

Abstract
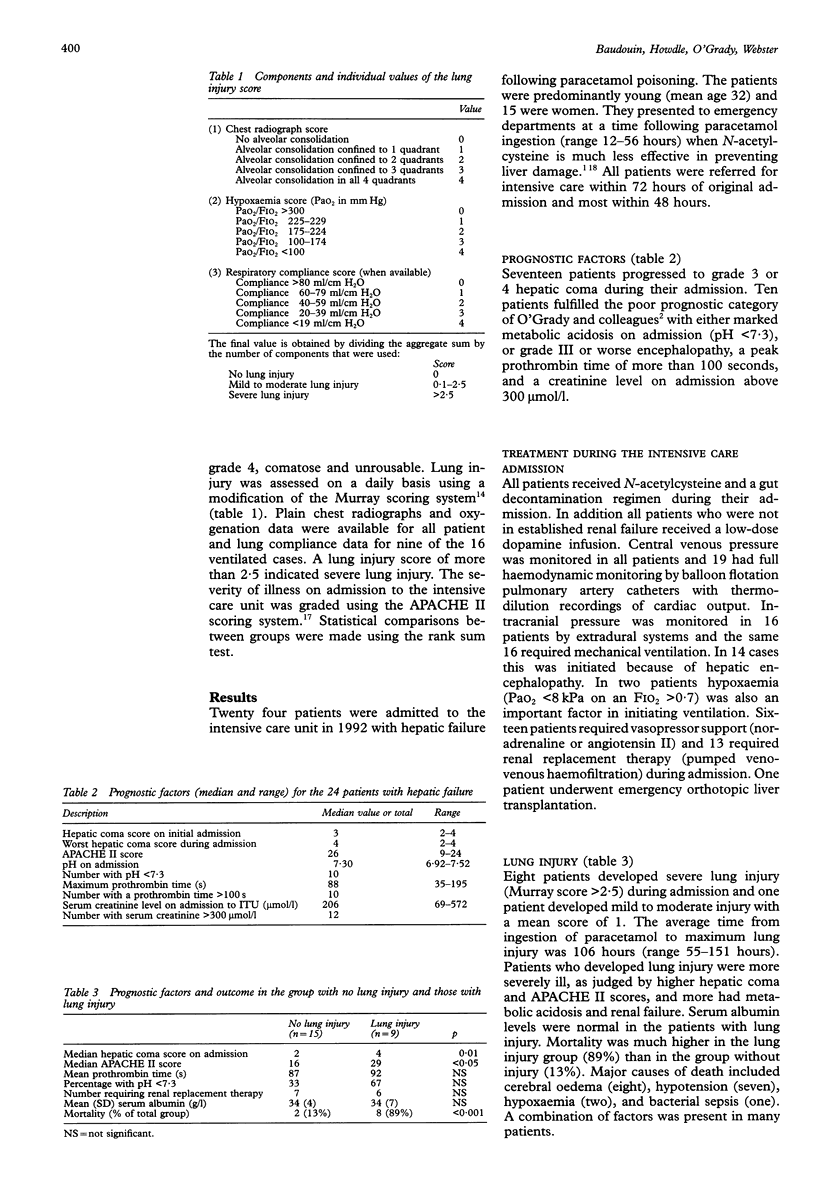
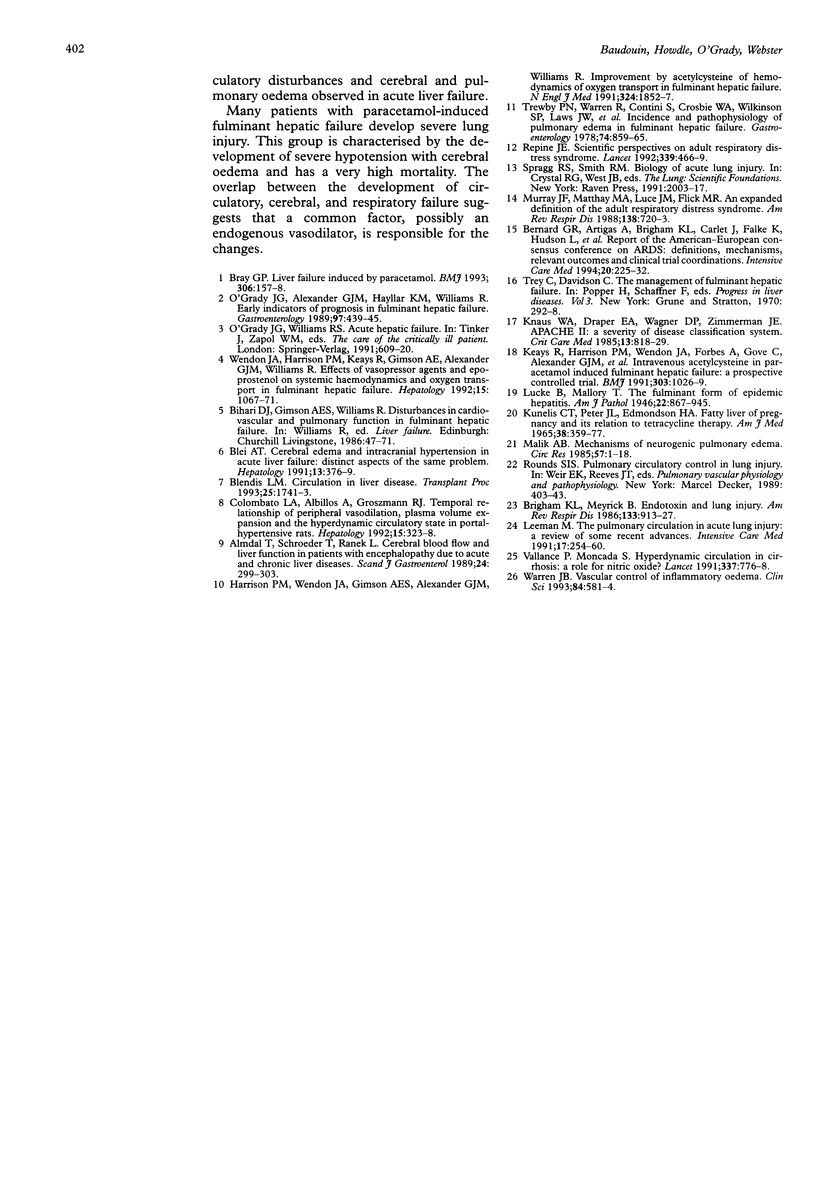
BACKGROUND--There is little information on the incidence of acute lung injury or changes in the pulmonary circulation in acute liver failure. The aim of this study was to record the incidence of acute lung injury in fulminant hepatic failure caused by paracetamol poisoning, to document the associated pulmonary circulatory changes, and to assess the impact of lung injury on patient outcome. METHODS--The degree of lung injury was retrospectively assessed by a standard scoring system (modified from Murray) in all patients with fulminant hepatic failure caused by paracetamol poisoning, admitted to the intensive care unit over a one year period. The severity of liver failure and illness, other organ system failure, and patient outcome were also analysed. RESULTS--Twenty four patients with paracetamol-induced liver failure were admitted and nine developed lung injury of whom eight (33%) had severe injury (Murray score > 2.5). In two patients hypoxaemia contributed to death. Patients with lung injury had higher median encephalopathy grades (4 v 2 in the non-injured group) and APACHE II scores (29 v 16). Circulatory failure, requiring vasoconstrictor support, occurred in all patients with lung injury but in only 40% of those without. Cerebral oedema, as detected by abnormal rises in intracranial pressure, also occurred in all patients with lung injury but in only 27% of the non-injured patients. The incidence of renal failure requiring renal replacement therapy was similar in both groups (67% and 47%). Pulmonary artery occlusion pressures were normal in the lung injury group. Cardiac output was high (median 11.2 1/min), systemic vascular resistance low (median 503 dynes/s/cm-5), and pulmonary vascular resistance low (median 70 dynes/s/cm-5), but not significantly different from the group without lung injury. Mortality was much higher in the lung injury group than in the non-injured group (89% v 13%). CONCLUSIONS--Acute lung injury was common in patients with paracetamol-induced fulminant hepatic failure and was associated with systemic circulatory failure and cerebral oedema. The development of acute lung injury was associated with high mortality.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Almdal T., Schroeder T., Ranek L. Cerebral blood flow and liver function in patients with encephalopathy due to acute and chronic liver diseases. Scand J Gastroenterol. 1989 Apr;24(3):299–303. doi: 10.3109/00365528909093050. [DOI] [PubMed] [Google Scholar]
