

ABSTRACT
Previous studies evaluated various risk factors for knee OA; however, no study has examined the association between spinal factors, such as total spinal alignment and spinal range of motion (ROM), with knee OA. The purpose of this study was to examine the influence of spinal factors including total spinal alignment and spinal ROM on knee OA in community-living elderly subjects. A total of 170 subjects ≥60 years old (mean age 69.4 years, 70 males and 100 females) enrolled in the study (Yakumo study) and underwent a basic health checkup. We evaluated A-P knee radiographs, sagittal parameters (thoracic kyphosis angle, lumbar lordosis angle, and spinal inclination angle) and spinal mobility (thoracic spinal ROM, lumbar spinal ROM and total spinal ROM) as determined with SpinalMouse®. The radiological assessment of knee OA was based on the Kellgren and Lawrence classification, and the knee flexion angle was measured while the subject was standing. Spinal inclination angle and thoracic spinal ROM correlated significantly with knee OA on univariate analyses. Multivariate logistic regression analysis indicated that an increase in spinal inclination angle (OR 1.073, p<0.05) was significantly associated with knee OA. Spinal inclination angle had significant positive correlation with knee flexion angle (r=0.286, p<0.001). The spinal inclination angle is the most important factor associated with knee OA.
Key Words: spinal imbalance, spinal inclination, knee osteoarthritis, elderly, knee-spine syndrome
INTRODUCTION
Knee Osteoarthritis (OA), a disease with regressive changes in the articular cartilage of the knee, is a clinical and public health problem in the elderly due to increasing medical and nursing care costs. There have been many studies on knee OA that have looked at ways to prevent and appropriately treat these patients. Studies evaluating risk factors for knee OA have reported older age, female sex, obesity, muscle strength, higher BMD, previous knee injury, genetic factors, oxidative stress and smoking as risk factors.1-13)However, few studies have examined the relationship between spinal factors and knee joint disorders in elderly people.14-17) Furthermore, to the best of our knowledge, no previous study has examined the association between spinal factors, such as total spinal alignment and spinal range of motion (ROM), and how they affect knee OA. Therefore, the objective of this study was to investigate the relationship between total spinal alignment, spinal ROM and knee OA in elderly subjects by screening a community population.
MATERIALS AND METHODS
The subjects were healthy volunteers who attended a basic health checkup supported by a local government in 2011. This checkup (Yakumo study) has been conducted in the town of Yakumo in a rural area of southern Hokkaido, Japan every August since 1982. The current study involved 170 subjects ≥60 years old (70 males and 100 females) who received examinations that included posteroanterior (PA) weight-bearing knee radiographs made with the knee in 45 degrees of flexion and the use of SpinalMouse® (Idiag, Volkerswill, Switzerland) for determining sagittal alignment of the total spine and spinal mobility. The knee flexion angle between the femoral axis (from the greater trochanter to the lateral condyle) and the tibial axis (from the head of the fibula to the lateral malleolus) was measured with a goniometer while the subject was standing. The average age of the subjects was 69.4 years old (range: 60~89). Subjects with a history of spinal or knee surgery, severe knee injury, Parkinson’s disease, and spinal compression fracture were excluded from the study. The study was approved by the Committee on Ethics in Human Research of Nagoya University.
Evaluation of spinal alignment and range of motion using SpinalMouse®
Spinal alignment and range of motion (ROM) were measured using SpinalMouse®, an electronic computer-aided device that noninvasively measures sagittal spinal ROM and intersegmental angles using the so-called surface technique. Intraclass coefficients of 0.92–0.95 have been determined for curvature measurement made with SpinalMouse®.18) In the current study, we measured each angle three times in a neutral standing position, maximum bending position and maximum extension position, and then used average data in our analyses. The evaluation items included the thoracic kyphosis angle (T1-T12), lumbar lordosis angle (T12-L5), spinal inclination angle, thoracic ROM, lumbar ROM and total spinal ROM. Spinal inclination angle was defined as the angle between a plumb line and a straight line from the first thoracic vertebra to the first sacral vertebra (Figure 1). A greater spinal inclination angle reflected a forward, stooped posture which gives poor sagittal balance. When evaluating the SpinalMouse® data, we found a significant correlation with the lumbar radiographic findings for the lumbar lordosis angle (r = 0.546, p < 0.0001), though the average lumbar lordosis angle estimated by the SpinalMouse® was smaller than that derived from plain radiograph. This finding indicates that the SpinalMouse® is still useful and acceptable for evaluating the spine ROM and total spine alignment, as described in the literature,18-25) although SpinalMouse® estimation of the angles is not compatible with that derived from plain radiographs. Thus, we decided to use the SpinalMouse® measurements of spine parameters for analyses in this study. The thoracic kyphosis and lumbar lordosis angles are shown as positive values in this study.
