

Abstract
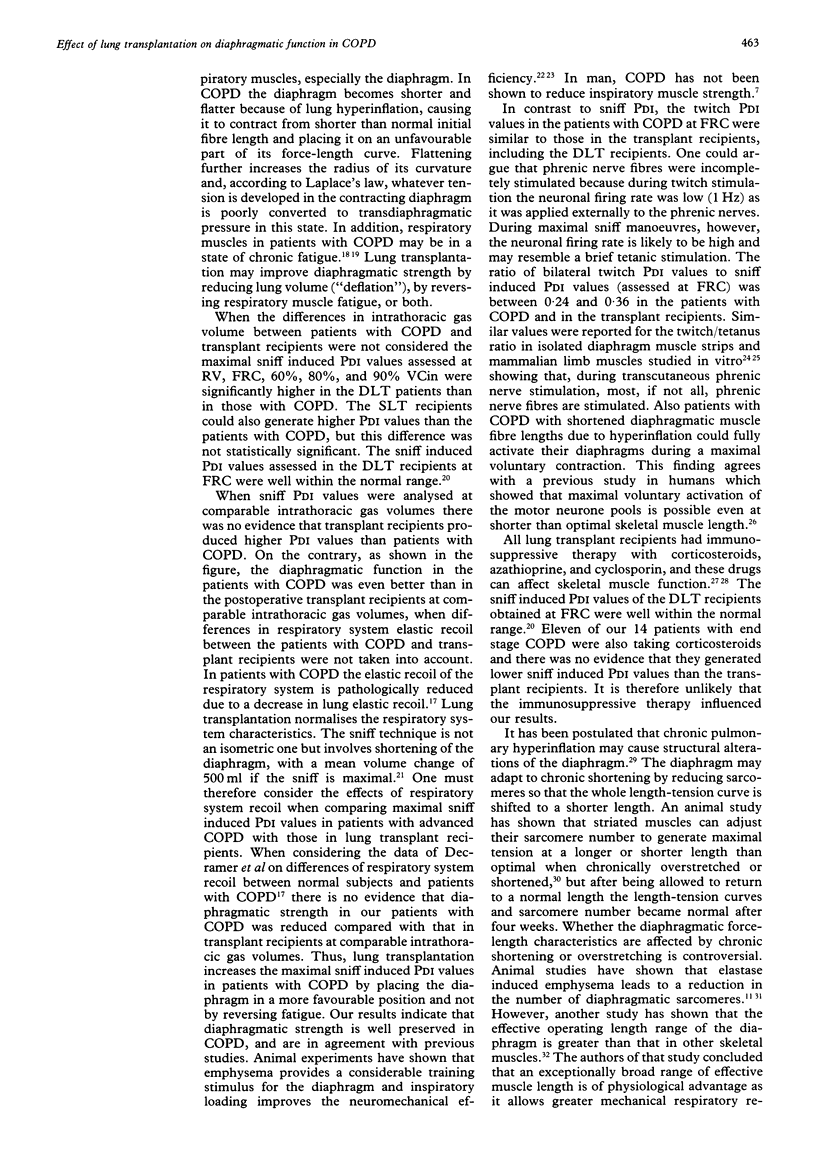
BACKGROUND--To date there are no data on the effects of lung transplantation on diaphragmatic function in patients with end stage chronic obstructive pulmonary disease (COPD). It is not known whether the relation between the transdiaphragmatic pressure (PDI) and lung volume is altered in recipients after transplantation as a result of changes in diaphragmatic structure caused by chronic hyperinflation. The effect of lung transplantation on diaphragmatic strength was determined in patients with COPD and the relation between postoperative PDI and lung volume analysed. METHODS--Diaphragmatic strength was assessed in eight double lung transplant recipients, six single lung transplant recipients, and in 14 patients with COPD whose lung function was similar to those of the transplant recipients preoperatively. PDI obtained during unilateral and bilateral phrenic nerve stimulation at 1 Hz (twitch PDI) at functional residual capacity (FRC) and during maximal sniff manoeuvres (sniff PDI) at various levels of inspiratory vital capacity (VCin) served as parameters for diaphragmatic strength. Sniff PDI assessed at the various VCin levels were used to analyse the PDI/lung volume relation. RESULTS--Lung transplantation caused a reduction in lung volume, especially in the double lung transplant recipients. As a consequence sniff PDI was higher in the double lung transplant recipients than in the patients with COPD at all levels of VCin analysed. However, sniff PDI values analysed at comparable intrathoracic gas volumes were not reduced in the patients with COPD when compared with those who underwent lung transplantation. Bilateral twitch PDI values were similar in the patients with COPD and in the lung transplant recipients. In the single lung transplant recipients unilateral twitch PDI values were similar on the transplanted and the non-transplanted side. The relation between PDI and lung volume was similar in the patients with COPD and in the lung transplant recipients. CONCLUSIONS--In patients with COPD lung transplantation leads to an increase the maximal sniff induced PDI values by placing the diaphragm in a more favourable position for pressure generation. Since patients with COPD and postoperative lung transplant recipients showed similar PDI/lung volume relations, this suggests that chronic pulmonary hyperinflation does not cause major functional alterations of the diaphragm.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Akabas S. R., Bazzy A. R., DiMauro S., Haddad G. G. Metabolic and functional adaptation of the diaphragm to training with resistive loads. J Appl Physiol (1985) 1989 Feb;66(2):529–535. doi: 10.1152/jappl.1989.66.2.529. [DOI] [PubMed] [Google Scholar]
- Arellano F., Krupp P. Muscular disorders associated with cyclosporin. Lancet. 1991 Apr 13;337(8746):915–915. doi: 10.1016/0140-6736(91)90245-k. [DOI] [PubMed] [Google Scholar]
- Bellemare F., Bigland-Ritchie B. Assessment of human diaphragm strength and activation using phrenic nerve stimulation. Respir Physiol. 1984 Dec;58(3):263–277. doi: 10.1016/0034-5687(84)90003-3. [DOI] [PubMed] [Google Scholar]
