

Abstract
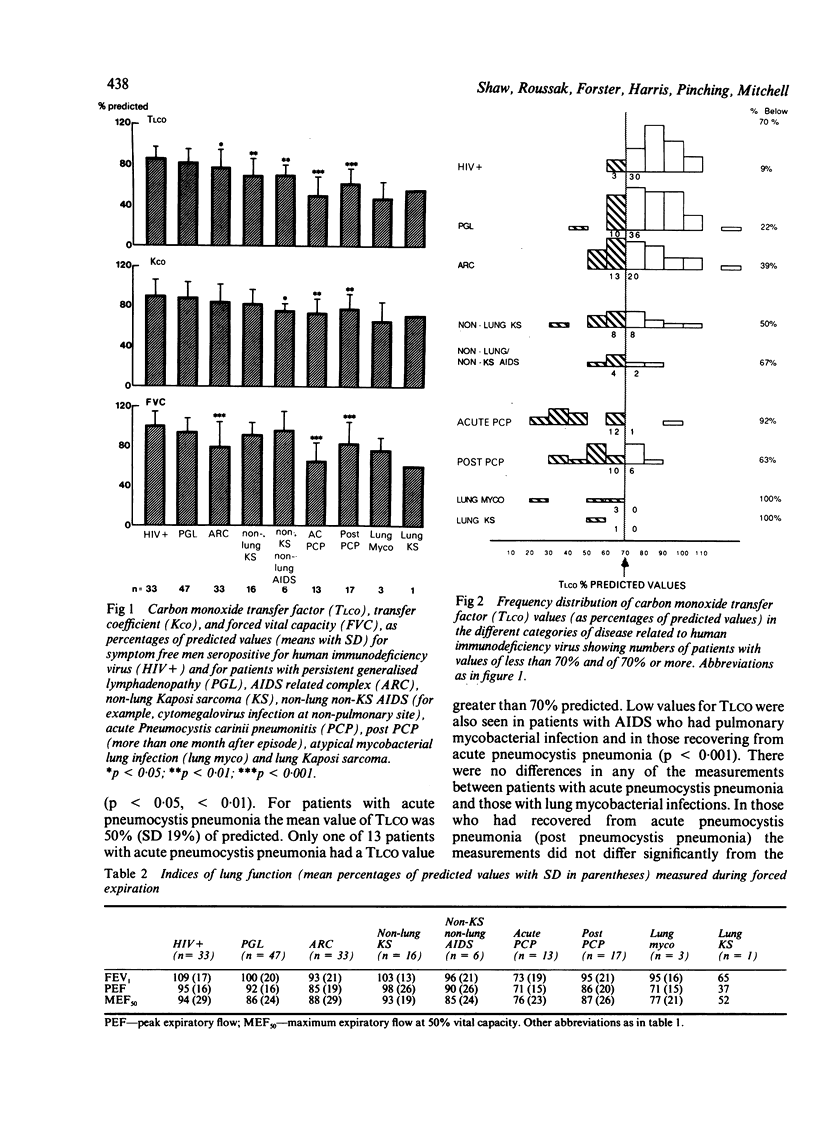
Pulmonary function was measured in 169 male patients seropositive for the human immunodeficiency virus (HIV). The transfer factor for carbon monoxide (TLCO) in symptom free patients and patients with persistent generalised lymphadenopathy was normal (greater than 83% of predicted values). Patients with the AIDS related complex, non-pulmonary Kaposi sarcoma, and non-pulmonary non-Kaposi sarcoma AIDS (that is, opportunist infections affecting other organs) had lower mean values for TLCO (77%, 70%, and 70% of predicted respectively). These values were significantly lower than values for symptom free patients. Lower mean values of 50% and 63% predicted TLCO were observed in patients during the acute and recovery phases of Pneumocystis carinii pneumonia. TLCO was also low in patients with lung mycobacterial infection and in a patient with lung Kaposi sarcoma. Forced expiratory volume in one second, peak expiratory flow, and maximal expiratory flow at 50% of vital capacity were significantly reduced only in patients with acute pneumocystis pneumonia. This study shows that abnormalities in the results of pulmonary function tests, particularly TLCO, although greatest in patients with pulmonary complications of AIDS, are also present in patients with AIDS but without other evidence of pulmonary disease, and in patients with the AIDS related complex. The predictive and prognostic implications of these findings require further investigation.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Coleman D. L., Dodek P. M., Golden J. A., Luce J. M., Golden E., Gold W. M., Murray J. F. Correlation between serial pulmonary function tests and fiberoptic bronchoscopy in patients with Pneumocystis carinii pneumonia and the acquired immune deficiency syndrome. Am Rev Respir Dis. 1984 Mar;129(3):491–493. doi: 10.1164/arrd.1984.129.3.491. [DOI] [PubMed] [Google Scholar]
- Engelberg L. A., Lerner C. W., Tapper M. L. Clinical features of Pneumocystis pneumonia in the acquired immune deficiency syndrome. Am Rev Respir Dis. 1984 Oct;130(4):689–694. doi: 10.1164/arrd.1984.130.4.689. [DOI] [PubMed] [Google Scholar]
- Epstein L. G., Sharer L. R., Cho E. S., Myenhofer M., Navia B., Price R. W. HTLV-III/LAV-like retrovirus particles in the brains of patients with AIDS encephalopathy. AIDS Res. 1984;1(6):447–454. doi: 10.1089/aid.1.1983.1.447. [DOI] [PubMed] [Google Scholar]
- Hopewell P. C., Luce J. M. Pulmonary involvement in the acquired immunodeficiency syndrome. Chest. 1985 Jan;87(1):104–112. doi: 10.1378/chest.87.1.104. [DOI] [PubMed] [Google Scholar]