Fig. 1.
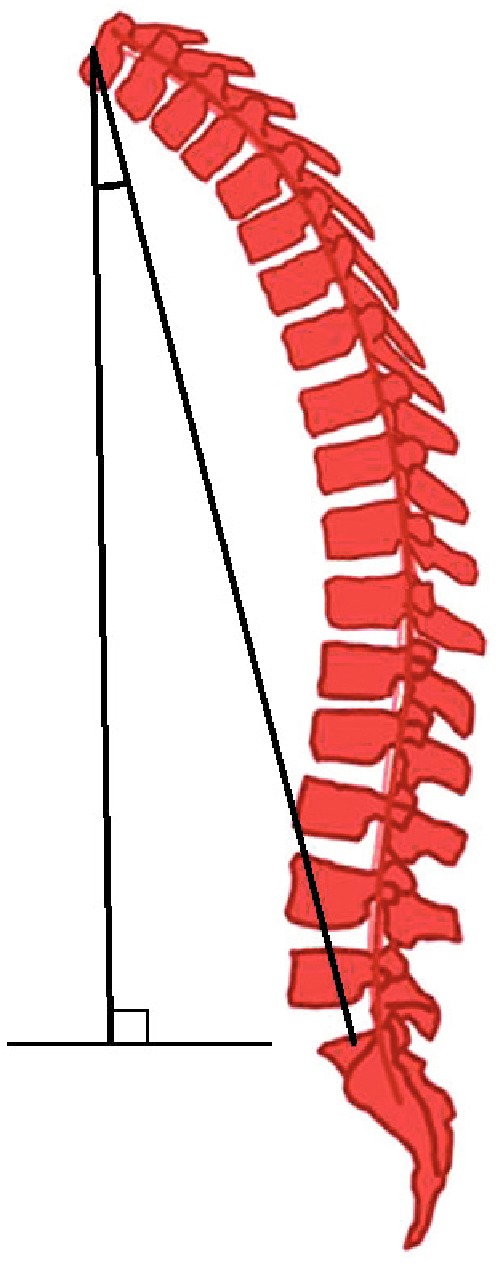
Spinal inclination angle. The angle between a plumb line and a straight line from the first thoracic vertebra to the first sacral vertebra.
Radiographic evaluation of knee OA
Radiographic examinations were performed on PA weight-bearing knee radiographs made with the knee in 45 degrees of flexion, according to Rosenberg et al. 26) The radiological assessment was based on the Kellgren and Lawrence (K-L) classification based on the presence or absence of a narrowed joint space, osteophyte formation and osteonecrosis, with each knee joint being graded from 0 to grade 4.27) A knee joint with grade 0 has no radiographic findings of OA, grade 1 has slight or unclear osteophyte formation, grade 2 has definite bony proliferative changes in the absence of a narrowed joint space, grade 3 has moderate joint space narrowing and grade 4 has more pronounced narrowing of the joint space associated with osteosclerosis of the subchondral bone. Subjects were categorized to the OA group if either knee was graded K-L grade ≥2. The no-OA group was defined as showing radiographic findings of K-L 0 or 1 in either knee.
Statistical Analysis
All data are shown as means ± standard deviation (SD) and were analyzed using SPSS Ver. 20 (SPSS, Chicago, IL, USA). An unpaired t test and Chi-square test was used to evaluate differences between the knee OA (+) and knee OA (–) groups for univariate analyses. We performed multivariate logistic regression analysis to evaluate the odds ratio (OR) with 95% confidence interval (95% CI) for potential risk factors for the occurrence of knee OA. Variables were included in a multiple logistic regression model if their univariate analysis p value was <0.20. We used Pearson’s correlation coefficient analysis for determining variables. The threshold for significance was a p value of <0.05.
