

Abstract
Statement of Problem:
Three main factors which determine the success of an All-ceramic restoration are esthetic value, resistance to fracture and third being the marginal fit. Marginal fit and internal adaptation are crucial factors in increasing the longevity of the restoration. Newer and economical CAD CAM systems have been introduced claiming better marginal fit and adaptation of All ceramic crowns. CAD CAM systems involves scanning of the die or the tooth preparation and milling of the restoration, which may have variations among the systems available.
Aim of the Study:
Our study intended to check the marginal fit and internal adaptation of commonly used CAD CAM systems namely CERAMILL and CEREC -In Lab MC XL.
Materials and Methods:
Two groups of typodont teeth (n = 10) were prepared using a standardized protocol to receive All ceramic copings. 10 samples of Group A were used for fabrication of copings using CERAMILL system and 10 samples of Group B were used for fabrication of copings using CEREC -In Lab MC XL system. They were then luted with glass ionomer cement under mild finger pressure. Samples were embedded in resin and sliced longitudinally. They were then viewed under stereomicroscope and readings were measured along 15 points using ImageScope software. The P value was set at 0.05 at 95% confidence interval with 80% power. The data were checked for normality and unpaired t-test was used to evaluate the results of the two groups.
Results:
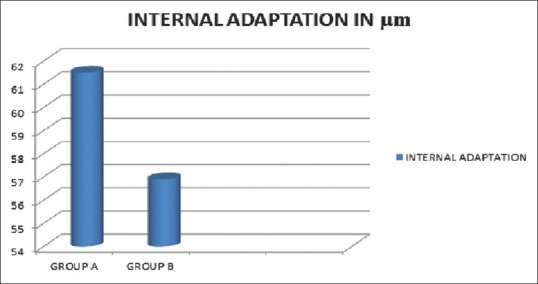
The overall internal adaptation was 61.5 ± 5.2 μm for CERAMILL and 56.9 ± 5.7 μm for CEREC -In Lab MC XL (P < 0.05). The marginal fit for CERAMILL was 83 μm and for CEREC -In Lab MC XL was 68 μm (P < 0.05).
Conclusion:
The marginal adaptation of CEREC -In Lab MC XL (68 μm) was found to be superior to CERAMILL (83 μm) (P < 0.05). Both the CEREC -In Lab MC XL and CERAMILL copings demonstrated internal adaptation and marginal fit within acceptable discrepancy range. When corroborating both the internal adaptation and marginal fit, CEREC -In Lab MC XL was found to be better than CERAMILL.
Keywords: All ceramic coping, CERAMILL CAD CAM, CEREC CAD CAM, internal adaptation, marginal fit
INTRODUCTION
The demand for better esthetics by the patients had increased over the years. The tooth color restorations like indirect composite and All ceramics play a major role in fulfilling the esthetic demands.[1,2] The use of All ceramics has increased due to its esthetics, color stability, and biocompatibility, but it was not indicated for long span bridges until the introduction of zirconia. Yttria stabilized zirconia solved the issues of All ceramic crown fracture in high-stress regions of the dental arch.[3,4] According to Millennium Research Group, it has been estimated that there would be an increase in the use of All ceramic crowns from 40% to almost 70% by 2015.
The weakest link in the fixed partial denture treatment is the tooth-restorative margin interface. The marginal fit is a crucial factor needed for long term success. Poor fit may cause dissolution of cement, percolation of fluid leading to secondary caries. Studies by Sailer et al. in 2006 and 2007 stated that All ceramic restorations failed by 10.9% and 21.7% due to secondary caries.[5,6,7] McLean has given a clinically acceptable, marginal fit to be within 120 μm.[8] The advent of CAD CAM systems using optical scanning and computerized processing produces an excellent fit and adaptation. Systems milling partially sintered zirconia could produce marginal values of 34–78 μm.[9,10] This value very well narrows down the marginal adaptation.