- Kovacs J. A., Hiemenz J. W., Macher A. M., Stover D., Murray H. W., Shelhamer J., Lane H. C., Urmacher C., Honig C., Longo D. L. Pneumocystis carinii pneumonia: a comparison between patients with the acquired immunodeficiency syndrome and patients with other immunodeficiencies. Ann Intern Med. 1984 May;100(5):663–671. doi: 10.7326/0003-4819-100-5-663. [DOI] [PubMed] [Google Scholar]
- Murray J. F., Felton C. P., Garay S. M., Gottlieb M. S., Hopewell P. C., Stover D. E., Teirstein A. S. Pulmonary complications of the acquired immunodeficiency syndrome. Report of a National Heart, Lung, and Blood Institute workshop. N Engl J Med. 1984 Jun 21;310(25):1682–1688. doi: 10.1056/NEJM198406213102529. [DOI] [PubMed] [Google Scholar]
- Murray J. F., Garay S. M., Hopewell P. C., Mills J., Snider G. L., Stover D. E. NHLBI workshop summary. Pulmonary complications of the acquired immunodeficiency syndrome: an update. Report of the second National Heart, Lung and Blood Institute workshop. Am Rev Respir Dis. 1987 Feb;135(2):504–509. doi: 10.1164/arrd.1987.135.2.504. [DOI] [PubMed] [Google Scholar]
- Overland E. S., Nolan A. J., Hopewell P. C. Alteration of pulmonary function in intravenous drug abusers. Prevalence, severity, and characterization of gas exchange abnormalities. Am J Med. 1980 Feb;68(2):231–237. doi: 10.1016/0002-9343(80)90359-9. [DOI] [PubMed] [Google Scholar]
- Salahuddin S. Z., Rose R. M., Groopman J. E., Markham P. D., Gallo R. C. Human T lymphotropic virus type III infection of human alveolar macrophages. Blood. 1986 Jul;68(1):281–284. [PubMed] [Google Scholar]
- Stover D. E., White D. A., Romano P. A., Gellene R. A., Robeson W. A. Spectrum of pulmonary diseases associated with the acquired immune deficiency syndrome. Am J Med. 1985 Mar;78(3):429–437. doi: 10.1016/0002-9343(85)90334-1. [DOI] [PubMed] [Google Scholar]
- Suffredini A. F., Ognibene F. P., Lack E. E., Simmons J. T., Brenner M., Gill V. J., Lane H. C., Fauci A. S., Parrillo J. E., Masur H. Nonspecific interstitial pneumonitis: a common cause of pulmonary disease in the acquired immunodeficiency syndrome. Ann Intern Med. 1987 Jul;107(1):7–13. doi: 10.7326/0003-4819-107-1-7. [DOI] [PubMed] [Google Scholar]
- Warren J. B., Shaw R. J., Weber J. N., Holt D. A., Keal E. E., Pinching A. J. Role of fibreoptic bronchoscopy in management of pneumonia in acquired immune deficiency syndrome. Br Med J (Clin Res Ed) 1985 Oct 12;291(6501):1012–1013. doi: 10.1136/bmj.291.6501.1012. [DOI] [PMC free article] [PubMed] [Google Scholar]