

Abstract
Objective: To evaluate a new method to plan the incisions of thoracic surgical operation with robot using three-dimensional (3D) reconstruction techniques. Methods: Three-dimensional reconstruction techniques were used to reconstruct the chest CT of patients with the software OSIRIX (APPLE®). Tumor location, size and relationship with the vein and artery were unambiguously obtained. The location of the incision was predetermined prior to the surgery. The operation time, set up time and work time were evaluated to assess the efficacy of this preplanning methodology. Results: A total of 4 cases are reported here. Tumors of different homogeneities were assessed, located in a 3D mode, and preplanned incisions successfully made to perform the procedure. This resulted in overall reduction of operation time and also provided effective visualization of the tumor during surgery. Conclusion: Our results suggest that this method can show the location of tumor, help in planning of appropriate incisions and define 3D anatomical relationships.
Keywords: Three dimensional reconstruction, surgical operation with robot, Da Vinci, minimal invasive surgery, thoracic surgery
Introduction
Philipe Mouret, a French doctor introduced TV laparoscopic cholecystectomy and ushered in a new era of minimally invasive surgery. With the advent of more convenient endoscopic instruments, endoscopic surgery has gradually unfolded in other surgical fields, such as gynecology, hepatobiliary surgery, orthopedics, ENT, Head and Neck Surgery, and Thoracic Surgery. Thoracoscopic surgery (Video-Assisted Thoracoscopic Surgery; VATS) began to develop in the 1990s. VATS has been used to obtain mediastinum biopsy, perform lobectomy [1], pleural tumor removal, thymoma resection, etc. The first totally robotic cholecystectomy was completed in March 1997 at St Pierre Hospital in Brussels, Belgium. Especially, Intuitive Surgical® Da Vinci surgical robot was successfully developed and obtained FDA approval. General surgery (gastrointestinal [2] surgical mainly), cardiac surgery, urology [3] were early to implement this revolutionary technique. As of September 2011, in China, more than 2000 cases have been performed, mainly in cardiac surgery, urology, general surgery (hepatobiliary and gastrointestinal), obstetrics and gynecology [4], and thoracic surgery [5-8]. Though randomly utilized, it seems that the overall use of robotic surgery in thoracic procedures have been limited [9].
Three-dimensional reconstruction techniques have been developed in recent years (Three-dimensional Reconstruction, 3D) as part of computer-assisted surgery in clinical applications [10,11]. Clear objective information that shows the location of the tumor and surrounding organs have been obtained using these reconstruction techniques. These have played a very important role in performing complex surgical procedures, to choose the best surgical approach, to reduce surgical injury, and to enhance tumor localization accuracy.
Post-processing of the radiographic image requires corresponding software, OsiriX software (developed by Apple), support, which uses medical image processing software for the Mac operating system. In this study, we explored whether the CT DICOM source image may be post-processed by OsiriX to obtain 3D view of intrathoracic tumor and whether surgical incisions may be planned preoperatively to optimally aid in planning surgery and performing the same with minimal injury. In order to optimally approach the tumor site, it is pertinent to have accurate idea about the surgical fields. This is only possible by planning appropriately placed surgical incisions. We determined whether OsiriX could help us with planning the surgical incisions and help prevent conversion of a minimally invasive procedure into open thoracotomy.
Materials and methods
Ethics
The study was approved by the Instituitional Review Board at the PLA General Hospital of China. All the patients enrolled in the current study gave signed informed consent before being enrolled in the current study.
Materials
The software equipment was as follows
GE 64 rows resolution CT, Apple Mac OS X operating system, the Mac OS platform OSIRIX medical image processing software, and Photoshop CS3 image-processing software.
Methods
Image data acquisition for 64 slice CT
Underwent chest 64 rows of high-resolution CT (plain or enhanced) check. Scan range: From the thoracic inlet to the diaphragmatic level. Scan parameters: Tube voltage 120 KV; to effectively current 100-150 mAs; slice thickness 5 mm; pitch 1.375:1; collimator width of 1.25 mm. The image data acquisition: DICOM format image data (Figure 1).
Figure 1.

