

Abstract
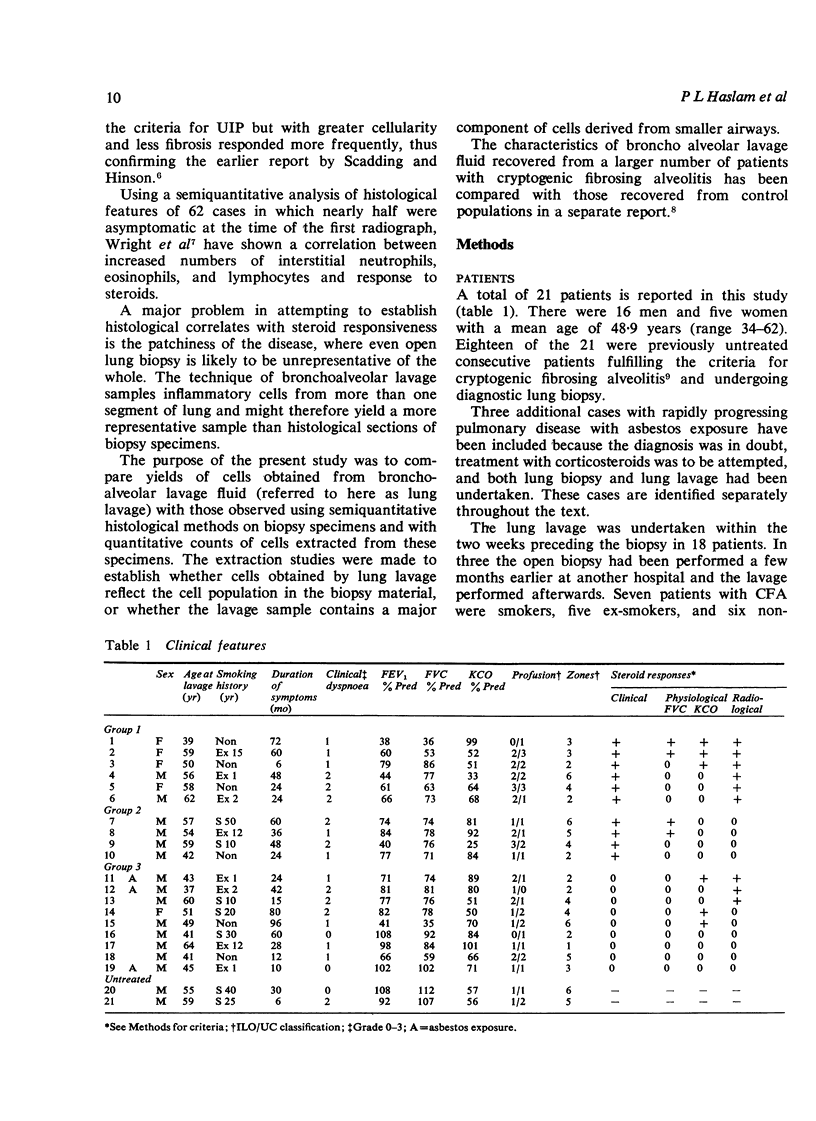
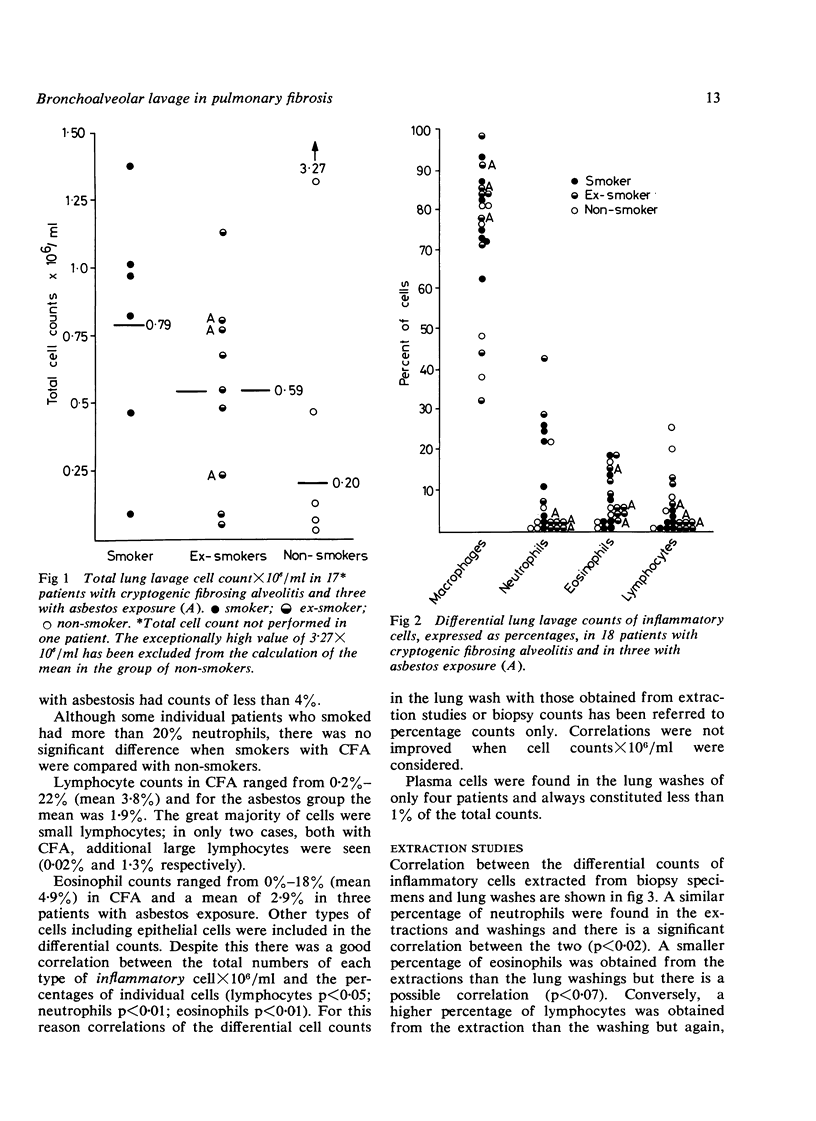
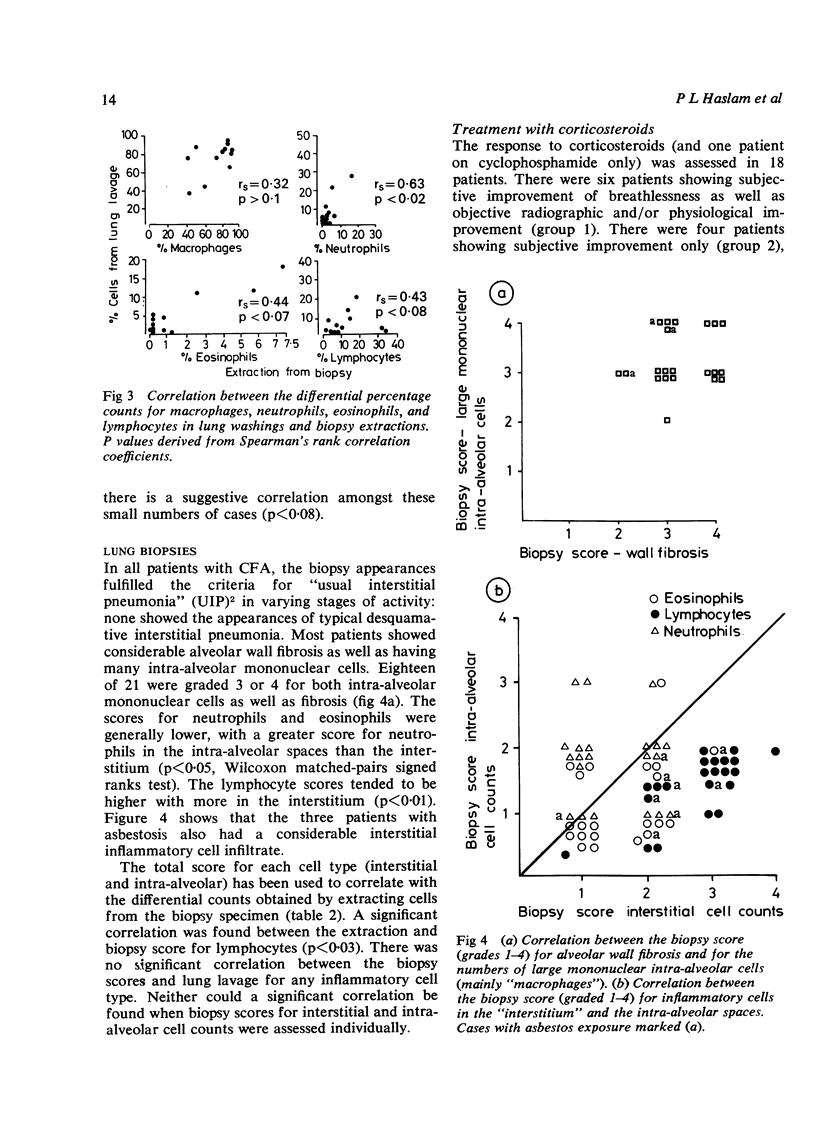
Bronchoalveolar lavage, open lung biopsy, and cell extraction from the biopsy material have been studied in 21 symptomatic patients with progressive pulmonary fibrosis (18 with cryptogenic fibrosing alveolitis, fulfilling also the criteria for “usual interstitial pneumonia” (UIP), and three with rapidly progressive disease probably related to asbestos exposure). The total and differential cell counts between the three different samples have been compared as well as the influence on them of smoking and their correlation with steroid responsiveness and later progress. There was no correlation between semiquantitative scores of cell types observed within alveolar spaces and in alveolar walls and the differential or total cell counts obtained from extraction or lung lavage samples. There was, however, some correlation between differential counts obtained from lung lavage and extractions (neutrophils p<0·02, eosinophils p<0·07, lymphocytes p<0·08) suggesting that lung lavage reflects the cellularity of the peripheral