

Abstract
Background
Hearing loss is one of the most common chronic conditions in older adults. In audiology literature, several studies have examined the attitudes and behavior of people with hearing loss; however, not much is known about the manner in which society in general views and perceives hearing loss. This exploratory study was aimed at understanding the social representation of hearing loss (among the general public) in the countries of India, Iran, Portugal, and the UK. We also compared these social representations.
Materials and methods
The study involved a cross-sectional design, and participants were recruited using the snowball sampling method. A total of 404 people from four countries participated in the study. Data were collected using a free-association task where participants were asked to produce up to five words or phrases that came to mind while thinking about hearing loss. In addition, they were also asked to indicate if each word they presented had positive, neutral, or negative associations in their view. Data were analyzed using various qualitative and quantitative methods.
Results
The most frequently occurring categories were: assessment and management; causes of hearing loss; communication difficulties; disability; hearing ability or disability; hearing instruments; negative mental state; the attitudes of others; and sound and acoustics of the environment. Some categories were reported with similar frequency in most countries (eg, causes of hearing loss, communication difficulties, and negative mental state), whereas others differed among countries. Participants in India reported significantly more positive and fewer negative associations when compared to participants from Iran, Portugal, and the UK. However, there was no statistical difference among neutral responses reported among these countries. Also, more differences were noted among these countries than similarities.
Conclusion
These findings provide useful insights into the public perception of hearing loss that may prove useful in public education and counseling.
Keywords: hearing loss, hearing impairment, social representation, societal attitude, cross-culture, perception of disability
Introduction
Hearing loss is one of the most frequent chronic conditions in older adults. There are over 360 million people (5% of the population) worldwide with disabling hearing loss.1 Hearing loss can result in various physical, mental, and social consequences to both the person with hearing loss and to their significant others.2,3 Despite these adverse consequences, only a small number of people with hearing loss seek help and adopt interventions for their hearing loss.4 Hearing loss is most often recognized as a medical problem related to the physical structure of the body and physical function of the body. However, research has clearly shown the close relationship between hearing loss and such factors as communication, emotions, identity, and social relations.5 That means that hearing loss is a multidimensional state of being and must be addressed from a clinical perspective in a multiprofessional way and in research in an interdisciplinary way.
The World Health Organization’s International Classification for Functioning, Disability and Health (ICF) model provides a comprehensive framework to understand and describe any disability.6 According to this model, health and disability are an interaction between such aspects as body, activities, participation, environmental, and personal factors. In the ICF core sets for hearing loss, various factors related to society have been identified to be important in relation to hearing loss.7–9 Studies on patient journeys of persons with hearing loss suggest that various aspects, including significant others and various people in the surrounding environment, can influence the help-seeking behavior of persons with hearing loss.10,11 Literature on hearing health care suggests that various factors (including the attitude of health professionals toward their patients) may have some impact on help-seeking behavior and outcome of hearing rehabilitation.12–15 This highlights the importance of understanding societal attitudes toward hearing loss. The limited scientific literature focusing on this specific area calls for an immediate need for research and subsequent documentation of findings.
Attitudes toward hearing loss
In the area of hearing health care, there is growing literature on attitudes to hearing help-seeking and hearing-aid uptake.15,16 Generally, studies of attitudes related to hearing loss have focused on the attitudes of the persons with hearing loss. Few studies have investigated the attitudes of others (eg, significant others, coworkers) to hearing loss.17,18 Also, these studies have generally used “stigma theory” as a theoretical basis.19 Attitudes of a person with hearing loss toward his/her hearing loss have been linked to coping behavior, acceptance of hearing loss, consultation with hearing health care professionals to seek help, and uptake and use of hearing rehabilitation.15 For example, higher uptake20 and more frequent use21 of hearing aids have been reported among those who accepted hearing loss than for those who did not accept and/or who had less acceptance of their hearing loss. From hearing health care professionals’ perspectives, acceptance of hearing loss generally refers to seeking help and taking up rehabilitation involving intervention strategies. Therefore, defining acceptance from a psychological viewpoint (ie, actively taking in thoughts, memories, and feelings without actively changing them) may be more appropriate in relation to health and disability, as many people with hearing loss, although aware of their difficulties, are not ready to take action toward it.22 Although these studies on attitudes toward people with hearing loss uncover some important information, not much is known about the attitudes and perception of the general population with regard to hearing loss.
Importance of environmental factors
Most studies in the literature have focused on the negative consequences of hearing loss, although emerging literature on positive experiences of hearing loss as reported by persons with hearing loss and their significant others does indeed exist.23 According to the ICF framework, various environmental and personal factors can act both as barriers and facilitators in relation to health and disability.24 Therefore, it is important to understand hearing disability and its consequences from a wider framework, wherein it captures positive, neutral, and negative aspects rather than solely negative perspectives.
As mentioned earlier, ICF’s environmental factors include societal attitudes, norms, practices, and ideologies. The theoretical base for attitude research is very restricted, and does not grasp the broader perspective of these environmental factors. A theory that has been developed in order to understand and explain not only a person’s worldview but also how it is related to behavioral aspects, is social representation theory (SRT). In this theory, attitude is recognized as a result of a person’s representation, indicating that it is a more fundamental and comprehensive approach to the issue of “societal attitudes”.
