopsy series, depending on how thoroughly the liver is sectioned, and they are more common in females (5:1). Haemangiomas are reported in 1% of autopsies, 90% are solitary. Their prevalence increases with age and there is a female preponderance only in younger patients. They may be heterogenous due to recent and old areas of thrombosis. Rare small benign lesions include focal nodular hyperplasia, bile duct adenoma and liver cell adenoma[3]; extremely rare lesions include lipoma, fibroma, inflammatory pseudotumour histiocytosis x and pancreatic heterotopia. Von Meyenberg complexes are relatively common, but measure at most 5 mm and are generally too small to be apparent on imaging. Solitary necrotic nodules are occasionally encountered and probably represent previous larval infestation.
Pathological features that have been shown to be negative prognostic factors in patients surgically treated for metastasing colorectal carcinoma include a higher number of liver metastases, and presence of satellitosis[4,5]. A review of 83 specimens for first partial hepatectomy for metastatic colorectal cancer at this institution showed focal lesions other than metastasis in five of them, all were simple cysts. Twenty-two of 83 cases contained small metastatic deposits (≤ 5 mm) either satellite to the main metastases or distant. No cases showed microscopic deposits not visible macroscopically. Six cases of re-excision contained four small lesions separate from the metastasis; one was a cyst and three were nodules of scar tissue related to previous surgery. Thus small lesions detected during liver imaging for metastatic colorectal cancer are statistically much more likely to be metastases than other incidental benign lesions, once cysts and haemangiomas have been excluded. Previous resections may leave nodules of scar tissue that resemble metastasis macroscopically.
Progress in ultrasound technology has been rapid and could establish it as the most accurate imaging technique for detecting liver metastases. Central to this has been the development of effective contrast agents in the form of microbubbles for intravenous injection and this has been underpinned by striking improvements in scanner performance using fast digital computers and by the development of new transducers[1]. Many of the developments in scanner technology have been stimulated by the special acoustic properties of the microbubbles in what has become a synergistic relationship between the equipment manufacturers and pharmaceutical houses.
The liver has emerged as a particularly promising application of the microbubble contrast agents because not only can Doppler and grey scale techniques be used to demonstrate the vascular phases much more effectively than with non-enhanced Doppler, but also the liver-specific late phase of some microbubbles depicts normally functioning liver with great precision. The vascular phases are analogous to a three-phase contrast CT scan with arterial and portal venous components at 20 s and around 1 min after an intravenous bolus, followed by an additional late ‘tissue’ phase. In the first two phases the microbubbles can be demonstrated with colour Doppler or, with the newer, more reflective microbubbles, using a non-linear technique as the phase inversion imaging which has excellent spatial resolution[2]. Many malignancies show a rapid and spectacular uptake of contrast in the arterial phase and the chaotic pattern of the vessels can be distinguished from the spoke-wheel pattern of FNH. The adult type of haemangioma shows minimal or no microbubble signals in this phase but scans after several minutes often show marked peripheral clumping of contrast which slowly percolates through the lesion in a centripetal fashion, exactly as seen on delayed contrast CT scanning.
When one of the agents that has a liver-specific phase is used, scanning late in the post-vascular phase (i.e. after 3–5 min) shows the distribution of normally functioning liver in a very spectacular way[3]. Again, the spatial resolution of the phase inversion mode has advantages in the detection of small lesions, and metastases down to 3 mm diameter have been convincingly demonstrated — sometimes smaller than can be detected with contrast-enhanced CT or MRI. The alternative non-linear method, Agent Detection Imaging (ADI, a development of power Doppler) has the advantage of allowing the microbubble signature to be displayed separately from the grey scale image and seems to allow even a few microbubble events to be detected and so has higher sensitivity. This is useful in characterizing lesions because it has been found that, while metastases and HCC have no or very scanty signals, haemangiomas show some or moderate signals. Lesions that contain functioning liver tissue have the same signal intensity as normal liver: this applies to regenerating nodules, focal fatty change and sparing and to FNH (which may actually show higher signals than the surrounding liver). The combination of the vascular and the later liverspecific phases promise to expand the role of ultrasound in the liver.
