

Abstract
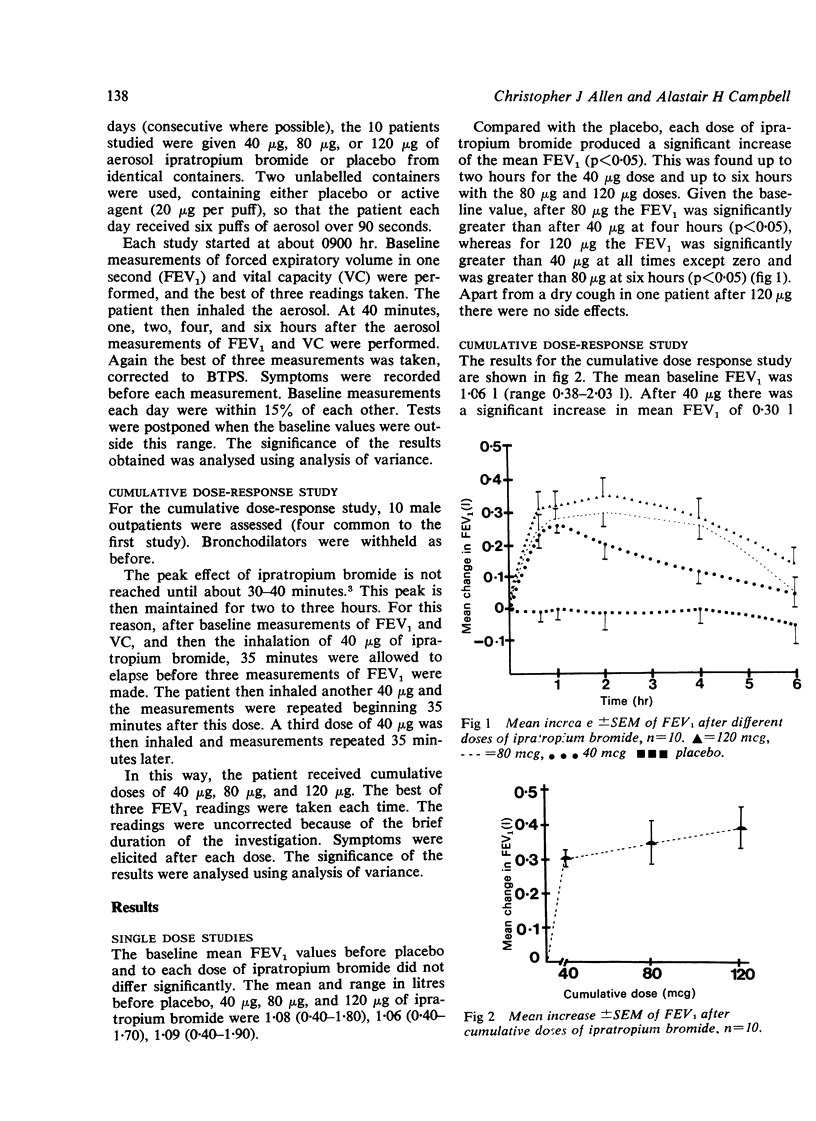
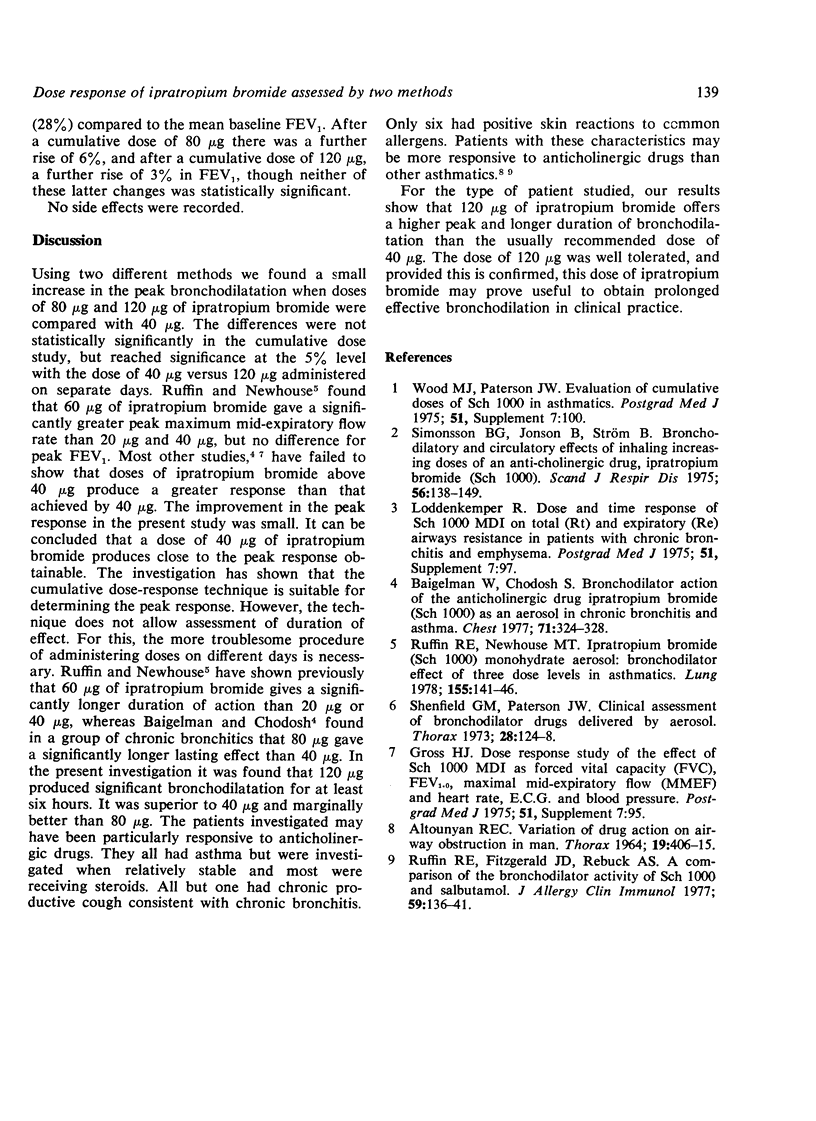
The dose-response relationships of ipratropium bromide were assessed by two different techniques in two groups of 10 male patients with partially reversible airways obstruction. In a randomised double-blind fashion on four days, 10 patients were given 40 μg, 80 μg, or 120 μg of ipratropium bromide or placebo from identical containers. Baseline FEV1 and vital capacity were measured and the measurements repeated after 40 minutes, one, two, four, and six hours, and any symptoms were elicited. In the second study, each patient received cumulative doses of 40 μg, 80 μg, and 120 μg. Baseline FEV1 was obtained and repeated 35 minutes after each dose. The peak increase of the FEV1 was comparable in both studies. The FEV1 was slightly greater after 120 μg than after 40 μg. Although this reached statistical significance only in the first study, it was concluded that the cumulative dose-response technique was suitable for determining the peak response. However, this technique was unsuitable for assessing duration of effect, which could be examined only in the first study. After 120 μg of ipratropium bromide, the FEV1 was significantly greater than after 40 μg at each time interval and it was greater than 80 μg at six hours (p<0·05). No significant side effects were noted in either study. When prolonged effective bronchodilation is sought, a dose of 120 μg of ipratropium bromide may be preferable to the recommended dose of 40 μg.