The freeware OsiriX can render a CT slice in three dimension to aid the localization of the tumor in its intrathoracic location. The tumor can be tagged, profile rotated and viewed at any desired angle.
The reconstruction process to define anatomical relations of the tumor using OsiriX (OsiriX can be freely downloaded from www.osirix-viewer.com)
DICOM files were imported to create 3D volume reconstruction. The displayed density was adjusted to reveal the lesions. The necessary measurements were made to plan the incisions. The tumor was tagged in 3D, and bony overlay accomplished by the software to go to the next level of planning incision by the robotic method.
Planning of incisions
Robotic surgery Da Vinci surgical operating system was used to plan incisions as follows.
1) On the surface to mark the tumor location (C). 2) Would be aligned with the axis of the fuselage of the tumor location, and, in its extended line, from tumor Camera incision position (A), determined not less than 10 cm of the intercostal placement Camera arm. 3) On both sides of the connection between A and C, symmetry to determine the incision positions ① ② two manipulators. Follow the principles of: ① A distance of not less than 8 cm; same ② A distance of not less than 8 cm; ① and ② distance of not less than 10 cm.
Results
Four patients-two cases with preoperative diagnosis of tumor in the right anterior mediastinal space, one under the left anterior mediastinal space, and one in the left posterior chest wall - were utilized for successful panning and removal of tumors based on the proposed model. Table 1 elaborates the patients’ profile and Table 2 provides the details of the tumor profiles and the details of the recovery times in the postoperative periods. The actual locations of the tumor in thoracic CT slices are shown in Supplementary Figure 1.
Table 1.
Clinical Profile of 4 patients in the current case series
| Patient | Gender | Age | Diagnostic Imaging (21-24) |
|---|---|---|---|
| CASE 1 | Male | 53 years old | Right anterior mediastinal space-occupying (3 cm×2 cm) |
| Thymoma | |||
| CASE 2 | Female | 41 years old | The right anterior mediastinal mass (about 3 cm in diameter) |
| Teratomas | |||
| CASE 3 | Female | 59 years old | Right anterior mediastinum abnormal lymph node (2.5 cm×1.5 cm) |
| CASE 4 | Male | 47 years old | Right after chest wall mass (4 cm×2 cm) |
| Schwannoma |
Table 2.
Incision and postoperative healing times
| Patient | Tumer size (cm) | Operation time (min) | SUT※ (min) | Bleeding (ml) | Bed time (d) |
|---|---|---|---|---|---|
| Case 1 | 3.3×2.5×1.5 | 150 | 12 | 150 | 3 |
| Case 2 | 3.5×3×2.5 | 120 | 15 | 30 | 2 |
| Case 3 | 2.3×1.5×1 | 120 | 10 | 10 | 4 |
| Case 4 | 4×2×1.5 | 90 | 8 | 30 | 1 |
SUT (set uptime) refers to the surgical incision to determine the operating system robotic arm put in place in time.
Figure 1 shows the application of the freeware OsiriX in rendering a CT slice to aid the localization of the tumor in its intrathoracic location. The tumor can then be tagged and the profile can be rotated and viewed at any angle. Figure 2 shows the detailed planning of the incisions using the Da Vinci robotic system, and the efficacy of the use of the rendered image with relation to the tumor locale.
Figure 2.
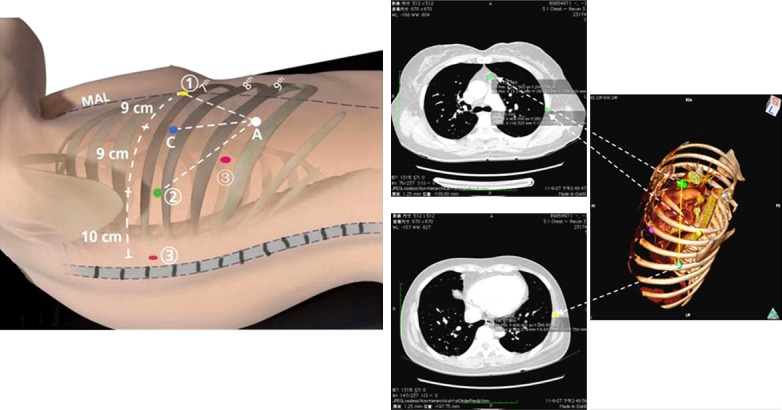
Detailed planning of the incisions using the Da Vinci robotic system, and the efficacy of the use of the rendered image with relation to the tumor locale.
