

Abstract
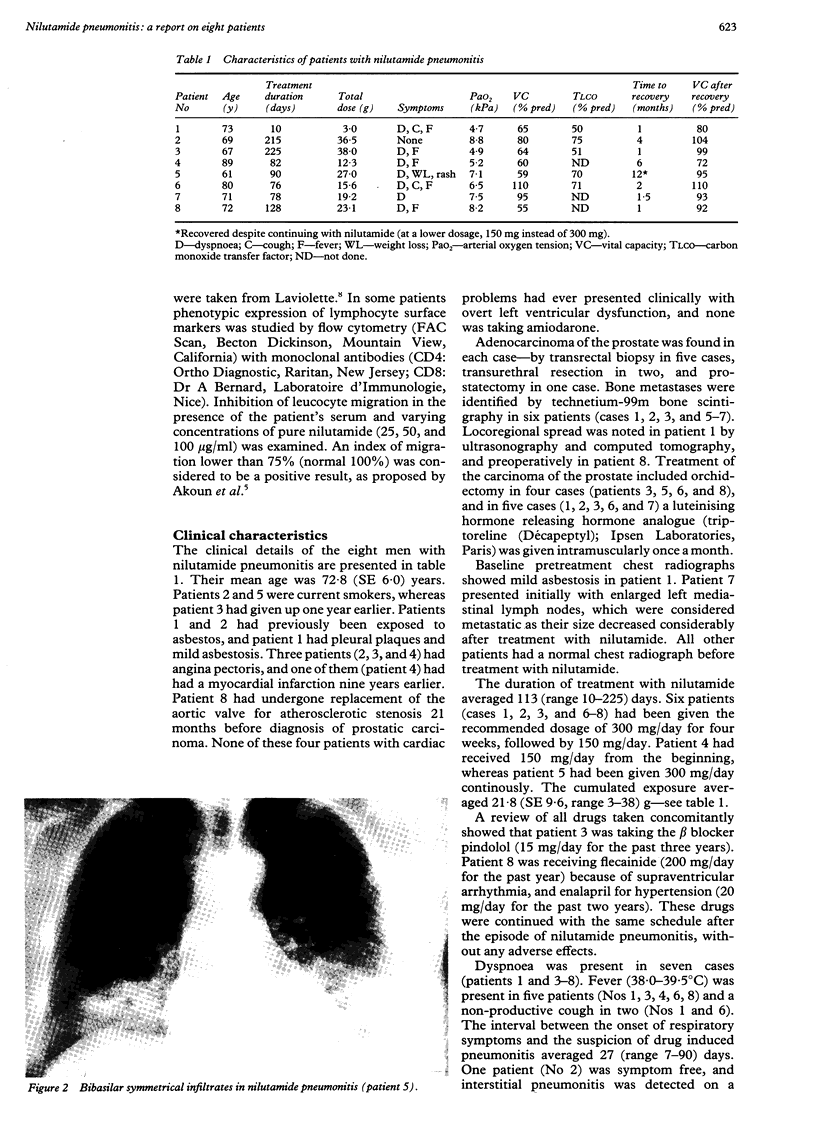
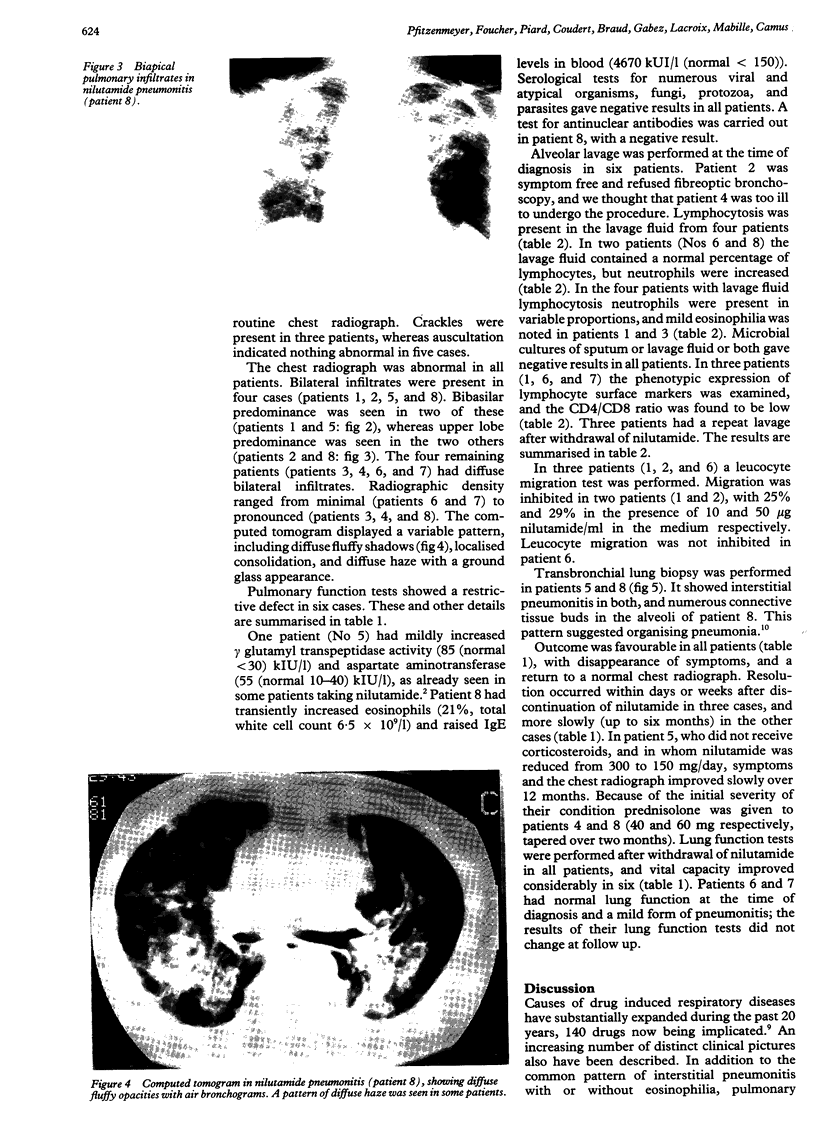
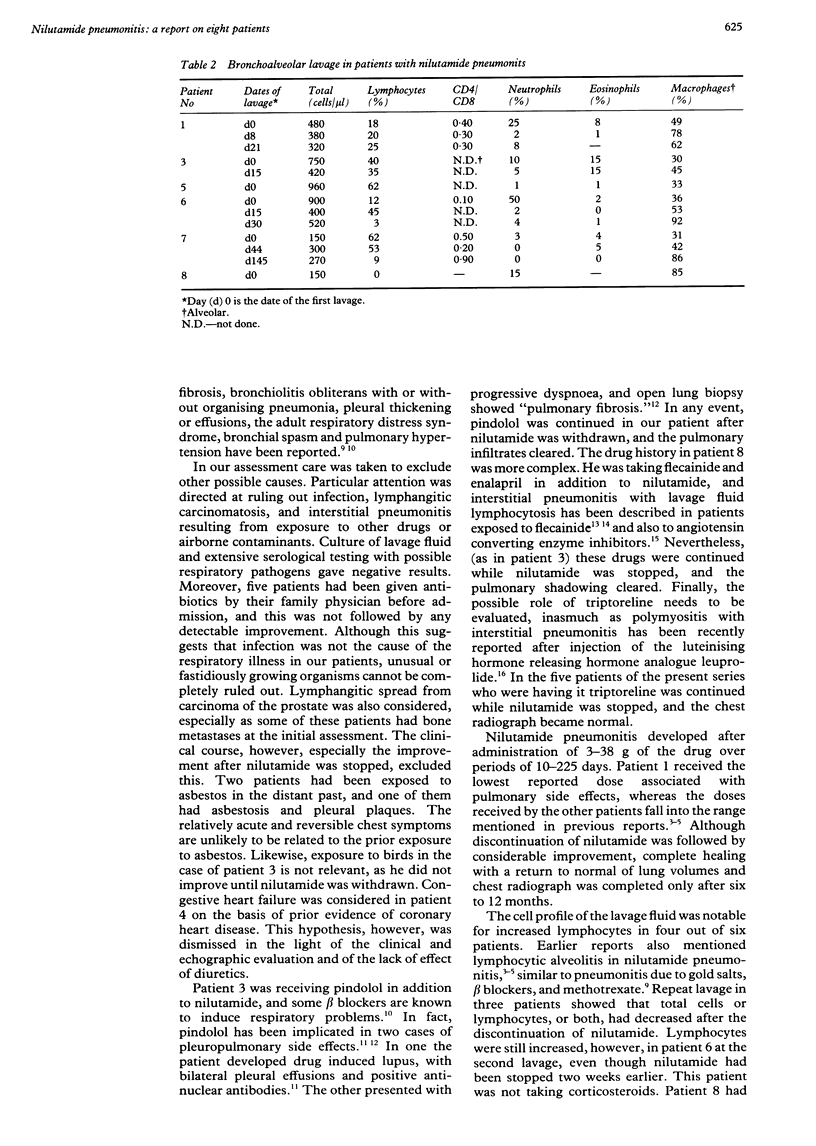
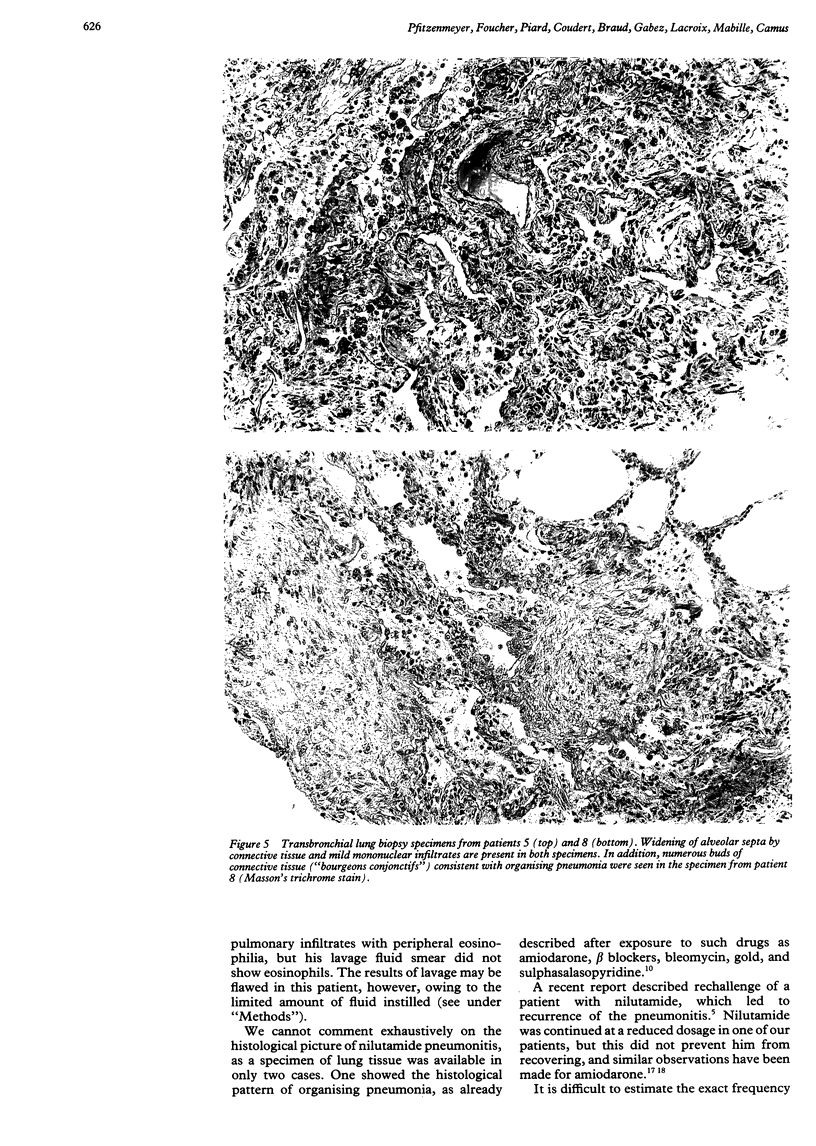
BACKGROUND: Nilutamide is a new, specific synthetic antiandrogen, released in several countries for the treatment of metastatic carcinoma of the prostate. Eight patients at the University Medical Centre at Dijon and affiliated referring hospitals developed reversible pulmonary opacities and respiratory symptoms while taking the drug. METHODS: Records of eight patients who developed new, otherwise unexplained chest opacities while taking nilutamide were reviewed. In each patient a careful aetiological search was made for other environmental or endogenous causes. Six patients underwent bronchoalveolar lavage, and lavage fluid was cultured. Corticosteroids were not given, unless gas exchange was compromised (two patients). RESULTS: The eight patients (all male) had had carcinoma of the prostate diagnosed on average 10.2 months earlier. All had improved with nilutamide, with a dramatic decrease of prostate specific antigen levels. Seven had received nilutamide at the recommended dosage of 150 mg/day, and one had received twice that amount. Treatment had lasted on average 