RESULTS
The basic characteristics of the subjects are listed in Table 1. A comparison of the subjects with and without knee OA determined by univariate analyses is shown in Table 2. There were 33 subjects (6 males and 27 females) defined as having knee OA. The average age of subjects in the knee OA (+) group was significantly higher than the knee OA (–) group (Table 2). There were significantly more females in the knee OA (+) group than in the knee OA (–) group. When univariate analyses of the spinal factors were performed in the knee OA (+), we identified spinal inclination angle, thoracic spinal ROM, and knee flexion angle as significant factors associated with the knee OA (+) (Table 2). Multivariate logistic regression analysis of selected variables related to spinal factors from the univariate analyses revealed that the spinal inclination angle was the only significant parameter associated with knee OA (+) (Table 3). This suggests that an increase in the spinal inclination angle is related to an increase in the occurrence of knee OA. We evaluated the correlations among variables as well; spinal inclination angle had significant negative correlations with lumbar lordosis angle (r=–0.593, p<0.01), lumbar spinal ROM (r=–0.283, p<0.01) and total spinal ROM (r=–0.166, p<0.05), and it had positive correlation with knee flexion angle (r=0.286, p<0.001) (Table 4).
Table 1.
Clinical background of the subjects
| Item | Value |
|---|---|
| Total number | 170 |
| Male/Female | 70/100 |
| Age (years) | 69.4 (6.9) |
| BMI (kg/cm2) | 23.2 (3.0) |
| Spinal alignment | |
| Thoracic kyphosis angle (°) | 41.5 (9.8) |
| Lumbar lordosis angle (°) | 18.7 (11.3) |
| Spinal inclination angle (°) | 3.5 (5.5) |
| Spinal ROM | |
| Thoracic spinal ROM (°) | 24.5 (12.0) |
| Lumbar spinal ROM (°) | 45.0 (15.4) |
| Total spinal ROM (°) | 93.7 (22.6) |
Values are shown as the number of subjects or as the mean (SD).
BMI=body mass index, ROM=range of motion
Table 2.
Difference in variables between subjects with and without knee OA
| Variables | Knee OA (+) | Knee OA (–) | Significance (p) |
|---|---|---|---|
| Subjects number | n=33 | n=137 | |
| Age (years) | 72.8±7.1 | 68.6±6.5 | 0.002* |
| Male/Female | 6/27 | 59/78 | 0.003* |
| BMI (kg/cm2) | 24.4±3.2 | 22.9±2.9 | 0.245 |
| Spinal alignment | |||
| Thoracic kyphosis angle (°) | 43.2±10.7 | 41.1±9.5 | 0.174 |
| Lumbar lordosis angle (°) | 17.8±9.7 | 18.9±11.7 | 0.785 |
| Spinal inclination angle (°) | 5.2±4.0 | 3.1±5.7 | <0.001* |
| Spinal ROM | |||
| Thoracic spinal ROM (°) | 19.9±9.4 | 25.6±12.3 | 0.011* |
| Lumbar spinal ROM (°) | 44.4±14.2 | 45.1±15.7 | 0.884 |
| Total spinal ROM (°) | 99.4±20.4 | 92.3±22.9 | 0.106 |
| Knee flexion angle (°) | 1.5±4.3 | 0.3±1.6 | 0.012* |
Values are shown as the mean (SD) or the number of subjects.
OA=osteoarthritis
Asterisk indicates significant difference.
Table 3.
Results of multivariate logistic regression analysis for risk of knee OA
| Parameter | OR | 95% CI | Significance (p) |
|---|---|---|---|
| Thoracic kyphosis angle | 1.02 | 0.978–1.064 | 0.174 |
| Spinal inclination angle (°) | 1.073 | 1.005–1.146 | 0.035* |
| Thoracic spinal ROM (°) | 0.971 | 0.935–1.008 | 0.124 |
| Total spinal ROM (°) | 1.013 | 0.994–1.032 | 0.168 |
OR=odds ratio, CI=confidence interval
Asterisk indicates significant difference.
Table 4.
