

Abstract
Previous epidemiologic studies suggested that vitamin D deficiency may be a risk factor of obesity. However, the result is still controversial. This meta-analysis aims to provide a comprehensive summary on the association between vitamin D deficiency and obesity. We systematically searched Pubmed database, Chinese Wanfang Data Knowledge Service Platform, and Chinese National Knowledge Infrastructure (CNKI), for the literatures on the relationship between vitamin D deficiency and obesity published from 2010 to 2015. The effect sizes of overall odds ratio (OR) and 95% confidence interval (CI) were estimated using Stata 11.0. Heterogeneity was evaluated using random-effects model and forest plots. Fifteen studies were eligible for inclusion in the meta-analysis, which included 3867 subjects with obesity and 9342 health subjects. Meta-analysis results showed that the prevalence of vitamin D deficiency was difference between obesity group and control group, and the pooled OR (95% CI) was 3.43 (2.33-5.06). The prevalence of vitamin D deficiency was associated with obesity in Asians and European-American, OR (95% CI) were 3.70 (1.98-6.90) and 3.09 (1.89-5.04), respectively. No publication bias was found in our study. vitamin D deficiency may be associated with obesity, irrespective of areas.
Keywords: Vitamin D, obesity, meta-analysis
Introduction
In recent decades, the prevalence of obesity risen steeply worldwide, which has become a major global health problem [1]. Obesity is associated with the development of cardiovascular diseases, hypertension, diabetes mellitus and various cancers, which leads to higher morbidity and mortality rates, reduce the quality of life and cause social discrimination [2,3]. Obesity is also a complex chronic metabolic disease, which defined by an excessive accumulation of body fat resulting from an imbalance between energy intake and expenditure [4]. In addition, genetic [5], environmental factors [6] and eating behavior [7] play important roles in the development of obesity. There are some studies suggesting that the level of serum 25-hydroxy vitamin D is associated with obesity.
Vitamin D is a lip soluble molecule obtained through exposure to sunlight and intake of foods containing this nutrient naturally. Moreover, vitamin D is responsible for the development and maintenance of bone tissue, as well as for calcium and phosphate homeostasis via coordinate effects on the kidney [8]. Vitamin D must be hydroxylated on carbon 25, forming 25-hydroxyvitamin D [25(OH) D] in the liver, and then on carbon 1, forming 1, 25-dihydroxyvitamin D [1, 25(OH) 2D] in the kidney [9]. Therefore, Serum 25(OH) D level is the most widely accepted biomarker to estimate short-term vitamin D status [10]. The Institute of Medicine (IOM) proposed that serum 25(OH) D levels above 20 ng/mL (>50 nmol/L) are adequate. However, the Endocrinology Society considers that serum 25(OH) D levels over 30 ng/mL (≥75 nmol/L) are optima [11]. Vitamin D deficiency and insufficiency is high prevalent worldwide, which is a public health concern around the world.
Several studies have shown that vitamin D deficiency is common in children and is associated with increasing age and obesity [12], and low vitamin D levels increase the risk of obesity in women [13] . However, the impact of vitamin D deficiency on obesity susceptibility is still under debate [14]. Thus, to further investigate the potential role of vitamin D in obesity, we performed the meta-analysis to provide a basis for intervention to obesity.
Materials and methods
Literature retrieval
We requested a literature search for the relation of vitamin D deficiency and obesity, which examined in epidemiologic studies published between 2010 and 2015. An electronic search was undertaken using the Pubmed database, Chinese Wanfang Data Knowledge Service Platform, and Chinese National Knowledge Infrastructure (CNKI). The following medical subject headings (Mesh) were used: (“obesity” OR “body mass index”) AND (“vitamin D” OR “25(OH) D”) in Chinese for Chinese database and in English for Pubmed. All references of the articles selected were also searched manually to identify relevant citations.
Inclusion criteria
The included criteria for the literature were consisted of: a) the paper was published in recent 5 years; b) human subjects; c) adequate data for extracting or calculating; this information may be presented as odds or rate ratios.Exclusion criteria: a) the indicators described in the article were with fewer association or data being incomplete; b) duplicate publication of articles.