parts of the lung in patients without overt bronchial disease. Steroid responsiveness related to the percentage of lymphocytes found in extraction samples (p<0·01) and was associated with a complementary fall in the percentage of macrophages (p<0·02). There was no relationship between steroid response and the numbers of neutrophils or eosinophils in extracted samples. There was a trend towards increased numbers of lymphocytes in the lung wash in those patients responding to steroids. Those cases showing more rapid progression before starting treatment tended to have higher percentages of lymphocytes, neutrophils, or eosinophils in the lung lavage than more slowly deteriorating cases (p<0·01). Follow-up studies showed that three cases having predominant lymphocytes in the lung lavage continued to do well while nine cases with predominant neutrophils or eosinophils or both showed a less satisfactory response to steroids and often deteriorated. Differential cell counts from biopsy extractions and lung lavage may give information additional to conventional light microscopy on the likelihood of steroid responsiveness as well as providing some measure of the activity of disease.
Full text
PDF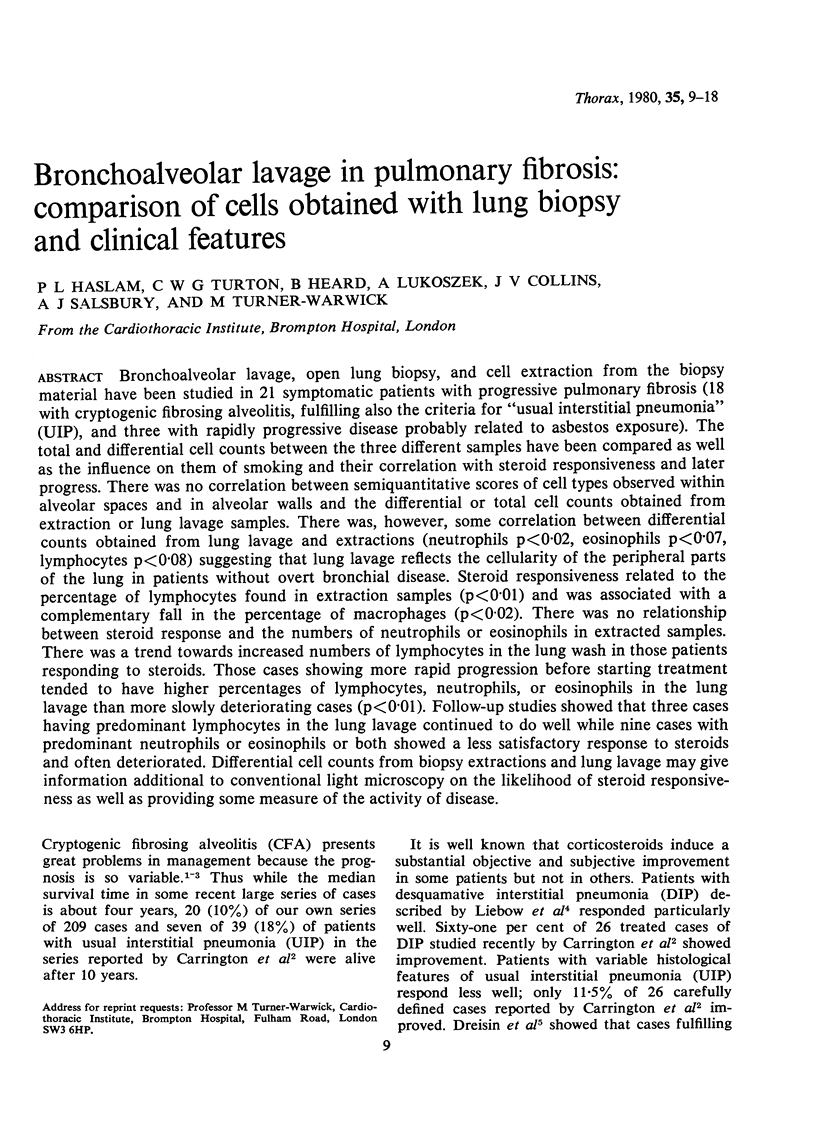





Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Carrington C. B., Gaensler E. A., Coutu R. E., FitzGerald M. X., Gupta R. G. Natural history and treated course of usual and desquamative interstitial pneumonia. N Engl J Med. 1978 Apr 13;298(15):801–809. doi: 10.1056/NEJM197804132981501. [DOI] [PubMed] [Google Scholar]
- Crystal R. G., Fulmer J. D., Roberts W. C., Moss M. L., Line B. R., Reynolds H. Y. Idiopathic pulmonary fibrosis. Clinical, histologic, radiographic, physiologic, scintigraphic, cytologic, and biochemical aspects. Ann Intern Med. 1976 Dec;85(6):769–788. doi: 10.7326/0003-4819-85-6-769. [DOI] [PubMed] [Google Scholar]
- Dreisin R. B., Schwarz M. I., Theofilopoulos A. N., Stanford R. E. Circulating immune complexes in the idiopathic interstitial pneumonias. N Engl J Med. 1978 Feb 16;298(7):353–357. doi: 10.1056/NEJM197802162980701. [DOI] [PubMed] [Google Scholar]
- LIEBOW A. A., STEER A., BILLINGSLEY J. G. DESQUAMATIVE INTERSTITIAL PNEUMONIA. Am J Med. 1965 Sep;39:369–404. doi: 10.1016/0002-9343(65)90206-8. [DOI] [PubMed] [Google Scholar]
