

Abstract
Objective
The decline in available oestrogen after menopause is a possible etiological factor in pelvic floor disorders like vaginal atrophy (VA), urinary incontinence (UI), overactive bladder (OAB) and pelvic organ prolapse (POP). This systematic review will examine the evidence for local oestrogen therapy in the treatment of these pelvic floor disorders.
Evidence Acquisition
We performed a systematic search in MEDLINE, EMBASE, the Cochrane Central Register of Controlled Trials and the non-MEDLINE subset of PubMed from inception to May 2014. We searched for local oestrogens and VA (I), UI/OAB (II) and POP (III). Part I was combined with broad methodological filters for randomized controlled trials (RCTs) and secondary evidence. For part I and II two reviewers independently selected RCTs evaluating the effect of topical oestrogens on symptoms and signs of VA and UI/OAB. In part III all studies of topical oestrogen therapy in the treatment of POP were selected. Data extraction and the assessment of risk of bias using the Cochrane Risk of Bias Tool was undertaken independently by two reviewers.
Evidence Synthesis
The included studies varied in ways of topical application, types of oestrogen, dosage and treatment durations. Objective and subjective outcomes were assessed by a variety of measures. Overall, subjective and urodynamic outcomes, vaginal maturation and vaginal pH changed in favor of vaginal oestrogens compared to placebo. No obvious differences between different application methods were revealed. Low doses already seemed to have a beneficial effect. Studies evaluating the effect of topical oestrogen in women with POP are scarce and mainly assessed symptoms and signs associated with VA instead of POP symptoms.
Conclusion
Topical oestrogen administration is effective for the treatment of VA and seems to decrease complaints of OAB and UI. The potential for local oestrogens in the prevention as well as treatment of POP needs further research.
Introduction
Oestrogen is of great importance in the function of the genital and lower urinary tract with oestrogen receptors being present in the bladder, urethra, vagina, and pelvic floor musculature [1].
Oestrogen receptors play a role in the supportive mechanism of the pelvis by controlling the synthesis and breakdown of collagen [2]. Also, the tissues of the female urinary continence mechanism are sensitive to oestrogen. Oestrogens may affect continence by enhancing urethral resistance by increasing the number of periurethral vessels that account for one-third of urethral pressure [3]. Moreover, oestrogens can reduce the frequency and amplitude of detrusor contractions and so raise the sensory threshold of the bladder and promote relaxation of the detrusor muscle [4,5].
For these reasons the decline in available oestrogen after menopause is a possible etiological factor for pelvic floor disorders. Pelvic floor disorders include stress urinary incontinence (SUI), urge urinary incontinence (UUI) and pelvic organ prolapse (POP) and together they are estimated to occur in up to 40% of postmenopausal women [6,7]. Half of all postmenopausal women are thought to suffer from vaginal atrophy (VA), which commonly causes symptoms such as vaginal dryness, irritation or itching, dyspareunia and thin and frail epithelia [8].
In the past, studies have focused on systemic hormone replacement therapies, more recently topical oestrogens have become the focus of interest in the treatment of pelvic floor disorders as this reduces adverse effects. Treatment with topical oestrogens (in the form of tablets, pessaries, creams, and the oestradiol-releasing vaginal ring) have proven to be effective for the symptoms associated with vaginal atrophy. A review of 19 randomized controlled trials (RCTs) including 4162 women concluded that the available topical oestrogens are equally effective in relation to each other for treating VA and associated symptoms [9]. However, additional trials providing long-term data were advised. Moreover, a large trial variation existed, with small sample sizes and diversity in the outcomes measuring efficacy, safety and tolerance of the use of local oestrogen in vaginal atrophy [9].
In the treatment of urinary incontinence different options are available, including pelvic floor muscle training, antimuscarinic medications (for urge urinary incontinence) and surgery (for stress urinary incontinence). Oestrogen has been used to treat incontinence over a number of years, either alone or in combination with some of these other options, and there is evidence that urinary incontinence may improve with local oestrogen treatment [10]. In contrast, systemic hormone replacement therapy seems to worsen urinary incontinence [11]. The possible worsening of urinary incontinence with systemic oestrogen therapy as well as the concerns about adverse effects of systemic treatment (for example regarding breast cancer, effects on endometrium or thromboembolic diseases), makes further evaluation of local oestrogen therapy in the treatment of urinary incontinence of great value. The currently available evidence has to be interpreted with caution because the treatment effects are based on a relatively low number of patients and a wide range of types, dosages and duration of oestrogen treatment [10]. Moreover, also in the studies regarding local oestrogen treatment for urinary tract symptoms, there is a diversity in the outcomes measured (urodynamic or clinical) and populations studied [12].
The available evidence regarding vaginal oestrogen therapy in postmenopausal women with overactive bladder (OAB) symptoms (urinary urgency, frequency, nocturia, with or without urge urinary incontinence) is encouraging [13,14]. However, it is not clear if subjective improvement in OAB symptoms reflects a direct effect on lower urinary tract function or a indirect effect via reversing VA [15].
How oestrogen changes collagen metabolism related to POP is still unclear [16]. One hypothesis is that oestrogen brings the collagen metabolism back to a premenopausal state [17]. Consequently, oestrogen deficiency could weaken the supporting ligaments of the pelvic organs, as well as causing thinning of the vaginal epithelium [18]. These factors could contribute to POP. Oestrogens alone or together with other forms of treatment (i.e. vaginal pessaries, pelvic floor muscle training or surgery), may help in the treatment of POP by increasing synthesis of collagen and improving the strength of the vaginal epithelium. Evidence regarding the effectiveness of topical oestrogens in the treatment of POP is, however, lacking [19].
With this systematic review we provide a complete overview of the current evidence regarding topical oestrogen therapy in the treatment of pelvic floor disorders.
Methods
Eligibility criteria
Studies regarding vaginal atrophy
All randomised controlled trials of vaginally administered oestrogen for the treatment of symptoms of vaginal atrophy (as defined by the trialists) in postmenopausal women with a duration of treatment of at least 12 weeks.
Outcomes regarding vaginal atrophy
Subjective efficacy:
- - Presence of vaginal dryness, vaginal itching/irritation and dyspareunia but also composite scores like:
- - Most bothersome symptom (MBS) approach: The MBS consists of a list of symptoms (most commonly the four symptoms of vaginal dryness, vaginal itching/irritation, dyspareunia and vaginal soreness). At baseline, participants address each of these symptoms as not present, mild, moderate, or severe and then select one symptom previously reported as moderate or severe as the MBS. The MBS is then re-evaluated at the end of treatment, and the change in severity is used to assess subjective improvement [20,21].
- - Urogenital score: includes the subjective assessment of symptoms like urinary frequency and urgency, dyspareunia and vaginal dryness[22].
- - Total score index of vaginal atrophy: reported from 0 to 3 according to the assessment of symptoms by the participant, in combination with the assessment of a physician according to gynaecologic examination (no symptoms: 0–0.50, minor symptoms: 0.51–1.00, moderate symptoms: 1.01–2.00, severe symptoms: 2.01–3.00) [23].
- - Clinician assessment of the vaginal wall appearance including assessment of the presence or absence of petechiae on the vaginal wall, vaginal wall pallor, friability of the vaginal wall (defined as any bleeding occurring during examination), vaginal dryness but also composite scores like:
- - Vaginal physical examination scale: includes assessment of vaginal wall petechiae, vaginal wall friability, rugae and decreased vaginal wall elasticity (conization) [24].
- - Genital Health Clinical Evaluation (GHCE): the GHCE is a tool used to assess six parameters (vaginal fluid secretion, epithelium, colour, moisture, rugosity and pH) scored on a scale 1 to 4. A higher score indicates less atrophy [28].
Objective efficacy: vaginal pH measurement and cytological assessment including vaginal maturation index (VMI), vaginal maturation value (VMV) and karyopyknotic index (KPI or KI). VMI represents the percentage of parabasal, intermediate and superficial squamous cells appearing on a vaginal smear [29]. Cytomorphologically, VA can be defined as a condition with a very low percentage of superficial cells and a high percentage of (para)basal and intermediate cells [30]. In a formula the different cell types can be multiplied by certain factors to obtain the VMV. There is a variety in formulas to calculate the VMV [8]. KPI or KI is described as measuring the relationship of superficial cells to intermediate cells [31] but also as the percentage of superficial cells of the total amount of the squamous cells examined [32,33].
Safety: Adverse events related to treatment
Studies regarding urinary incontinence and overactive bladder symptoms
All randomised controlled trials of local oestrogen therapy for the treatment of overactive bladder symptoms, urinary stress, urge or mixed incontinence in postmenopausal women diagnosed by symptom classification or by urodynamic diagnosis, as defined by the trialists.
Outcomes regarding urinary incontinence and overactive bladder
Subjective efficacy: Patient reported symptoms of urinary incontinence, urgency and/or overactive bladder, improvement or cure of symptoms of urinary incontinence, urgency and/or overactive bladder, and disease specific quality of life questionnaire (Incontinence Impact Questionnaire (IIQ)).
Semi-objective efficacy: Frequency of micturitions and number of incontinent episodes (as indicated from bladder diary), pad tests (weight of urine loss) and pad changes.
Objective efficacy: Urodynamic measures including maximum bladder capacity (ml), maximum urethral closure pressure (MUCP) (cmH20) and volume at first urge to void (ml).
Safety: Adverse events related to treatment.
Studies regarding pelvic organ prolapse
All studies of local oestrogen therapy for the treatment of pelvic organ prolapse in postmenopausal women with any degree of pelvic organ prolapse.