- Bernard G. R., Artigas A., Brigham K. L., Carlet J., Falke K., Hudson L., Lamy M., LeGall J. R., Morris A., Spragg R. Report of the American-European consensus conference on ARDS: definitions, mechanisms, relevant outcomes and clinical trial coordination. The Consensus Committee. Intensive Care Med. 1994;20(3):225–232. doi: 10.1007/BF01704707. [DOI] [PubMed] [Google Scholar]
- Blei A. T. Cerebral edema and intracranial hypertension in acute liver failure: distinct aspects of the same problem. Hepatology. 1991 Feb;13(2):376–379. [PubMed] [Google Scholar]
- Blendis L. M. Circulation in liver disease. Transplant Proc. 1993 Apr;25(2):1741–1743. [PubMed] [Google Scholar]
- Bray G. P. Liver failure induced by paracetamol. BMJ. 1993 Jan 16;306(6871):157–158. doi: 10.1136/bmj.306.6871.157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brigham K. L., Meyrick B. Endotoxin and lung injury. Am Rev Respir Dis. 1986 May;133(5):913–927. [PubMed] [Google Scholar]
- Colombato L. A., Albillos A., Groszmann R. J. Temporal relationship of peripheral vasodilatation, plasma volume expansion and the hyperdynamic circulatory state in portal-hypertensive rats. Hepatology. 1992 Feb;15(2):323–328. doi: 10.1002/hep.1840150224. [DOI] [PubMed] [Google Scholar]
- Harrison P. M., Wendon J. A., Gimson A. E., Alexander G. J., Williams R. Improvement by acetylcysteine of hemodynamics and oxygen transport in fulminant hepatic failure. N Engl J Med. 1991 Jun 27;324(26):1852–1857. doi: 10.1056/NEJM199106273242604. [DOI] [PubMed] [Google Scholar]
- KUNELIS C. T., PETERS J. L., EDMONDSON H. A. FATTY LIVER OF PREGNANCY AND ITS RELATIONSHIP TO TETRACYCLINE THERAPY. Am J Med. 1965 Mar;38:359–377. doi: 10.1016/0002-9343(65)90145-2. [DOI] [PubMed] [Google Scholar]