Figure 3 represents a DICOM viewer showing the physical location of the tumor and tagging of the same tumor after 3D rendering. Figure 4 shows multiple views of a tumor. These rotational views enable to obtain a holistic global view of the tumor, which enormously helps to plan the incisions and the surgical approach prior to surgery. Figure 5 shows actual port placement and the right panel shows the healed incisions.
Figure 3.
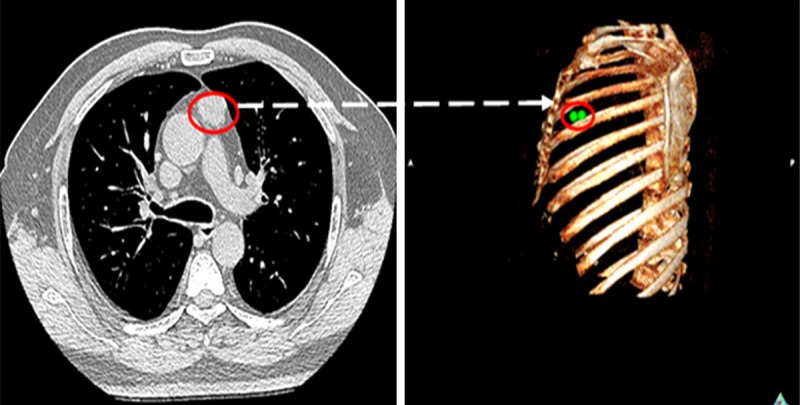
A DICOM viewer showing the physical location of the tumor and tagging of the same tumor after 3D rendering.
Figure 4.
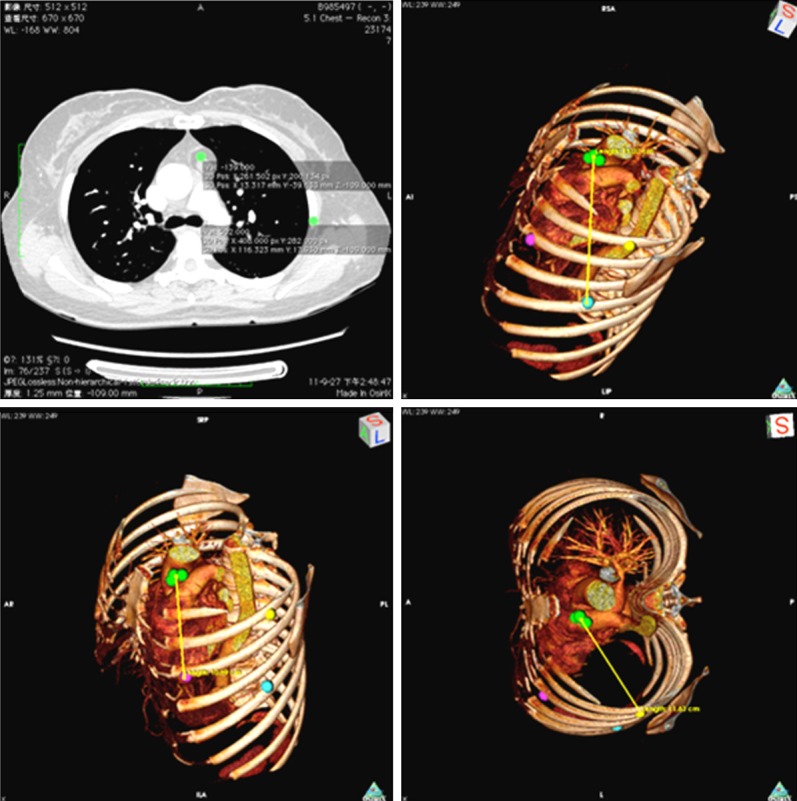
Multiple rotational views of a tumor.
Figure 5.