Social representation theory
SRT was first formulated by Moscovici, who defined it thus: Systems of values, ideas and practices with a two-fold function: first, to establish an order which will enable individuals to orientate themselves in their material and social world and to master it; secondly, to enable communication to take place amongst members of a community by providing them with a code for social exchange and a code for naming and classifying unambiguously the various aspects of their world and their individual and group history.25 Social representation is the collective knowledge made to organize behavior and guide communications in groups.26,27 In other words, social representation refers to common knowledge and information that is collectively elaborated by groups in intercommunication processes. This theory has been applied in various disciplines to understand particular social phenomena.28–31
Although studies based on “attitudes” provide important information about various social phenomena, research has clearly demonstrated the lack of correlation between the attitude and the actual behavior.32 However, with the use of SRT, which reveals what perceptions the population as a whole may have on a particular phenomenon, the degree of measurable correlation and influence upon the actual behavior that these perceptions have can be clearly seen.33,34
Cross-cultural studies in hearing health care
Over 80% of people with hearing loss live in low- and middle-income countries. However, very limited published research is produced in those countries. In February 2013, an international seminar entitled Cross-Cultural Communication: Exploring Cross-Cultural Differences and Similarities in Attitudes Towards Hearing Help-Seeking and Uptake of Hearing Aids was held in Bristol, UK. The seminar concluded that there are few cross-cultural studies in the area of hearing health care. Also, an immediate need for research in this area was identified.35 Moreover, it is worth noting that the ICF is a global conceptual framework that should be culturally neutral, and the factors discussed here are expected to be a global phenomenon, although we do not know much about cultural differences regarding social representation of hearing loss. Previous research has indicated that there are cultural differences in how hearing loss is perceived and managed in people with different cultural backgrounds (for review, see Zhao et al),35 but to the best of our knowledge no comparative study has been conducted with regard to social representation of hearing loss. Therefore, we are keen to develop international cross-cultural studies that provide better understanding of how hearing loss is perceived and managed across the globe.
Study aim
The current study was exploratory in nature, and was aimed at understanding the general public’s social representation of hearing loss in India, Iran, Portugal, and the UK. We also compared these results to explore cross-cultural differences and similarities among these countries.
Materials and methods
Ethical considerations
Ethical approval was obtained for each country from local institutional ethical boards, which included: the All India Institute of Speech and Hearing, Mysore, India; the Department of Audiology, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran; the School of Allied Health Sciences, Polytechnic Institute of Porto, Porto, Portugal; and the Research Ethics Committee, Anglia Ruskin University, Cambridge, UK.
Study design and participants
The study used a cross-sectional design, and the data were collected from a researcher based in each country. However, the main author coordinated the data collection with regular online meetings and email interactions to ensure that they all followed the method consistently. The four countries chosen differ in terms of culture, economy, and health care-service delivery. Table 1 provides some useful information about these four countries.
Table 1.
Population details in India, Iran, Portugal, and the UK
| India | Iran | Portugal | UK | |
|---|---|---|---|---|
| Population (million) | 1,210 | 77 | 11 | 64 |
| Continent | Asia | Asia | Europe | Europe |
| City where data collected | Mysore | Tehran | Porto | Cambridge |
| Population in city where data collected (million) | 1 | 8.3 | 1.3 | 0.13 |
| National language (language of local place if different) | Hindi (Kannada) | Farsi | Portuguese | English |
| Main health care-service provision | Private | Public | Private | Public |
Participants were recruited using the snowball sampling method. Researchers approached colleagues and friends in each country via place of work (university) with the study-information sheet, requesting their participation. Participants signed no separate consent form. However, completing the questionnaire and returning it was considered consent. The participants were also requested to pass the study-information sheet and questionnaire to their acquaintances. Those who were interested in participating were given the opportunity to ask questions and complete a simple questionnaire. In total, 404 people from four countries participated in the study (Table 2). The study sample consisted of individuals from the general population with no particular knowledge on hearing loss, although it included a few elderly individuals with hearing difficulties.
Table 2.
Demographic details
| All countries (n=404) |
India (n=101) |
Iran (n=100) |
Portugal (n=103) |
UK (n=100) |
|
|---|---|---|---|---|---|
| Age, years (mean ± SD) | 41.14±16.8 | 42.82±14.6 | 41.47±14.8 | 38.70±19.6 | 41.62±17.5 |
| Sex (% male) | 50.2 | 46.6 | 51 | 49.5 | 54 |
| Education (%) | |||||
| • Compulsory | 17.4 | 24.8 | 7 | 29.1 | 8 |
| • Secondary | 24.4 | 7.9 | 11 | 44.7 | 33 |
| • Tertiary | 58.2 | 67.3 | 82 | 26.2 | 59 |
| Profession (%) | |||||
| • Nonmanual | 46.3 | 49.5 | 53 | 19.4 | 64 |
| • Manual | 16.6 | 16.8 | 27 | 13.6 | 9 |
| • No occupation | 37.1 | 33.7 | 20 | 67 | 27 |
| Family history of hearing loss (% yes) | 40.1 | 29.7 | 31 | 49.5 | 50 |
Data collection
Data were collected using a free-association task, in which the object of representation is used to prompt associations, such as hearing loss or hearing aids. This method is commonly used in the social sciences to access the semantic content of social representation.30,31,36 In the first instance, the respondents were asked to state in writing the first four to five words or expressions that came to their minds when thinking about hearing loss. As the responses are elicited spontaneously, they are less controlled, and provide a better understanding of what constitutes the semantic universe of the term or subject studied.37 Following this, they were asked to indicate if the words or phrases reported represented a positive, neutral, or negative aspect of the phenomenon studied. Demographic information such as age, sex, education, profession, and family history of hearing loss. No interview was conducted, but researchers explained the instructions if the participants had problems understanding the written instructions.
In the first instance, an English-language version of the questionnaires that was developed was used in the UK. Furthermore, it was translated into Kannada, Farsi, and Portuguese, and the translated versions were used in India, Iran, and Portugal respectively. We followed the well-accepted forward- and back-translation method.38 The aim of the translation process was to achieve different language versions of the English questionnaire that were conceptually equivalent in each of the target countries/cultures. Therefore, the focus was on cross-cultural and conceptual rather than on linguistic/literal equivalence. This process involved four main stages: 1) forward translation; 2) expert back translation; 3) review and resolution of any discrepancies; and 4) pretesting with five participants each: in India, Iran, and Portugal. The translation of the associations (ie, responses from questionnaires) from the local language to English was made by the researchers who collected the data in each country. The data analysis was done centrally by two authors to ensure consistency. However, the first researcher cross-checked and discussed the words and phrases collected in the different countries with the researchers before the categorization process started.
