

A 63-year-old Caucasian male, diabetic for 1 year presented with a week long history of feeling unwell. He never had urinary problems in the past. Examination was notable for a palpable lower abdominal cystic mass. Investigation showed elevated BUN 62 mg/dl and creatinine 2.9 mg/dl. Contrast-enhanced computed tomography showed bilateral hydroureteronephrosis [Figure 1], marked distention of the bladder [Figure 2, solid arrow] and posteriorly located diverticulum [Figure 2, open arrow], with diverticular mouth in the center (double arrow). Catheterization resulted in 5 L of urine in first 6 h and resolution of renal failure (creatinine 1.7 mg/dl). In-hospital management also included intravenous followed by oral antibiotics for Escherichia coli bacteremia and urinary infection. Follow-up ultrasonography [Figure 3] and urodynamic studies showed noncontractile trigone with postero-laterally located diverticula. Intermittent self- catheterization was advised to prevent further obstruction with a plan for surgery.
Figure 1.
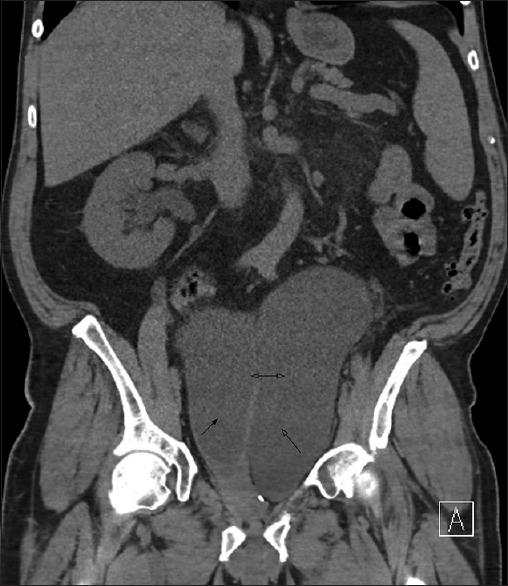
Vertical section of the computed tomography abdomen and pelvis showing the distended bladder (solid arrow head), with diverticula (open arrow), diverticular mouth (double arrow) and right kidney hydronephrosis
Figure 2.
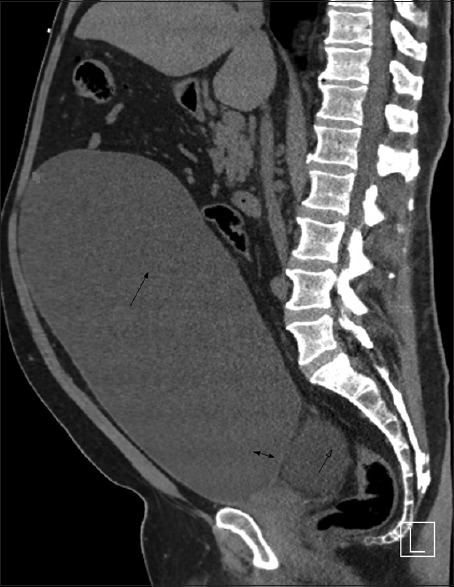
Coronal section of the computed tomography abdomen and pelvis showing the distended bladder (solid arrow) with diverticulum (open arrow). Double arrow points to the diverticular mouth
Figure 3.
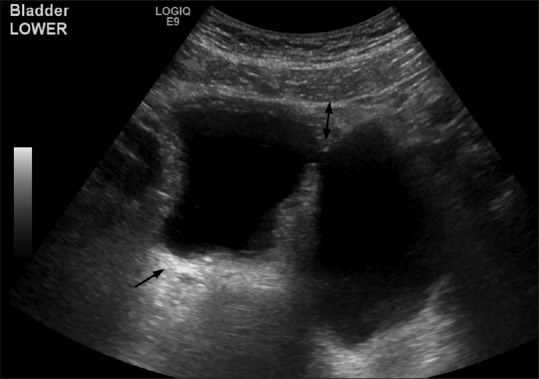
Ultrasonography of bladder showing left side bladder (arrow) and posterolateral diverticula. Diverticular mouth is marked by double arrow
Primary bladder diverticula are congenital, smooth walled, solitary in nature and rarely diagnosed in adults.[1] Symptoms of associated vesico-ureteric reflux, infection, hematuria, abdominal pain and mass are present in childhood. Acquired or secondary form of diverticula seen in adults are usually multiple, with trabeculated bladder wall, and secondary to either both benign and malignant outflow obstruction or neurogenic bladders.[2] Differential diagnosis includes midline cyst due to incomplete obliteration of Urachus and Müllerian duct, bladder neck obstruction related to posterior urethral diverticulum, prostatic retention cyst, ejaculatory and vas deferens cyst. Diagnosis relies on radiologic and endoscopic findings.[3] Most diverticula are asymptomatic and small, but symptomatic (infection, rupture, reflux, stone or tumor) and large diverticula requires diverticulectomy either by open, laparoscopic or transurethral methods.[3,4]
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Shah KJ. Bladder diverticulum: An uncommon cause of acute retention of urine in a male child. Br J Radiol. 1979;52:504–6. doi: 10.1259/0007-1285-52-618-504. [DOI] [PubMed] [Google Scholar]
- 2.Kwan DJ, Lowe FC. Congenital bladder diverticulum: An unusual presentation with abdominal mass, urinary retention, and renal failure in a young adult. Urol Radiol. 1992;14:194–6. doi: 10.1007/BF02926928. [DOI] [PubMed] [Google Scholar]
- 3.Pace AM, Powell C. Congenital vesical diverticulum in a 38-year-old female. Int Urol Nephrol. 2005;37:473–5. doi: 10.1007/s11255-004-8074-x. [DOI] [PubMed] [Google Scholar]
- 4.Doehn C, Baumgärtel M, Fornara P, Jocham D. The largest bladder diverticulum ever? J Urol. 1999;162:793–4. doi: 10.1097/00005392-199909010-00050. [DOI] [PubMed] [Google Scholar]