Outcomes regarding pelvic organ prolapse
Subjective efficacy: patient reported symptoms of POP (sense of pressure or bulge vaginally, abdominal or back pain, urinary or bowel symptoms), improvement or cure of symptoms associated with POP, satisfaction with treatment outcome, postponement or no need for other treatments like pelvic floor muscle training, mechanical devices or surgery, disease-specific quality of life questionnaire (Urogenital Distress Inventory (UDI)) and clinicians observed improvement or cure of POP using the POP-Q system [34].
Safety: Adverse events related to treatment.
Interventions
Oestrogenic preparations administered intra-vaginally, including creams, tablets, ovules/pessaries and rings.
Search strategy
Our review followed the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) guidelines for reporting. A medical information specialist (JL) performed a comprehensive search of MEDLINE and EMBASE (via the OVID-interface), CENTRAL, the non-MEDLINE subset of PubMed and prospective trial registers from inception to May the 25th 2014. Both indexterms and text words were used, with no language or other restrictions.
The search consisted of three parts. The basis was an extensive search for local or vaginally applied oestrogens. This search was successively combined with a broad search for 1] vaginal atrophy (VA), 2] urinary incontinence/overactive bladder (UI/OAB) and 3] pelvic organ prolapse (POP). The VA–search, retrieving many randomized controlled trials (RCTs), was combined with a sensitive filter for RCTs (adapted from the Cochrane Collaboration). In addition we checked the availability of systematic reviews (SRs) by applying a methodological filter for secondary studies. No methodological filters were needed for part 2 and 3 (for the OVID MEDLINE search strategy see S1 Appendix).
We cross-checked the reference lists and the citing articles of the identified relevant papers and adapted the search in case of additional relevant studies. The results were entered and de-duplicated in Reference Manager (version 12.0).
Data collection and analysis
Eligible studies were selected from the identified references by applying the inclusion criteria, first on title and abstract, and in a second step on full text.
If studies were sufficiently similar with regard to clinical aspects and study design, a pooled effect (fixed effect model) was calculated using Review Manager (version 5.2) software. In case of substantial heterogeneity a random effects model was used.
Studies that did not report their results in enough detail to allow data extraction (e.g. missing standard deviations, or presentation of the results in graphs) were not included in the appendices with the analyses. The results of these studies are described narratively in the Results section.
The effect measures were risk ratio (RR) for dichotomous data and mean difference (MD) for continuous data, with 95% confidence intervals (CI). Data analysis was performed using Review Manager software following the guidance the Cochrane Reviewers’ Handbook [35]
Assessment of risk of bias
Risk of bias was assessed using the Cochrane Risk of Bias Tool [35]. We assessed the risk of bias of the studies that were published after the date of the search in the Cochrane reviews of Suckling [9], Cody [10] or Ismail [19] or studies that were not included in the Cochrane reviews but were considered relevant for our review. For the studies included in the Cochrane reviews we used the Cochrane author’s assessment of risk of bias. Selection, data extraction and risk of bias assessment were performed by two reviewers independently. Disagreements were resolved by discussion, or if necessary, by a third reviewer.
Results
Topical oestrogens to treat vaginal atrophy
Studies
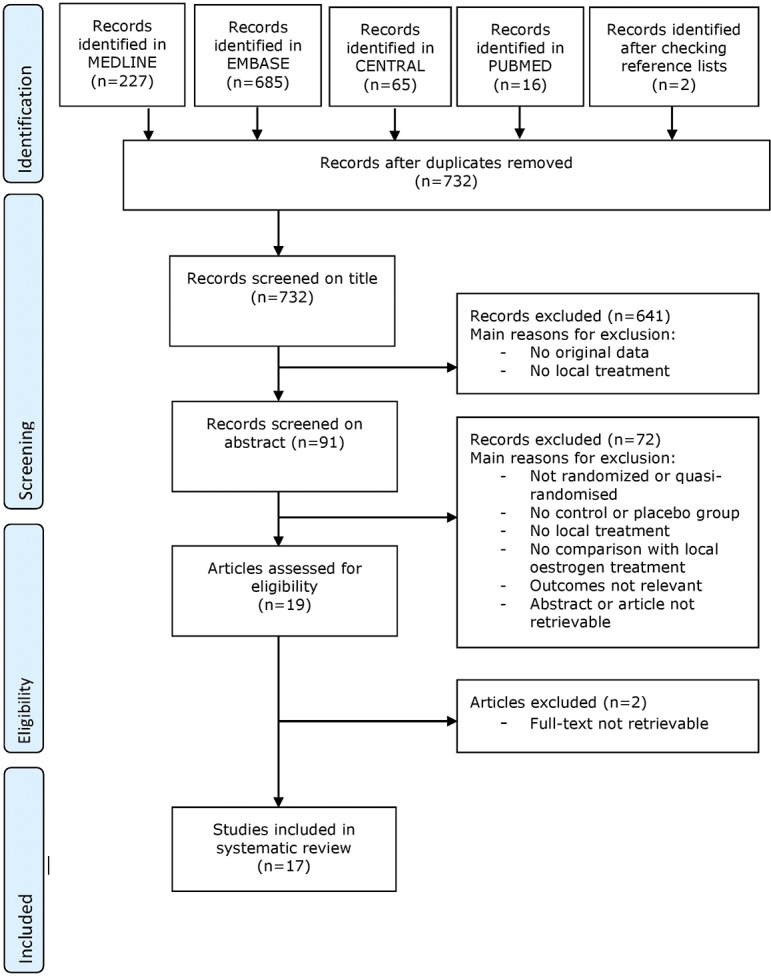
Our literature search considering topical oestrogen treatment for vaginal atrophy retrieved 532 studies. A total of 32 randomized controlled trials (31 articles) were selected for this review, of which 18 were also included in the Cochrane review of Suckling and co-workers [9]. Main reasons for exclusion and the flow of records through the selection process are provided in the flowchart (Fig 1).
Fig 1. Flow chart local oestrogens for vaginal atrophy.

As can be seen in Table 1, there was a wide variety of topical oestrogen administration forms. Local administration of oestrogen was compared to placebo or no treatment or non-hormonal treatment. Other studies compared different application forms, doses or combination treatment. The 32 trials included over 6500 participants. Treatment ranged from 12 weeks up to 12 months, 24 out of the 32 studies were included in the quantitative analysis. Eight studies did not report their data in sufficient detail to allow data extraction [36–43].
Table 1. Comparisons in studies regarding local oestrogen treatment for vaginal atrophy.
| Intervention | Control | Studies |
|---|---|---|
| Vaginal oestrogen versus placebo | ||
| Tablets/pessary 0.01–0.03 mg | Placebo | Bachmann et al. 2008; Eriksen et al. 1992;Jaisamrarn et al. 2013; Griesser et al. 2012; Simon et al. 2008; Simunic et al. 2003 |
| Ovule 1mg | Placebo | Dessole et al. 2004 |
| Cream 0,3–0.625mg | Placebo | Freedman et al. 2009; Raghunandan et al. 2010; Bachmann et al. 2009; Lima et al. 2013 |
| Gel 0.05 mg | Placebo | Cano et al. 2012 |
| Ring 0.0075 mg/24hr | Placebo | Casper et al. 1999 study 2; Speroff et al. 2003 |
| Pessary 0,2 mg | Placebo | Griesser et al. 2012 |
| Depot 3.5mg | Placebo | Foidart et al.1991 |
| Different application methods of vaginal oestrogen | ||
| Ring 0.0065–0.0095 mg/24h | Patch 0.014 mg | Gupta et al. 2008 |
| Tablet 0.025 mg | Weisberg et al. 2005 | |
| Cream 0.5 mg | Barentsen et al. 1997; Ayton et al. 1996; Nachtigall et al. 1995 | |
| Pessary 0.5 mg | Henriksson et al. 1994; Casper et al. 1999 study 1 | |
| Tablet 25 microgram | Cream 1gram / 1,25mg | Manonai et al. 2001; Rioux et al. 2000 |
| Vaginal oestrogen versus non-hormonal treatment | ||
| Cream 0.5–0.625 mg | Replens | Bygdeman et al. 1996; Nachtigall et al. 1994 |
| Different doses of vaginal oestrogen | ||
| Tablet 0.01 mg | Tablet 0.025 mg | Bachmann et al. 2008 |
| Ring 0.10–0.14 mg | Ring 0.05–0.06 mg | Nash et al. 1999; Speroff et al. 2003 |
| Promestriene 1% cream | Estriol 0.1% cream | Bruno et al. 2012 |
| Tablet 25 microgram | Vagitory 0,5mg | Dugal et al. 2000 |
| Vaginal oestrogen versus combination therapy | ||
| Oestrogen cream 0.625 mg and 0.5 mg of 2% testosterone cream | Oestrogen cream 0.625 mg | Raghunandan et al. 2010 |
| Ovule 1 mg and pelvic floor rehabilitation | Ovule 1 mg | Capobianco et al. 2012 |
| Triple therapy: Oestrogen and Lactobacilli Acidophili ovule plus pelvic floor rehabilitation (1 mg oestrogen + 50 mg lyophilisate) | Oestrogen ovule plus pelvic floor rehabilitation (1 mg oestrogen) | Capobianco et al. 2014 |
| Oestrogen cream 0.5 mg and benzidamine | Oestrogen cream 0.5 mg | Melis et al. 1997 |
Risk of bias
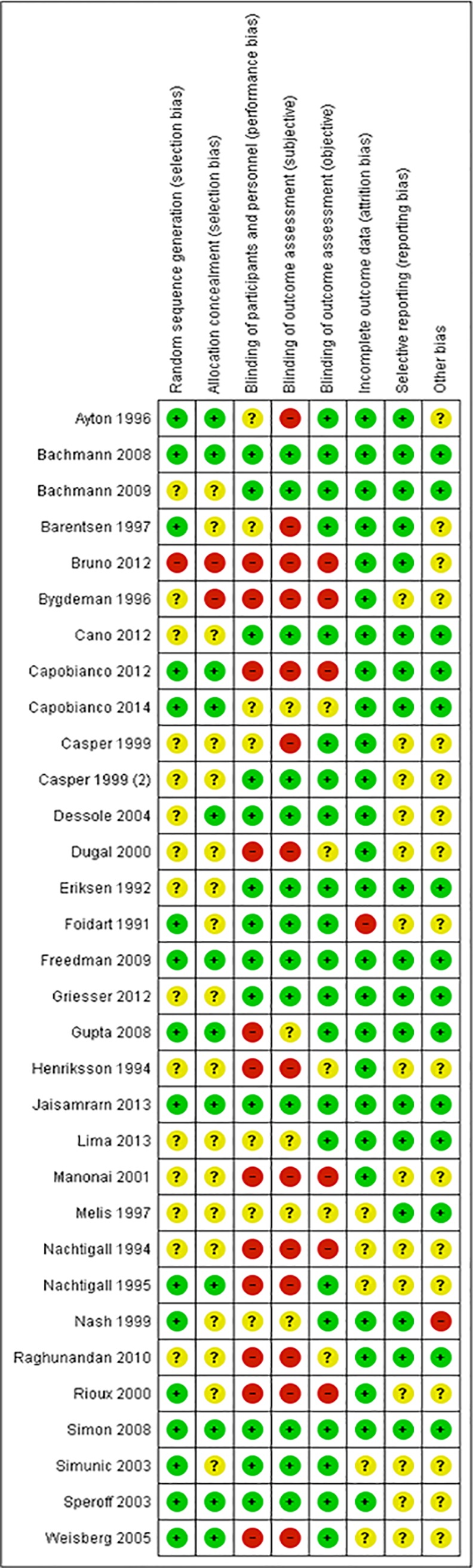
As can be seen in Figs 2 and 3, about half of the trials used an adequate method of randomization (randomization sequence and allocation concealment). Fifteen trials did not report details on the randomization method [22,27,28,33,37,40,44–51]. In studies that compared different forms of applications the women could not be blinded. Blinding of the outcome assessors was often unclear. Dropouts or losses to follow up were reported in most trials included in the review and were acceptable and comparable between groups in most studies. In two studies the percentage of dropouts exceeded 20% [52,53]. The studies published after the Cochrane review all reported all predefined outcomes. In the Cochrane review reporting bias was not assessed [9]. In two studies there was a statistically significant difference in age between the treatment groups [42,54]. The risk of bias tables in the Cochrane review did not provide enough details for an assessment of other types of bias [9].