113 (range 10-225) days, and the mean cumulated exposure was 21.8 (3-38) grams. The chest radiographs showed bilateral infiltrates, with no consistent topographic predilection. A restrictive lung defect was present in six patients and hypoxia in all (mean arterial oxygen tension (PaO2) 6.6 kPa). Bronchoalveolar lavage showed lymphocytosis in four patients and neutrophilia in two. The outcome was favourable in all patients after they had stopped nilutamide only (five patients), with corticosteroids (two patients) or a simple reduction of nilutamide from 300 to 150 mg/day (one patient). Recovery was associated with improvement of pulmonary function and PaO2. CONCLUSION: Nilutamide is associated with interstitial pneumonitis in about 1% of patients and appears reversible.
Full text
PDF
Images in this article


Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Akoun G. M., Cadranel J. L., Israel-Biet D., Gauthier-Rahman S. Flecainide-associated pneumonitis. Lancet. 1991 Jan 5;337(8732):49–49. doi: 10.1016/0140-6736(91)93367-i. [DOI] [PubMed] [Google Scholar]
- Akoun G. M., Liote H. A., Liote F., Gauthier-Rahman S., Kuntz D. Provocation test coupled with bronchoalveolar lavage in diagnosis of drug (nilutamide)-induced hypersensitivity pneumonitis. Chest. 1990 Feb;97(2):495–498. doi: 10.1378/chest.97.2.495. [DOI] [PubMed] [Google Scholar]