In this article, we discuss social representation of hearing loss. However, we have presented results of social representation of hearing aids in a recent article.39
Data analysis
The data were analyzed using various qualitative and quantitative methods: categorization of associations, co-occurrence analysis, and χ2 analysis.
We used the qualitative content-analysis method40 for the categorization of associations, which involved grouping words and phrases that have the same meaning. The data analysis from all four countries was done mainly by the primary researcher and cross-checked by another researcher. Any discrepancies were resolved by discussion among the researchers. When there was no consensus, or if the meaning of the words/phrases was not clear, researchers who performed the analysis consulted with the researchers who collected and translated data in the respective countries. Where responses involved several words or a sentence, a significant keyword was identified, which helped in assigning them to a specific category. Also, the positive, neutral, and negative associations reported by each country’s participants were counted.
The co-occurrence analysis (also known as “similarities analysis” or “maximum tree”) is based on mathematical graph theory,41 and presents an index that shows the frequency of the categories reported (bigger bubbles representing the more frequent) and also the frequency of the categories co-occurring (ie, the number of people reporting the same answer). The number corresponding to the connection between each category indicates the number of people reporting in both categories. Although there could be a large number of these connections, the index shows only the main connections. This analysis was performed using the software program Iramuteq (IRaMuTeQ, Version 0.7 alpha 2, Toulouse, France),42 which uses the Igraph package43 of the R-based software for multidimensional analysis of texts.44 The χ2 analysis was also performed to determine if there were any associations among countries in terms of positive, neutral, and negative connotations reported.
These methods (ie, free-association task for data collection, content analysis, and co-occurrence analysis for data analysis) are theoretically and methodologically well founded,37,45,46 and are used in social science to access the semantic content of social representations.30,31,36
Challenges in data collection and analysis
In this international study, we aimed to collect data in several countries, including the People’s Republic of China (PRC), India, Iran, Portugal, and the UK. However, the data in the PRC had some issues, presenting challenges to interpretation, eg, over 20% of the words or phrases reported had no meaning related to hearing loss, and a large proportion of the participants had indicated positive, neutral, and negative connotations with the words or phrases incorrectly (eg, negative mental state with positive connotation). We were unable to resolve this even after the researchers analyzing the data had extensive consultation with the researcher who collected and translated the data. Therefore, the data from the PRC was not included in any of the steps of the analysis and reporting. This may highlight one of any number of possible challenges in international cross-cultural research.
Moreover, there were some interesting observations made while collecting the data. For example, although the questionnaire was distributed in the local language of Kannada, approximately 35% of the Indian respondents reported answers in English. This may be because in India, people often use both English and the local language for both social and business purposes. Some respondents in Iran found it difficult to come up with five words or phrases, although most participants managed to come up with four to five words or phrases after pondering on the matter for a while.
Results
Table 2 shows the demographic details of the study participants. There was an equal spread of age- and sex-matched participants from each of the four countries. The age ranges of participants in different countries were: India 26–83 years, Iran 19–79 years, Portugal 18–85 years, and the UK 18–89 years. However, the population sample varied slightly in terms of other demographic variables. In the Portugal sample, there was a high percentage of people with no occupation. Also, in Portugal and the UK, the family history of hearing loss was as much as 50%, which may be due to the higher percentage of the aging population in these countries.
The participants’ responses fell into 34 main categories based on meaning, although not all categories were found in all four countries. Table 3 shows the categories and the frequency of those categories in each country. The most frequently occurring categories included assessment and management, causes of hearing loss, communication difficulties, disability, hearing ability, or disability, hearing instruments, negative mental state, others’ attitudes, and sound and acoustics of the environment. Some categories were reported with similar frequency in most countries, and these included causes of hearing loss, communication difficulties, and negative mental state. However, some categories were reported more frequently in some countries than in others (eg, the “hearing instruments” category was reported in Iran and the UK more frequently, whereas the category “others’ attitudes” was more frequently reported in India and Iran).
Table 3.
Percentage of categories reported in different countries
| Categories | Percentage of responses
|
|||||
|---|---|---|---|---|---|---|
| All countries | India | Iran | Portugal | UK | ||
| 1 | Activity limitations | 2.8 | 2.0 | 3.9 | 2.8 | 2.7 |
| 2 | Aging | 3.7 | 0.8 | 7.8 | 3.2 | 3 |
| 3 | Alternative modes of communication | 2.4 | 2.4 | 1.8 | 1.8 | 3.7 |
| 4 | Assessment and management | 6.7 | 14.7 | 3.5 | 4.4 | 3.9 |
| 5 | Attitude of the individual | 0.8 | 1 | 0.4 | 0.8 | 1 |
| 6 | Body structure | 3.1 | 1 | 4.3 | 5.7 | 1.2 |
