

Abstract
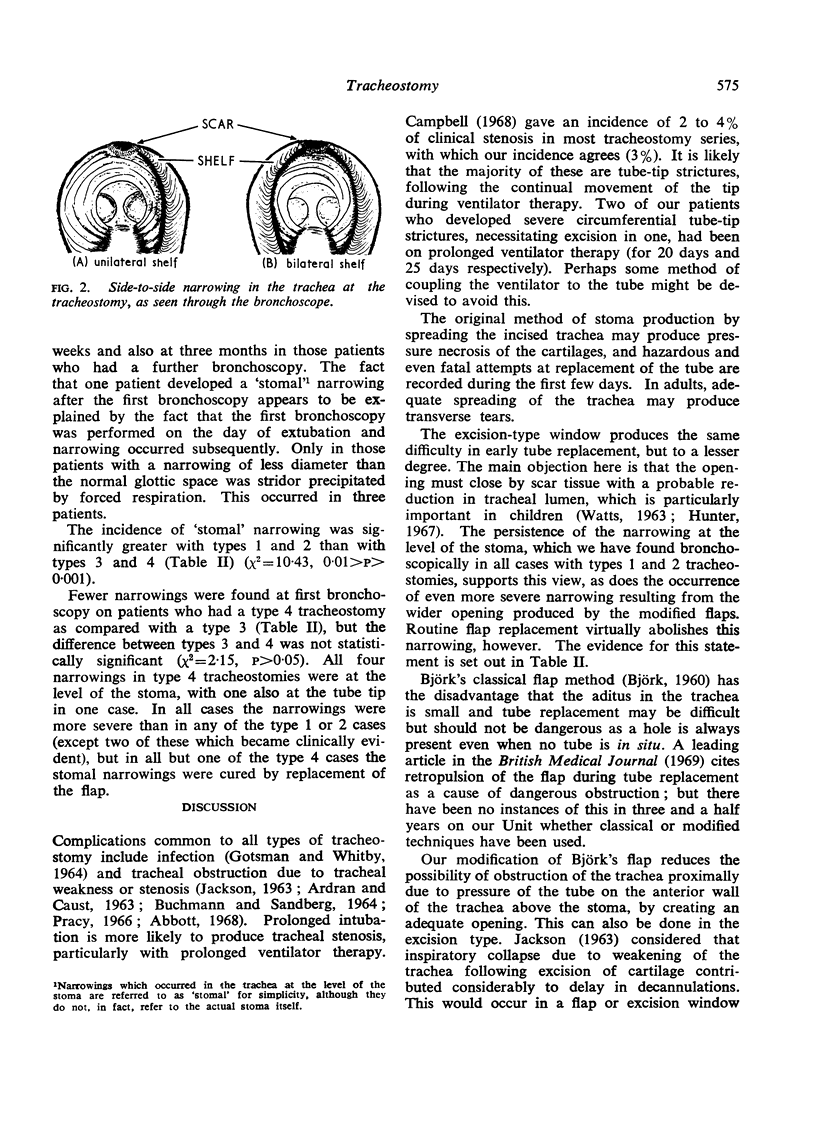
In this paper a comparison has been made between excision-type window tracheostomies and classical Björk flap and modified flap tracheostomies, based upon a review of all tracheostomies performed at Harare Hospital, Salisbury, over a 20-month period, together with bronchoscopic follow-up whenever possible.