Literature screening and quality assessment in process
Two investigators independently reviewed the titles and abstracts of all articles selected in order to assess whether the studies were eligible for inclusion in the meta-analysis, and the consensus were resolved by expert assessment. The following information were recorded for each study: author, year of publication, country, type of study, age and number of participants, method of vitamin D measurement, numbers of obesity and control group with deficient vitamin D status.
Statistical analysis
Meta-analysis was performed using Stata version 11.0. The association between vitamin D deficiency and obesity was evaluated by odds ratio (OR) and 95% confidence interval (CI), heterogeneity test was performed; the random-effect model was applied if heterogeneity exist. publication bias was estimated using funnel plot graphics, Begg’s and Egger’s test.
Results
Characteristics of the eligible studies
Fifteen studies were eligible for inclusion in the meta-analysis, which included 3867 subjects with obesity and 9342 healthy subjects. Figure 1 shows flow diagram for screening studies. The main characteristics of the studies included in this review are presented in Table 1.
Figure 1.
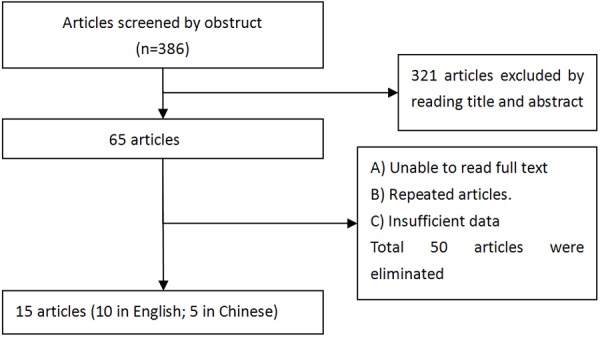
Flowchart of study selection for the association of vitamin D and obesity.
Table 1.
Main Characteristic of the Studies investigation between vitamin D deficiency and obesity
| First author | Year | Country | Design | Age rang mean (DP) | n | Method for assessing serum 25(OH) D | VitaminD deficiency (nmol/l) | obesity | control | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
|
| |||||||||||
| VitD (+) | n | VitD (+) | N | ||||||||
| Gonzalez L [21] | 2015 | Latin America | cross-sectional | 38~70 | 797 | Immunoassay | 30 | 24 | 348 | 7 | 165 |
| Stokic E [22] | 2015 | Serbia | case-control | 26~50 | 86 | Enzyme immunoassay | 50 | 44 | 50 | 11 | 36 |
| Ling Feng [23] | 2013 | China | case-control | 4~14 | 183 | ELISA | 37.5 | 52 | 78 | 11 | 105 |
| Turer CB [24] | 2013 | US | cross-sectional | 6~18 | 12292 | RIA | 50 | 645 | 1897 | 1622 | 7728 |
| Reyman M [25] | 2014 | Holland | case-control | 7~16 | 96 | ELISA | 37.5 | 36 | 64 | 5 | 32 |
| Guasch A [26] | 2012 | Spain | cross-sectional | 45~49 | 316 | Electro chemiluminescence immunoassay | 25 | 32 | 266 | 4 | 50 |
| Junshi Li [27] | 2015 | China | case-control | 5~7 | 526 | ELISA | 50 | 28 | 59 | 34 | 360 |
| Hongyuan Zhang [28] | 2014 | China | case-control | 3~6 | 70 | ELISA | 75 | 7 | 39 | 1 | 31 |
| Yulian Xiao [29] | 2012 | China | case-control | 6~12 | 447 | ELISA | 37.5 | 62 | 212 | 30 | 235 |
| Ying Wang [30] | 2011 | China | case-control | 31~68 | 224 | ELISA | 50 | 13 | 52 | 8 | 68 |
| Al-Sultan AI [31] | 2011 | Saudi Arabia | case-control | 18~25 | 160 | HPLC | 37.5 | 29 | 76 | 19 | 84 |
| Olson ML [32] | 2012 | USA | cross-sectional | 6~16 | 498 | CLIA | 50 | 205 | 411 | 19 | 87 |
| Poomthavorn P [33] | 2012 | Thailand | cross-sectional | 8~14 | 179 | HPLC | 50 | 17 | 150 | 3 | 29 |
| Elizondo-Montemayor L [34] | 2010 | Mexico | cross-sectional | 6~12 | 954 | Competitive immunoluminometric direct assay | 50 | 27 | 99 | 13 | 99 |
| Khor GL [35] | 2011 | Malaysia | cross-sectional | 7~12 | 402 | Diaspora Liason | 50 nmol/l | 60 | 66 | 194 | 233 |
ELISA, enzyme-linked immunosorbent assay; RIA, radioimmunoassay; HPLC, high performance liquid chromatography; CLIA, chemiluminescent immunoassay.