| 7 | Causes of hearing loss | 8 | 8.6 | 9.6 | 7.7 | 6.6 |
| 8 | Challenging | 1.6 | 1.2 | 0.2 | 2.8 | 2.3 |
| 9 | Communication difficulties | 8.5 | 8.1 | 4.3 | 10.9 | 10.3 |
| 10 | Coping strategies | 1.3 | 1.4 | 1 | 0.8 | 1.8 |
| 11 | Dependence on others | 1.3 | 1 | 1 | 1 | 1.6 |
| 12 | Dependence on other senses | 0.9 | 1.4 | 0.2 | 1.2 | 1 |
| 13 | Disability | 11.5 | 2 | 13 | 17.4 | 13.5 |
| 14 | Education, employment and career issues | 1 | 2 | 0.6 | 0.8 | 0.4 |
| 15 | Friends and family members | 0.9 | – | 0.6 | 2.6 | 0.2 |
| 16 | Health condition | 2 | 6.2 | 0.8 | 0.6 | – |
| 17 | Hearing ability or disability | 4.6 | 8.2 | 2.2 | 4.4 | 3.5 |
| 18 | Hearing instruments | 4.9 | 0.6 | 9.6 | 3.8 | 5.5 |
| 19 | Isolation | 3.9 | 0.8 | 4.3 | 4 | 6.6 |
| 20 | Lifestyle and relationship changes | 2.2 | 2.6 | 0.2 | 3.6 | 2.3 |
| 21 | Need for support | 1.8 | 5.8 | 0.2 | – | 1.2 |
| 22 | Negative mental state | 8.5 | 5.8 | 8.8 | 7.1 | 12.3 |
| 23 | Not well understood | 1.1 | 3.2 | – | 0.4 | 0.8 |
| 24 | Orientation | 0.4 | – | 0.2 | 0.4 | 0.8 |
| 25 | Others’ attitudes | 3.6 | 4.6 | 4.7 | 2.2 | 2.9 |
| 26 | Positive mental state | 0.7 | 0.2 | 2.2 | – | 0.2 |
| 27 | Problem for others | 0.5 | 2 | – | – | 0.61 |
| 28 | Reduced ability | 1.6 | 1.6 | 0.8 | 3.6 | 0.4 |
| 29 | Social support | 0.4 | 1.6 | – | – | – |
| 30 | Sound and acoustics of the environment | 3.8 | 0.2 | 3.3 | 4.3 | 4.9 |
| 31 | Stress and exhaustion | 0.5 | – | 1.6 | – | 0.2 |
| 32 | Symptoms of hearing loss | 2.7 | 4.6 | 1 | 1.2 | 1.8 |
| 33 | Voice and speech functions | 2.5 | 3.2 | 5.9 | – | 1 |
| 34 | Vulnerable | 1.5 | 2 | 0.8 | 1 | 2.05 |
We counted positive, neutral, and negative connotations associated with responses to each category to identify what kinds of connotations they had. It is important to note that each category can carry a positive, neutral, or negative connotation depending on the respondents’ social representation. For example, “sympathy from others” can be a positive aspect, and “negligence and rudeness from others” can be seen as a negative aspect of the “others’ attitudes” category. Generally, the frequently occurring category “assessment and management” was largely associated with positive connotations, such categories as “hearing instruments” and “causes of hearing loss” were largely associated with neutral connotations, and such categories as “communication difficulties” and “negative mental state” were largely associated with negative connotations. Detailed analysis of the connotations to each category will be presented in our future articles.
Figure 1 shows the frequency of the positive, negative, and neutral connotations for hearing loss-related aspects in all countries. Respondents in India had significantly more positive connotations reported for hearing loss when compared to Iran (χ2=7.1, df=1; P=0.007), Portugal (χ2=13.71, df=1; P=0.0002), and the UK (χ2=25.12, df=1; P<0.0001). Although small differences were noted in the positive connotations reported by respondents in Iran, Portugal, and the UK, they were not statistically significant. No statistically significant differences were observed in neutral connotations reported by respondents among any of the four countries. Also, respondents in India had significantly fewer negative connotations reported when compared to respondents in Iran (χ2=4.57, df=1; P=0.03), Portugal (χ2=7.57, df=1; P=0.006), and the UK (χ2=7.43, df=1; P=0.006). However, no other statistically significant differences were observed among negative connotations reported by respondents in Iran, Portugal, or the UK.
Figure 1.
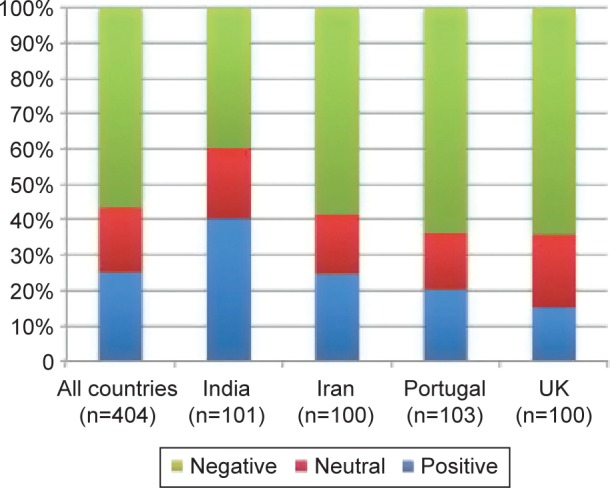
Percentages of associations ranked positive, neutral, and negative among participant groups.
Figure 2 presents the co-occurrence analysis index for all countries together, which have five themes (as indicated in color shading), based on the co-occurrence nodes. The numbers on the lines connecting two categories indicate the percentage of individuals who mentioned both these categories. The thickness of the lines is in proportion to the number. However, no meaning is associated with the vertical or horizontal connections. The most frequent category, “disability”, was linked with other frequent categories – “causes of hearing loss”, “communication difficulties”, “negative mental state”, and “hearing instruments” – by approximately 10%. This suggests that approximately 10% of the people talking about disability also talked about one of the other most frequent categories. The “disability”, “communication difficulties”, and “negative mental state” categories largely had negative connotations. However, the “causes of hearing loss” and “hearing instruments” categories had more neutral or positive connotations. Generally, hearing loss was considered a negative phenomenon within the societies of the countries participating in the study.
Figure 2.

Co-occurrence analysis index of qualitative categories for all countries (n=404).
Notes: Different colors indicate different themes in the data. The number on the line suggests the interconnection between two categories.
Figures 3–6 demonstrate co-occurrence analysis indices for India, Iran, Portugal, and the UK, respectively. These figures help us understand the differences and similarities across countries. Social representations of hearing loss in India and the UK are more solid when compared to the social representations in Iran and Portugal.
Figure 3.

Co-occurrence analysis index of qualitative categories for India (n=101).
Note: The number on the line suggests the interconnection between two categories.
Figure 4.

Co-occurrence analysis index of qualitative categories for Iran (n=100).
Note: The number on the line suggests the interconnection between two categories.
Figure 5.

Co-occurrence analysis index of qualitative categories for Portugal (n=103).
Note: The number on the line suggests the interconnection between two categories.
Figure 6.

Co-occurrence analysis index of qualitative categories for the UK (n=100).
