

Highlights
-
•
A rare case of abdominal pain after low velocity trauma based on traumatic rupture of Meckel’s diverticulum.
-
•
Meckel’s diverticulum is an embryological anomaly of the digestive tract.
-
•
Histopathological proof of a perforated diverticulum.
-
•
Consider perforation of a Meckel’s diverticulum as cause of acute deterioration.
Keywords: Meckel’s diverticulum, Traumatic rupture, Blunt trauma
Abstract
Introduction
a Meckel’s diverticulum is one of the most common congenital anomalies of the digestive tract. The reported lifetime complication rate is 4%, mostly due to hemorrhage, obstruction, perforation or inflammation. A symptomatic Meckel’s diverticulum due to rupture after blunt abdominal trauma is very rare. We believe this case report is the first reporting a rupture of a Meckel’s diverticulum after a low velocity blunt abdominal trauma and outlining the importance of a thorough and complete examination of the patient after blunt abdominal trauma.
Presentation of case
a 17-year-old male presented with abdominal pain after blunt abdominal trauma during a soccer game. Physical examination showed signs of peritonitis in all quadrants of the abdomen. During admission the patient deteriorated with decreasing blood pressure and raising pulse rate. A CT-scan showed free abdominal fluid. Our patient was scheduled for an emergent laparotomy where a perforated Meckel’s diverticulum with fecal spill was found. A segmental ileal resection was performed. Post-operative, patient developed a pneumonia and also intra-abdominal abscesses treated with percutaneous drainage. After an admission period of 17-days the patient was discharged.
Conclusion
perforation of a Meckel’s diverticulum is rarely suspected as a cause of acute deterioration following blunt abdominal trauma. This case shows the importance of awareness of this kind of injury especially in male patients.
1. Introduction
In 1809 Johann Meckel was the first to describe the embryological and pathological features of the ileal diverticulum [1]. A Meckel’s diverticulum is one of the most common anomalies of the digestive tract, developing when a remnant of the embryological connection between the umbilical and bowel remains. Occurrence follows a rough ‘law of 2s’: 2% of the population, 2 ft. (60 cm) from the ileocaecal valve; 2 in. (5 cm) in length; and twice as common in males as in females [2]. The reported lifetime complication rate is 4% [3], [4]. Symptomatic cases usually present with hemorrhage, obstruction, perforation and inflammation [5].
Rarely a Meckel's diverticulum presents because of a rupture secondary to blunt trauma, since the diverticulum is not bound by ligaments and therefore no acceleration or deceleration injury is expected.
2. Presentation of case
A 17-year-old male, without medical history, presented with abdominal pain after a firm kick in the abdomen during a soccer game. Physical examination showed signs of peritonitis in all quadrants. Blood pressure, pulse and temperature were 138/88 mmHg, 93/min and 39.3 °C respectively. Laboratory tests showed: hemoglobin 9.8 mmol/L, leukocytes 1.7 × 109, and CRP 30 mg/L. Ultrasound at presentation showed minimal free abdominal fluid and no signs of traumatic injury of abdominal organs. The patient was admitted for observation. Within five hours after admission, the clinical condition deteriorated with decrease of the blood pressure (105/50 mmHg) and increasing pulse rate (118/min). The CT-scan showed abdominal fluid and minimal free air in the abdominal cavity, interpreted as due to bowel perforation. Abdominal exploration showed fecal spill in all quadrants and a ruptured Meckel’s diverticulum (Fig. 1). A segmental ileal resection including the Meckel’s diverticulum was performed. Despite intravenous antibiotics, the postoperative course was complicated with a mild pneumonia and several intra-abdominal abscesses which needed percutaneous drainage. The patient was discharged after an admission period of 17 days. The histopathological examination of the resection specimen revealed a perforated diverticulum of 4.2 cm in length, lined with intestinal mucosa (Fig. 2, Fig. 3). This work has been reported in line with the CARE criteria [6].
Fig. 1.

Perioperative image of Meckel’s diverticulum.
Fig. 2.
