

Abstract
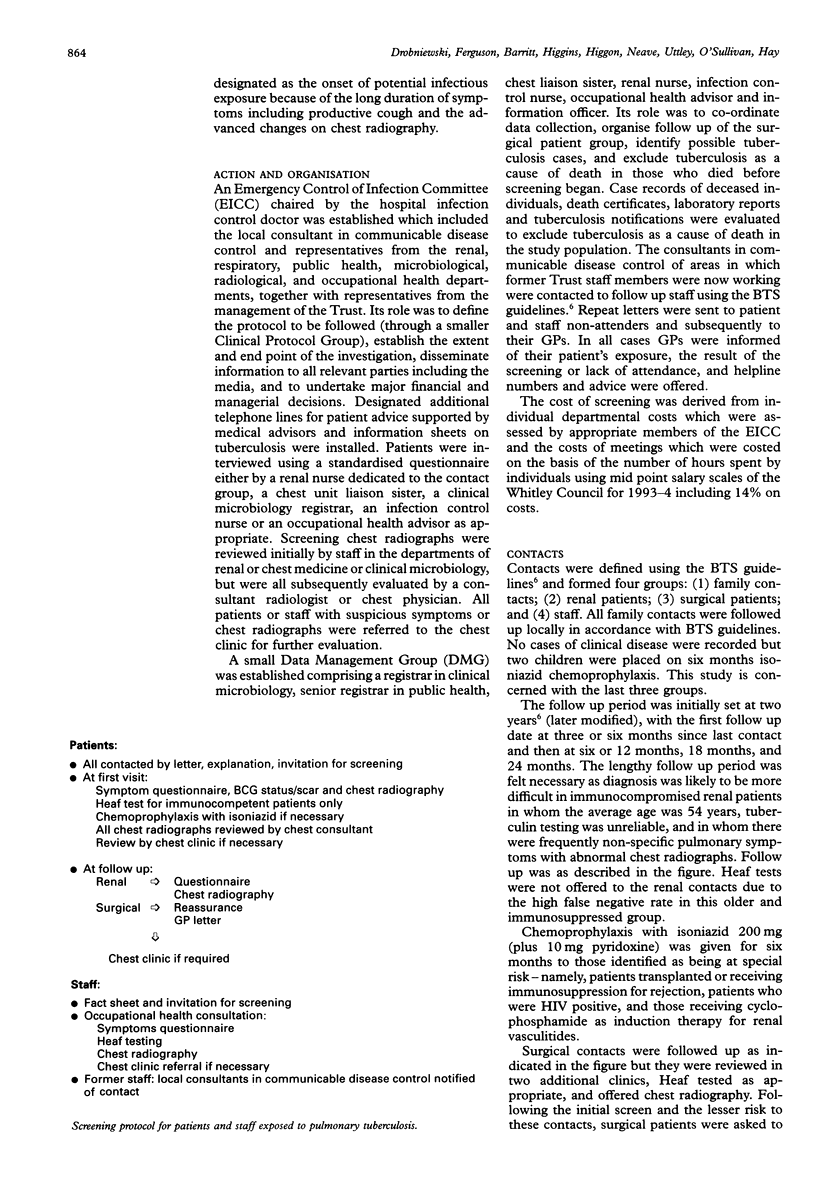
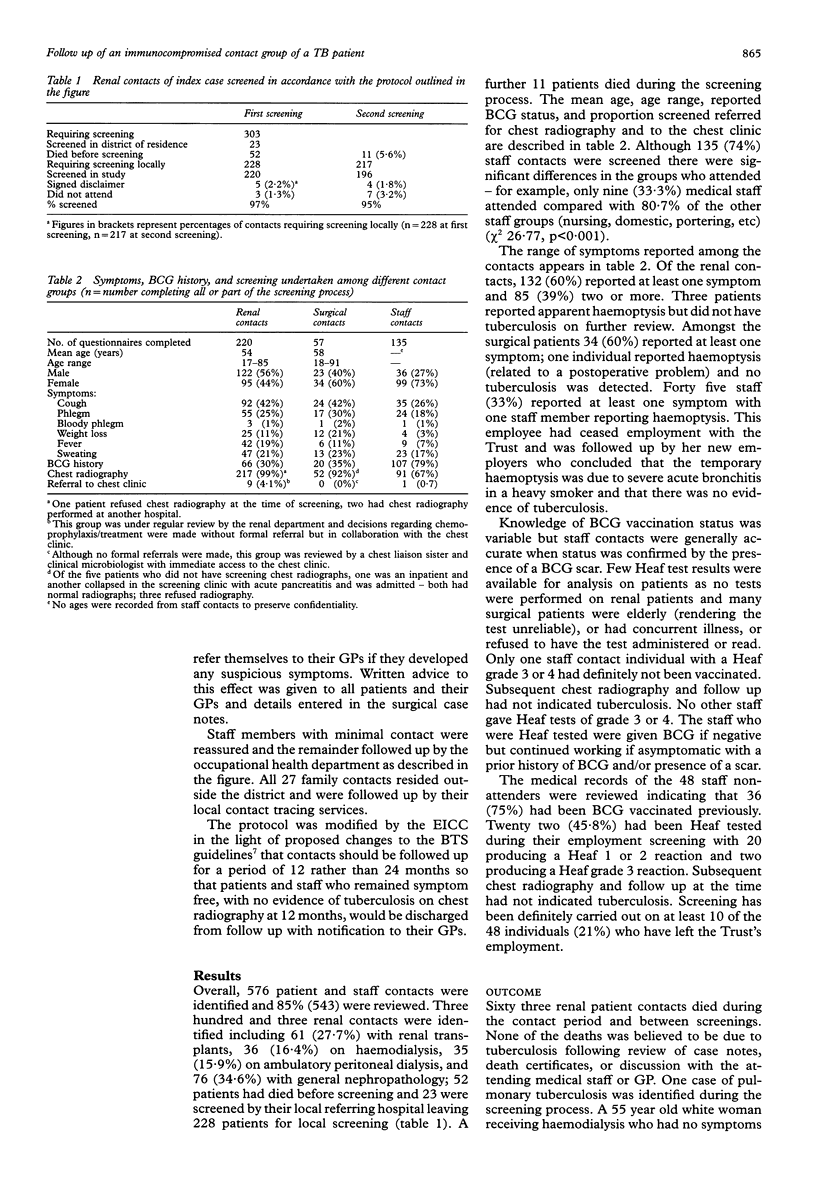
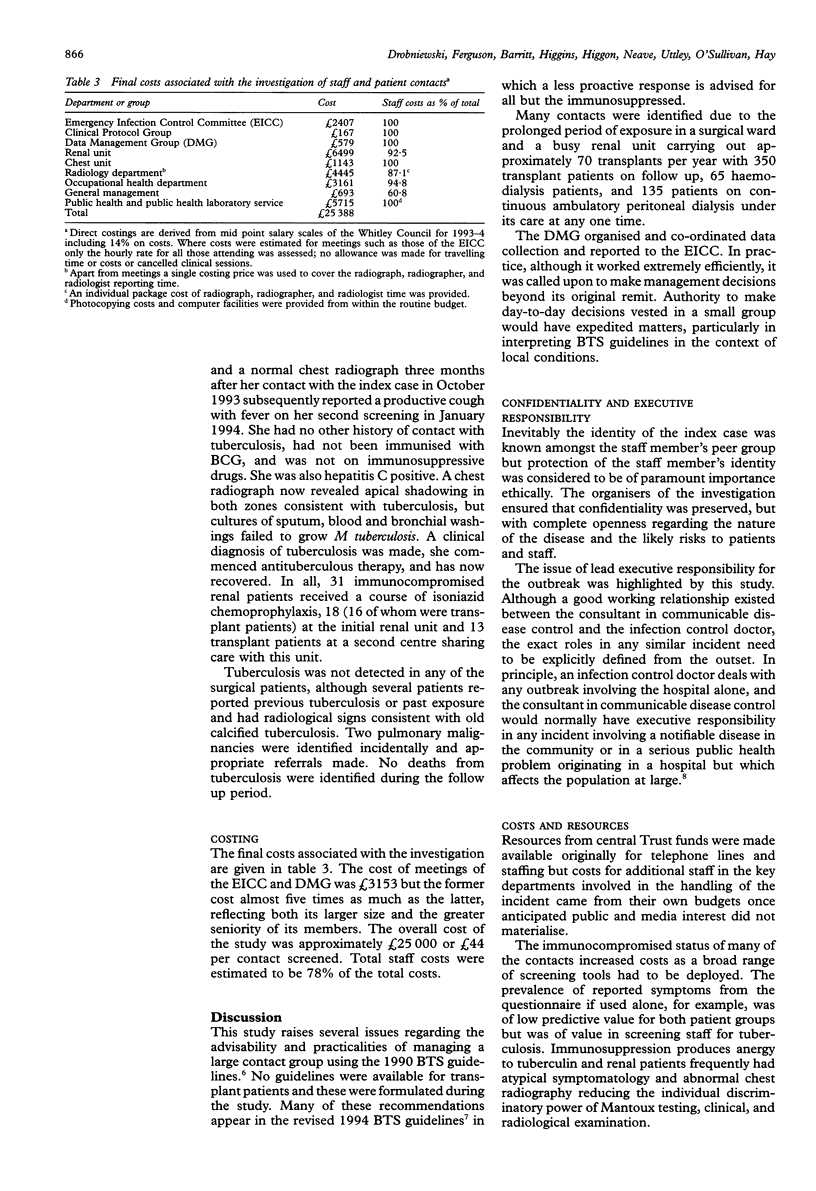
BACKGROUND--The organisation, management, outcome and cost of follow up of a large group of mainly immunocompromised patients and healthcare workers who were exposed to a staff member of a London renal unit with smear positive pulmonary tuberculosis are described. METHODS--Following British Thoracic Society (BTS) guidelines, 576 close contacts were identified and divided into three groups: (1) 303 renal patients including 61 with renal transplants; (2) 90 surgical patients; and (3) 183 staff members. Screened contacts were interviewed, completed a symptoms questionnaire, and were offered a chest radiograph and Heaf or Mantoux test if appropriate with referral to a chest physician if required. RESULTS--Overall, 524 (85%) living contacts have been screened: 243 (97%) renal (first screening), 63 (70%) surgical, and 135 (74%) staff contacts. Thirty one transplant patients were prescribed isoniazid chemoprophylaxis. Fifty two renal patients had died before screening and 11 deaths occurred after first interview. One case of tuberculosis epidemiologically related to the index case was diagnosed on clinical criteria. A review of the case records and/or death certificates and entries on to tuberculosis registers indicated no further cases. The cost of the investigation was estimated to be approximately franc25 000, or franc44 per contact screened, with staff costs comprising 79% of the total. CONCLUSIONS--Undiagnosed tuberculosis in