Note: The number on the line suggests the interconnection between two categories.
The Indian social representation index presents four main nodes (Figure 3): hearing ability or disability, communication difficulties, assessment and management, and negative mental state. As “assessment and management” (one of the most frequently occurring categories) possesses a positive connotation, the Indian responses toward hearing loss were more positive than the responses toward hearing loss from other countries. This suggests that the respondents in India saw that hearing loss can be resolved through some kind of management. However, the responses were generally dispersed as more of the less frequently occurring categories were integrated.
Iran’s social representation index presents four main nodes (Figure 4): disability, hearing instruments, causes of hearing loss, and aging. The most frequently occurring categories “disability” and “hearing instruments” were linked to each other by approximately 20%. Also, the “hearing instruments” category was the only frequent category with positive connotations, whereas the other frequently occurring categories generally had negative connotations.
Portugal’s social representation index presents the two main nodes (Figure 5) of disability and communication difficulties, which were linked to each other by approximately 25%. The responses were generally dispersed with the addition of less frequently occurring categories. Also, no positive connotations were noted in any of the most frequently occurring categories.
The UK social representation index presents three main nodes (Figure 6): disability, communication difficulties, and negative mental state. The “disability” category was linked with the “communication difficulties” and “negative mental state” categories by 17% and 14%, respectively. Other categories, such as “isolation”, “hearing instruments”, “causes of hearing loss”, “alternative modes of communication”, and “sound and acoustics of the environment”, were also fairly common. Generally, the most frequently occurring categories carried more negative connotations.
Discussion
In order to deal fully with hearing loss, there is a need to approach it in a holistic way. The importance of addressing the issue from both a medical and social/behavioral angle is well documented.47 The scientific literature on hearing loss focuses overwhelmingly on the medical perspective, and rarely addresses social concerns.8,9
In audiological literature, when such aspects as attitudes to hearing loss are the subject for research, the theory of stigma is most often used.48 For example, a study on women with normal hearing regarding their perception toward hearing loss and hearing aids suggests that both of these aspects are stigmatized in this population.49 Also, another study suggests that hearing loss is stigmatized in the entertainment-television industry by depicting those with hearing loss as comical, embarrassing, lonely, and threatening to one’s work.50 Therefore, the stigmatization may be contributing to the denial of hearing loss and not using hearing aids. However, this theoretical approach has been criticized for victimization of the stigmatized person, among other reasons.51 Moreover, it has not been successful in including the behavioral dimension. In the field of psychology, prototype is another approach that has been used in obtaining an indirect measure of the attitudes of people toward various disabilities, including hearing loss.52,53 Prototype is defined as “cognitive representations of characteristics that describe a person or object and viewed prototypes about disability as components that may help form and maintain attitudes toward disability”.52 In other words, prototype is an abstract mental representation of the members of a group toward a category. In recent years, a more elaborate theoretical approach has been developed (SRT), which is popular in the area of social sciences. SRT takes into account broader social dialogues as it explores the socially constructed reality based on the common understanding of a phenomenon in any given particular social group.27 It is important to note that attitudes and stigmatization are consequences of social representation, hence social representation is a more fundamental aspect of society that influences people’s behavior. The strength of SRT is that it covers different aspects of social and environmental factors not included in ICF. This approach has not been used in any prior audiological research to this date, hence its significance. By using SRT, we have been able to disclose a broader perspective on hearing loss than by using stigma theory, and by including and comparing data from different parts of the world, we have been able to investigate cross-cultural differences in social representations of hearing loss. As this is the first time SRT has been used as a theoretical framework in relation to understanding social representation of hearing loss, there is no knowledge base to relate the current study results to previous literature. Therefore, we have to interpret the results in a tentative way. Further studies using SRT might disclose different versions of social representation on hearing loss.
As discussed earlier, each category (hearing instruments being one example) can have positive, neutral, or negative connotations depending on respondents’ perception. However, in general, hearing loss is seen as a negative phenomenon, with over 50% of negative connotations reported (Figure 1). Also, statistically significant differences among the countries were noted, with participants in India reporting more positive and less negative connotations when compared to participants from Iran, Portugal, and the UK. The positive connotations regarding hearing loss was not in the view of celebrating deafness, as many deaf people might do within the deaf culture, rather than focusing on solutions to hearing loss as a condition. For example, respondents in India think there is some solution to hearing loss (as in assessment and management), whereas in other countries the main focus was on other aspects, such as disability, communication difficulties, and negative mental state, which were generally seen as negative. This general tendency of respondents in India to focus on assessment and management of hearing loss rather than on consequences of hearing loss may have contributed to this sample having more positive aspects as when compared to other countries. In addition, the Indian population may be facing various other social consequences, which have much more negative consequences than hearing loss, and that may have led them to think about hearing loss slightly more positively when compared to other countries. It is surprising to see a relatively large proportion of positive (eg, being able to diagnose and manage hearing loss) and neutral (eg, hearing instruments) connotations about hearing loss reported from the general public, although the literature on hearing loss focuses in large part on adverse or negative consequences. Such positive and negative characterizations of disability have also been highlighted in previous research. For example, prototype research from McCaughey and Strohmer52 suggests that a sample of undergraduate students report 70% negative and 17% positive characteristics toward hearing impairment. Moreover, a recent qualitative study examined help-seeking behavior in people with hearing loss, suggesting that the balance among positive energy and negative stressors play an important role in triggering help-seeking behavior.19 Therefore, the results of this study strengthen the argument emphasizing the importance of capturing both positive and negative aspects of such disabilities as hearing loss.24 This way of thinking also has implications for audiological rehabilitation, especially during counseling sessions that encourage people with hearing loss to focus on positive aspects, which may foster better acceptance and coping.
Analysis of the categories suggests that no single category has a dominant position in terms of size, but the analysis gives a clear indication that the representation of hearing loss varies in the different countries. The study results can be the basis for further research where both content and structure of the representations are further explored.