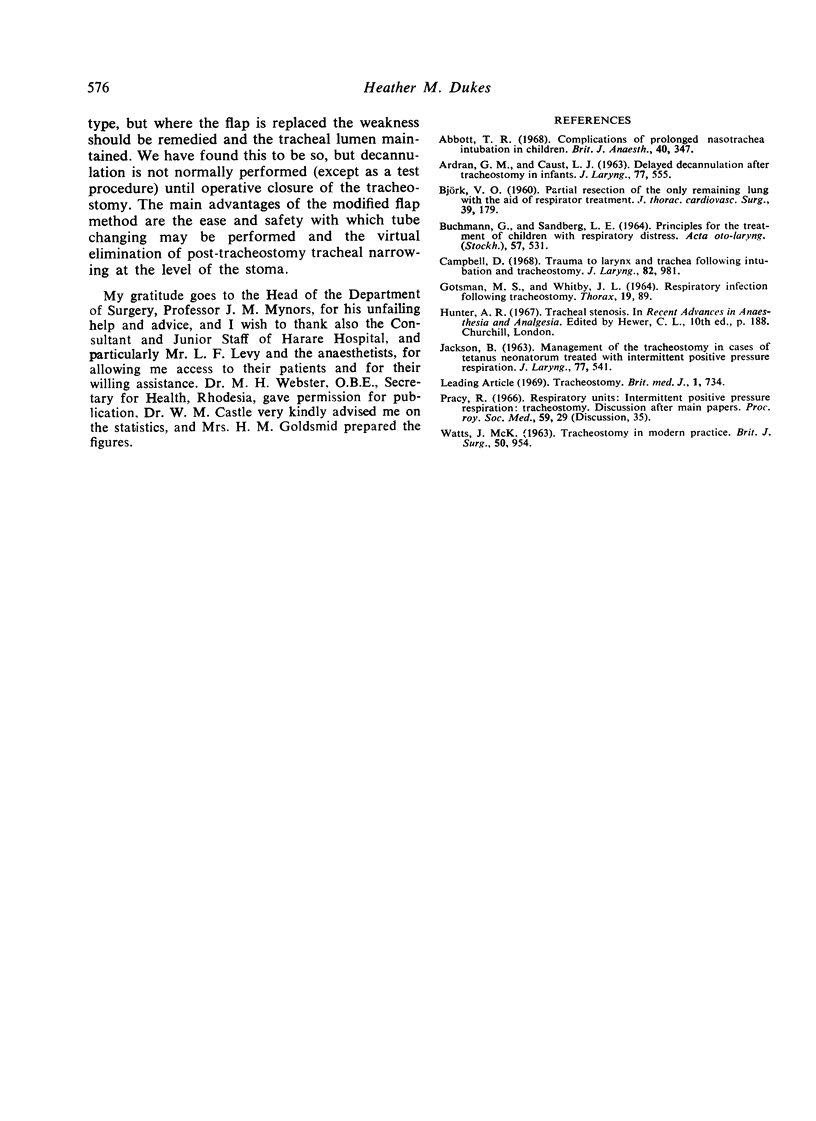
The modified flap type of tracheostomy is constructed by means of a broad-based flap dividing two tracheal rings and having rounded corners. It produces a good stoma through which tube changing can be performed with ease and safety. Any form of permanent defect in the trachea left by merely extubating a tracheostomy will almost always produce a narrowing at the level of the stoma, which is probably most severe if a flap-type of stoma has been made. Routine replacement of a modified flap will nearly always avoid this.