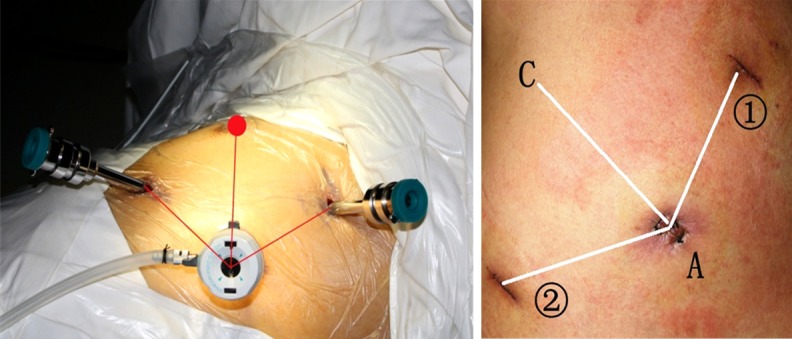
Actual port placement. The right panel shows the healed incisions.
Discussion
Robotic surgery using the Da Vinci system has revolutionized approaches to complex surgical procedures [12-14]. DICOM format file was used that contains all the data of the CT scan in continuous level and affords restoration of the most accurate details on reconstruction. Tumor density can be altered in silico to distinguish between adjacent fat. The software has a powerful tagging feature OsiriX first mark, three-dimensional reconstruction of the lesion on the CT images of the two-dimensional interface, the previous marker in the corresponding position. The OsiriX software can be freely downloaded from its official website without incurring additional cost to either the patient or the health care facility; and importantly, it provides adequate image processing functions [15-18].
The application of three-dimensional reconstruction techniques to determine the robot incision method is feasible. This method improves the surgeon’s experience in choosing the robotic surgery incision, is simple and easy to operate, and can be tested in preoperative surgical incisions to meet the set principle, to avoid increasing the difficulty of operation, in turn reducing the requirement of complete thoracotomy. Hence, we believe that this approach should be more widely applied in the clinical work space.
Disclosure of conflict of interest
None.
Abbreviations
- MIS
Minimally Invasive Surgery
- VATS
Video-Assisted Thoracoscopic Surgery
- FDA
Food and Drug Administration
- 3DR
Three-dimensional Reconstruction
- DICOM
Digital imaging and Communications in Medicine
- CT
Computed Tomography
- MRI
Magnetic resonance imaging
- PET
Positron Emission Computed Tomography
- SUT
Set Up Time
- OPT
Operation Time
- WT
Working Time
Supporting Information
References
- 1.Lewis RJ, Caccavale RJ, Sisler GE, Mackenzie JW. One hundred consecutive patients undergoing video-assisted thoracic operations. Ann Thorac Surg. 1992;54:421–6. doi: 10.1016/0003-4975(92)90431-3. [DOI] [PubMed] [Google Scholar]
- 2.Song J, Oh SJ, Kang WH, Hyung WJ, Choi SH, Noh SH. Robot-assisted gastrectomy with lymph node dissection for gastric cancer: lessons learned from an initial 100 consecutive procedures. Ann Surg. 2009;249:927–32. doi: 10.1097/01.sla.0000351688.64999.73. [DOI] [PubMed] [Google Scholar]
- 3.Patel VR, Sivaraman A, Coelho RF, Chauhan S, Palmer KJ, Orvieto MA, Camacho I, Coughlin G, Rocco B. Pentafecta: A new concept for reporting outcomes of robot-assisted laparoscopic radical prostatectomy. Eur Urol. 2011;59:702–7. doi: 10.1016/j.eururo.2011.01.032. [DOI] [PubMed] [Google Scholar]
- 4.Sert BM, Abeler VM. Robotic-assisted laparoscopic radical hysterectomy (Piver type III) with pelvic node dissection--case report. Eur J Gynaecol Oncol. 2006;27:531–3. [PubMed] [Google Scholar]
- 5.Park BJ, Flores RM, Rusch VW. Robotic assistance for video-assisted thoracic surgical lobectomy: Technique and initial results. J Thorac Cardiovasc Surg. 2006;131:54–9. doi: 10.1016/j.jtcvs.2005.07.031. [DOI] [PubMed] [Google Scholar]