Meta-analysis
Heterogeneity was found in our study (X2=4.51, P=0.000, I2=81.2%). Thus, the random-effects model was used for meta-analysis, and the results showed a pooled OR (95% CI) for the association between vitamin D deficiency and obesity was 3.43 (2.33-5.06), as is shown by the forest plots (Figure 2). The prevalence of vitamin D deficiency was associated with obesity in Asians and European-American, OR (95% CI) were 3.70 (1.98-6.90) and 3.09 (1.89-5.04), respectively (Figures 3, 4).
Figure 2.
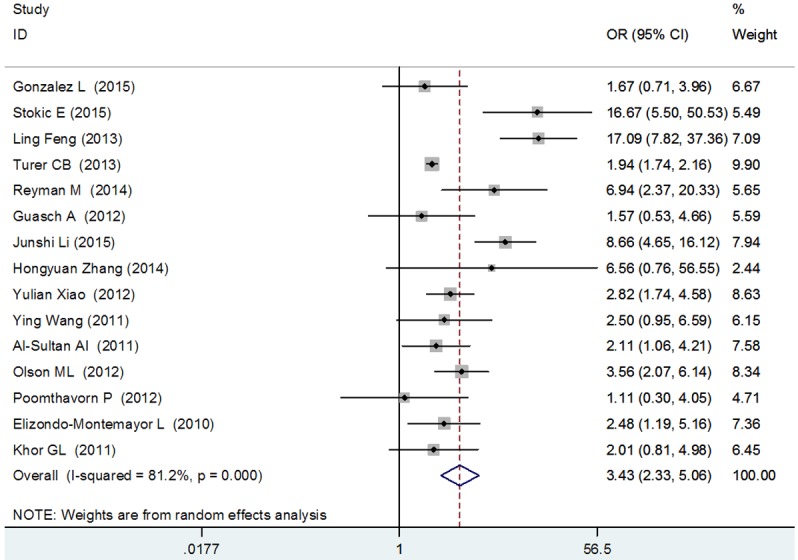
Forest plot for association between vitamin D deficiency and obesity.
Figure 3.
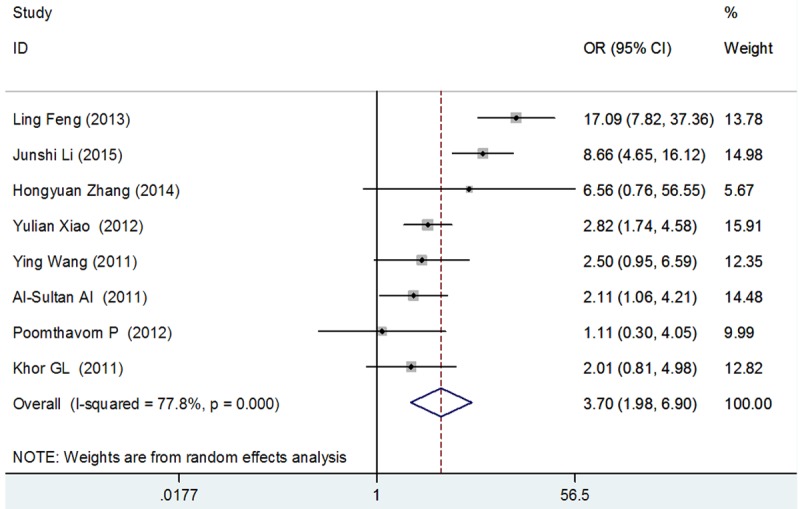
Forest plot for association between vitamin D deficiency and obesity in Asians.