Fig 2. Risk of bias graph: review authors’ judgements about each risk of bias item presented as percentages across all included studies regarding local oestrogen treatment for vaginal atrophy.

Fig 3. Risk of bias summary: review authors’ judgements about each risk of bias item for each included study regarding local oestrogen treatment for vaginal atrophy.
Comparison 1: Vaginal oestrogen versus placebo
The 15 studies that compared vaginal oestrogen with placebo varied in ways of application, types of oestrogen, doses and treatment durations. Both objective and subjective outcomes were assessed by a variety of measures. Grouping studies by outcome was therefore often not possible, resulting in analyses with three studies at the most.
After 12 to 52 weeks of treatment, women treated with local oestrogen experienced less often symptoms associated with vaginal atrophy or rated symptoms as less severe compared to the placebo treated women (analysis 1–9, S2 Appendix). The women treated with local oestrogen showed less signs of vaginal atrophy at physical examination, had an increase in vaginal maturation and had lower pH values compared to the placebo treated women (analysis 10–21, S2 Appendix). Most studies reported results after 12 weeks of treatment. Results were consistent across studies and type of oestrogen application and the differences were statistically significant. Adverse events occurred at similar rates in both the oestrogen and placebo treated groups; severe adverse events were rarely reported (analysis 22–25, S2 Appendix).
Comparison 2: Different application methods of vaginal oestrogen
Seven studies compared an oestrogen vaginal ring to another method of local oestrogen application (patch, tablet, cream, pessary) [36,37,41,49,53,55,56] and two studies compared an oestrogen vaginal tablet to an oestrogen cream [27,57].
When comparing different application methods of oestrogen no clear differences in symptoms, signs, pH value and adverse events could be demonstrated (analysis 26–41, S2 Appendix). The number of women per comparison was small however, resulting in wide confidence intervals. Treatment duration varied between 12 and 48 weeks; most outcomes were reported for 12 weeks of treatment.
Comparison 3: Vaginal oestrogen versus non-hormonal treatment
The two studies that compared vaginal oestrogen to a non-hormonal treatment both looked at the effect of vaginal oestrogen cream versus a non-hormonal vaginal gel (Replens). In both studies participants were treated for a period of 12 weeks [44,51].
Comparison between oestrogen and non-hormonal treatment (Replens) showed inconsistent results regarding vaginal pH (analysis 42, S2 Appendix) and no differences between groups regarding symptoms (data regarding symptoms could not be extracted for data analysis). Signs seemed to improve more with vaginal oestrogen treatment (analysis 43–46, S2 Appendix). Both studies described no difference in adverse events between the two groups, serious side effects were not reported.
Comparison 4: Different doses of vaginal oestrogen
This comparison group consisted of five trials. Bachmann and co-workers studied treatment with a vaginal oestrogen tablet containing 0.01 mg or 0.025 mg estradiol (E2) [58]. Nash and co-workers investigated the use of a vaginal ring containing E2 0.14 mg/day versus a vaginal E2 ring 0.06 mg/day [42]. Speroff evaluated treatment with a vaginal ring containing 0.05 mg/day or 0.1 mg/day [43]. Bruno assessed promestriene (Colpotrofine) 1% cream versus estriol (Ovestrion) 0.1% cream [54] en Dugal a 0.025 mg 17 β-estradiol vaginal tablet versus 0.5 mg estriol [46].
No obvious differences were reported in the comparison of different doses of vaginal oestrogen regarding symptoms of VA with the exception of two studies showing a significant decrease in vaginal dryness in favor of a higher dose of oestrogen [46,54].
Concerning signs at physical examination Bachmann and co-workers graded vaginal health with the use of a compound score of five parameters assessed over time (secretions, epithelial surface thickness and integrity, vaginal color, and pH). At week 7 the mean score for the 0.025 mg estradiol (E2) group was significantly lower (meaning less vaginal atrophy) than for the 0.01 mg E2 group. No data could be extracted for data analysis [58]. Other studies evaluating signs did not reveal significant differences between treatment groups [42,46].
The studies evaluating vaginal maturation did not show statistically significant differences between groups (analysis 47 and 48, S2 Appendix) [42,43,46,58].
Bachmann and co-workers described the percentage of participants with pH less than 5 after 12 weeks of treatment as 51% and 39% in the 0.025 mg and 0.01 mg E2 groups respectively. However it was unclear if this outcome was statistically significant [58]. The other studies in this comparison group did not evaluate vaginal pH as an outcome measure.
No differences in adverse events were reported and overall adverse events were mild to moderate (analysis 49, S2 Appendix) [43,46,54,58].
Comparison 5: Vaginal oestrogen versus combination therapy including vaginal oestrogen
Raghunandan and co-workers evaluated vaginal oestrogen cream and combined oestrogen and testosterone cream [22]. Capobianco and co-workers investigated in 2012 treatment with a vaginal oestrogen ovule versus a similar ovule in combination with pelvic floor rehabilitation (PFR), together called ‘combination therapy’ [32]. In 2014 they evaluated treatment with a vaginal oestrogen ovule in combination with PFR versus an oestrogen ovule in combination with PFR and Lactobacilli Acidophili (together called ‘triple therapy’) [59]. Melis and co-workers studied oestrogen cream versus oestrogen cream combined with benzidamine (an anti-inflammatory and anti-bacterial compound) [50]. Participants were treated for three to six months. Sample sizes ranged from 50–206 participants.
Combination therapy and triple therapy seemed to have more beneficial effects regarding symptoms and signs of VA, vaginal cytology and pH when compared to oestrogen alone and oestrogen plus PFR respectively (analysis 50–59, S2 Appendix).
The improvement in symptoms, signs and vaginal cytology seemed comparable between treatment with oestrogen cream and oestrogen plus testosterone cream (analysis 60–62, S2 Appendix), but the sample size was small, resulting in wide confidence intervals.
Melis and co-workers did not provide data in enough detail to include in the analysis but reported that combining oestrogen with benzidamine was significantly more effective for treatment of vaginal symptoms compared to oestrogen alone [50]. They did not describe a difference in increase in superficial cells between both groups. In all four studies no significant adverse events were reported.
Topical oestrogens to treat urinary incontinence
Studies
Our literature search resulted in a total of 732 studies. Main reasons for exclusion are provided in the flow chart (Fig 4). Seventeen studies were eligible for this review, of which ten were also included in the Cochrane review of Cody and co-workers [10]. Four studies were also included in the VA search [23,32,33,59].
Fig 4. Flow chart local oestrogens for urinary incontinence and overactive bladder.
As can be seen in Table 2, local administration of oestrogen was compared to placebo or no treatment [23,33,60–65] or non-hormonal treatment [64–69]. The remaining studies compared different application forms, doses or including another treatment [32,59,61,70–72]. The 17 studies included over 3100 participants. Treatment ranged from three weeks up to 12 months. Fourteen of the 17 studies presented their data with sufficient detail to include in the quantitative analysis.