healthcare workers working with immunosuppressed patients can lead to large and expensive follow up studies. The applicability of the 1990 and 1994 BTS guidelines to the investigation of tuberculosis in an immunocompromised nosocomial group, and the role of the infection control doctor and the consultant in Communicable Disease Control in overlapping nosocomial and community incidents, are discussed.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Alland D., Kalkut G. E., Moss A. R., McAdam R. A., Hahn J. A., Bosworth W., Drucker E., Bloom B. R. Transmission of tuberculosis in New York City. An analysis by DNA fingerprinting and conventional epidemiologic methods. N Engl J Med. 1994 Jun 16;330(24):1710–1716. doi: 10.1056/NEJM199406163302403. [DOI] [PubMed] [Google Scholar]
- Bloom B. R., Murray C. J. Tuberculosis: commentary on a reemergent killer. Science. 1992 Aug 21;257(5073):1055–1064. doi: 10.1126/science.257.5073.1055. [DOI] [PubMed] [Google Scholar]
- Drobniewski F. A., Kent R. J., Stoker N. G., Uttley A. H. Molecular biology in the diagnosis and epidemiology of tuberculosis. J Hosp Infect. 1994 Dec;28(4):249–263. doi: 10.1016/0195-6701(94)90089-2. [DOI] [PubMed] [Google Scholar]
- Higgins R. M., Cahn A. P., Porter D., Richardson A. J., Mitchell R. G., Hopkin J. M., Morris P. J. Mycobacterial infections after renal transplantation. Q J Med. 1991 Feb;78(286):145–153. [PubMed] [Google Scholar]