- Bensaid J., Aldigier J. C., Gualde N. Systemic lupus erythematosus syndrome induced by pindolol. Br Med J. 1979 Jun 16;1(6178):1603–1604. doi: 10.1136/bmj.1.6178.1603. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Béland G., Elhilali M., Fradet Y., Laroche B., Ramsey E. W., Trachtenberg J., Venner P. M., Tewari H. D. Total androgen ablation: Canadian experience. Urol Clin North Am. 1991 Feb;18(1):75–82. [PubMed] [Google Scholar]
- Camus P., Lombard J. N., Perrichon M., Piard F., Guérin J. C., Thivolet F. B., Jeannin L. Bronchiolitis obliterans organising pneumonia in patients taking acebutolol or amiodarone. Thorax. 1989 Sep;44(9):711–715. doi: 10.1136/thx.44.9.711. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cooper J. A., Jr, White D. A., Matthay R. A. Drug-induced pulmonary disease. Part 1: Cytotoxic drugs. Am Rev Respir Dis. 1986 Feb;133(2):321–340. doi: 10.1164/arrd.1986.133.2.321. [DOI] [PubMed] [Google Scholar]
- Crayton H., Bohlmann T., Sufit R., Graziano F. M. Drug induced polymyositis secondary to leuprolide acetate (Lupron) therapy for prostate carcinoma. Clin Exp Rheumatol. 1991 Sep-Oct;9(5):525–528. [PubMed] [Google Scholar]