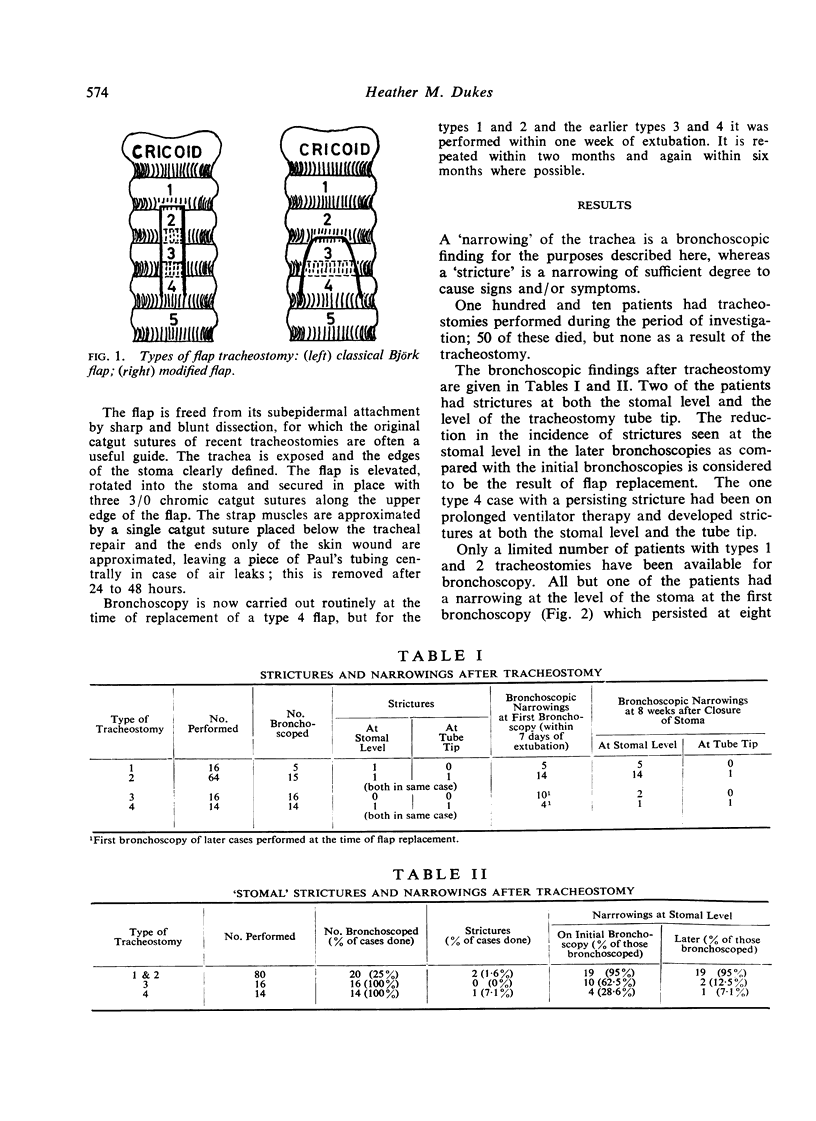
A serious stricture was produced in three (3%) patients in the series. In two, this was at the level of the tube tip in patients who had been on prolonged artificial ventilation; one required resection. These strictures are probably due to movement of the tube tip during ventilator therapy, and it is suggested that some method of coupling the ventilator to the tube might be devised to avoid this.
Full text
PDF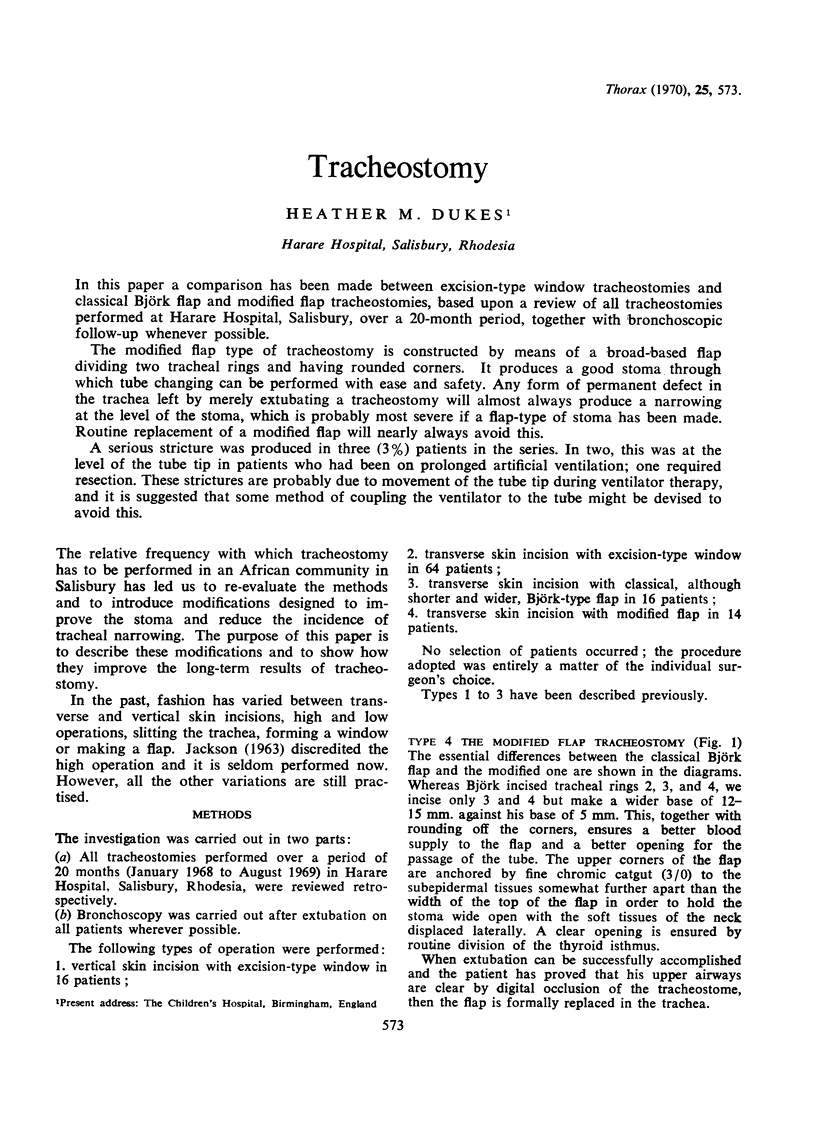
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- ARDRAN G. M., CAUST L. J. DELAYED DECANNULATION AFTER TRACHEOSTOMY IN INFANTS. J Laryngol Otol. 1963 Jul;77:555–566. doi: 10.1017/s0022215100061016. [DOI] [PubMed] [Google Scholar]
- Abbott T. R. Complications of prolonged nasotracheal intubation in children. Br J Anaesth. 1968 May;40(5):347–353. doi: 10.1093/bja/40.5.347. [DOI] [PubMed] [Google Scholar]
- BJORK V. O. Partial resection of the only remaining lung with the aid of respirator treatment. J Thorac Cardiovasc Surg. 1960 Feb;39:179–188. [PubMed] [Google Scholar]
