

Abstract
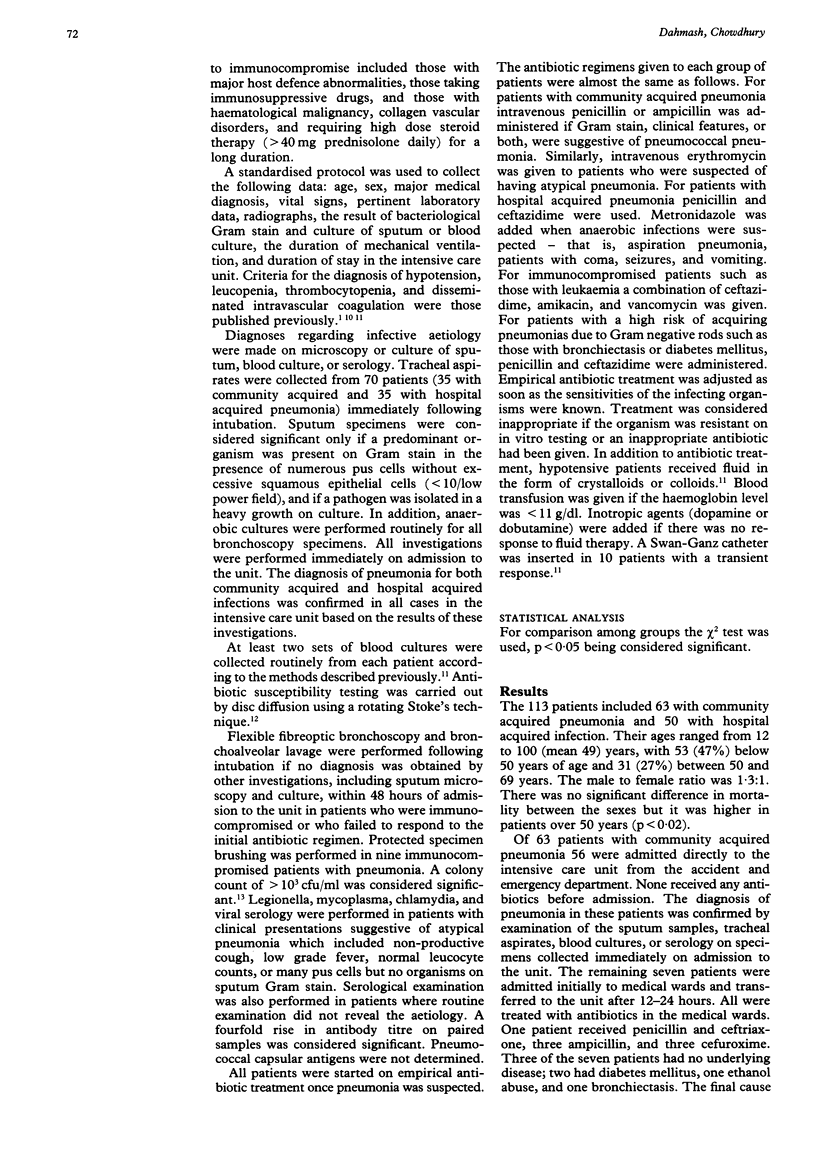
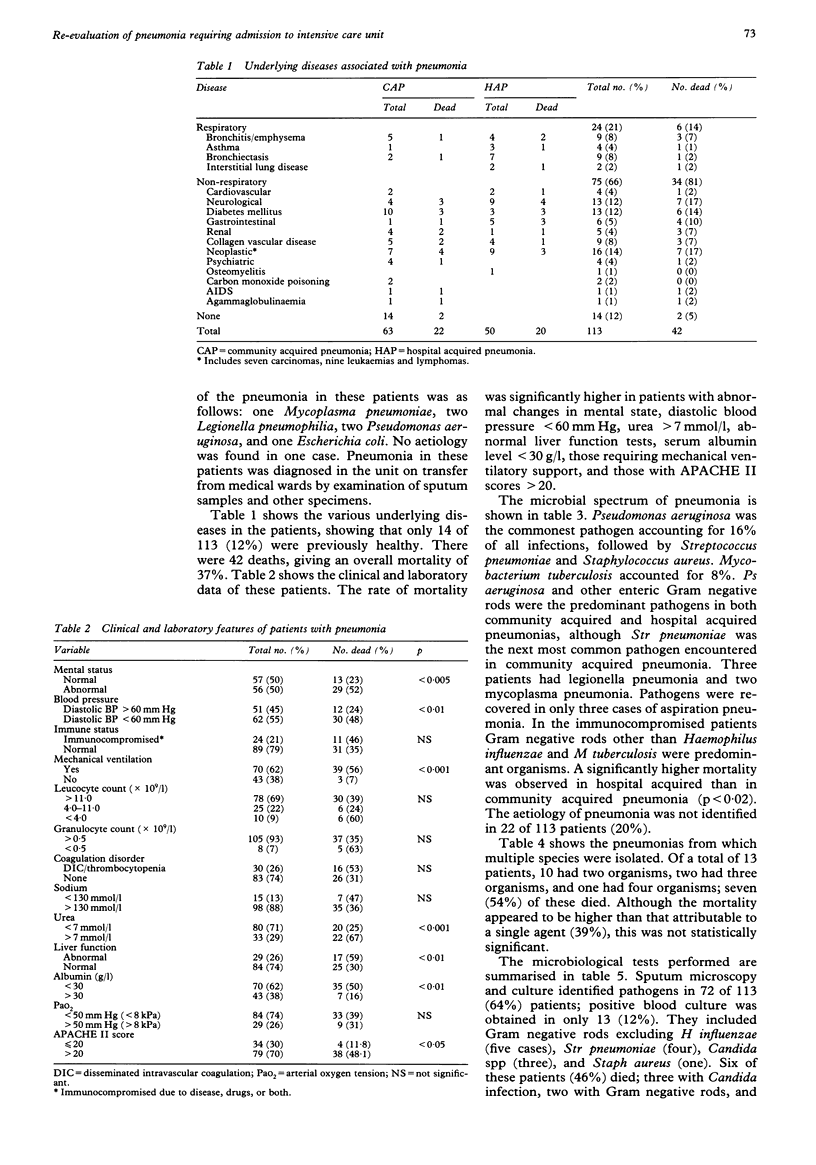
BACKGROUND--Appropriate treatment of severe community and hospital acquired pneumonias requiring admission to a medical intensive care unit depends on knowledge of the likely aetiological agents in any community. Little is known about the pattern and outcome of patients with such pneumonias in Saudi Arabia. METHODS--In a prospective study 113 patients with pneumonia were investigated in the medical intensive care unit at King Khalid University Hospital, Riyadh, Saudi Arabia between September 1991 and December 1992. The diagnosis was established by microscopy and culture of sputum, blood culture, or serological examination. A standard proforma was used to collect demographic, clinical, and laboratory data. RESULTS--A microbiological diagnosis was made in 80% of the cases with a single pathogen accounting for 69% of the isolates and multiple pathogens for 11%. Pseudomonas aeruginosa was the most common infecting agent (16%), followed by Streptococcus pneumoniae (12%), Staphylococcus aureus (9%), and Mycobacterium tuberculosis (8%). Pneumonia due to Legionella pneumophilia was diagnosed in three patients and infection due to Mycoplasma pneumoniae in two. These five cases were identified by serological examination. Gram negative rods were the predominant pathogens in both community and hospital acquired pneumonia. The aetiology of pneumonia was not identified in 20% of cases. The overall mortality was 37%. Patients with hospital acquired pneumonia had a higher mortality than those with a community acquired pneumonia. Similarly, a high mortality was found in patients who had a serious underlying disease, abnormal mental state, diastolic blood pressure < 60 mm Hg, blood urea > 7 mmol/l, abnormal liver function tests, serum albumin < 30 g/l, those who required mechanical ventilatory support, and those with APACHE II scores > 20. CONCLUSIONS--This study highlights two major findings which differ from previous reports on the aetiology of pneumonia. Firstly, Gram negative rods were the predominant pathogens in community acquired pneumonia and secondly, M tuberculosis was an important cause of pneumonia in these patients, indicating that tuberculous pneumonia should be considered in the differential diagnosis of pneumonia in Saudi Arabia.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- A'Court C., Garrard C. S. Nosocomial pneumonia in the intensive care unit: mechanisms and significance. Thorax. 1992 Jun;47(6):465–473. doi: 10.1136/thx.47.6.465. [DOI] [PMC free article] [PubMed] [Google Scholar]