The properties of microbubbles can also be exploited in entirely new ways to reveal the way they flow through the liver and its lesions, thus providing functional haemodynamic information[4]. This is promising for studying the haemodynamics of focal lesions, but a timing method that interrogates the whole liver seems to be approaching acceptance as a clinical tool for studying arteriovenous shunting which occur in malignancy and in cirrhosis as well as in a few benign masses, notably FNH and oestrogen adenomas but, importantly, not in haemangiomas of the adult type. If a microbubble bolus is given via a peripheral vein, it arrives in the hepatic veins draining the liver earlier than normal when shunts are present[5]. This can be timed simply by noting the interval from the injection time until the signal increase in a spectral Doppler gate placed on an hepatic vein. Early arrival seems to be very sensitive to the presence of liver malignancy though the limits have not yet been defined, particularly the critical question of whether malignancies too small to be imaged can be detected, although the pathophysiology of malignant neovascularization suggests that this may prove to be the case. Obviously cirrhosis will be a source of false positives as will the other benign conditions know to have such shunts, but haemangiomas, at least of the adult type, seem to have a normal transit time. This method relies on a similar haemodynamic changes to the Doppler perfusion index and the relative advantages of the two approaches remains to be evaluated.
Cancer Imaging. 2015 May 5;1(1):77–85.
Imaging liver metastases: current limitations and future prospects for CT and MRI
Liver metastases from extra-hepatic primary tumours arrive as cellular emboli in arterial or portal venous blood. Histopathological studies suggest that these clumps of tumour cells lodge in the pre-sinusoidal arterioles, terminal portal venules, in the sinusoids themselves, or in the adjacent spaces of Disse. Factors favouring the liver as a fertile ground for seeding metastatic tumours include its high volume blood flow (about 25% of cardiac output), its favourable microscopic anatomy — liver sinusoids are of suitable size for trapping cells and there are gaps of similar size in the sub-endothelial basement membrane — and its rich biochemical environment which favours rapid growth. The rate at which microscopic metastases enlarge is variable and depends, inter alia, on the site of the primary tumour, its histological cell type, its grade of malignancy, the presence of sub-populations of different cell types, and probably also on local environmental factors within the liver. The observation of tumour emboli in terminal branches of the portal vein is one which is well established[1,2] and there seems to be no doubt that all liver metastases start out as tumours of microscopic size.
The sensitivity of imaging is usually overstated
The sensitivities of CT and MRI are typically quoted as 85–90% and CTAP at 85–95%. How can these figures be true when all metastases start out as microscopic deposits and the physical limitations of imaging methods are well known? Plainly the answer is that the observation of ‘85% sensitivity’ is a measure not just of the imaging test, but also of the reference standard against which imaging is judged. This explains why recent and continuing improvements in imaging technology, with resolution of smaller and smaller lesions, have resulted in little or no improvement in apparent sensitivity, because the reference standards are also improving at about the same rate. In parallel with this is a trend to study patients with early disease, so that the current challenge for radiology is to detect smaller and smaller lesions at an earlier and earlier stage of growth. The difficulty we have is that non-invasive imaging is now approaching the accuracy of direct surgical examination of the liver, and of the conventional pathological approach to liver lesions.
The reference standards are limited
In a post-mortem study of 150 livers containing metastases, it was found that 11% of livers looked and felt normal at the surface but contained deep-seated lesions on sectioning[3]. In an autopsy study of patients who died within a month of primary surgery for colorectal cancer Goligher[4] found that five of 31 livers which had been ‘normal’ at laparotomy were shown to contain occult metastases on pathological examination. In a CT follow-up study of the growth rate of colorectal liver metastases, Finlay et al.[5] estimated that the mean age of synchronous liver metastases at the time of surgery was 2–3 years, but even so a majority of the lesions in this study were not detected at laparotomy, although they were visible on early post-operative CT. The conventional approach to pathological examination of the intact liver is to slice the organ at intervals of about 1 cm, with inspection and palpation of each slice. It is easy to see how lesions of sub-millimetre size are overlooked.
The quoted sensitivity of imaging methods should be regarded not as an absolute figure with any independent validity, but as a comparative value related to reference standards which in the best studies are definable and explicit, but unfortunately in other studies are imprecise. Historical comparisons are of little value as not only have the reference standards for assessment of imaging methods been improving in parallel with imaging technology, but the availability of imaging has produced a shift in the selection of patients so that we are now seeing much earlier disease than in the past.