Figure 4.
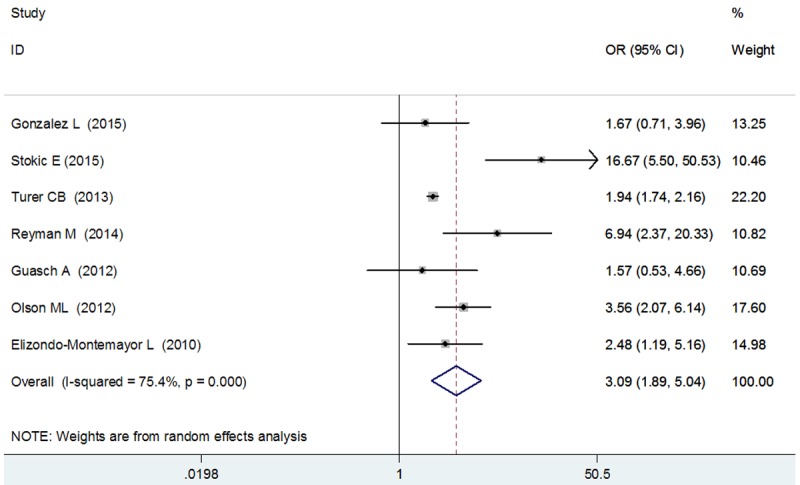
Forest plot for association between vitamin D deficiency and obesity in European-American.
Publication bias
Begg’s and Egger’s test was used to evaluate publication bias with the funnel plot. A little publication bias was identified according to the funnel plot (Figure 5) and Egger’s test (P=0.031). We performed a sensitivity analysis by excluding this study from our analysis, and the pooled estimate of OR did not change drastically (Figure 6).
Figure 5.
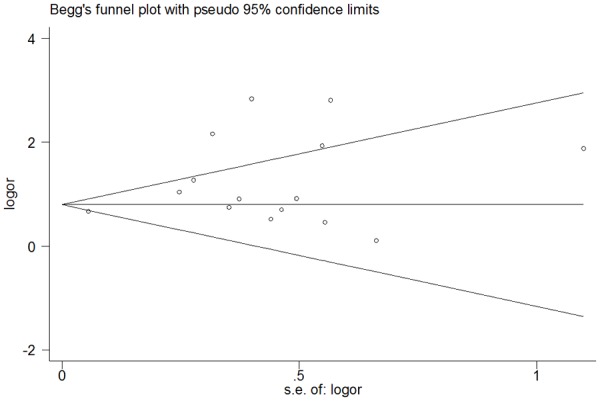
Funnel plot for association between vitamin D deficiency and obesity.
Figure 6.
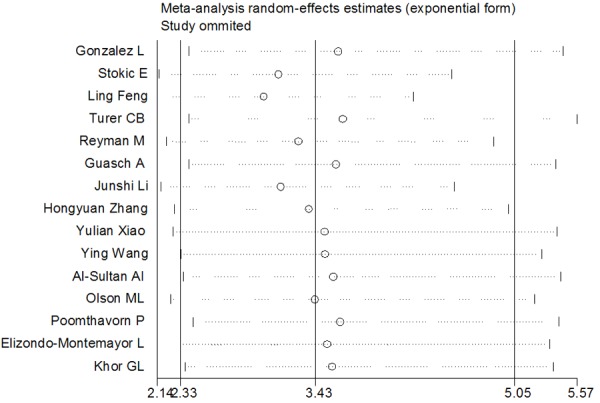
Sensitivity analyses for association between vitamin D deficiency and obesity.