- 6.Gharagozloo F, Margolis M, Tempesta B. Robot-assisted thoracoscopic lobectomy for early-stage lung cancer. Ann Thorac Surg. 2008;85:1880–5. doi: 10.1016/j.athoracsur.2008.02.085. [DOI] [PubMed] [Google Scholar]
- 7.Kernstine KH. Robotics in thoracic surgery. Am J Surg. 2004;188(Suppl 4A):89S–97S. doi: 10.1016/j.amjsurg.2004.08.002. [DOI] [PubMed] [Google Scholar]
- 8.D’Amico TA. Robotics in thoracic surgery: applications and outcomes. J Thorac Cardiovasc Surg. 2006;131:19–20. doi: 10.1016/j.jtcvs.2005.09.007. [DOI] [PubMed] [Google Scholar]
- 9.Veronesi G, Galetta D, Maisonneuve P, Melfi F, Schmid RA, Borri A, Vannucci F, Spaggiari L. Four-arm robotic lobectomy for the treatment of early-stage lung cancer. J Thorac Cardiovasc Surg. 2010;140:19–25. doi: 10.1016/j.jtcvs.2009.10.025. [DOI] [PubMed] [Google Scholar]
- 10.Ferretti GR, Vining DJ, Knoplioch J, Coulomb M. Tracheobronchial tree: three-dimensional spiral CT with bronchoscopic perspective. J Comput Assist Tomogr. 1996;20:777–781. doi: 10.1097/00004728-199609000-00018. [DOI] [PubMed] [Google Scholar]
- 11.Takahashi M, Ashtari M, Papp Z, Patel M, Goldstein J, Maguire WM, Eacobacci T, Khan A, Herman PG. CT angiography of carotid bifurcation: artifacts and pitfalls in shaded-surface display. AJR Am J Roentgenol. 1997;168:813–7. doi: 10.2214/ajr.168.3.9057540. [DOI] [PubMed] [Google Scholar]
- 12.Cadiere GB, Himpens J, Germay O, Izizaw R, Degueldre M, Vandromme J, Capelluto E, Bruyns J. Feasibility of robotic laparoscopic surgery: 146 cases. World J Surg. 2001;25:1467–77. doi: 10.1007/s00268-001-0132-2. [DOI] [PubMed] [Google Scholar]
- 13.Ruurda JP, Broeders IA, Simmermacher RP, Borel RIH, Van Vroonhoven TJ. Feasibility of robot-assisted laparoscopic surgery: an evaluation of 35 robot-assisted laparoscopic cholecystectomies. Surg Laparosc Endosc Percutan Tech. 2002;12:41–5. doi: 10.1097/00129689-200202000-00007. [DOI] [PubMed] [Google Scholar]
- 14.Boyd WD, Stahl KD. The Janus syndrome: a perspective on a new era of computer-enhanced robotic cardiac surgery. J Thorac Cardiovasc Surg. 2003;126:625–30. doi: 10.1016/s0022-5223(02)73573-3. [DOI] [PubMed] [Google Scholar]
- 15.Rosset A, Spadola L, Ratib O. OsiriX: an open-source software for navigating in multidimensional DICOM images. J Digit Imaging. 2004;17:205–16. doi: 10.1007/s10278-004-1014-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Rosset C, Rosset A, Ratib O. General consumer communication tools for improved image management and communiciation tools for improved image management and communication in medicine. J Digit Imaging. 2005;18:270–9. doi: 10.1007/s10278-005-6703-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Ratib O, Rosset A. Open-source software in medical imaging: Development of OsiriX. Int J CARS. 2006;1:187–96. [Google Scholar]
- 18.Braumann C, Jacobi CA, Menenakos C, Ismail M, Rueckert JC, Mueller JM. Robotic-assisted laparoscopic and thoracoscopic surgery with the da Vinci system: a 4-year experience in a single institution. Surg Laparosc Endosc Percutan Tech. 2008;18:260–6. doi: 10.1097/SLE.0b013e31816f85e5. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.