Correlations between measured variables
| Variables | Thoracic kyphosis angle (°) |
Lumbar lordosis angle (°) |
Spinal inclination angle (°) |
Thoracic spinal ROM (°) |
Lumbar spinal ROM (°) |
Total spinal ROM (°) |
Knee flexion angle (°) |
|---|---|---|---|---|---|---|---|
| Thoracic kyphosis angle (°) | 0.424** | –0.082 | –0.237** | 0.110 | 0.017 | –0.174* | |
| Lumbar lordosis angle (°) | –0.593** | –0.091 | 0.351** | 0.220** | –0.271*** | ||
| Spinal inclination angle (°) | –0.069 | –0.283** | –0.166* | 0.286*** | |||
| Thoracic spinal ROM (°) | –0.387** | –0.334** | –0.145 | ||||
| Lumbar spinal ROM (°) | 0.507** | –0.140 | |||||
| Total spinal ROM (°) | –0.144 | ||||||
| Knee flexion angle (°) |
Data represent Pearson’s correlation coefficient.
*p<0.05, ** p<0.01, *** p<0.001
DISCUSSION
The interrelationship between a pathological state of the knee joint and spinal alignment was first reported by Itoi et al. 14) By analyzing lateral radiographic films of the whole spine and lower extremities in osteoporotic patients, they found that individuals with thoracic kyphosis, a primary deformity of the osteoporotic spine, appeared to compensate with knee flexion along with the lumbar spine, sacroiliac joint and hip joint. On the other hand, Tsuji et al. reported that the presence of patella-femoral pain correlated well with sacral inclination and knee flexion position and also with changes in lumbar kyphosis. Furthermore, they called this significant correlation between lumbar kyphosis and knee flexion position as the knee-spine syndrome.15) Similarly, Murata et al. performed radiological examinations of the lumbar spine in a standing position to evaluate the relationship between lumbar lordosis and degenerative changes of the knee joint. They suggested that degenerative changes in the knee might be a factor in the development of similar changes in the lumbar spine with loss of lordosis and this might be called the "knee spine syndrome".16) However, both of these studies used the presence of patella-femoral pain and/or knee flexion position, not radiographic evidence of knee OA, as the determinant of a knee joint disorder. They also evaluated the association between sagittal alignment of the spine and knee joint using only radiographs of the lumbar spine. Looking at whole spinal balance, Harato et al. examined ten healthy females in a gait analysis of simulated knee flexion contracture to elucidate the knee-spine syndrome. Results of their study suggested knee flexion contracture significantly influenced three-dimensional trunk kinematics and would lead to spinal imbalance.17) In the current study, we demonstrated, for the first time, the relationship between total spinal factors and the occurrence of radiographic knee OA in elderly subjects.
The present study demonstrated that increased spinal inclination angle was an independent factor related to knee OA in the elderly in multivariate analysis. In addition, decreased lumbar lordosis, decreased spinal ROM, and increased knee flexion angle had significant correlations with an increased spinal inclination angle. In contrast, we found that the thoracic kyphosis angle was not a significantly important factor in the occurrence of knee OA and did not correlate with the spinal inclination angle, whereas, lumbar lordosis, lumbar spinal ROM and total spinal ROM correlated significantly with the spinal inclination angle. As we found in a previous study, elderly people have difficulty maintaining sagittal balance due to inflexibility of the spine which results in decompensated sagittal balance.21)
We speculate that a relationship exists between knee OA and the spinal inclination angle, but we are unsure which factor arose first. In an elderly person with an increased spinal inclination angle, head bent forward, and sagittal imbalance, the individual must maintain hip and knee flexion to preserve their global sagittal alignment and stand appropriately on their feet (Figure 2). The knee joint becomes overloaded in a flexed position, and this continuous overload leads to knee OA, which may be referred to as the spine-knee syndrome. On the other hand, if an elderly person had knee OA first, they would stand in a slouched position with their knees flexed, which can be referred to as the knee-spine syndrome (Figure 3). This study demonstrated a significant relationship between increased spinal inclination angle and knee OA, which forms a basis for further investigation into this issue.
Fig. 2.