Discussion
Obesity is caused by combined effect of many factors. Although the diet, gene or other life styles are thought to play an important role in the development of obesity, the role of vitamin can’t be ignored. It is a subject of controversy whether the vitamin D deficiency is a consequence of or a factor predisposing to obesity. Therefore, to further investigate if vitamin D deficiency is associated with changes in BMI, we conducted a meta-analysis from different populations. The results of present meta-analysis were based on 15 articles, which indicated that the prevalence of vitamin D deficiency was associated with obesity and the pooled OR (95% CI was 3.43 (2.33-5.06). The results from meta-analysis indicated that obese subjects in different subgroups have higher prevalence of vitamin D deficiency.
However, the mechanisms that link excess body weight and vitamin D are not fully elucidated. The possible explanation maybe that certain vitamin D receptor (VDR) polymorphisms are associated with obesity, expression of human VDR in mature mice adiposities lead to expression of VDR in preadipocyte cell lines, thereby inhibited adiposity differentiation and increased adipose mass [15]. Alternatively, some experimental data have suggested that vitamin D deficiency can cause greater adiposity by promoting parathyroid hormone levels and overflow of calcium into adipocytes, thereby increasing lipogenesis [16]. On the other hand , leptin plays a very important role in the occurrence and development of obesity, and vitamin D is a essential factor of generating this leptin, which can cause obstacles of leptin synthesis. Thus, depletion of vitamin D can increase appetite and lead to obesity [17]. Additionally, outdoor activity, food intake and exercise levels can influence 25(OH) D levels [18].
A recent meta-analysis study reported the vitamin D deficiency was associated with obesity irrespective of age, latitude, cut-offs to define vitamin D deficiency and the Human Development Index of the study location [19]. However, Saneei P [20] et al. included 34 studies in the meta-analysis, and their results support a significant inverse weak correlation between serum 25(OH) D levels and BMI in adult population. Our study showed that there are now consistent evidences of an association between the vitamin D deficiency and high risk of obesity incidence, irrespective of areas. These results suggest taking some proper measures to control obesity.
Limitations
Nonetheless, the current study had some limitations. We had limited data on physical activity and sedentary lifestyles, and these may be indirect measures of sunshine exposure. Finally, it must be kept in mind that several confounding factors have not been taken into account in this meta-analysis.
Conclusion
In conclusion, our results indicate positive association between vitamin D deficiency and obesity was found. The concept of maintaining an increased vitamin D status for decreasing adiposity also warrants further evaluation.
Acknowledgements
This research was supported by the National Natural Science Foundation of China (81072367), the Anhui Provincial Natural Science Foundation (1308085MH135), National Training Programs of Innovation and Entrepreneurship for Undergraduates (201510368035), Provincial Natural Science Research Project of Anhui Colleges (KJ2014A265), and Wannan Medical key scientific research projects Engagement Fund (WK2014Z05).
Disclosure of conflict of interest
None.