- BUCHMANN G., SANDBERG L. E. PRINCIPLES FOR THE TREATMENT OF CHILDREN WITH RESPIRATORY DISTRESS. Acta Otolaryngol. 1964 Jun;57:531–538. doi: 10.3109/00016486409137115. [DOI] [PubMed] [Google Scholar]
- Campbell D. Trauma to larynx and trachea following intubation and tracheostomy. J Laryngol Otol. 1968 Nov;82(11):981–986. doi: 10.1017/s0022215100069759. [DOI] [PubMed] [Google Scholar]
- GOTSMAN M. S., WHITBY J. L. RESPIRATORY INFECTION FOLLOWING TRACHEOSTOMY. Thorax. 1964 Jan;19:89–96. doi: 10.1136/thx.19.1.89. [DOI] [PMC free article] [PubMed] [Google Scholar]
- JACKSON B. MANAGEMENT OF THE TRACHEOSTOMY IN CASES OF TETANUS NEONATORUM TREATED WITH INTERMITTENT POSITIVE PRESSURE RESPIRATION. J Laryngol Otol. 1963 Jul;77:541–554. doi: 10.1017/s0022215100061004. [DOI] [PubMed] [Google Scholar]
- WATTS J. M. TRACHEOSTOMY IN MODERN PRACTICE. Br J Surg. 1963 Nov;50:954–975. doi: 10.1002/bjs.18005022709. [DOI] [PubMed] [Google Scholar]