

Abstract
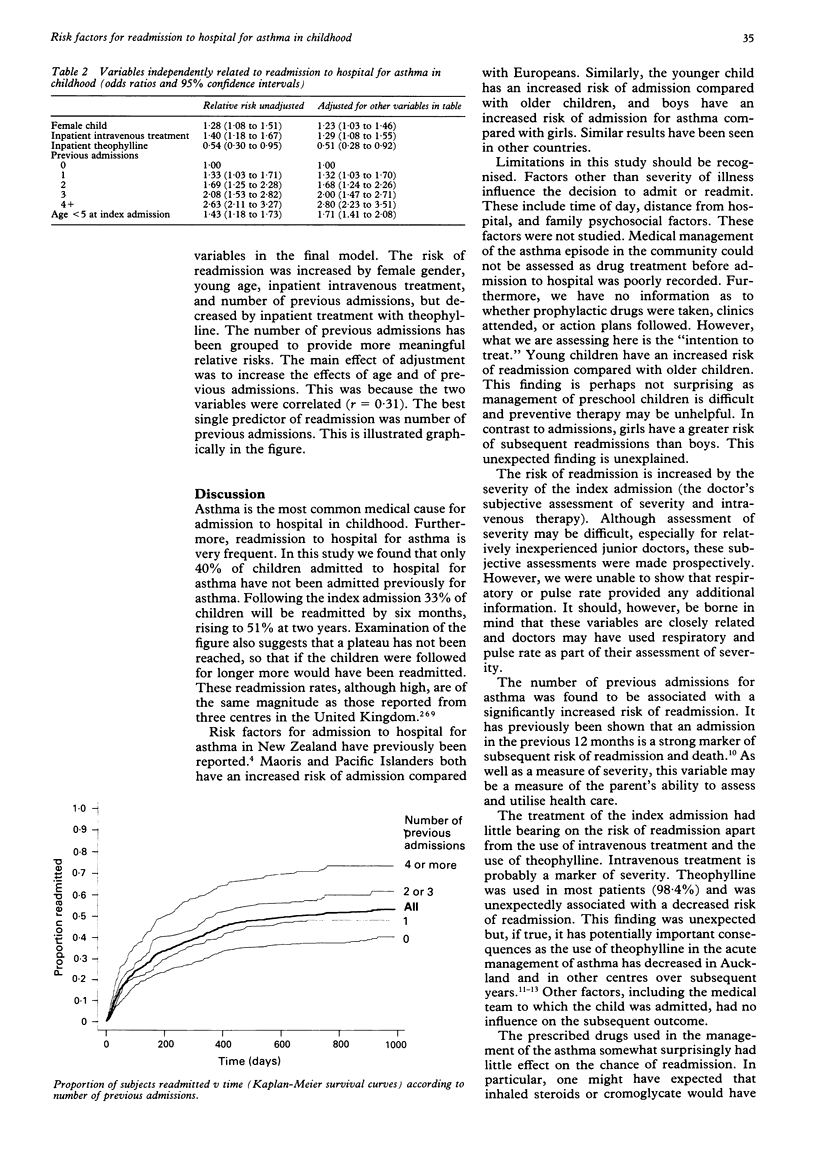
BACKGROUND--Readmissions account for part of the increase in hospital admissions for asthma in childhood seen in many countries. METHODS--This observational study recorded demographic features and the severity, treatment and management of asthma in 1034 individual children admitted to hospital over a one year period, followed for a maximum of 33 months. RESULTS--Readmissions were common, with 33% readmitted by six months and 51% by two years. After controlling for a wide range of variables, factors that significantly increased readmission were: female sex (relative risk (RR) 1.23; 95% confidence interval (CI) 1.03 to 1.46), young age (age < 5 years RR 1.71; 95% CI 1.41 to 2.08), number of previous admissions (one previous admission RR 1.32; two, RR 1.68; three, RR 2.00; four or more, RR 2.80), and inpatient intravenous treatment (RR 1.29; 95% CI 1.08 to 1.55). Inpatient treatment with theophylline was used frequently (98.4%), but was associated with decreased readmissions (RR 0.51, 95% CI 0.28 to 0.92). Factors which did not predict readmission included ethnicity, respiratory and pulse rate, medical team, prescribed prophylactic treatment, type of follow up, or the use of action plans. CONCLUSIONS--Risk factors for readmission relate to the characteristics of the individual (age and sex), severity of the condition (intravenous treatment), and number of previous admissions which may reflect severity or behaviour of the illness. Medical treatment and management did not influence readmissions. Strategies to reduce the high readmission rate for asthma in childhood need to be developed.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Anderson H. R. Increase in hospital admissions for childhood asthma: trends in referral, severity, and readmissions from 1970 to 1985 in a health region of the United Kingdom. Thorax. 1989 Aug;44(8):614–619. doi: 10.1136/thx.44.8.614. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Asthma: a follow up statement from an international paediatric asthma consensus group. Arch Dis Child. 1992 Feb;67(2):240–248. doi: 10.1136/adc.67.2.240. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Conway S. P., Littlewood J. M. Admission to hospital with asthma. Arch Dis Child. 1985 Jul;60(7):636–639. doi: 10.1136/adc.60.7.636. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Crane J., Pearce N., Burgess C., Woodman K., Robson B., Beasley R. Markers of risk of asthma death or readmission in the 12 months following a hospital admission for asthma. Int J Epidemiol. 1992 Aug;21(4):737–744. doi: 10.1093/ije/21.4.737. [DOI] [PubMed] [Google Scholar]