References
- 1.Ng M, Fleming T, Robinson M, Thomson B, Graetz N, Margono C, Mullany EC, Biryukov S, Abbafati C, Abera SF, Abraham JP, Abu-Rmeileh NM, Achoki T, AlBuhairan FS, Alemu ZA, Alfonso R, Ali MK, Ali R, Guzman NA, Ammar W, Anwari P, Banerjee A, Barquera S, Basu S, Bennett DA, Bhutta Z, Blore J, Cabral N, Nonato IC, Chang JC, Chowdhury R, Courville KJ, Criqui MH, Cundiff DK, Dabhadkar KC, Dandona L, Davis A, Dayama A, Dharmaratne SD, Ding EL, Durrani AM, Esteghamati A, Farzadfar F, Fay DF, Feigin VL, Flaxman A, Forouzanfar MH, Goto A, Green MA, Gupta R, Hafezi-Nejad N, Hankey GJ, Harewood HC, Havmoeller R, Hay S, Hernandez L, Husseini A, Idrisov BT, Ikeda N, Islami F, Jahangir E, Jassal SK, Jee SH, Jeffreys M, Jonas JB, Kabagambe EK, Khalifa SE, Kengne AP, Khader YS, Khang YH, Kim D, Kimokoti RW, Kinge JM, Kokubo Y, Kosen S, Kwan G, Lai T, Leinsalu M, Li Y, Liang X, Liu S, Logroscino G, Lotufo PA, Lu Y, Ma J, Mainoo NK, Mensah GA, Merriman TR, Mokdad AH, Moschandreas J, Naghavi M, Naheed A, Nand D, Narayan KM, Nelson EL, Neuhouser ML, Nisar MI, Ohkubo T, Oti SO, Pedroza A, Prabhakaran D, Roy N, Sampson U, Seo H, Sepanlou SG, Shibuya K, Shiri R, Shiue I, Singh GM, Singh JA, Skirbekk V, Stapelberg NJ, Sturua L, Sykes BL, Tobias M, Tran BX, Trasande L, Toyoshima H, van de Vijver S, Vasankari TJ, Veerman JL, Velasquez-Melendez G, Vlassov VV, Vollset SE, Vos T, Wang C, Wang X, Weiderpass E, Werdecker A, Wright JL, Yang YC, Yatsuya H, Yoon J, Yoon SJ, Zhao Y, Zhou M, Zhu S, Lopez AD, Murray CJ, Gakidou E. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2014;384:766–781. doi: 10.1016/S0140-6736(14)60460-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Mitchell NS, Catenacci VA, Wyatt HR, Hill JO. Obesity: overview of an epidemic. Psychiatr Clin North Am. 2011;34:717–732. doi: 10.1016/j.psc.2011.08.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Lavie CJ, McAuley PA, Church TS, Milani RV, Blair SN. Obesity and cardiovascular diseases: implications regarding fitness, fatness, and severity in the obesity paradox. J Am Coll Cardiol. 2014;63:1345–1354. doi: 10.1016/j.jacc.2014.01.022. [DOI] [PubMed] [Google Scholar]
- 4.El-Sayed Moustafa JS, Froguel P. From obesity genetics to the future of personalized obesity therapy. Nat Rev Endocrinol. 2013;9:402–413. doi: 10.1038/nrendo.2013.57. [DOI] [PubMed] [Google Scholar]
- 5.Nan C, Guo B, Warner C, Fowler T, Barrett T, Boomsma D, Nelson T, Whitfield K, Beunen G, Thomis M, Maes HH, Derom C, Ordonana J, Deeks J, Zeegers M. Heritability of body mass index in pre-adolescence, young adulthood and late adulthood. Eur J Epidemiol. 2012;27:247–253. doi: 10.1007/s10654-012-9678-6. [DOI] [PubMed] [Google Scholar]
- 6.Velasquez-Melendez G, Mendes LL, Padez CM. Built environment and social environment: associations with overweight and obesity in a sample of Brazilian adults. Cad Saude Publica. 2013;29:1988–1996. doi: 10.1590/0102-311x00078112. [DOI] [PubMed] [Google Scholar]
- 7.Lazarevich I, Irigoyen-Camacho ME, Velazquez-Alva Mdel C. Obesity, eating behaviour and mental health among university students in Mexico City. Nutr Hosp. 2013;28:1892–1899. [PubMed] [Google Scholar]
- 8.Turner AG, Anderson PH, Morris HA. Vitamin D and bone health. Scand J Clin Lab Invest Suppl. 2012;243:65–72. doi: 10.3109/00365513.2012.681963. [DOI] [PubMed] [Google Scholar]