Table 2. Comparisons in studies regarding local oestrogen treatment for urinary incontinence and/or overactive bladder symptoms.
| Intervention | Comparison | Studies |
|---|---|---|
| Vaginal oestrogen versus placebo or no treatment | ||
| Oestrogen 0,025–3 mg | Placebo | Simunic et al. 2003; Cardozo et al. 2001; Dessole et al. 2004; Sacco et al. 1990; Enzelsberger 1991–1; Enzelsberger 1991–2 |
| Triple therapy (local oestrogen (dose unclear), physiotherapy and electrostimulation) | No treatment | Holtedahl et al. 1998 |
| Premarin cream 2 gr/night (1.25 mg oestrogen) | No treatment | Henalla et al. 1989; Henalla et al. 1990 |
| Different application methods of vaginal oestrogen | ||
| Oestrogen Ring 0,5mg | Oestrogen Pessary 0,5mg | Lose et al. 2000 |
| Vaginal oestrogen versus non-hormonal treatment | ||
| Oestrogen cream 0,625mg + tolterodine | Tolterodine | Tseng et al. 2009; Serati et al. 2009 |
| Oestrogen ring 1mg (7,5microgram/24hr) | Oral oxybutynin | Nelken et al. 2011 |
| Oestrogen suppository 1mg | Phenylpropanolamine | Beisland et al. 1984 |
| Premarin cream 2 gr/night (1.25 mg oestrogen) | Pelvic floor exercises | Henalla et al. 1989; Henalla et al. 1990 |
| Premarin cream 2 gr/night (1.25 mg oestrogen) | Electrostimulation | Henalla et al. 1989 |
| Different doses of vaginal oestrogen | ||
| 1mg (application form unclear) | 3mg (application form unclear) | Enzelsberger 1991 |
| 0,5-1mg (application form unclear) | 2mg (application form unclear) | Enzelsberger 1990 |
| Vaginal oestrogen versus oral oestrogen | ||
| Oestrogen cream 0,625mg | Oral oestrogen 0,625mg | Long et al. 2006 |
| Vaginal oestrogen vs combination therapy | ||
| Oestrogen ovule 1mg + PFR | Oestrogen Ovule 1mg | Capobianco et al. 2012 |
| Triple therapy: Oestrogen and Lactobacilli Acidophili ovule plus pelvic floor rehabilitation (1mg oestrogen + 50 mg lyophilisate) | Oestrogen ovule plus pelvic floor rehabilitation (1mg oestrogen) | Capobianco et al. 2014 |
Risk of Bias
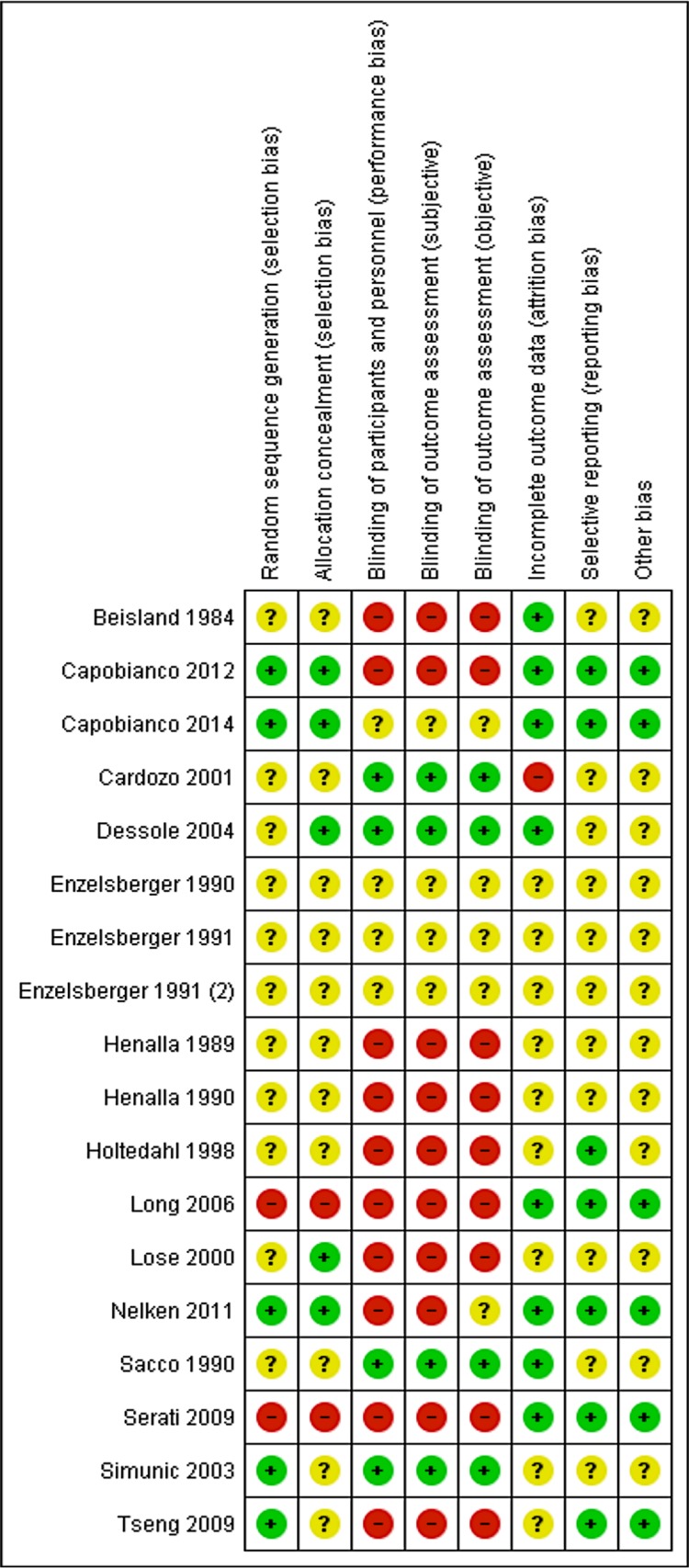
As can be seen in Figs 5 and 6, five studies used an adequate method of randomization [23,32,59,67,69]. Two studies had high risk of selection bias [68,72] and in ten studies it was unclear whether an adequate random sequence generation method was used [33,60–66,70,71]. Almost half of the studies were not blinded, and in four studies blinding was unclear. Four studies were double blinded [23,33,60,62]. Dropouts or losses to follow up were reported in most of the trials, with acceptable dropout rates. Studies included after the search date of the Cochrane review were at low risk of reporting bias. In one study we found baseline differences [63]. The risk of bias assessment of the studies included in the Cochrane review did not include reporting bias or details on other biases [10].
Fig 5. Risk of bias graph: review authors’ judgements about each risk of bias item presented as percentages across all included studies regarding local oestrogen treatment for urinary incontinence and/or overactive bladder.

Fig 6. Risk of bias summary: review authors’ judgements about each risk of bias item for each included study regarding local oestrogen treatment for urinary incontinence and/or overactive bladder.
Comparison 1: Vaginal oestrogen versus placebo or no treatment
This group consisted of eight studies of which five studies used a placebo controlled design [23,33,60–62], two studies compared vaginal oestrogen to no treatment [64,65] and one study compared vaginal oestrogen (in a combination therapy with physiotherapy and electrostimulation) with a no treatment group [63].
Two studies applied vaginal oestrogen with the use of ovules [33,63], two studies used oestrogen vaginal tablets [23,60] and three studies prescribed an oestrogen vaginal cream [62,64,65]. In one study the method of application was unclear [61].
Overall, subjective, semi-objective and urodynamic outcomes changed in favor of the vaginal oestrogen groups compared to placebo (analysis 1–4, S3 Appendix).
Treatment side effects were equally distributed in the vaginal oestrogen and placebo group in the study of Simunic and co-workers. No severe adverse events were reported [23]. Three other studies reported no significant differences in adverse events between groups [33,60,61].
Comparison 2: Different application methods of vaginal oestrogen
One study compared a vaginal oestrogen ring with a vaginal oestrogen pessary in a group of 251 postmenopausal women for a treatment period of 24 weeks [70].
Response to treatment with respect to stress and urge incontinence, urgency, frequency, dysuria and nocturia was comparable between groups. The overall subjective judgment (acceptability) of the type of administration was in favor of the vaginal ring (analysis 5, S3 Appendix), this was not based on an experience with both application methods. The percentage of women reporting side effects in the pessary group was slightly higher compared to the women in the ring group (35.9% versus 25.4%), but the difference was not statistically different (analysis 6, S3 Appendix).
Comparison 3: Vaginal oestrogen versus non-hormonal treatment or combination treatment
Two studies compared vaginal oestrogen cream combined with tolterodine (a competitive cholinergic receptor antagonist) with tolterodine alone [68,69]. One study evaluated the differences between treatment with an oestrogen vaginal ring and oral treatment with oxybutynin (an anticholinergic drug used for relaxation of the detrusor muscle) [67]. Another study compared a vaginal oestrogen suppository to phenylpropanolamine (PPA; a nonselective adrenergic receptor agonist and norepinephrine reuptake inhibitor) [66]. Two studies assessed Premarin vaginal cream versus PFR [64,65] and one of these studies also evaluated Premarin vaginal cream versus pelvic floor electrostimulation (interferential therapy) [65].
Treatment effects with vaginal oestrogen only or non-hormonal treatment (combined or not combined with vaginal oestrogen) were largely similar regarding subjective efficacy (analysis 7–11, S3 Appendix).