- Jereb J. A., Burwen D. R., Dooley S. W., Haas W. H., Crawford J. T., Geiter L. J., Edmond M. B., Dowling J. N., Shapiro R., Pasculle A. W. Nosocomial outbreak of tuberculosis in a renal transplant unit: application of a new technique for restriction fragment length polymorphism analysis of Mycobacterium tuberculosis isolates. J Infect Dis. 1993 Nov;168(5):1219–1224. doi: 10.1093/infdis/168.5.1219. [DOI] [PubMed] [Google Scholar]
- Jereb J. A., Burwen D. R., Dooley S. W., Haas W. H., Crawford J. T., Geiter L. J., Edmond M. B., Dowling J. N., Shapiro R., Pasculle A. W. Nosocomial outbreak of tuberculosis in a renal transplant unit: application of a new technique for restriction fragment length polymorphism analysis of Mycobacterium tuberculosis isolates. J Infect Dis. 1993 Nov;168(5):1219–1224. doi: 10.1093/infdis/168.5.1219. [DOI] [PubMed] [Google Scholar]
- Qunibi W. Y., al-Sibai M. B., Taher S., Harder E. J., de Vol E., al-Furayh O., Ginn H. E. Mycobacterial infection after renal transplantation--report of 14 cases and review of the literature. Q J Med. 1990 Oct;77(282):1039–1060. doi: 10.1093/qjmed/77.1.1039. [DOI] [PubMed] [Google Scholar]
- Rodrigues L. C., Smith P. G. Tuberculosis in developing countries and methods for its control. Trans R Soc Trop Med Hyg. 1990 Sep-Oct;84(5):739–744. doi: 10.1016/0035-9203(90)90172-b. [DOI] [PubMed] [Google Scholar]
- Small P. M., Hopewell P. C., Singh S. P., Paz A., Parsonnet J., Ruston D. C., Schecter G. F., Daley C. L., Schoolnik G. K. The epidemiology of tuberculosis in San Francisco. A population-based study using conventional and molecular methods. N Engl J Med. 1994 Jun 16;330(24):1703–1709. doi: 10.1056/NEJM199406163302402. [DOI] [PubMed] [Google Scholar]