- 9.St-Arnaud R, Glorieux FH. 24,25-Dihydroxyvitamin D--active metabolite or inactive catabolite? Endocrinology. 1998;139:3371–3374. doi: 10.1210/endo.139.8.6185. [DOI] [PubMed] [Google Scholar]
- 10.Afzal S, Brondum-Jacobsen P, Bojesen SE, Nordestgaard BG. Vitamin D concentration, obesity, and risk of diabetes: a mendelian randomisation study. Lancet Diabetes Endocrinol. 2014;2:298–306. doi: 10.1016/S2213-8587(13)70200-6. [DOI] [PubMed] [Google Scholar]
- 11.Holick MF, Binkley NC, Bischoff-Ferrari HA, Gordon CM, Hanley DA, Heaney RP, Murad MH, Weaver CM, Endocrine S. Evaluation, treatment, and prevention of vitamin D deficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2011;96:1911–1930. doi: 10.1210/jc.2011-0385. [DOI] [PubMed] [Google Scholar]
- 12.Robinson C, Chiang M, Thompson SN, Sondike SB. Occurrence of vitamin D deficiency in pediatric patients at high risk in West Virginia. South Med J. 2012;105:504–507. doi: 10.1097/SMJ.0b013e3182675e8a. [DOI] [PubMed] [Google Scholar]
- 13.Gonzalez-Molero I, Rojo-Martinez G, Morcillo S, Gutierrez C, Rubio E, Perez-Valero V, Esteva I, Ruiz de Adana MS, Almaraz MC, Colomo N, Olveira G, Soriguer F. Hypovitaminosis D and incidence of obesity: a prospective study. Eur J Clin Nutr. 2013;67:680–682. doi: 10.1038/ejcn.2013.48. [DOI] [PubMed] [Google Scholar]
- 14.Creo AL, Rosen JS, Ariza AJ, Hidaka KM, Binns HJ. Vitamin D levels, insulin resistance, and cardiovascular risks in very young obese children. J Pediatr Endocrinol Metab. 2013;26:97–104. doi: 10.1515/jpem-2012-0244. [DOI] [PubMed] [Google Scholar]
- 15.Wong KE, Kong J, Zhang W, Szeto FL, Ye H, Deb DK, Brady MJ, Li YC. Targeted expression of human vitamin D receptor in adipocytes decreases energy expenditure and induces obesity in mice. J Biol Chem. 2011;286:33804–33810. doi: 10.1074/jbc.M111.257568. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Hjelmesaeth J, Hofso D, Aasheim ET, Jenssen T, Moan J, Hager H, Roislien J, Bollerslev J. Parathyroid hormone, but not vitamin D, is associated with the metabolic syndrome in morbidly obese women and men: a cross-sectional study. Cardiovasc Diabetol. 2009;8:7. doi: 10.1186/1475-2840-8-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Kremer R, Campbell PP, Reinhardt T, Gilsanz V. Vitamin D status and its relationship to body fat, final height, and peak bone mass in young women. J Clin Endocrinol Metab. 2009;94:67–73. doi: 10.1210/jc.2008-1575. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Kumar J, Muntner P, Kaskel FJ, Hailpern SM, Melamed ML. Prevalence and associations of 25-hydroxyvitamin D deficiency in US children: NHANES 2001-2004. Pediatrics. 2009;124:e362–370. doi: 10.1542/peds.2009-0051. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Pereira-Santos M, Costa PR, Assis AM, Santos CA, Santos DB. Obesity and vitamin D deficiency: a systematic review and meta-analysis. Obes Rev. 2015;16:341–349. doi: 10.1111/obr.12239. [DOI] [PubMed] [Google Scholar]
- 20.Saneei P, Salehi-Abargouei A, Esmaillzadeh A. Serum 25-hydroxy vitamin D levels in relation to body mass index: a systematic review and meta-analysis. Obes Rev. 2013;14:393–404. doi: 10.1111/obr.12016. [DOI] [PubMed] [Google Scholar]
- 21.Gonzalez L, Ramos-Trautmann G, Diaz-Luquis GM, Perez CM, Palacios C. Vitamin D status is inversely associated with obesity in a clinicbased sample in Puerto Rico. Nutr Res. 2015;35:287–293. doi: 10.1016/j.nutres.2015.02.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Stokic E, Kupusinac A, Tomic-Naglic D, Zavisic BK, Mitrovic M, Smiljenic D, Soskic S, Isenovic E. Obesity and vitamin D deficiency: trends to promote a more proatherogenic cardiometabolic risk profile. Angiology. 2015;66:237–243. doi: 10.1177/0003319714528569. [DOI] [PubMed] [Google Scholar]