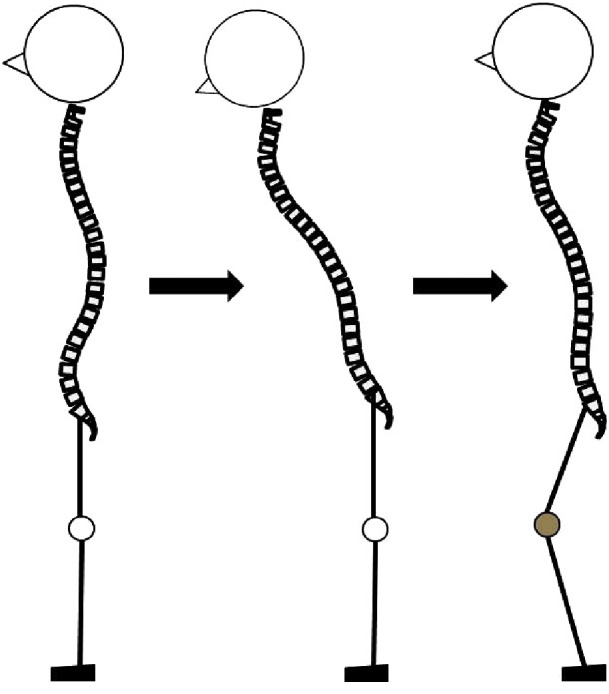
Spine-knee syndrome. An increased spinal inclination angle with the head bent forward and sagittal imbalance must maintain hip and knee flexion to preserve their global sagittal alignment.
Fig. 3.
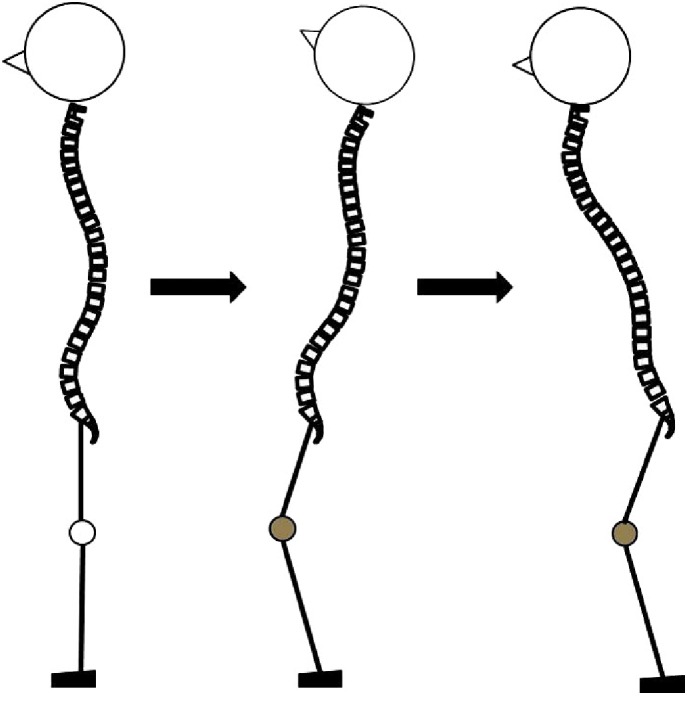
Knee-spine syndrome. An elderly person with knee OA should stand in a slouched position with their knee flexed.
This study had several limitations. First, the number of subjects in our study was relatively small. Second, radiographs of the entire spine, hips and ankle joints were not performed. Ideally, full radiographic examination of the entire spine would be useful for a complete evaluation of sagittal alignment, and hip radiographs or radiographs of the lower limbs on standing would be useful for evaluating total sagittal alignment of the lower extremities. Thus, we were unable to properly evaluate the correlation between knee OA and real alignment in these volunteers. Third, we could not determine the real cause of spinal imbalance because we did not perform radiographs of the thoracic and thoracolumbar area. Although subjects with a history of spinal compression fracture were excluded from the study, some elderly people might have asymptomatic osteoporotic fractures due to bone density loss, and this condition leads to spinal imbalance. However, radiographs of the chest, whole spine, and hip/knee joints would have exposed healthy people to an unnecessary amount of radiation. We believe that SpinalMouse® is a useful tool for checking the health of the spine because subjects are not exposed to radiation. SpinalMouse® is a simple and noninvasive device that has been shown to be reliable in many studies.18-25) Thus, this may be sufficient as the first study demonstrating the relationships between total spinal factors and knee OA in elderly subjects.
CONCLUSION
This is the first study that examined the relationships between total spinal alignment, spinal ROM and knee OA in elderly subjects. The spinal inclination angle is the most important factor associated with knee OA, although spinal ROM is also associated with knee OA. Decreased lumbar lordosis and lumbar ROM is related to increased spinal inclination angle.
ACKNOWLEDGEMENT
We are grateful to the staff of the Comprehensive Health Care Program held in Yakumo, Hokkaido.