Bladder diary variables improved slightly more in the tolterodine plus oestrogen group as compared to the tolterodine alone group in a small study of 40 participants in each group (analysis 12 and 13, S3 Appendix); the differences were however, not statistically significant for most outcomes [69]. In another study, users of an estradiol vaginal ring and users of oral oxybutinine both reported a lower frequency of daily voids after 12 weeks treatment, but these decreases were not statistically significant (analysis 14, S3 Appendix) [67]. In two small studies the percentage of women with stress urinary incontinence that were cured or improved was lower in the oestrogen group compared to the groups with pelvic floor exercises or electrostimulation, For the comparison with exercise this difference was statistically significant (analysis 15 and 16, S3 Appendix) [64,65].
Increase in MUCP seemed greatest in patients treated with oestrogens compared to pelvic floor exercises or electrostimulation [65]. No statistically significant difference in urodynamic variables were reported between PPA and estriol when administered separately [66] (data could not be extracted for analysis).
Vaginal discharge occurred more often in the ring groups while complaints of dry mouth and constipation occurred more in the oxybutynin group (analysis 17, S3 Appendix) [67]. Tseng and co-workers described no significant adverse events in both treatment groups (tolterodine/oestrogen vs tolterodine alone, 80 women in total) [69]. Beisland and co-workers (n = 20) reported one patient with genital bleeding during combined treatment (PPA/oestrogen) and one patient with insomnia after three days of PPA treatment [66].
Comparison 4: Different doses of vaginal oestrogen
Two studies, both performed by Enzelsberger and co-workers, assessed the differences in symptoms of urge urinary incontinence between treatment with different doses of vaginal oestrogen [61,71]. Both studies were unclear about the method of application, only mentioning the different doses in both treatment groups. In the first study, 0.5–1 mg vaginal oestrogen was compared to 2 mg vaginal oestrogen [71]. The other study compared 1 mg vaginal oestrogen to 3 mg vaginal oestrogen (and placebo, see analysis 2 and 3, S3 Appendix) [61].
Regarding bladder diary variables data from the 0.5–1 mg group in the study of Enzelsberger and co-workers in 1990 seemed to be the same as the data from the 1 mg group in their study in 1991 (analysis 18 and 19, S3 Appendix). In the first study, nocturia as well as micturition frequency decreased significantly more compared to baseline in the high dose group compared to the low dose group [71]. In the second study, nocturia occurred significantly less frequent after treatment in the high dose group (3 mg). The difference in urinary frequency between the two groups was not significant [61].
No significant differences regarding urodynamic variables between high dose and low dose treatment groups in both studies were found except for the difference in bladder capacity; the results suggest that the capacity increased with increasing dose. However confidence intervals were large (analysis 20 and 21, S3 Appendix).
Comparison 5: Vaginal oestrogen versus oral oestrogen
One study investigating vaginal versus oral oestrogen therapy was included. This study compared treatment with oestrogen vaginal cream to oral oestrogen in the same dose in 57 postmenopausal women [72].
Oral oestrogen seemed to be more effective in decreasing urinary frequency compared to vaginal cream whereas vaginal cream was more effective in decreasing nocturia. Changes of other symptoms, including stress and urge urinary incontinence, were not statistically significantly different between the two groups (analysis 22, S3 Appendix). Among improved patients there was no statistically significant difference in the mean number of stress urinary incontinence episodes per week (analysis 23, S3 Appendix). Adverse events were not reported.
Comparison 6: Vaginal oestrogen versus combination therapy including vaginal oestrogen
Two studies provided evidence for the effectiveness of combination therapy. Compared to oestrogen therapy alone, combining PFR with oestrogen resulted in higher mean values for all urodynamic outcomes (statistically significant except for bladder capacity) [32]. In the second study, Lactobacilli acidophilli was added to treatment with PFR and oestrogen. Compared to oestrogen therapy plus PFR, the mean values of all urodynamic outcomes were higher in the triple therapy group with statistically significant differences for MUP, MUCP and the pressure transmission ratio (PTR) [59] (analysis 24–27, S3 Appendix).
In both studies no systemic adverse reactions were observed.
Topical oestrogens to treat pelvic organ prolapse
Studies
Our literature search on local oestrogen therapy for pelvic organ prolapse resulted in a total of 305 studies (Fig 7). Main reasons for exclusion were the absence of original data of local treatment, irrelevance of outcomes or irretrievable abstracts. This left us with three studies, of which one was available in full text [73]. For the other two studies we used the abstracts to extract information from [74,75]. One study was also included in the Cochrane review of Ismail and co-workers, published in 2010 [19,73].
Fig 7. Flowchart local oestrogens for pelvic organ prolapse.

As can be seen in Table 3, two out of the three studies investigated local administration of oestrogen versus placebo or no treatment [73,75]. One study compared local oestrogen therapy in combination with oral duloxetine (a selective serotonin and norepinephrine reuptake inhibitor) and Kegel exercises to surgical treatment (anterior colporrhaphy) [74]. In the studies 16 to 48 women were enrolled. The duration of treatment ranged from two weeks up to three months. None of the studies reported data that could be included in the quantitative analysis.
Table 3. Comparisons in studies regarding local oestrogen treatment for pelvic organ prolapse.
| Intervention | Comparison | Studies |
|---|---|---|
| Vaginal oestrogen versus placebo or no treatment | ||
| Oestrogen Pessary 25 microgram | Placebo | Felding et al. 1992 |
| Oestrogen Cream 1 gram (dose of oestrogen unclear) | No treatment | Vaccaro et al. 2011 |
| Vaginal oestrogen versus surgical treatment | ||
| Vaginal oestrogen 25 microgram (+ duloxetine p.o. + Kegel exercises) | Anterior colporrhaphy | Nikas et al. 2012 |
Risk of bias
As can be seen in Figs 8 and 9, all three studies were unclear about the randomization method. One study had a double blind design [73]; the other studies were not blinded. Two studies reported acceptable rates of dropout or no dropouts. One study enrolled 40 women of which 70% had completed treatment at the time of publication of the abstract [75]. From all three studies it was not clear if all predefined outcomes were reported. In two studies there were no differences in baseline characteristics between the different treatment groups [73,75]. In one study insufficient information was provided [74].
Fig 8. Risk of bias graph: review authors’ judgements about each risk of bias item presented as percentages across all included studies regarding local oestrogen treatment for pelvic organ prolapse.

Fig 9. Risk of bias summary: review authors’ judgements about each risk of bias item for each included study regarding local oestrogen treatment for pelvic organ prolapse.

Comparison 1: Vaginal oestrogen versus placebo or no treatment
One study compared treatment with a vaginal oestrogen pessary to placebo [73]. The other study compared vaginal oestrogen cream to no treatment [75].
Vaccaro and co-workers described a statistically significant difference in vaginal symptoms (dryness, soreness, and irritation) on a visual analogue scale (VAS) between the treatment group and no treatment group in favor of the treatment group [75]. Felding and co-workers did not describe (differences in) decrease of relevant symptoms [73].
Felding and co-workers reported that thickness of the vaginal wall (assessed histologically with the use of a vaginal wall punch biopsy) was statistically significantly more increased in the treatment group compared to the placebo group [73]. Vaccaro and co-workers described a statistically significant difference in Vaginal Health Composite Score (VHCS; evaluates the amount of epithelial rugosity/integrity, vaginal color, pH and secretions) between the treatment group and no treatment group in favor of the treatment group [75]. No adverse events were reported.
Comparison 2: Vaginal oestrogen versus surgical treatment
One study evaluated the efficacy of treatment with 25 microgram estradiol vaginally plus 40 mg of Duloxetine orally and Kegel exercises versus anterior colporrhaphy in 16 women with stage I cystocele [74].
All women reported less vaginal dryness, no information was provided regarding POP symptoms. No case of progress of the cystocele was reported during oestrogen treatment. Post-operative examination in the group that underwent anterior colporrhaphy revealed successful treatment of the cystocele.
Discussion
This is a review providing a systematic, extensive overview of the effects of local oestrogen treatment on pelvic floor disorders including vaginal atrophy, urinary incontinence, overactive bladder symptoms as well as pelvic organ prolapse. We intended to perform a meta-analysis of the available data. However, due to wide variation in outcome assessment of different pelvic floor symptoms, the variation in type and dosage of the investigated oestrogen treatment regimens and the variety in comparisons made, it was not feasible to perform a proper meta-analysis. As a result this systematic review mainly summarizes and discusses the outcome and interpretation of individual studies. We investigated the risk of bias of the included studies to ensure the integrity of conclusions drawn regarding subjective and objective efficacy and safety. Before further interpreting these conclusions potential limitations need to be addressed.
Although we systematically and thoroughly reviewed the available literature, results need to be interpreted cautiously due to small sample sizes in most studies, variation in trial design, wide variation in outcomes assessing efficacy and safety and a variation in type and dosage of oestrogen used. Moreover, because of the many different definitions of VA, combining study results was often not possible. These limitations in the data analysis resulted in imprecise effect estimates [8]. Additionally, data for each of the pre-defined outcome measures of this review were not available in all trials and the analysis of the outcome measures could only be based on the studies where data extraction was possible, which raised the probability of selective reporting. However, we compared the conclusions of the studies for which data extraction was not possible with the studies included in the analysis, and these were in line. The risk of bias of the included studies was generally moderate, mainly caused by inadequate blinding of participants and personnel (performance bias).
We did not evaluate serum absorption or endometrium stimulation of the different topical oestrogens in the assessment of safety. Low dose vaginal oestrogens have been used for many years in the treatment of women with pelvic floor disorders and recently published guidelines have shown them to be safe [76]. For this review we were more interested in differences in local adverse events between the treatments examined which could cause discontinuation of treatment (i.e. vaginal discharge, irritation).