- 23.Ling F, Jinrong L, Fan Y. Relationship of serum 25-hydroxyvitamin D with obesity and inflammatory cytokines in children. Chin J Contemp Pediatr. 2013;15:875–879. [PubMed] [Google Scholar]
- 24.Turer CB, Lin H, Flores G. Prevalence of vitamin D deficiency among overweight and obese US children. Pediatrics. 2013;131:e152–161. doi: 10.1542/peds.2012-1711. [DOI] [PubMed] [Google Scholar]
- 25.Reyman M, Verrijn Stuart AA, van Summeren M, Rakhshandehroo M, Nuboer R, de Boer FK, van den Ham HJ, Kalkhoven E, Prakken B, Schipper HS. Vitamin D deficiency in childhood obesity is associated with high levels of circulating inflammatory mediators, and low insulin sensitivity. Int J Obes (Lond) 2014;38:46–52. doi: 10.1038/ijo.2013.75. [DOI] [PubMed] [Google Scholar]
- 26.Guasch A, Bullo M, Rabassa A, Bonada A, Del Castillo D, Sabench F, Salas-Salvado J. Plasma vitamin D and parathormone are associated with obesity and atherogenic dyslipidemia: a cross-sectional study. Cardiovasc Diabetol. 2012;11:149. doi: 10.1186/1475-2840-11-149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Junshi L. Relationship between 25- hydroxy vitamin D and simple obesity in children. China Prac Med. 2015;10:128–129. [Google Scholar]
- 28.Hongyuan Z, Ling Z, Cuicui M. Survey on the serum vitamin D and its affecting factors in overweight and obese children aged 3-6years from a kindergarten in Shenyang City. Pract Prev Med. 2014;21:1291–1293. [Google Scholar]
- 29.Yulian X, Ping D, Meizhen T. Simple obesity effect detection and intervention of children’s serum vitamin D level was observed. Journal of Guandong Medical College. 2012;30:270–271. [Google Scholar]
- 30.Ying W, Li Y, Guangli L. The relationship between serum vitamin D level and obesity. China J Endocrinol Metab. 2011;27:589–590. [Google Scholar]
- 31.Al-Sultan AI, Amin TT, Abou-Seif MA, Al Naboli MR. Vitamin D, parathyroid hormone levels and insulin sensitivity among obese young adult Saudis. Eur Rev Med Pharmacol Sci. 2011;15:135–147. [PubMed] [Google Scholar]
- 32.Olson ML, Maalouf NM, Oden JD, White PC, Hutchison MR. Vitamin D deficiency in obese children and its relationship to glucose homeostasis. J Clin Endocrinol Metab. 2012;97:279–285. doi: 10.1210/jc.2011-1507. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Poomthavorn P, Saowan S, Mahachoklertwattana P, Chailurkit L, Khlairit P. Vitamin D status and glucose homeostasis in obese children and adolescents living in the tropics. Int J Obes (Lond) 2012;36:491–495. doi: 10.1038/ijo.2011.260. [DOI] [PubMed] [Google Scholar]
- 34.Elizondo-Montemayor L, Ugalde-Casas PA, Serrano-Gonzalez M, Cuello-Garcia CA, Borbolla-Escoboza JR. Serum 25-hydroxyvitamin d concentration, life factors and obesity in Mexican children. Obesity (Silver Spring) 2010;18:1805–1811. doi: 10.1038/oby.2009.448. [DOI] [PubMed] [Google Scholar]
- 35.Khor GL, Chee WS, Shariff ZM, Poh BK, Arumugam M, Rahman JA, Theobald HE. High prevalence of vitamin D insufficiency and its association with BMI-for-age among primary school children in Kuala Lumpur, Malaysia. BMC Public Health. 2011;11:95. doi: 10.1186/1471-2458-11-95. [DOI] [PMC free article] [PubMed] [Google Scholar]