- Horwood L. J., Dawson K. P., Mogridge N. Admission patterns for childhood acute asthma: Christchurch 1974-89. N Z Med J. 1991 Jul 10;104(915):277–279. [PubMed] [Google Scholar]
- Mayo P. H., Richman J., Harris H. W. Results of a program to reduce admissions for adult asthma. Ann Intern Med. 1990 Jun 1;112(11):864–871. doi: 10.7326/0003-4819-112-11-864. [DOI] [PubMed] [Google Scholar]
- Mitchell E. A., Burr D. Comparison of the characteristics of children with multiple admissions to hospital for asthma with those with a single admission. N Z Med J. 1987 Dec 9;100(837):736–738. [PubMed] [Google Scholar]
- Mitchell E. A. Consensus on acute asthma management in children. Ad Hoc Paediatric Group. N Z Med J. 1992 Sep 9;105(941):353–355. [PubMed] [Google Scholar]
- Mitchell E. A., Cutler D. R. Paediatric admissions to Auckland Hospital for asthma from 1970-1980. N Z Med J. 1984 Feb 8;97(749):67–70. [PubMed] [Google Scholar]
- Mitchell E. A. International trends in hospital admission rates for asthma. Arch Dis Child. 1985 Apr;60(4):376–378. doi: 10.1136/adc.60.4.376. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mundy A. R. Artificial urinary sphincters. Arch Dis Child. 1986 Jan;61(1):1–3. doi: 10.1136/adc.61.1.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rachelefsky G. S. Review of asthma self-management programs. J Allergy Clin Immunol. 1987 Sep;80(3 Pt 2):506–511. doi: 10.1016/0091-6749(87)90087-x. [DOI] [PubMed] [Google Scholar]
- Robertson C. F., Heycock E., Bishop J., Nolan T., Olinsky A., Phelan P. D. Prevalence of asthma in Melbourne schoolchildren: changes over 26 years. BMJ. 1991 May 11;302(6785):1116–1118. doi: 10.1136/bmj.302.6785.1116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sears M. R., Taylor D. R., Print C. G., Lake D. C., Li Q. Q., Flannery E. M., Yates D. M., Lucas M. K., Herbison G. P. Regular inhaled beta-agonist treatment in bronchial asthma. Lancet. 1990 Dec 8;336(8728):1391–1396. doi: 10.1016/0140-6736(90)93098-a. [DOI] [PubMed] [Google Scholar]
- Storr J., Barrell E., Lenney W. Rising asthma admissions and self referral. Arch Dis Child. 1988 Jul;63(7):774–779. doi: 10.1136/adc.63.7.774. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vollmer W. M., Buist A. S., Osborne M. L. Twenty year trends in hospital discharges for asthma among members of a health maintenance organization. J Clin Epidemiol. 1992 Sep;45(9):999–1006. doi: 10.1016/0895-4356(92)90115-4. [DOI] [PubMed] [Google Scholar]
- Warner J. O., Götz M., Landau L. I., Levison H., Milner A. D., Pedersen S., Silverman M. Management of asthma: a consensus statement. Arch Dis Child. 1989 Jul;64(7):1065–1079. doi: 10.1136/adc.64.7.1065. [DOI] [PMC free article] [PubMed] [Google Scholar]