- Braun N. M., Arora N. S., Rochester D. F. Force-length relationship of the normal human diaphragm. J Appl Physiol Respir Environ Exerc Physiol. 1982 Aug;53(2):405–412. doi: 10.1152/jappl.1982.53.2.405. [DOI] [PubMed] [Google Scholar]
- Byrd R. B., Hyatt R. E. Maximal respiratory pressures in chronic obstructive lung disease. Am Rev Respir Dis. 1968 Nov;98(5):848–856. doi: 10.1164/arrd.1968.98.5.848. [DOI] [PubMed] [Google Scholar]
- Close R. I. Dynamic properties of mammalian skeletal muscles. Physiol Rev. 1972 Jan;52(1):129–197. doi: 10.1152/physrev.1972.52.1.129. [DOI] [PubMed] [Google Scholar]
- Decramer M., Demedts M., Rochette F., Billiet L. Maximal transrespiratory pressures in obstructive lung disease. Bull Eur Physiopathol Respir. 1980 Jul-Aug;16(4):479–490. [PubMed] [Google Scholar]
- Dekhuijzen P. N., Decramer M. Steroid-induced myopathy and its significance to respiratory disease: a known disease rediscovered. Eur Respir J. 1992 Sep;5(8):997–1003. [PubMed] [Google Scholar]
- Farkas G. A., Roussos C. Adaptability of the hamster diaphragm to exercise and/or emphysema. J Appl Physiol Respir Environ Exerc Physiol. 1982 Nov;53(5):1263–1272. doi: 10.1152/jappl.1982.53.5.1263. [DOI] [PubMed] [Google Scholar]
- Farkas G. A., Roussos C. Diaphragm in emphysematous hamsters: sarcomere adaptability. J Appl Physiol Respir Environ Exerc Physiol. 1983 Jun;54(6):1635–1640. doi: 10.1152/jappl.1983.54.6.1635. [DOI] [PubMed] [Google Scholar]
- Flenley D. C. Inspiratory muscle training. Eur J Respir Dis. 1985 Sep;67(3):153–158. [PubMed] [Google Scholar]
- Gandevia S. C., McKenzie D. K. Activation of human muscles at short muscle lengths during maximal static efforts. J Physiol. 1988 Dec;407:599–613. doi: 10.1113/jphysiol.1988.sp017434. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ishikawa S., Hayes J. A. Functional morphotometry of the diaphragm in patients with chronic obstructive lung disease. Am Rev Respir Dis. 1973 Jul;108(1):135–138. doi: 10.1164/arrd.1973.108.1.135. [DOI] [PubMed] [Google Scholar]
- Kelsen S. G., Wolanski T., Supinski G. S., Roessmann U. The effect of elastase-induced emphysema on diaphragmatic muscle structure in hamsters. Am Rev Respir Dis. 1983 Mar;127(3):330–334. doi: 10.1164/arrd.1983.127.3.330. [DOI] [PubMed] [Google Scholar]
- Kim M. J., Druz W. S., Danon J., Machnach W., Sharp J. T. Mechanics of the canine diaphragm. J Appl Physiol. 1976 Sep;41(3):369–382. doi: 10.1152/jappl.1976.41.3.369. [DOI] [PubMed] [Google Scholar]
- Mier A., Brophy C., Moxham J., Green M. Twitch pressures in the assessment of diaphragm weakness. Thorax. 1989 Dec;44(12):990–996. doi: 10.1136/thx.44.12.990. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miller J. M., Moxham J., Green M. The maximal sniff in the assessment of diaphragm function in man. Clin Sci (Lond) 1985 Jul;69(1):91–96. doi: 10.1042/cs0690091. [DOI] [PubMed] [Google Scholar]