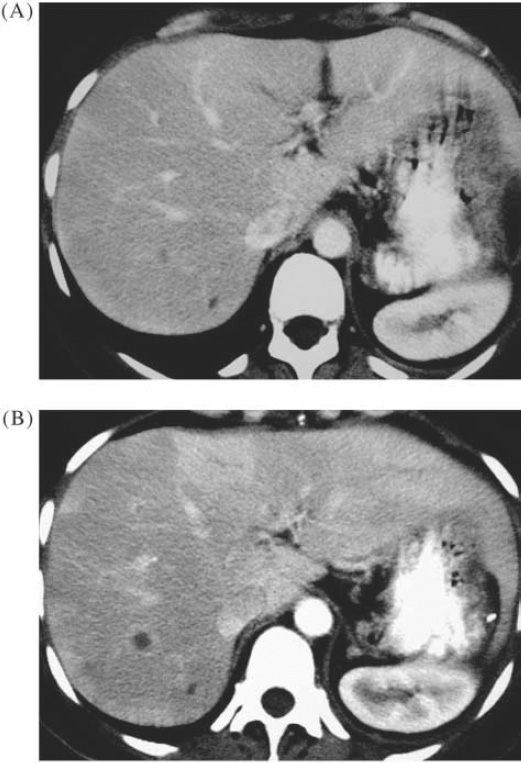
Metastasis from ovarian cancer. (A) CT showed lesions which are too small to characterize reliably; (B) CT 9 months later showed growth of metastasis.
The sensitivity of imaging depends on the size of the lesions
Correlation with whole liver pathology at autopsy or after transplantation is rarely achievable, so the best reference standard for most imaging studies is surgical exploration with intra-operative ultrasound. With this approach, current imaging is shown to be very successful for lesions larger than 1 cm, but relatively poor for smaller lesions. In a recent multi-observer study comparing dual phase spiral CT with SPIO-enhanced MRI for detection of colorectal metastases, we found these techniques to have sensitivities of 94% and 99% respectively for detecting lesions larger than 1 cm[6]. However, when considering lesions smaller than 1 cm (which were still detected surgically or by intra-operative ultrasound) the sensitivities of SPIO-enhanced MRI and dual phase spiral CT were about 60% and 45%, respectively. In this study about one third of all the lesions detected were smaller than 1 cm. In other studies in which lesions smaller than 1 cm have been specifically identified, sensitivity of detection by imaging methods has been equally unsatisfactory[7]. CT arterio-portography (CTAP) has been shown to be more sensitive for small lesions than either CT with intravenous contrast enhancement, or MRI[8,9]. However, CTAP is invasive and produces more false positives than the other techniques[10]. Further, recent studies have suggested that spiral CT with intravenous enhancement will detect as many lesions as CTAP with fewer false positives[11], that CTAP is insensitive for lesions smaller than 1 cm[12], and also that SPIO-enhanced MRI is at least as accurate as CTAP[13]. So, we should currently expect to demonstrate metastases of 1 cm or larger with a sensitivity approaching 100% using SPIO-enhanced MRI, and sensitivity of 90–95% using spiral CT. The sensitivity of imaging methods for detecting lesions smaller than 1 cm is in the region of 50% when surgery with IOUS is used as the gold standard, but the ‘true’ accuracy of the reference standard itself cannot be established at present.