The global index presents five main themes (Figure 2 and Table 3). “Disability” was the most common category, which was linked to other frequently occurring categories such as “communication difficulties”, “negative mental state”, “causes of hearing loss”, and “hearing instruments”. It is not surprising to find “disability” as one of the main categories. However, it is interesting to note that other categories occurring, such as “communication difficulties” and “negative mental state” have been found to be the consequences of uncorrected hearing loss.53 Disability was also linked to such aspects as aging, reduced abilities, alternative modes of communication, and dependence on other senses. These findings that demonstrate the connection between such factors as aging, disability, and communication difficulties are consistent with the disability literature, in which the studies have largely been conducted on people with disabilities.54 This may suggest that society’s general understanding, or common knowledge of the phenomenon, coincides well with the reports of people with disabilities. Another main category, “communication difficulties”, has been primarily linked to “hearing ability or disability”, “lifestyle and relationship changes”, and others’ attitudes. Again the connections between these factors have been documented well in the disability literature.55 Moreover, “causes of hearing loss” were linked to “assessment and management” as well as to “symptoms of hearing loss”. This may generally be related to the natural progression of thinking from one aspect to another. For example, those who think about the cause may generally think about the symptoms, and also about possible assessment and management of the condition. Also, “hearing instrument” responses were linked to “voice and speech functions”. This may suggest the link between hearing and speech as a feedback loop, highlighting the importance of good hearing to monitor our voice and speech functions. Overall, these co-occurrence indices provide some insight into how the people in each country conceptualize hearing loss. The current study demonstrates the complexity of views surrounding hearing loss, although there seems to be a distinct pattern emerging.
Comparing the results across countries suggests that that the social representation of the four countries varied markedly (Figures 2–6). “Hearing ability or disability”, “communication difficulties”, and “assessment and management” were the main categories occurring in India. “Hearing instruments”, “disability”, and “ageing” were the main categories occurring in Iran. Portugal and the UK had “disability” as one of the most frequent categories, but they differed in terms of Portugal having “communication difficulties” and the UK having “negative mental state” as the second-most frequently occurring categories. Although the study reveals the social representation of hearing loss in four countries, it is important to note that the study is by nature descriptive. This is due to the design of the study, which does not include the study of mechanisms behind different groups and their everyday knowledge (ie, understanding the reasons for differences and similarities in social representations) or the social structures, laws, and traditions of the different countries in relation to illness and disability. Martz et al53 explored and compared disability prototypes in the US and Russia. They reported significant differences among categories reported (ability focus, disability focus, negative emotions, and stigma) when examining two samples across the three disability categories of AIDS, hearing impairment, and spinal cord injury. These results indicate some cross-cultural differences in perception of and attitudes toward disabilities, including hearing loss. However, the limited literature in this area limits our discussion in terms of comparing and contrasting current findings with previous research.
We believe that these findings provide useful insights into the public perception of hearing loss that may prove useful in public education and counseling.
Advantages and limitations
The study involved data collection from four culturally different countries, adding significantly to our knowledge about how hearing loss is represented across different societies. Many cross-cultural studies have used psychometric scales; however, we argue that the method used in this study (free-association task) may have some advantages in collecting data neutrally on a cultural level, hence the cross-cultural comparison being more appropriate. The study also has some limitations. We aimed to collect data to represent the general population of the respective countries. However, the sample was recruited via educational institutes and also from one city. These factors, in addition to the snowball sampling method of sample recruitment, may have introduced some bias. Hence, future studies must employ the maximum-variation sampling method (in terms of age, sex, education, etc), in order to overcome the sampling bias. There was no particular method for sample-size calculation, although to produce reasonable clusters with the software used (Iramuteq), approximately 100 participants were needed. Considering this and the fact that this was an exploratory study, we feel the sample size was appropriate. The populations across four countries were age- and sex-matched. However, there were some differences in terms of educational level, profession, and family history of hearing loss. In addition, other important factors, such as ethnic group and religion, were not included in the study. Therefore, those factors may have some bearing toward the validity of the sample representations. In terms of data analysis, two authors centrally analyzing the data proved helpful in ensuring that the analysis was consistent, and that the same name was applied to categories when the meaning was the same. This also helped to compare the data across countries. However, translating the raw data before analyzing it may have compromised the richness of the data to some degree. Moreover, although the categorization was made with consensus from two of the researchers, some element of subjectivity may have existed, which could have been affected by the researchers’ preconceptions concerning the phenomenon. Furthermore, various factors (eg, age, sex, education, ethic group, etc) that may influence the social representation of hearing loss need to be explored.
Conclusion
This exploratory study reports the general public’s social representation of hearing loss in India, Iran, Portugal, and the UK. SRT appears to be a fruitful approach to investigate views on hearing loss from a broader perspective that includes biopsychosocial considerations. Five clusters of components in social representation were revealed and centered around the nodes: disability, causes of hearing loss, communication difficulties, negative mental state, and hearing instruments. Cross-cultural differences in the respondents’ social representations of hearing loss were disclosed. Although neutral and positive connotations occurred, the negative associations, most often linked to different aspects of disability, were the most frequent. Also, there were a number of positive aspects of hearing loss that had not been highlighted in the previous literature on hearing loss. In India, the proportion of negative associations was significantly lower than in the other countries; in fact, respondents in India perceived more opportunities than obstacles overall. However, due to the low sample size, these results must be viewed with caution and should be considered tentative. Further research on the formation of social representations of hearing loss in different counties, and the role of local contextual factors, is needed.
Acknowledgments
Data collection in the People’s Republic of China was partially funded by National Social Science Foundation of China (grants 15BYY071/14BYY066).
Footnotes
Disclosure
The authors report no conflicts of interest in this work.
References
- 1.World Health Organization Deafness and hearing loss. 2015. [Accessed July 1, 2014]. Available from: http://www.who.int/mediacentre/factsheets/fs300/en.