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- ALTOUNYAN R. E. VARIATION OF DRUG ACTION ON AIRWAY OBSTRUCTION IN MAN. Thorax. 1964 Sep;19:406–415. doi: 10.1136/thx.19.5.406. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baigelman W., Chodosh S. Bronchodilator action of the anticholinergic drug, ipratropium bromide (Sch 1000), as an aerosol in chronic bronchitis and asthma. Chest. 1977 Mar;71(3):324–328. doi: 10.1378/chest.71.3.324. [DOI] [PubMed] [Google Scholar]
- Ruffin R. E., Fitzgerald J. D., Rebuck A. S. A comparison of the bronchodilator activity of Sch 1000 and salbutamol. J Allergy Clin Immunol. 1977 Feb;59(2):136–141. doi: 10.1016/0091-6749(77)90215-9. [DOI] [PubMed] [Google Scholar]
- Ruffin R. E., Newhouse M. T. Ipratropium bromide (Sch 1000) monohydrate aerosol: bronchodilator effect of three dose levels in asthmatics. Lung. 1978;155(2):141–146. doi: 10.1007/BF02730688. [DOI] [PubMed] [Google Scholar]
- Shenfield G. M., Paterson J. W. Clinical assessment of bronchodilator drugs delivered by aerosol. Thorax. 1973 Mar;28(2):124–128. doi: 10.1136/thx.28.2.124. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Simonsson B. G., Jonson B., Ström B. Bronchodilatory and circulatory effects of inhaling increasing doses of an anti-cholinergic drug, ipratropium bromide (SCH 1000). Scand J Respir Dis. 1975 Sep;56(3):138–149. [PubMed] [Google Scholar]