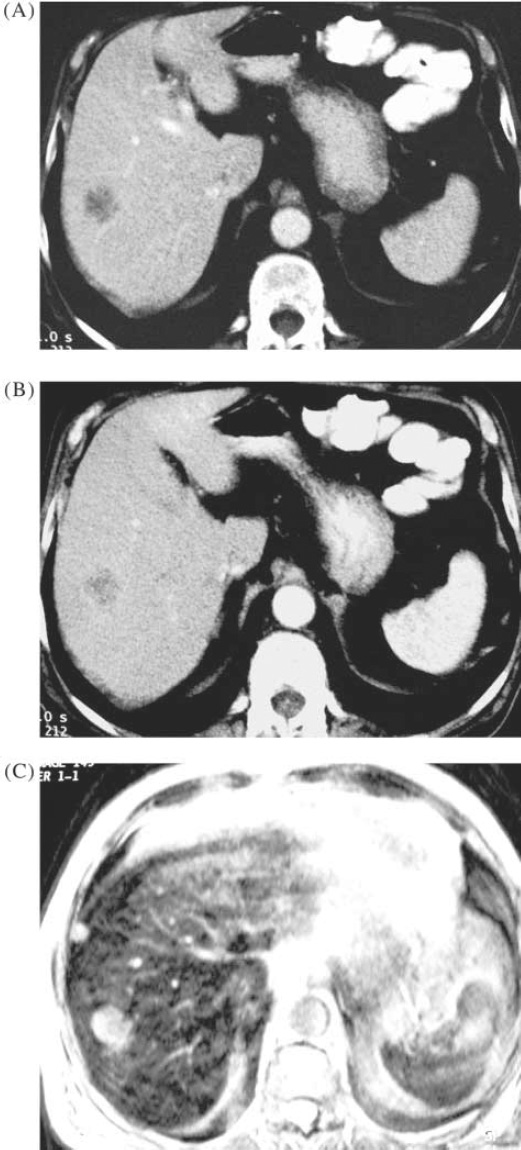
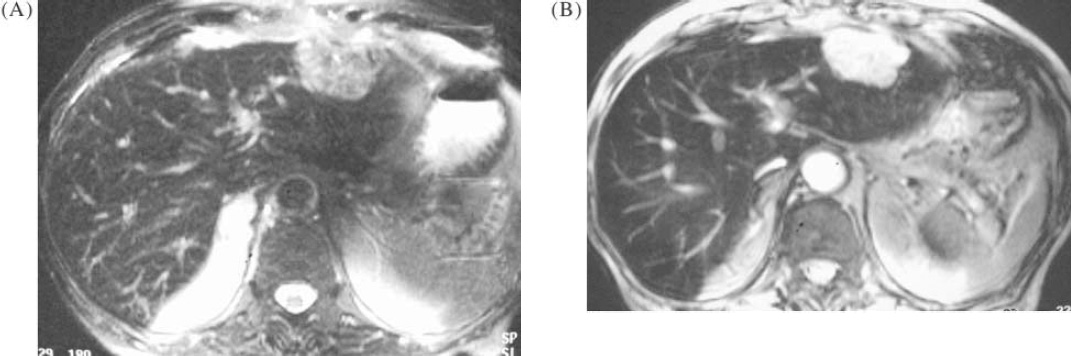
Colorectal metastases. Arterial phase CT (A) and portal phase CT (B) show a single metastasis. SPIO-enhanced MRI (C) shows an additional 1 cm lesion.
Optimizing current imaging techniques
MRI
There is now good evidence that superparamagnetic iron oxide (SPIO) enhanced MRI offers the most sensitive method for detecting small liver lesions. Optimization of SPIO enhancement requires careful consideration of the type of sequence used and the dose of contrast given. SPIO effects depend on susceptibility changes in liver parenchyma which increase with higher field strength so that when spin echo sequences are used, T2-weighted images are most appropriate at 0.5 T, whilst at 1.5 T proton density or T1-weighted images[7,14] may be more effective. Susceptibility effects are smaller with turbo spin echo (TSE) acquisitions so the effect of SPIO enhancement is less, whilst gradient echo sequences are more sensitive to susceptibility and are more appropriate with SPIO.
CT
Optimum technique for liver CT requires consideration of the volume and rate of contrast medium injection, the use of single or multiple phases of acquisition, and the trade off between beam collimation and table pitch to produce the most effective resolution in a single breath-hold acquisition. The timing of acquisition also needs careful planning. With a conventional single detector array, single breath-hold volume acquisition to encompass the whole liver requires beam collimation of 5–8 mm (thinner slices show better spatial resolution but worse contrast resolution), table pitch of 1–2 (theoretical optimum is about 1.4) and an interval of 25–30 s between the end of contrast injection (100–150 ml at 4–5 ml/s) and the start of portal phase acquisition. The addition of arterial-dominant phase acquisition shows clear advantages for hypervascular metastases (e.g. from islet cell tumours of the pancreas, carcinoids, phaeochromocytoma, melanoma and renal cell cancer) but the advantages of dual phase imaging are less clear-cut for patients with breast, lung, and colorectal primaries. The recent introduction of multidetector CT allows more rapid acquisition of thinner slices, or alternatively a faster time constant to allow more dynamic phases to be obtained. The advantages of both approaches may be constrained by considerations of increasing radiation dose, but even so it is likely that improvements in both detection and characterization of sub-centimetre lesions will be demonstrable with multidetector devices.
MR technique with SPIO. (A) T2-weighted FSE sequence shows large metastasis in left lobe; (B) optimized gradient echo T2 shows improved contrast between the tumour and normal liver, better visualization of vascular structures, and an additional lesion in segment 8.