- BATH J. C., BOISSARD G. P., CALDER M. A., MOFFAT M. A. PNEUMONIA IN HOSPITAL PRACTICE IN EDINBURGH 1960-1962. Br J Dis Chest. 1964 Jan;58:1–16. doi: 10.1016/s0007-0971(64)80017-6. [DOI] [PubMed] [Google Scholar]
- Berger R., Arango L. Etiologic diagnosis of bacterial nosocomial pneumonia in seriously ill patients. Crit Care Med. 1985 Oct;13(10):833–836. doi: 10.1097/00003246-198510000-00011. [DOI] [PubMed] [Google Scholar]
- Chastre J., Fagon J. Y., Domart Y., Gibert C. Diagnosis of nosocomial pneumonia in intensive care unit patients. Eur J Clin Microbiol Infect Dis. 1989 Jan;8(1):35–39. doi: 10.1007/BF01964118. [DOI] [PubMed] [Google Scholar]
- Dahmash N. S., Chowdhury N. H., Fayed D. F. Septic shock in critically ill patients: aetiology, management and outcome. J Infect. 1993 Mar;26(2):159–170. doi: 10.1016/0163-4453(93)92815-e. [DOI] [PubMed] [Google Scholar]
- Goldstraw P. The practice of cardiothoracic surgeons in the perioperative staging of non-small cell lung cancer. Thorax. 1992 Jan;47(1):1–2. doi: 10.1136/thx.47.1.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Karalus N. C., Cursons R. T., Leng R. A., Mahood C. B., Rothwell R. P., Hancock B., Cepulis S., Wawatai M., Coleman L. Community acquired pneumonia: aetiology and prognostic index evaluation. Thorax. 1991 Jun;46(6):413–418. doi: 10.1136/thx.46.6.413. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Knaus W. A., Draper E. A., Wagner D. P., Zimmerman J. E. APACHE II: a severity of disease classification system. Crit Care Med. 1985 Oct;13(10):818–829. [PubMed] [Google Scholar]
- Mandelli M., Mosconi P., Langer M., Cigada M. Prevention of pneumonia in an intensive care unit: a randomized multicenter clinical trial. Intensive Care Unit Group of Infection Control. Crit Care Med. 1989 Jun;17(6):501–505. doi: 10.1097/00003246-198906000-00003. [DOI] [PubMed] [Google Scholar]
- Mock C. N., Burchard K. W., Hasan F., Reed M. Surgical intensive care unit pneumonia. Surgery. 1988 Sep;104(3):494–499. [PubMed] [Google Scholar]
- Mufson M. A., Chang V., Gill V., Wood S. C., Romansky M. J., Chanock R. M. The role of viruses, mycoplasmas and bacteria in acute pneumonia in civilian adults. Am J Epidemiol. 1967 Nov;86(3):526–544. doi: 10.1093/oxfordjournals.aje.a120763. [DOI] [PubMed] [Google Scholar]
- Nielsen S. L., Røder B., Magnussen P., Engquist A., Frimodt-Møller N. Nosocomial pneumonia in an intensive care unit in a Danish university hospital: incidence, mortality and etiology. Scand J Infect Dis. 1992;24(1):65–70. doi: 10.3109/00365549209048402. [DOI] [PubMed] [Google Scholar]