- Ramirez J., Kieffer R. F., Jr, Ball W. C., Jr Bronchopulmonary lavage in man. Ann Intern Med. 1965 Nov;63(5):819–828. doi: 10.7326/0003-4819-63-5-819. [DOI] [PubMed] [Google Scholar]
- Scadding J. G., Hinson K. F. Diffuse fibrosing alveolitis (diffuse interstitial fibrosis of the lungs). Correlation of histology at biopsy with prognosis. Thorax. 1967 Jul;22(4):291–304. doi: 10.1136/thx.22.4.291. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stack B. H., Choo-Kang Y. F., Heard B. E. The prognosis of cryptogenic fibrosing alveolitis. Thorax. 1972 Sep;27(5):535–542. doi: 10.1136/thx.27.5.535. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Turner-Warwick M., Haslam P. Antibodies in some chronic fibrosing lung diseases. I. Non organ-specific autoantibodies. Clin Allergy. 1971 Mar;1(1):83–95. doi: 10.1111/j.1365-2222.1971.tb02450.x. [DOI] [PubMed] [Google Scholar]
- Weinberger S. E., Kelman J. A., Elson N. A., Young R. C., Jr, Reynolds H. Y., Fulmer J. D., Crystal R. G. Bronchoalveolar lavage in interstitial lung disease. Ann Intern Med. 1978 Oct;89(4):459–466. doi: 10.7326/0003-4819-89-4-459. [DOI] [PubMed] [Google Scholar]