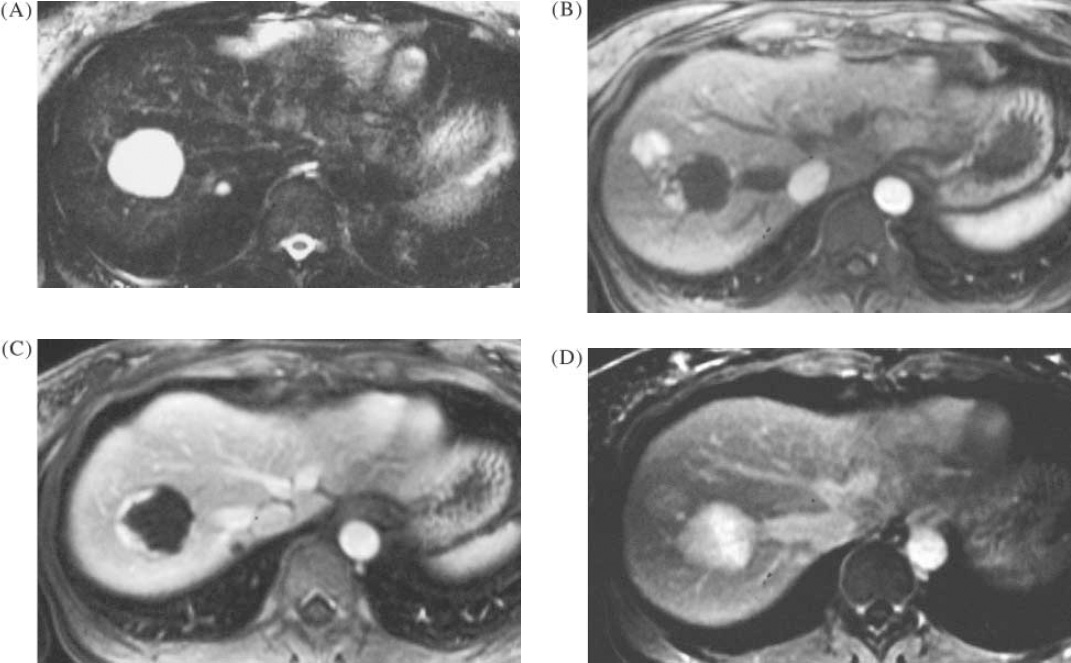
Benign liver lesions in a patient with colorectal cancer. (A) TSE T2 image showing 3 cm lesion which was indeterminate on ultrasound, also a second lesion of 7 mm. (B) and (C) T1-weighted image with gadolinium enhancement, arterial phases, showing typical peripheral nodular enhancement in the larger lesion but also an additional hypervascular lesion. Delayed post-gadolinium T1 image showing complete infilling of the 3 cm and 7 mm lesions, typical for haemangioma, and a faint persistent stain in the hypervascular lesion, suggestive of focal nodular hyperplasia. The FNH lesion was undetected on T2-weighted MRI, and also on ultrasound.
The smallest lesions visible on contrast enhanced MR and CT are currently of the order of 3–4 mm diameter, although the majority of metastases in this size range are not visualized. Surgical examination and intra-operative ultrasound may detect lesions down to about 2 mm size, if they are close to the liver surface.
Distinguishing benign focal lesions from metastases
The increasing use of non-invasive liver imaging has resulted in the much more frequent discovery of focal lesions in patients with no signs or symptoms of liver disease. When large, their features are usually sufficiently characteristic to distinguish from primary or secondary liver tumours, but with small lesions this distinction is more difficult. Incidental lesions in patients with no suspicion of primary malignancy are almost invariably benign[15], but small lesions seen in patients undergoing staging procedures or surveillance following treatment of primary malignancy turn out to be metastatic in about 10% of cases[16]. Techniques for identifying specific benign pathologies in the liver include:
in-phase and opposed-phase T1-weighted MRI — to identify areas of focal fatty change, or areas of focal sparing in a diffusely fatty liver;
dynamic Gd-enhanced MRI — to identify characteristic peripheral nodular enhancement in haemangiomas, to demonstrate focal perfusion changes due to non-portal splanchnic venous inflow, and to demonstrate a complete lack of enhancement in simple cysts;
pre- and post-SPIO T2-weighted MRI — to identify uptake of SPIO in benign hepatocellular lesions, particularly focal nodular hyperplasia.