Tolerability of the different application methods of topical oestrogen was not examined. Suckling and co-workers previously stressed the difficulty of comparing participant acceptability between the ring, cream and tablets due to the differences in frequency of administration. They did suggest a better tolerability of the vaginal ring over other topical vaginal oestrogen preparations due to its delivery system and ease of use. However, in the studies that led to this conclusion, women with pelvic organ prolapse were often excluded from participation. The ring may not be suitable to those with limited vaginal space or pelvic organ prolapse [77]. For that reason it cannot be concluded which application method is accepted best by the patient.
We did not specifically differentiate between different types of oestrogen (i.e. estradiol, estriol, promestriene, synthethic conjugated estrogens) in the description of our results. This subdivision has been previously made by Rees and co-workers in the EMAS clinical guide published in 2012 [76]. With this review we aimed to assess if oestrogens in general are effective in different pelvic floor disorders.
Summary of findings regarding local oestrogen treatment for vaginal atrophy
Studies comparing vaginal oestrogen treatment to placebo were consistent in reporting more beneficial effects on symptoms and signs of VA, vaginal maturation and vaginal pH after oestrogen treatment. Regarding most subjective and objective outcome measures no obvious differences between the different application methods were found. Comparison between oestrogen and non-hormonal treatment (Replens) showed no differences in outcome as far as symptoms and vaginal pH. Signs at physical examination seemed to improve more with vaginal oestrogen treatment [44,51]. No obvious differences were identified in the comparison of different doses of vaginal oestrogen with the exception of two studies showing a significant decrease in vaginal dryness in favor of a higher dose of oestrogen [46,54]. Combination therapy (vaginal oestrogen ovule combined with PFR and/or Lactobacilli Acidophili) seemed to have more beneficial effects regarding symptoms and signs of VA, vaginal cytology and pH as compared to only oestrogens [32,59].
Summary of findings regarding local oestrogen treatment for urinary incontinence and overactive bladder
Overall, subjective, semi-objective and urodynamic variables changed in favor of the vaginal oestrogen groups compared to placebo. No obvious differences in efficacy outcome measures between different application methods were revealed. Treatment with vaginal oestrogen only or non-hormonal treatment (combined or not combined with vaginal oestrogen) was similar regarding subjective efficacy. In two small studies there was a significant reduction in pad weights in the group that received pelvic floor exercises compared to oestrogen treatment [64,65]. Increase in MUCP seemed greatest in patients treated with oestrogens compared to pelvic floor exercises or electrostimulation [65]. Bladder diary variables improved in favor of the tolterodine plus oestrogen group compared to the tolterodine only group in a small study of 40 participants in each group [69]. Nocturia seemed to decrease more after treatment in a high dose (2 mg or 3 mg) group compared to a low dose group (0.5–1 mg) [61,71]. Oral oestrogen seemed to be more effective in decreasing urinary frequency compared to vaginal cream whereas vaginal cream was more effective in decreasing nocturia [72]. Combination therapy (vaginal oestrogen ovule combined with PFR) and triple therapy (oestrogen ovule in combination with PFR and Lactobacilli Acidophili) caused significantly more improvement in symptoms of stress urinary incontinence [32,59].
Summary of findings regarding local oestrogen treatment for pelvic organ prolapse
The studies evaluating the effect of local oestrogen treatment versus placebo or no treatment in women with POP mainly assessed symptoms and signs associated with VA instead of POP symptoms (i.e. sense of pressure or bulge vaginally) [73,75]. This was the same in the study comparing conservative treatment with 25 microgram estradiol vaginally plus 40 mg of Duloxetine orally and Kegel exercises versus anterior colporrhaphy [74]. With these findings and the lack of studies investigating the effect of vaginal oestrogen treatment on POP symptoms, the potential for local oestrogens in the prevention as well as treatment of POP needs to be further established.
Implications for research
Our findings are consistent with the Cochrane reviews regarding local oestrogen treatment for vaginal atrophy published in 2006 [9], for urinary incontinence published in 2012 [10] and for POP published in 2010 [19].
Suckling and co-workers recommended in 2006 that intra-vaginal oestrogenic preparations versus placebo should be researched more. Since their review, an additional 10 placebo-controlled studies have been published and these were included in our review. They also recommended that additional trials providing long-term data (over six months) about efficacy and safety were required. Unfortunately, such long-term studies are still lacking.
With respect to OAB symptoms it was already described by Robinson and co-workers that there is some evidence that vaginal oestrogen could be useful in the management of OAB symptoms [15]. We included two studies evaluating the effect of local oestrogen treatment on overactive bladder symptoms that were excluded in the Cochrane review of 2012 because not all participants had urinary incontinence at baseline. Long and co-workers described that local oestrogen could relieve OAB symptoms while Serati and co-workers described no synergistic effect of local oestrogen when administered together with antimuscarinic medication [68,72]. Bladder diary variables improved slightly more when tolterodine was combined with topical oestrogen compared to tolterodine only in a small study of 40 participants [69].
Regarding local oestrogen treatment for pelvic organ prolapse further research should focus on the effect of oestrogen treatment on POP symptoms and signs. There is a need for well-organized randomized controlled trials with adequate sample size comparing topical oestrogen treatment to placebo evaluating at least symptoms of sense of pressure or bulge vaginally, self-reported improvement or cure of symptoms, quality of life related to pelvic floor symptoms, delay or no need for alternative treatments and clinicians observations of improvement of POP using the POP-Q system.
Implications for practice
Vaginal oestrogen treatment in the form of creams, pessaries, tablets and rings have proven to be effective and safe in the treatment of VA related symptoms at dosages of 10 mcg and more [52,58]. The differences in efficacy between different application methods are very limited. In clinical practice patient preference should guide the selection of the application method. In case pelvic organ prolapse is present, or the vagina is short, a vaginal ring is probably not the best option.
There is evidence implicating a beneficial effect of vaginal oestrogen treatment on urinary incontinence and overactive bladder symptoms, potentially combined with other treatment modalities like PFR or antimuscarinic medication. Again, the way oestrogens are administered plays a minor role. There is too little evidence to recommend on a preferred dose to realize the best outcome.
Regarding vaginal oestrogen treatment for POP the available literature is insufficient to provide evidence based recommendations for clinical practice. One can imagine that relieving VA-related symptoms in patients with POP could relief the sense of vaginal bulge associated with POP, however there are so far no robust data to support this.
Conclusion
Pelvic floor symptoms are complex and multi-factorial. The decline in available oestrogen after menopause is a risk factor for development of worsening of pelvic floor symptoms. Topical oestrogen administration has proven to be effective for the treatment of vaginal atrophy and seems to decrease symptoms of overactive bladder and urinary incontinence. Literature suggests benefit for women with POP although more evidence is needed. Physicians treating women with pelvic floor symptoms should be aware of the capacity of topical oestrogen treatment and include it in their counseling when discussing treatment options.
Supporting Information
(DOC)
(DOC)
(DOC)
(DOC)
Data Availability
All relevant data are within the paper and its Supporting Information files.
Funding Statement
The authors have no support or funding to report.
References
- 1. Iosif CS, Batra S, Ek A, Astedt B (1981) Estrogen receptors in the human female lower uninary tract. AmJObstetGynecol 141: 817–820. [DOI] [PubMed] [Google Scholar]
- 2. Chung dJ, Bai SW (2006) Roles of sex steroid receptors and cell cycle regulation in pathogenesis of pelvic organ prolapse. CurrOpinObstetGynecol 18: 551–554. [DOI] [PubMed] [Google Scholar]
- 3. Rud T, Andersson KE, Asmussen M, Hunting A, Ulmsten U (1980) Factors maintaining the intraurethral pressure in women. Invest Urol 17: 343–347. [PubMed] [Google Scholar]
- 4. Matsubara S, Okada H, Shirakawa T, Gotoh A, Kuno T, et al. (2002) Estrogen levels influence beta-3-adrenoceptor-mediated relaxation of the female rat detrusor muscle. Urology 59: 621–625. [DOI] [PubMed] [Google Scholar]
- 5. Shenfeld OZ, McCammon KA, Blackmore PF, Ratz PH (1999) Rapid effects of estrogen and progesterone on tone and spontaneous rhythmic contractions of the rabbit bladder. Urol Res 27: 386–392. [DOI] [PubMed] [Google Scholar]
- 6. Kenton K, Mueller ER (2006) The global burden of female pelvic floor disorders. BJUInt 98 Suppl 1: 1–5. [DOI] [PubMed] [Google Scholar]
- 7. Nygaard I, Barber MD, Burgio KL, Kenton K, Meikle S, et al. (2008) Prevalence of symptomatic pelvic floor disorders in US women. JAMA 300: 1311–1316. 10.1001/jama.300.11.1311 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Weber MA, Limpens J, Roovers JP (2014) Assessment of vaginal atrophy: a review. IntUrogynecolJ. [DOI] [PubMed] [Google Scholar]
- 9. Suckling J, Lethaby A, Kennedy R (2006) Local oestrogen for vaginal atrophy in postmenopausal women. [Review] [57 refs][Update of Cochrane Database Syst Rev. 2003;(4):CD001500; ]. Cochrane Database SystRev: CD001500. [DOI] [PubMed] [Google Scholar]
- 10. Cody JD, Jacobs ML, Richardson K, Moehrer B, Hextall A (2012) Oestrogen therapy for urinary incontinence in post-menopausal women. CochraneDatabaseSystRev 10: CD001405. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Hendrix SL, Cochrane BB, Nygaard IE, Handa VL, Barnabei VM, et al. (2005) Effects of estrogen with and without progestin on urinary incontinence. JAMA 293: 935–948. [DOI] [PubMed] [Google Scholar]
- 12. Ewies AA, Alfhaily F (2010) Topical vaginal estrogen therapy in managing postmenopausal urinary symptoms: a reality or a gimmick? Climacteric 13: 405–418. 10.3109/13697137.2010.500748 [DOI] [PubMed] [Google Scholar]
- 13. Cardozo L, Lose G, McClish D, Versi E (2004) A systematic review of the effects of estrogens for symptoms suggestive of overactive bladder. Acta ObstetGynecolScand 83: 892–897. [DOI] [PubMed] [Google Scholar]
- 14.Benness CJ, Wise BG, Cutner A, Cardozo LD (1992) Does low dose vaginal estradiol improve frequency and urgency in postmenopausal women? (Abstract). Proceedings of the American Urogynecology Society, 13thannual meeting, Sept2730, 1992, Cambridge, Massachussetts 3: 281.