- Keays R., Harrison P. M., Wendon J. A., Forbes A., Gove C., Alexander G. J., Williams R. Intravenous acetylcysteine in paracetamol induced fulminant hepatic failure: a prospective controlled trial. BMJ. 1991 Oct 26;303(6809):1026–1029. doi: 10.1136/bmj.303.6809.1026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Knaus W. A., Draper E. A., Wagner D. P., Zimmerman J. E. APACHE II: a severity of disease classification system. Crit Care Med. 1985 Oct;13(10):818–829. [PubMed] [Google Scholar]
- Leeman M. The pulmonary circulation in acute lung injury: a review of some recent advances. Intensive Care Med. 1991;17(5):254–260. doi: 10.1007/BF01713933. [DOI] [PubMed] [Google Scholar]
- Lucké B., Mallory T. The Fulminant Form of Epidemic Hepatitis. Am J Pathol. 1946 Sep;22(5):867–945. [PMC free article] [PubMed] [Google Scholar]
- Malik A. B. Mechanisms of neurogenic pulmonary edema. Circ Res. 1985 Jul;57(1):1–18. doi: 10.1161/01.res.57.1.1. [DOI] [PubMed] [Google Scholar]
- Murray J. F., Matthay M. A., Luce J. M., Flick M. R. An expanded definition of the adult respiratory distress syndrome. Am Rev Respir Dis. 1988 Sep;138(3):720–723. doi: 10.1164/ajrccm/138.3.720. [DOI] [PubMed] [Google Scholar]
- O'Grady J. G., Alexander G. J., Hayllar K. M., Williams R. Early indicators of prognosis in fulminant hepatic failure. Gastroenterology. 1989 Aug;97(2):439–445. doi: 10.1016/0016-5085(89)90081-4. [DOI] [PubMed] [Google Scholar]
- Repine J. E. Scientific perspectives on adult respiratory distress syndrome. Lancet. 1992 Feb 22;339(8791):466–469. doi: 10.1016/0140-6736(92)91067-i. [DOI] [PubMed] [Google Scholar]
- Trewby P. N., Warren R., Contini S., Crosbie W. A., Wilkinson S. P., Laws J. W., Williams R. Incidence and pathophysiology of pulmonary edema in fulminant hepatic failure. Gastroenterology. 1978 May;74(5 Pt 1):859–865. [PubMed] [Google Scholar]
- Vallance P., Moncada S. Hyperdynamic circulation in cirrhosis: a role for nitric oxide? Lancet. 1991 Mar 30;337(8744):776–778. doi: 10.1016/0140-6736(91)91384-7. [DOI] [PubMed] [Google Scholar]
- Warren J. B. Vascular control of inflammatory oedema. Clin Sci (Lond) 1993 Jun;84(6):581–584. doi: 10.1042/cs0840581. [DOI] [PubMed] [Google Scholar]
- Wendon J. A., Harrison P. M., Keays R., Gimson A. E., Alexander G. J., Williams R. Effects of vasopressor agents and epoprostenol on systemic hemodynamics and oxygen transport in fulminant hepatic failure. Hepatology. 1992 Jun;15(6):1067–1071. doi: 10.1002/hep.1840150616. [DOI] [PubMed] [Google Scholar]