- 2.Chia EM, Wang J, Rochtchina E, Cumming RR, Newall P, Mitchell P. Hearing impairment and health-related quality of life: the Blue Mountains hearing study. Ear Hear. 2007;28(2):187–195. doi: 10.1097/AUD.0b013e31803126b6. [DOI] [PubMed] [Google Scholar]
- 3.Manchaiah VK, Stephens D, Zhao F, Kramer SE. The role of communication partners in the audiological enablement/rehabilitation of a person with hearing impairment: an overview. Audiol Med. 2012;10(1):21–30. [Google Scholar]
- 4.Davis A, Smith P, Ferguson M, Stephens D, Gianopoulos I. Acceptability, benefits and costs of early screening of hearing disability: a study of potential screening tests and models. Health Technol Assess. 2007;11(42):1–294. doi: 10.3310/hta11420. [DOI] [PubMed] [Google Scholar]
- 5.Manchaiah VK, Stephens D. Perspectives in defining ‘hearing loss’ and its consequences. Hear Balance Commun. 2013;11(1):6–16. [Google Scholar]
- 6.World Health Organization . International Classification of Functioning, Disability and Health. Geneva: WHO; 2001. [Google Scholar]
- 7.ICF Research Branch ICF Core Set for hearing loss. 2013. [Accessed October 19, 2015]. Available from: http://www.icf-research-branch.org/icf-core-sets-projects-sp-1641024398/other-health-conditions/icf-core-set-for-hearing-loss.
- 8.Granberg S, Möller K, Skagerstrand A, Möller C, Danermark B. The ICF Core Sets for hearing loss: researcher perspective, Part II: Linking outcome measures to the International Classification of Functioning, Disability and Health (ICF) Int J Audiol. 2014;53(2):77–87. doi: 10.3109/14992027.2013.858279. [DOI] [PubMed] [Google Scholar]
- 9.Granberg S, Swanepoel DW, Englund U, Möller C, Danermark B. The ICF core sets for hearing loss project: International expert survey on functioning and disability of adults with hearing loss using the International Classification of Functioning, Disability, and Health (ICF) Int J Audiol. 2014;53(8):497–506. doi: 10.3109/14992027.2014.900196. [DOI] [PubMed] [Google Scholar]
- 10.Manchaiah VK, Stephens D, Meredith R. The patient journey of adults with hearing impairment: the patients’ view. Clin Otolaryngol. 2011;36:227–234. doi: 10.1111/j.1749-4486.2011.02320.x. [DOI] [PubMed] [Google Scholar]
- 11.Manchaiah VK, Stephens D. The patient journey of adults with sudden-onset acquired hearing impairment: a pilot study. J Laryngol Otol. 2012;126(5):475–481. doi: 10.1017/S0022215111003197. [DOI] [PubMed] [Google Scholar]
- 12.Meyer C, Hickson L. What factors influence help-seeking for hearing impairment and hearing aid adoption in older adults? Int J Audiol. 2012;51(2):66–74. doi: 10.3109/14992027.2011.611178. [DOI] [PubMed] [Google Scholar]
- 13.Laplante-Lévesque A, Hickson L, Worrall L. Factors influencing rehabilitation decisions of adults with acquired hearing impairment. Int J Audiol. 2010;49:497–507. doi: 10.3109/14992021003645902. [DOI] [PubMed] [Google Scholar]
- 14.Kochkin S. MarkeTrak VII: obstacles to adult non-user adoption of hearing aids. Hear J. 2007;60(4):27–43. [Google Scholar]
- 15.Kundsen LV, Oberg M, Nielsen C, Naylor G, Kramer SE. Factors influencing help seeking, hearing aid uptake, hearing aid use and satisfaction with hearing aids: a literature review. Trends Amplif. 2010;14(3):127–154. doi: 10.1177/1084713810385712. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Jensted L, Moon J. Systematic review of barriers and facilitators to hearing aid uptake in older adults. Audiol Res. 2011;1(e25):91–96. doi: 10.4081/audiores.2011.e25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Hétu R, Jones L, Getty L. The impact of acquired hearing impairment on intimate relationships: implications for rehabilitation. Audiology. 1993;32(6):363–381. doi: 10.3109/00206099309071867. [DOI] [PubMed] [Google Scholar]
- 18.Hétu R, Getty L, Waridle S. Attitudes towards co-workers affected by occupational hearing loss. II: Focus groups interviews. Br J Audiol. 1994;28(6):313–325. doi: 10.3109/03005369409077315. [DOI] [PubMed] [Google Scholar]
- 19.Southall K, Gagné JP, Jennings MB. Stigma: negative and positive influence on help-seeking for adults with acquired hearing loss. Int J Audiol. 2010;49(11):804–814. doi: 10.3109/14992027.2010.498447. [DOI] [PubMed] [Google Scholar]
- 20.Garstecki DC, Erler SF. Hearing loss, control, and demographic factors influencing hearing aid use among older adults. J Speech Lang Hear Res. 1998;41(3):527–537. doi: 10.1044/jslhr.4103.527. [DOI] [PubMed] [Google Scholar]
- 21.Jerram JCK, Purdy S. Technology, expectations, and adjustment to hearing loss: predictors of hearing aid outcome. J Am Acad Audiol. 2001;12(2):64–79. [PubMed] [Google Scholar]
- 22.Manchaiah VK, Molander P, Rönnberg J, Andersson G, Lunner T. The acceptance of hearing disability among adults experiencing hearing difficulties: a cross-sectional study. BMJ Open. 2014;4(1):e004066. doi: 10.1136/bmjopen-2013-004066. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Manchaiah V, Baguley D, Pyykkö I, Kentala E, Levo H. Positive experiences associated with acquired hearing loss, Ménière’s disease and tinnitus: a review. Int J Audiol. 2015;54(1):1–10. doi: 10.3109/14992027.2014.953217. [DOI] [PubMed] [Google Scholar]
- 24.Manchaiah V, Möller K, Pyykkö I, Durisala N. Capturing positive experiences of a health condition such as hearing loss when using the ICF framework. Hear Balance Commun. 2015;13(3):134–136. [Google Scholar]