- Decensi A., Guarneri D., Paoletti M. C., Lalanne J. M., Merlo F., Boccardo F. Phase II study of the pure non-steroidal antiandrogen nilutamide in prostatic cancer. Italian Prostatic Cancer Project (PONCAP). Eur J Cancer. 1991;27(9):1100–1104. doi: 10.1016/0277-5379(91)90301-s. [DOI] [PubMed] [Google Scholar]
- Gomez J. L., Dupont A., Cusan L., Tremblay M., Tremblay M., Labrie F. Simultaneous liver and lung toxicity related to the nonsteroidal antiandrogen nilutamide (Anandron): a case report. Am J Med. 1992 May;92(5):563–566. doi: 10.1016/0002-9343(92)90756-2. [DOI] [PubMed] [Google Scholar]
- Hanston P., Evrard P., Mahieu P., Wallemacq P., Friob M., Hassoun A. Flecainide-associated interstitial pneumonitis. Lancet. 1991 Feb 9;337(8737):371–372. doi: 10.1016/0140-6736(91)91010-r. [DOI] [PubMed] [Google Scholar]
- Laviolette M. Lymphocyte fluctuation in bronchoalveolar lavage fluid in normal volunteers. Thorax. 1985 Sep;40(9):651–656. doi: 10.1136/thx.40.9.651. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leech J. A., Gallastegui J., Swiryn S. Pulmonary toxicity of amiodarone. Chest. 1984 Mar;85(3):444–445. doi: 10.1378/chest.85.3.444. [DOI] [PubMed] [Google Scholar]