- Nielsen S. L., Røder B., Magnussen P., Engquist A., Frimodt-Møller N. Nosocomial pneumonia in an intensive care unit in a Danish university hospital: incidence, mortality and etiology. Scand J Infect Dis. 1992;24(1):65–70. doi: 10.3109/00365549209048402. [DOI] [PubMed] [Google Scholar]
- Potgieter P. D., Hammond J. M. Etiology and diagnosis of pneumonia requiring ICU admission. Chest. 1992 Jan;101(1):199–203. doi: 10.1378/chest.101.1.199. [DOI] [PubMed] [Google Scholar]
- Ruiz-Santana S., García Jimenez A., Esteban A., Guerra L., Alvarez B., Corcia S., Gudin J., Martinez A., Quintana E., Armengol S. ICU pneumonias: a multi-institutional study. Crit Care Med. 1987 Oct;15(10):930–932. doi: 10.1097/00003246-198710000-00007. [DOI] [PubMed] [Google Scholar]
- Scheld W. M., Mandell G. L. Nosocomial pneumonia: pathogenesis and recent advances in diagnosis and therapy. Rev Infect Dis. 1991 Jul-Aug;13 (Suppl 9):S743–S751. doi: 10.1093/clinids/13.supplement_9.s743. [DOI] [PubMed] [Google Scholar]
- Sullivan R. J., Jr, Dowdle W. R., Marine W. M., Hierholzer J. C. Adult pneumonia in a general hospital. Etiology and host risk factors. Arch Intern Med. 1972 Jun;129(6):935–942. [PubMed] [Google Scholar]
- Sörensen J., Cederholm I., Carlsson C. Pneumonia: a deadly disease despite intensive care treatment. Scand J Infect Dis. 1986;18(4):329–335. doi: 10.3109/00365548609032344. [DOI] [PubMed] [Google Scholar]
- Sörensen J., Forsberg P., Håkanson E., Maller R., Sederholm C., Sörén L., Carlsson C. A new diagnostic approach to the patient with severe pneumonia. Scand J Infect Dis. 1989;21(1):33–41. doi: 10.3109/00365548909035678. [DOI] [PubMed] [Google Scholar]
- Tobin M. J., Grenvik A. Nosocomial lung infection and its diagnosis. Crit Care Med. 1984 Mar;12(3):191–199. doi: 10.1097/00003246-198403000-00008. [DOI] [PubMed] [Google Scholar]
- Toews G. B. Nosocomial pneumonia. Clin Chest Med. 1987 Sep;8(3):467–479. [PubMed] [Google Scholar]
- Villers D., Derriennic M., Raffi F., Germaud P., Baron D., Nicolas F., Courtieu A. L. Reliability of the bronchoscopic protected catheter brush in intubated and ventilated patients. Chest. 1985 Oct;88(4):527–530. doi: 10.1378/chest.88.4.527. [DOI] [PubMed] [Google Scholar]
- Wimberley N. W., Bass J. B., Jr, Boyd B. W., Kirkpatrick M. B., Serio R. A., Pollock H. M. Use of a bronchoscopic protected catheter brush for the diagnosis of pulmonary infections. Chest. 1982 May;81(5):556–562. doi: 10.1378/chest.81.5.556. [DOI] [PubMed] [Google Scholar]
- Woodhead M. A. Management of pneumonia. Respir Med. 1992 Nov;86(6):459–469. doi: 10.1016/s0954-6111(96)80003-5. [DOI] [PubMed] [Google Scholar]