- 25.Moscovici S. Foreword. In: Herzlich C, editor. Health and Illness: A Social Psychological Analysis. London: Academic Press; 1973. [Google Scholar]
- 26.Moscovici S. La Psychanalyse, Son Image et Son Public. 2nd ed. Paris: PUF; 1976. [Google Scholar]
- 27.Moscovici S. Social Representations: Explorations in Social Psychology. New York: NYU Press; 2001. [Google Scholar]
- 28.Höijer B. Social representations theory. A new theory for media research. Nordicom Rev. 2011;32(2):3–16. [Google Scholar]
- 29.Buijs A, Hovardas T, Figari H, et al. Understanding people’s ideas on natural resource management: research on social representations of nature. Soc Nat Resour. 2012;25(11):1167–1181. [Google Scholar]
- 30.Danermark B, Englund U, Germundsson P, Ratinaud P. French and Swedish teachers’ social representations of social workers. Eur J Soc Work. 2013;17(4):491–507. [Google Scholar]
- 31.Linton AC, Germundsson P, Heimann M, Danermark B. Teachers’ social representation of students with Asperger diagnosis. Eur J Spec Needs Educ. 2013;28(4):392–412. [Google Scholar]
- 32.Kollmuss A, Agyeman J. Mind the gap: Why do people act environmentally and what are the barriers to pro-environmental behavior?’. Environ Educ Res. 2002;8(3):239–260. [Google Scholar]
- 33.Jodelet D. Les Représentations Sociales. Paris: PUF; 1989. Représentations sociales: un domaine en expansion. [Google Scholar]
- 34.Wagner W, Hayes N. Everyday Discourse and Common Sense: The Theory of Social Representations. London: Palgrave Macmillan; 2005. [Google Scholar]
- 35.Zhao F, Manchaiah V, St Claire L, et al. Exploring the influence of culture on hearing help-seeking and hearing aid uptake: a discussion paper. Int J Audiol. 2015;54(7):435–443. doi: 10.3109/14992027.2015.1005848. [DOI] [PubMed] [Google Scholar]
- 36.Wagner W, Valencia J, Elejabarrieta F. Relevance, discourse and the ‘hot’ stable core of social representations – a structural analysis of word associations. Br J Soc Psychol. 1996;35(3):331–351. [Google Scholar]
- 37.Abric JC. Pratiques Socials et Représentations. Paris: PUF; 1994. Méthodologie de recueil des representations sociales. [Google Scholar]
- 38.Beaton DE, Bombardier C, Guillemin F, Ferraz MB. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine. 2000;25(24):3186–3191. doi: 10.1097/00007632-200012150-00014. [DOI] [PubMed] [Google Scholar]
- 39.Manchaiah V, Danermark B, Swarnalatha Nagara V, et al. Social representation of hearing aids: cross-cultural study in India, Iran, Portugal, and the United Kingdom. Clin Interv Aging. 2015;10:1601–1615. doi: 10.2147/CIA.S86108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Graneheim UH, Lundman B. Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurs Educ Today. 2014;24(2):105–112. doi: 10.1016/j.nedt.2003.10.001. [DOI] [PubMed] [Google Scholar]
- 41.Flament C. Théories des Graphes et Structures Sociales. Paris: Gauthier-Villars; 1964. [Google Scholar]
- 42.Ratinaud P, Marchand P. Improbable search of a homogenous diversity: the debate on national identity. Languages. 2012;3(187):93–107. [Google Scholar]
- 43.Csárdi G, Nepusz T. The Igraph software package for complex network research. Interjournal Complex Syst. 2006;1695:1695–1704. [Google Scholar]
- 44.R Development Core Team The R project for statistical computing. [Accessed May 5, 2014]. Available from: http://www.R-project.org.
- 45.Lahlou S. A method to extract social representations from linguistic corpora. Jpn J Exp Soc Psychol. 1996;35(3):278–391. [Google Scholar]
- 46.Tsoukalas I. A method for studying social representations. Qual Quant. 2006;40(6):959–981. [Google Scholar]
- 47.Bhaskar R, Danermark B. Metatheory, interdisciplinarity and disability research: a critical realist perspective. Scand J Disabil Res. 2006;8(4):278–297. [Google Scholar]
- 48.Hétu R. The stigma attached to hearing impairment. Scand Audiol Suppl. 1996;43:12–24. [PubMed] [Google Scholar]
- 49.Erler SF, Garstecki DC. Hearing loss- and hearing aid-related stigma: perceptions of women with age-normal hearing. Am J Audiol. 2002;11(2):83–91. doi: 10.1044/1059-0889(2002/020). [DOI] [PubMed] [Google Scholar]
- 50.Foss KA. (De)stigmatizing the silent epidemic: representations of hearing loss in entertainment television. Health Commun. 2014;29(9):888–900. doi: 10.1080/10410236.2013.814079. [DOI] [PubMed] [Google Scholar]
- 51.Anspach RR. From stigma to identity politics: political activism among the physically disabled and former mental patients. Soc Sci Med Med Psychol Med Sociol. 1979;13A(6):765–773. doi: 10.1016/0271-7123(79)90123-8. [DOI] [PubMed] [Google Scholar]
- 52.McCaughey TJ, Strohmer DC. Prototypes as an indirect measure of attitudes toward disability groups. Rehabil Couns Bull. 2005;48(2):89–99. [Google Scholar]
- 53.Martz E, Strohmer D, Fitzgerald D, Daniel S, Arm J. Disability prototypes in the United States and the Russian Federation: an international comparison. Rehabil Couns Bull. 2009;53(1):16–26. [Google Scholar]
- 54.Monini S, Filippi C, Baldini R, Barbara M. Perceived disability from hearing and voice changes in the elderly. Geriatr Gerontol Int. 2015;15(2):147–155. doi: 10.1111/ggi.12242. [DOI] [PubMed] [Google Scholar]
- 55.Arlinger S. Negative consequences of uncorrected hearing loss – a review. Int J Audiol. 2003;42(Suppl 2):S17–S20. [PubMed] [Google Scholar]