- 15. Robinson D, Cardozo L, Milsom I, Pons ME, Kirby M, et al. (2013) Oestrogens and overactive bladder. NeurourolUrodyn. [DOI] [PubMed] [Google Scholar]
- 16. Kerkhof MH, Hendriks L, Brolmann HA (2009) Changes in connective tissue in patients with pelvic organ prolapse—a review of the current literature. Int Urogynecol J Pelvic Floor Dysfunct 20: 461–474. 10.1007/s00192-008-0737-1 [DOI] [PubMed] [Google Scholar]
- 17. Moalli PA, Shand SH, Zyczynski HM, Gordy SC, Meyn LA (2005) Remodeling of vaginal connective tissue in patients with prolapse. Obstet Gynecol 106: 953–963. [DOI] [PubMed] [Google Scholar]
- 18. Reay Jones NH, Healy JC, King LJ, Saini S, Shousha S, et al. (2003) Pelvic connective tissue resilience decreases with vaginal delivery, menopause and uterine prolapse. BrJSurg 90: 466–472. [DOI] [PubMed] [Google Scholar]
- 19. Ismail SI, Bain C, Hagen S (2010) Oestrogens for treatment or prevention of pelvic organ prolapse in postmenopausal women. CochraneDatabaseSystRev: CD007063. [DOI] [PubMed] [Google Scholar]
- 20.US Department of Health and Human Services.Food and Drug Administration. (2003) Center for Drug Evaluation and Research (CDER). Guidance for Industry. Estrogen and estrogen/progestin drug products to treat vasomotor symptoms and vulvar and vaginal atrophy symptoms—recommendations for clinical evaluation.
- 21.US Department of Health an Human Services. (2006) Food and Drug Administration. Center for Drug Evaluation and Research (CDER). Guidance for Industry. Patient-reported outcome measures: use in medical product development to support labeling claims.
- 22. Raghunandan C, Agrawal S, Dubey P, Choudhury M, Jain A (2010) A comparative study of the effects of local estrogen with or without local testosterone on vulvovaginal and sexual dysfunction in postmenopausal women. J Sex Med 7: 1284–1290. 10.1111/j.1743-6109.2009.01667.x [DOI] [PubMed] [Google Scholar]
- 23. Simunic V, Banovic I, Ciglar S, Jeren L, Pavicic BD, et al. (2003) Local estrogen treatment in patients with urogenital symptoms. Int J Gynaecol Obstet 82: 187–197. [DOI] [PubMed] [Google Scholar]
- 24. Greendale GA, Zibecchi L, Petersen L, Ouslander JG, Kahn B, et al. (1999) Development and validation of a physical examination scale to assess vaginal atrophy and inflammation. Climacteric 2: 197–204. [DOI] [PubMed] [Google Scholar]
- 25.Bachmann G (1994) Vulvo-vaginal complaints: Lobo R, editor.
- 26. Castelo-Branco C, Cancelo MJ, Villero J, Nohales F, Julia MD (2005) Management of post-menopausal vaginal atrophy and atrophic vaginitis. [Review] [32 refs]. Maturitas 52 Suppl 1: S46–S52. [DOI] [PubMed] [Google Scholar]
- 27. Manonai J, Theppisai U, Suthutvoravut S, Udomsubpayakul U, Chittacharoen A (2001) The effect of estradiol vaginal tablet and conjugated estrogen cream on urogenital symptoms in postmenopausal women: a comparative study. J Obstet Gynaecol Res 27: 255–260. [DOI] [PubMed] [Google Scholar]
- 28. Bachmann G, Bouchard C, Hoppe D, Ranganath R, Altomare C, et al. (2009) Efficacy and safety of low-dose regimens of conjugated estrogens cream administered vaginally. Menopause 16: 719–727. 10.1097/gme.0b013e3181a48c4e [DOI] [PubMed] [Google Scholar]
- 29. McEndree B (1955) Clinical application of the vaginal maturation index. [Review] [31 refs]. Nurse Pract 24: 48–42. [PubMed] [Google Scholar]
- 30. van der Laak JA, Schijf CP, Kerstens HM, Heijnen-Wijnen TH, de Wilde PC, et al. (1999) Development and validation of a computerized cytomorphometric method to assess the maturation of vaginal epithelial cells. Cytometry 35: 196–202. [PubMed] [Google Scholar]
- 31. Schaffer J, Fantl JA (1996) Urogenital effects of the menopause. [Review] [69 refs]. Baillieres ClinObstetGynaecol 10: 401–417. [DOI] [PubMed] [Google Scholar]
- 32. Capobianco G, Donolo E, Borghero G, Dessole F, Cherchi PL, et al. (2012) Effects of intravaginal estriol and pelvic floor rehabilitation on urogenital aging in postmenopausal women. Arch Gynecol Obstet 285: 397–403. 10.1007/s00404-011-1955-1 [DOI] [PubMed] [Google Scholar]
- 33. Dessole S, Rubattu G, Ambrosini G, Gallo O, Capobianco G, et al. (2004) Efficacy of low-dose intravaginal estriol on urogenital aging in postmenopausal women. Menopause 11: 49–56. [DOI] [PubMed] [Google Scholar]
- 34. Bump RC, Mattiasson A, Bo K, Brubaker LP, DeLancey JO, et al. (1996) The standardization of terminology of female pelvic organ prolapse and pelvic floor dysfunction. AmJObstetGynecol 175: 10–17. [DOI] [PubMed] [Google Scholar]
- 35.Higgins JPT, Green S, editors (2011) Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane collaboration. Available from www.cochrane-handbook.org.
- 36. Ayton RA, Darling GM, Murkies AL, Farrell EA, Weisberg E, et al. (1996) A comparative study of safety and efficacy of continuous low dose oestradiol released from a vaginal ring compared with conjugated equine oestrogen vaginal cream in the treatment of postmenopausal urogenital atrophy. BrJ Obstet Gynaecol 103: 351–358. [DOI] [PubMed] [Google Scholar]
- 37. Casper F, Petri E (1999) Local treatment of urogenital atrophy with an estradiol-releasing vaginal ring: a comparative and a placebo-controlled multicenter study. Vaginal Ring Study Group. Int UrogynecolJ Pelvic Floor Dysfunct 10: 171–176. [DOI] [PubMed] [Google Scholar]
- 38. Foidart JM, Vervliet J, Buytaert P (1991) Efficacy of sustained-release vaginal oestriol in alleviating urogenital and systemic climacteric complaints. Maturitas 13: 99–107. [DOI] [PubMed] [Google Scholar]
- 39. Jaisamrarn U, Triratanachat S, Chaikittisilpa S, Grob P, Prasauskas V, et al. (2013) Ultra-low-dose estriol and lactobacilli in the local treatment of postmenopausal vaginal atrophy. Climacteric 16: 347–355. 10.3109/13697137.2013.769097 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Lima SM, Yamada SS, Reis BF, Postigo S, Galvao da Silva MA, et al. (2013) Effective treatment of vaginal atrophy with isoflavone vaginal gel. Maturitas. [DOI] [PubMed] [Google Scholar]
- 41. Nachtigall LE (1995) Clinical trial of the estradiol vaginal ring in the U.S. Maturitas 22 Suppl: S43–S47. [DOI] [PubMed] [Google Scholar]
- 42. Nash HA, Alvarez-Sanchez F, Mishell DR Jr, Fraser IS, Maruo T, et al. (1999) Estradiol-delivering vaginal rings for hormone replacement therapy. Am J Obstet Gynecol 181: 1400–1406. [DOI] [PubMed] [Google Scholar]
- 43. Speroff L (2003) Efficacy and tolerability of a novel estradiol vaginal ring for relief of menopausal symptoms. Obstet Gynecol 102: 823–834. [DOI] [PubMed] [Google Scholar]
- 44. Bygdeman M, Swahn ML (1996) Replens versus dienoestrol cream in the symptomatic treatment of vaginal atrophy in postmenopausal women. Maturitas 23: 259–263. [DOI] [PubMed] [Google Scholar]
- 45. Cano A, Estevez J, Usandizaga R, Gallo JL, Guinot M, et al. (2012) The therapeutic effect of a new ultra low concentration estriol gel formulation (0.005% estriol vaginal gel) on symptoms and signs of postmenopausal vaginal atrophy: results from a pivotal phase III study. Menopause 19: 1130–1139. [DOI] [PubMed] [Google Scholar]
- 46. Dugal R, Hesla K, Sordal T, Aase KH, Lilleeidet O, et al. (2000) Comparison of usefulness of estradiol vaginal tablets and estriol vagitories for treatment of vaginal atrophy. Acta Obstet Gynecol Scand 79: 293–297. [PubMed] [Google Scholar]
- 47. Eriksen PS, Rasmussen H (1992) Low-dose 17 beta-estradiol vaginal tablets in the treatment of atrophic vaginitis: a double-blind placebo controlled study. EurJ Obstet Gynecol ReprodBiol 44: 137–144. [DOI] [PubMed] [Google Scholar]
- 48. Griesser H, Skonietzki S, Fischer T, Fielder K, Suesskind M (2012) Low dose estriol pessaries for the treatment of vaginal atrophy: a double-blind placebo-controlled trial investigating the efficacy of pessaries containing 0.2mg and 0.03mg estriol. Maturitas 71: 360–368. 10.1016/j.maturitas.2011.12.022 [DOI] [PubMed] [Google Scholar]