We also thank Ms. Kae Shikii and Ms. Saho Horiuchi of Nagoya University for their assistance of data collection.
CONFLICT OF INTEREST
The authors have no financial conflicts of interest.
REFERENCES
- 1).Blagojevic M, Jinks C, Jeffery A, Jordan KP. Risk factors for onset of osteoarthritis of the knee in older adults: a systematic review and meta-analysis. Osteoarthritis Cartilage, 2010; 18: 24–33. [DOI] [PubMed]
- 2).Burger H, van Daele PL, Odding E, Valkenburg HA, Hofman A, Grobbee DE, Schutte HE, Birkenhager JC, Pols HA. Association of radiographically evident osteoarthritis with higher bone mineral density and increased bone loss with age. The Rotterdam Study. Arthritis Rheum, 1996; 39: 81–86. [DOI] [PubMed]
- 3).Davis MA, Ettinger WH, Neuhaus JM, Cho SA, Hauck WW. The association of knee injury and obesity with unilateral and bilateral osteoarthritis of the knee. Am J Epidemiol, 1989; 130: 278–288. [DOI] [PubMed]
- 4).Hart DJ, Doyle DV, Spector TD. Incidence and risk factors for radiographic knee osteoarthritis in middle-aged women: the Chingford Study. Arthritis Rheum, 1999; 42: 17–24. [DOI] [PubMed]
- 5).Ikeda T, Mabuchi A, Fukuda A, Kawakami A, Ryo Y, Yamamoto S, Miyoshi K, Haga N, Hiraoka H, Takatori Y, Kawaguchi H, Nakamura K, Ikegawa S. Association analysis of single nucleotide polymorphisms in cartilage-specific collagen genes with knee and hip osteoarthritis in the Japanese population. J Bone Miner Res, 2002; 17: 1290–1296. [DOI] [PubMed]
- 6).Loeser RF, Carlson CS, Del Carlo M, Cole A. Detection of nitrotyrosine in aging and osteoarthritic cartilage: Correlation of oxidative damage with the presence of interleukin-1beta and with chondrocyte resistance to insulin-like growth factor 1. Arthritis Rheum, 2002; 46: 2349–2357. [DOI] [PubMed]
- 7).Muraki S, Akune T, Oka H, Ishimoto Y, Nagata K, Yoshida M, Tokimura F, Nakamura K, Kawaguchi H, Yoshimura N. Incidence and risk factors for radiographic knee osteoarthritis and knee pain in Japanese men and women: a longitudinal population-based cohort study. Arthritis Rheum, 2012; 64: 1447–1456. [DOI] [PubMed]
- 8).Seki T, Hasegawa Y, Yamaguchi J, Kanoh T, Ishiguro N, Tsuboi M, Ito Y, Hamajima N, Suzuki K. Association of serum carotenoids, retinol, and tocopherols with radiographic knee osteoarthritis: possible risk factors in rural Japanese inhabitants. J Orthop Sci, 2010; 15: 477–484. [DOI] [PubMed]
- 9).Slemenda C, Heilman DK, Brandt KD, Katz BP, Mazzuca SA, Braunstein EM, Byrd D. Reduced quadriceps strength relative to body weight: a risk factor for knee osteoarthritis in women? Arthritis Rheum, 1998; 41: 1951–1959. [DOI] [PubMed]
- 10).Sudo A, Miyamoto N, Horikawa K, Urawa M, Yamakawa T, Yamada T, Uchida A. Prevalence and risk factors for knee osteoarthritis in elderly Japanese men and women. J Orthop Sci, 2008; 13: 413–418. [DOI] [PubMed]
- 11).Wilder FV, Hall BJ, Barrett JP, Jr., Lemrow NB. History of acute knee injury and osteoarthritis of the knee: a prospective epidemiological assessment. The Clearwater Osteoarthritis Study. Osteoarthritis Cartilage, 2002; 10: 611–616. [DOI] [PubMed]
- 12).Yoshimura N, Nishioka S, Kinoshita H, Hori N, Nishioka T, Ryujin M, Mantani Y, Miyake M, Coggon D, Cooper C. Risk factors for knee osteoarthritis in Japanese women: heavy weight, previous joint injuries, and occupational activities. J Rheumatol, 2004; 31: 157–162. [PubMed]