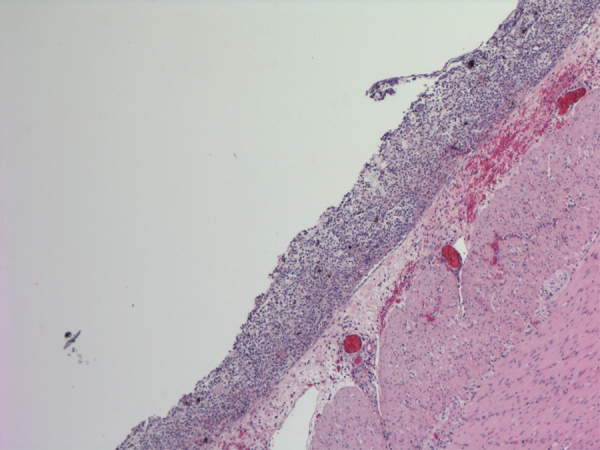
Histopathologic view of perforated Meckel’s diverticulum, showing signs of feces contamination.
Fig. 3.
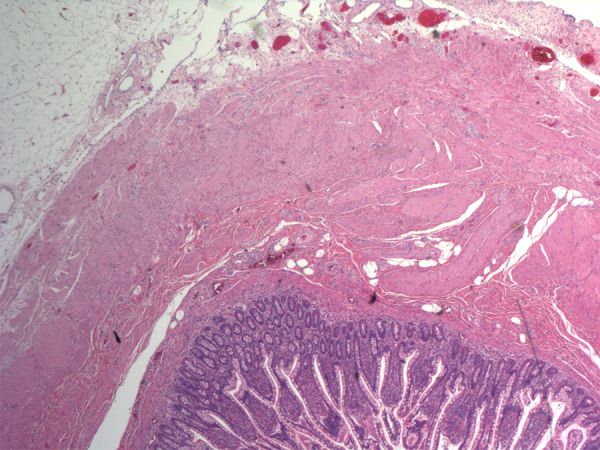
Histopathologic view of Meckel’s divertikel lined with intestinal mucosa.
3. Discussion
A congenital ileal diverticulum, is the remnant of the proximal part of the yolk stalk which results after failure of obliteration. The diverticulum typically appears as a fingerlike pouch that arises from the antimesenteric border of the ileum. The wall of the diverticulum contains all layers of the ileum and may contain small patches of gastric and pancreatic tissues. The gastric mucosa often secretes acid, producing ulceration and bleeding [7]. Preoperative diagnosis of the diverticulum is described to be low (5.7%), but this has improved with the use of radionuclide scanning with 99mTc sodium pertechnetate [2], [8].
When a patient presents with an acute abdomen following blunt abdominal trauma, the most probable causes are injuries of liver and spleen. When perforation of a hollow organ is suspected, attention is mostly drawn to the duodenum and jejuno-ileum. Given the low incidence of both a Meckel’s diverticulum and blunt small bowel injuries, it is not surprising that reports of Meckel’s diverticulum perforation from blunt trauma are exceedingly rare, and therefore incidence is unknown. The first is reported by Park and Lucas in 1970 and to the best of our knowledge, only four other cases are described of traumatic rupture of a Meckel’s diverticulum, all following road accidents [1], [9], [10], [11]. We believe that our report is the first following low velocity blunt abdominal trauma.
The strength in our case would be the fact that although imaging modalities could not point out the cause of deterioration, patient was taken into surgery to prevent further harm. Pointing out the importance of proper clinical acuity, and not only relying on modern technologies in clinical decision making. However, you could debate if the delay between admission and surgery was too long, and thereby contributing to the complications post-operatively.
Factors associated with increased risk of complications are: male sex, age below 50 years, heterotopic mucosa and a length greater than 2 cm [3], [12], [13]. In literature, seat-belt use is also associated with increased incidence of small bowel injuries [9]. Possible reasons for developing complications in our patient, is the fact that he is male, aged below 50 years and had a length of the diverticulum >2 cm. Only heterotopic epithelium in the diverticulum was not found in this case. In our opinion the most convincing reason for the raised complications, is that the diverticulum was crushed between the foot of the center forward and the vertebrae. Crush injury leads to increased intra-abdominal pressure which can cause a closed-loop obstruction at susceptible areas such as the terminal ileum or rectum which leads to perforation [14].
With this case report, we want to highlight the importance of thorough physical examination and particularly a wide differential diagnosis to prevent missing rare but important and sometimes life-threatening diagnoses.
4. Conclusion
Although a perforation of a Meckel’s diverticulum is a rare complication after low velocity blunt abdominal trauma, this case shows the importance of awareness of this kind of injury especially in male patients.
Conflicts of interest
None.
Source of funding
This case report is realized without any funding.
Ethical approval
There was no ethics approval required for this case report.
Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Author contribution
W. Tummers: author of case report, involved with the patient during admission. J. van der Vorst: co-author, involved with the patient at time of surgery and during admission. D. Swank: co-author, surgeon responsible for the emergency surgery.
Guarantor
J. van der Vorst and W. Tummers.
Acknowledgment
E. de Jonge, pathologist, M.D. Ph.D., Groene Hart hospital, Gouda.
Contributor Information
W.S. Tummers, Email: w.s.f.j.tummers@lumc.nl.
J.R. van der Vorst, Email: joost.van.der.vorst@ghz.nl.
D.J. Swank, Email: Dingeman.Swank@ghz.nl.
References
- 1.Ekwunife C.N., Mbadugha T.N., Ogbue U.N. Isolated Meckel’s diverticulum perforation as a sequel to blunt abdominal trauma: a case report. J. Med. Case Rep. 2014;8:111. doi: 10.1186/1752-1947-8-111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Henry M.M., Thompson J.N. 2th ed. Elsevier; Philadelphia: 2005. Clinical Surgery. [Google Scholar]
- 3.Park J.J., Wolff B.G., Tollefson M.K., Walsh E.E., Larson D.R. Meckel diverticulum: the Mayo clinic experience with 1476 patients 1950–2002. Ann. Surg. 2005;241:529–533. doi: 10.1097/01.sla.0000154270.14308.5f. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Soltero M.J., Bill A.H. The natural history of Meckel’s diverticulum and its relation to incidental removal. A study of 202 cases of diseased Meckel’s diverticulum found in King County, Washington, over a fifteen year period. Am. J. Surg. 1976;132:168–173. doi: 10.1016/0002-9610(76)90043-x. [DOI] [PubMed] [Google Scholar]
- 5.Turgeon D.K., Barnett J.L. Meckel’s diverticulum. Am. J. Gastroenterol. 1990;85:777–784. [PubMed] [Google Scholar]
- 6.Gagnier J., Kienle G., Altman D.G., Moher D., Sox H., Riley D.S., CARE group The CARE guidelines: consensus-based clinical case report guideline development. J. Clin. Epidemiol. 2013;67(1):46–51. doi: 10.1016/j.jclinepi.2013.08.003. [DOI] [PubMed] [Google Scholar]
- 7.Moore K.L., Persaud T.V.N. 7th ed. Elsevier; Philadelphia: 2003. The Developing Human, Clinically Oriented Embyrology. [Google Scholar]
- 8.Yamaguchi M., Takeuchi S., Awazu S. Meckel’s diverticulum: investigation of 600 patients in Japanese literature. Am. J. Surg. 1978;146:247–249. doi: 10.1016/0002-9610(78)90238-6. [DOI] [PubMed] [Google Scholar]
- 9.Park H., Lucas C.E. Perforated Meckel’s diverticulum following blunt abdominal trauma. J. Trauma. 1970;10:706–707. [PubMed] [Google Scholar]
- 10.Kazemi K., Jalaeian H., Fattahi M.R., Hosseini S.V., Shafiee M., Roshan N. Ruptured Mekel’s diverticulum following blunt abdominal trauma. Med. Princ. Pract. 2008;17:161–163. doi: 10.1159/000112973. [DOI] [PubMed] [Google Scholar]
- 11.Sartorelli K.H., Healey C., Deross A. Perforated Meckel’s diverticulum in a child after blunt abdominal trauma. J. Trauma. 2007;63:1167–1168. doi: 10.1097/01.ta.0000223940.42486.c8. [DOI] [PubMed] [Google Scholar]
- 12.McKay R. High incidence of symptomatic Meckel’s diverticulum in patients less than fifty years of age: an indication for resection. Am. Surg. 2007;73:271–275. [PubMed] [Google Scholar]
- 13.Varcoe R.L., Wong S.W., Taylor C.F., Newstead G.L. Diverticulectomy is inadequate treatment for short Meckel’s diverticulum with heterotopic mucosa. ANZ J. Surg. 2004;74:869–872. doi: 10.1111/j.1445-1433.2004.03191.x. [DOI] [PubMed] [Google Scholar]
- 14.Hefny A.F., Al-Ashaal Y.I., Bani-Hashem A.M., Abu-Zidan F.M. Seatbelt syndrome associated with an isolated rectal injury: case report. World J. Emerg. Surg. 2010;5(February (1)):4. doi: 10.1186/1749-7922-5-4. [DOI] [PMC free article] [PubMed] [Google Scholar]