- Liu F. L., Cohen R. D., Downar E., Butany J. W., Edelson J. D., Rebuck A. S. Amiodarone pulmonary toxicity: functional and ultrastructural evaluation. Thorax. 1986 Feb;41(2):100–105. doi: 10.1136/thx.41.2.100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miller A., Thornton J. C., Warshaw R., Anderson H., Teirstein A. S., Selikoff I. J. Single breath diffusing capacity in a representative sample of the population of Michigan, a large industrial state. Predicted values, lower limits of normal, and frequencies of abnormality by smoking history. Am Rev Respir Dis. 1983 Mar;127(3):270–277. doi: 10.1164/arrd.1983.127.3.270. [DOI] [PubMed] [Google Scholar]
- Musk A. W., Pollard J. A. Pindolol and pulmonary fibrosis. Br Med J. 1979 Sep 8;2(6190):581–582. doi: 10.1136/bmj.2.6190.581-a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schatz P. L., Mesologites D., Hyun J., Smith G. J., Lahiri B. Captopril-induced hypersensitivity lung disease. An immune-complex-mediated phenomenon. Chest. 1989 Mar;95(3):685–687. doi: 10.1378/chest.95.3.685. [DOI] [PubMed] [Google Scholar]
- Seigneur J., Trechot P. F., Hubert J., Lamy P. Pulmonary complications of hormone treatment in prostate carcinoma. Chest. 1988 May;93(5):1106–1106. doi: 10.1378/chest.93.5.1106. [DOI] [PubMed] [Google Scholar]