- 13).Yudoh K, Nguyen v T, Nakamura H, Hongo-Masuko K, Kato T, Nishioka K. Potential involvement of oxidative stress in cartilage senescence and development of osteoarthritis: oxidative stress induces chondrocyte telomere instability and downregulation of chondrocyte function. Arthritis Res Ther, 2005; 7: R380–391. [DOI] [PMC free article] [PubMed]
- 14).Itoi E. Roentgenographic analysis of posture in spinal osteoporotics. Spine, 1991; 16: 750–756. [DOI] [PubMed]
- 15).Tsuji T, Matsuyama Y, Goto M, Yimin Y, Sato K, Hasegawa Y, Ishiguro N. Knee-spine syndrome: correlation between sacral inclination and patellofemoral joint pain. J Orthop Sci, 2002; 7(5): 519–523. [DOI] [PubMed]
- 16).Murata Y, Takahashi K, Yamagata M, Hanaoka E, Moriya H. The knee-spine syndrome. Association between lumbar lordosis and extension of the knee. J Bone Joint Surg Br, 2003; 85: 95–99. [DOI] [PubMed]
- 17).Harato K, Nagura T, Matsumoto H, Otani T, Toyama Y, Suda Y. A gait analysis of simulated knee flexion contracture to elucidate knee-spine syndrome. Gait Posture, 2008; 28: 687–692. [DOI] [PubMed]
- 18).Post RB, Leferink VJ. Spinal mobility: sagittal range of motion measured with the SpinalMouse, a new non-invasive device. Arch Orthop Trauma Surg, 2004; 124: 187–192. [DOI] [PubMed]
- 19).Imagama S, Matsuyama Y, Hasegawa Y, Sakai Y, Ito Z, Ishiguro N, Hamajima N. Back muscle strength and spinal mobility are predictors of quality of life in middle-aged and elderly males. Eur Spine J, 2011; 20: 954–961. [DOI] [PMC free article] [PubMed]
- 20).Hirano K, Imagama S, Hasegawa Y, Wakao N, Muramoto A, Ishiguro N. Impact of spinal imbalance and back muscle strength on locomotive syndrome in community-living elderly people. J Orthop Sci, 2012; 17: 532–537. [DOI] [PubMed]
- 21).Imagama S, Hasegawa Y, Matsuyama Y, Sakai Y, Ito Z, Hamajima N, Ishiguro N. Influence of sagittal balance and physical ability associated with exercise on quality of life in middle-aged and elderly people. Arch Osteoporos, 2011; 6: 13–20. [DOI] [PMC free article] [PubMed]
- 22).Imagama S, Hasegawa Y, Wakao N, Hirano K, Hamajima N, Ishiguro N. Influence of lumbar kyphosis and back muscle strength on the symptoms of gastroesophageal reflux disease in middle-aged and elderly people. Eur Spine J, 2012; 21: 2149–2157. [DOI] [PMC free article] [PubMed]
- 23).Imagama S, Ito Z, Wakao N, Seki T, Hirano K, Muramoto A, Sakai Y, Matsuyama Y, Hamajima N, Ishiguro N, Hasegawa Y. Influence of spinal sagittal alignment, body balance, muscle strength, and physical ability on falling of middle-aged and elderly males. Eur Spine J, 2013; 22(6): 1346–1353. [DOI] [PMC free article] [PubMed]
- 24).Post RB, Leferink VJ. Sagittal range of motion after a spinal fracture: does ROM correlate with functional outcome? Eur Spine J, 2004; 13: 489–494. [DOI] [PMC free article] [PubMed]
- 25).Imagama S, Hasegawa Y, Wakao N, Hirano K, Muramoto A, Ishiguro N. Impact of spinal alignment and back muscle strength on shoulder range of motion in middle-aged and elderly people in a prospective cohort study. Eur Spine J, 2014; 23(7): 1414–1419. [DOI] [PubMed]
- 26).Rosenberg TD, Paulos LE, Parker RD, Coward DB, Scott SM. The forty-five-degree posteroanterior flexion weight-bearing radiograph of the knee. J Bone Joint Surg Am, 1988; 70: 1479–1483. [PubMed]
- 27).Kellgren JH, Lawrence JS. Radiological assessment of osteo-arthrosis. Ann Rheum Dis, 1957; 16: 494–502. [DOI] [PMC free article] [PubMed]