- Morrison N. J., Richardson J., Dunn L., Pardy R. L. Respiratory muscle performance in normal elderly subjects and patients with COPD. Chest. 1989 Jan;95(1):90–94. doi: 10.1378/chest.95.1.90. [DOI] [PubMed] [Google Scholar]
- Moxham J., Morris A. J., Spiro S. G., Edwards R. H., Green M. Contractile properties and fatigue of the diaphragm in man. Thorax. 1981 Mar;36(3):164–168. doi: 10.1136/thx.36.3.164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Newell S. Z., McKenzie D. K., Gandevia S. C. Inspiratory and skeletal muscle strength and endurance and diaphragmatic activation in patients with chronic airflow limitation. Thorax. 1989 Nov;44(11):903–912. doi: 10.1136/thx.44.11.903. [DOI] [PMC free article] [PubMed] [Google Scholar]
- North J., Mallabar M., Desrochers R. Vocational preparation and employability development. Child Welfare. 1988 Nov-Dec;67(6):573–586. [PubMed] [Google Scholar]
- Rochester D. F., Arora N. S. Respiratory muscle failure. Med Clin North Am. 1983 May;67(3):573–597. doi: 10.1016/s0025-7125(16)31190-7. [DOI] [PubMed] [Google Scholar]
- SCHOTTELIUS B. A., THOMSON J. D., HINES H. M. Capacity of skeletal muscle to develop isometric tension after prolonged shortening. Am J Physiol. 1954 Dec;179(3):491–494. doi: 10.1152/ajplegacy.1954.179.3.491. [DOI] [PubMed] [Google Scholar]
- Scott K. W., Hoy J. The cross sectional area of diaphragmatic muscle fibres in emphysema, measured by an automated image analysis system. J Pathol. 1976 Oct;120(2):121–128. doi: 10.1002/path.1711200208. [DOI] [PubMed] [Google Scholar]
- Similowski T., Yan S., Gauthier A. P., Macklem P. T., Bellemare F. Contractile properties of the human diaphragm during chronic hyperinflation. N Engl J Med. 1991 Sep 26;325(13):917–923. doi: 10.1056/NEJM199109263251304. [DOI] [PubMed] [Google Scholar]
- Steele R. H., Heard B. E. Size of the diaphragm in chronic bronchitis. Thorax. 1973 Jan;28(1):55–60. doi: 10.1136/thx.28.1.55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tabary J. C., Tabary C., Tardieu C., Tardieu G., Goldspink G. Physiological and structural changes in the cat's soleus muscle due to immobilization at different lengths by plaster casts. J Physiol. 1972 Jul;224(1):231–244. doi: 10.1113/jphysiol.1972.sp009891. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thurlbeck W. M. Diaphragm and body weight in emphysema. Thorax. 1978 Aug;33(4):483–487. doi: 10.1136/thx.33.4.483. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wanke T., Schenz G., Zwick H., Popp W., Ritschka L., Flicker M. Dependence of maximal sniff generated mouth and transdiaphragmatic pressures on lung volume. Thorax. 1990 May;45(5):352–355. doi: 10.1136/thx.45.5.352. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Williams T. J., Grossman R. F., Maurer J. R. Long-term functional follow-up of lung transplant recipients. Clin Chest Med. 1990 Jun;11(2):347–358. [PubMed] [Google Scholar]
- Williams T. J., Patterson G. A., McClean P. A., Zamel N., Maurer J. R. Maximal exercise testing in single and double lung transplant recipients. Am Rev Respir Dis. 1992 Jan;145(1):101–105. doi: 10.1164/ajrccm/145.1.101. [DOI] [PubMed] [Google Scholar]