- 49. Henriksson L, Stjernquist M, Boquist L, Alander U, Selinus I (1994) A comparative multicenter study of the effects of continuous low-dose estradiol released from a new vaginal ring versus estriol vaginal pessaries in postmenopausal women with symptoms and signs of urogenital atrophy. Am J Obstet Gynecol 171: 624–632. [DOI] [PubMed] [Google Scholar]
- 50. Melis GB, Paoletti AM, Murgia C, Piras B, Pilia I, et al. (1997) Vaginal estriol and benzidamine in the treatment of urogenital disorders during the postmenopause. <ORIGINAL> ESTRIOLO VAGINALE E BENZIDAMINA NEL TRATTAMENTO DEI DISTURBI UROGINECOLOGICI DEL CLIMATERIO. Giornale Italiano di Ostetricia e Ginecologia 19: 303–312. [Google Scholar]
- 51. Nachtigall LE (1994) Comparative study: Replens versus local estrogen in menopausal women. Fertil Steril 61: 178–180. [DOI] [PubMed] [Google Scholar]
- 52. Simon J, Nachtigall L, Gut R, Lang E, Archer DF, et al. (2008) Effective treatment of vaginal atrophy with an ultra-low-dose estradiol vaginal tablet.[Erratum appears in Obstet Gynecol. 2008 Dec;112(6):1392]. Obstet Gynecol 112: 1053–1060. 10.1097/AOG.0b013e31818aa7c3 [DOI] [PubMed] [Google Scholar]
- 53. Weisberg E, Ayton R, Darling G, Farrell E, Murkies A, et al. (2005) Endometrial and vaginal effects of low-dose estradiol delivered by vaginal ring or vaginal tablet. Climacteric 8: 83–92. [DOI] [PubMed] [Google Scholar]
- 54. Bruno RV (2012) Treatment of urogenital atrophy with the local administration of oestrogens: A randomized, controlled study in climateric and postmenopausal women. Revista Brasileira de Medicina 69: 230–235. [Google Scholar]
- 55. Barentsen R, van de Weijer PH, Schram JH (1997) Continuous low dose estradiol released from a vaginal ring versus estriol vaginal cream for urogenital atrophy. EurJ Obstet Gynecol ReprodBiol 71: 73–80. [DOI] [PubMed] [Google Scholar]
- 56. Gupta P, Ozel B, Stanczyk FZ, Felix JC, Mishell DR Jr (2008) The effect of transdermal and vaginal estrogen therapy on markers of postmenopausal estrogen status. Menopause 15: 94–97. [DOI] [PubMed] [Google Scholar]
- 57. Rioux JE, Devlin C, Gelfand MM, Steinberg WM, Hepburn DS (2000) 17beta-estradiol vaginal tablet versus conjugated equine estrogen vaginal cream to relieve menopausal atrophic vaginitis. Menopause 7: 156–161. [DOI] [PubMed] [Google Scholar]
- 58. Bachmann G, Lobo RA, Gut R, Nachtigall L, Notelovitz M (2008) Efficacy of low-dose estradiol vaginal tablets in the treatment of atrophic vaginitis: a randomized controlled trial. Obstet Gynecol 111: 67–76. 10.1097/01.AOG.0000296714.12226.0f [DOI] [PubMed] [Google Scholar]
- 59. Capobianco G, Wenger JM, Meloni GB, Dessole M, Cherchi PL, et al. (2014) Triple therapy with Lactobacilli acidophili, estriol plus pelvic floor rehabilitation for symptoms of urogenital aging in postmenopausal women. Arch Gynecol Obstet 289: 601–608. 10.1007/s00404-013-3030-6 [DOI] [PubMed] [Google Scholar]
- 60. Cardozo LD, Wise BG, Benness CJ (2001) Vaginal oestradiol for the treatment of lower urinary tract symptoms in postmenopausal women—a double-blind placebo-controlled study. J Obstet Gynaecol 21: 383–385. [DOI] [PubMed] [Google Scholar]
- 61. Enzelsberger H, Kurz C, Schatten C, Huber J (1991) Effects of intravaginal application of oestriol tablets in women with urge incontinence. <ORIGINAL> ZUR WIRKSAMKEIT EINER INTRAVAGINALEN OSTRIOLTABLETTENAPPLIKATION BEI FRAUEN MIT URGE-INKONTINENZ. Geburtshilfe Frauenheilkd 51: 834–838. [DOI] [PubMed] [Google Scholar]
- 62. Sacco F, Rigon G, Carbone A, Sacchini D (1990) Transvaginal estrogen therapy of stress incontinence. Minerva Ginecol 42: 539–544. [PubMed] [Google Scholar]
- 63. Holtedahl K, Verelst M, Schiefloe A (1998) A population based, randomized, controlled trial of conservative treatment for urinary incontinence in women. Acta Obstet Gynecol Scand 77: 671–677. [DOI] [PubMed] [Google Scholar]
- 64. Henalla SM, Millar DR, Wallace KJ (1990) Surgical versus conservative management for post-menopausal genuine stress incontinence of urine. NeurourolUrodyn 9: 436–437. [Google Scholar]
- 65. Henalla SM, Hutchins CJ, Castleden CM (1989) Non-operative methods in the treatment of female genuine stress incontinence or urine. JObstetGynaecol 9: 222–225. [Google Scholar]
- 66. Beisland HO, Fossberg E, Moer A, Sander S (1984) Urethral sphincteric insufficiency in postmenopausal females: treatment with phenylpropanolamine and estriol separately and in combination. A urodynamic and clinical evaluation. Urol Int 39: 211–216. [DOI] [PubMed] [Google Scholar]
- 67. Nelken RS, Ozel BZ, Leegant AR, Felix JC, Mishell DR Jr (2011) Randomized trial of estradiol vaginal ring versus oral oxybutynin for the treatment of overactive bladder. Menopause 18: 962–966. 10.1097/gme.0b013e3182104977 [DOI] [PubMed] [Google Scholar]
- 68. Serati M, Salvatore S, Uccella S, Cardozo L, Bolis P (2009) Is there a synergistic effect of topical oestrogens when administered with antimuscarinics in the treatment of symptomatic detrusor overactivity? EurUrol 55: 713–719. [DOI] [PubMed] [Google Scholar]
- 69. Tseng LH, Wang AC, Chang YL, Soong YK, Lloyd LK, et al. (2009) Randomized comparison of tolterodine with vaginal estrogen cream versus tolterodine alone for the treatment of postmenopausal women with overactive bladder syndrome. NeurourolUrodyn 28: 47–51. [DOI] [PubMed] [Google Scholar]
- 70. Lose G, Englev E (2000) Oestradiol-releasing vaginal ring versus oestriol vaginal pessaries in the treatment of bothersome lower urinary tract symptoms. BJOG 107: 1029–1034. [DOI] [PubMed] [Google Scholar]
- 71. Enzelsberger H, Schatten C, Kurz C, Zorzi P (1990) [Treatment of female urge incontinence by local estrogen therapy]. [German]. GynakolRundsch 30 Suppl 1: 235–236. [PubMed] [Google Scholar]
- 72. Long CY, Liu CM, Hsu SC, Chen YH, Wu CH, et al. (2006) A randomized comparative study of the effects of oral and topical estrogen therapy on the lower urinary tract of hysterectomized postmenopausal women. Fertil Steril 85: 155–160. [DOI] [PubMed] [Google Scholar]
- 73. Felding C, Mikkelsen AL, Clausen HV, Loft A, Larsen LG (1992) Preoperative treatment with oestradiol in women scheduled for vaginal operation for genital prolapse. A randomised, double-blind trial. Maturitas 15: 241–249. [DOI] [PubMed] [Google Scholar]
- 74.Nikas I, Koundouri MRA, Gavriil I, Kilbasanis I (2012) Management of cystocele with associated urine incontinence in menopausal women. Maturitas Conference: 9th European Congress on Menopause and Andropause Athens Greece. Conference Start: 20120328 Conference End: 20120331. Conference Publication:: S74.
- 75.Vaccaro CM, Crisp CC, Estanol MV, Fellner AN, Mutema GK, et al. (2011) Administration of vaginal estrogen in women with vaginal atrophy prior to prolapse surgery: An assessment of quality of life outcomes and medication adherence. International Urogynecology Journal and Pelvic Floor Dysfunction Conference: 36th Annual Meeting of the International Urogynecological Association, IUGA 2011 Lisbon Portugal. Conference Start: 20110628 Conference End: 20110702. Conference Publication:: S1839-S1840.
- 76. Rees M, Perez-Lopez FR, Ceasu I, Depypere H, Erel T, et al. (2012) EMAS clinical guide: low-dose vaginal estrogens for postmenopausal vaginal atrophy. Maturitas 73: 171–174. 10.1016/j.maturitas.2012.06.009 [DOI] [PubMed] [Google Scholar]
- 77. Smith P (1993) Estrogens and the urogenital tract. Studies on steroid hormone receptors and a clinical study on a new estradiol-releasing vaginal ring. Acta ObstetGynecolScandSuppl 157: 1–26. [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
(DOC)
(DOC)
(DOC)
(DOC)
Data Availability Statement
All relevant data are within the paper and its Supporting Information files.