Digitalization in prosthodontics has paved the way for new generation ceramics with unprecedented strength and performance. The aim of this study is to compare the internal adaptation and marginal fit of All ceramic systems IN LAB MCXL (Sirona Co; New York, USA) and CERAMILL (Amann Girbach Co.; Austria). CEREC 1 was introduced mainly for inlays, CEREC 2 (1994) and CEREC 3 (2000) has been introduced latter were producing all ceramic crowns with good marginal fit and adaptation.[11,12] CERAMILL is another CAD CAM system, which has been widely used in labs because of cost effectiveness. There is no evidence of direct comparison of these two systems in the literature available till date on marginal fit and internal adaptation using the same methodology. Hence, an in vitro study was planned with the research hypothesis stating that “Will Ceramill (Amann Girbach Co.; Austria) CAD CAM zirconia copings have better marginal fit and internal adaptation than CEREC in lab MC XL (Sirona) CAD CAM zirconia copings?” The null hypothesis is that there will be no difference in marginal fit and internal adaptation between CERAMILL and CEREC in lab MC XL CAD CAM zirconia copings.
MATERIALS AND METHODS
Sample preparation
An in vitro study was planned to check both the marginal fit and internal adaptation of the systems in typhodont tooth. 20 identical samples of typodont mandibular first molar (Nissin Co., Kyoto, Japan) were taken. Sample size calculation was done using the formula from the standard deviations taken from the previous studies with the power of the study at 80% with a confidence interval of 95%.[13] The P value set at 0.05 for the study. Putty indices (Affinis, Coltene Whaledent, Switzerland) of the tooth were made to assess the amount of tooth reduction. Tooth preparation design was planned with occlusal reduction of 1.5 mm at the center with axial reduction of 1 mm to maintain an axial height of 4 mm throughout. The total occlusal convergence of 10° was planned with 1 mm wide smooth continuous radial shoulder[13] [Figure 1]. The tooth preparations were standardized using a Milling Unit (Dentsply Ceramco, York) with a micro motor handpiece (Marathon Co.; Wausau, USA) was suspended from the arm of the surveyor [Figure 2]. The samples were stabilized by embedding them in plaster (White gold plaster, Asian Co., India) bases. All the samples were reduced occlusally by 1.5 mm with an airotor handpiece (NSK Co., Japan) using diamond bur (ISO 289/014) (MANI Co., Japan) and checked with putty index. Samples were then milled in the milling unit to get a uniform axial reduction, height, and taper. All the 20 samples thus had uniform margin, and the occlusal reduction was evaluated with putty indices. All the tooth samples were prepared by a single operator to reduce bias.
Figure 1.
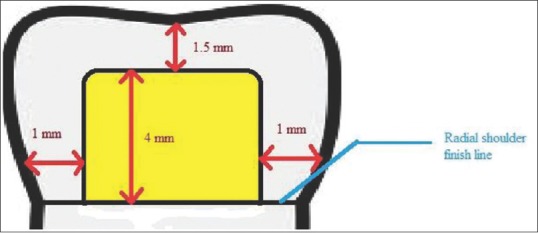
Schematic representation of standardized tooth reduction measurements
Figure 2.

Sample preparation using milling unit
Fabrication of copings
Prepared samples were divided into two groups of 10 each.[13] Group A was selected to receive zirconia copings fabricated by CERAMILL (Amann Girbach Co.; Austria) and Group B received copings fabricated by CEREC in lab MC XL (Sirona Co., New York, USA). The Group A CERAMMIL samples were optically scanned at Vitallium labs Chennai and the digital model was constructed from it. Spacer thickness of 40 μm was adjusted in the system.[14,15] Virtual designing of the coping was then done in the CAD software of CERAMILL. After completion of designing data was then fed into milling unit to get the corresponding copings using Yttria stabilized zirconia blocks from CERAMILL (Ceramill motion). Group B CEREC in lab MC XL samples were scanned at Jays Dental Care; Chennai and virtual models were made. Spacer thickness of 40 μm was maintained as constant here also.[14,15] After designing, data were fed to milling unit and zirconia copings were obtained from CEREC blanks (in coris TZI) [Figure 3]. Following manufacturers instruction[16] Copings were thoroughly dried before sintering for 30 min at 80°C and 10 min at 150°C. Then sintering done at 1510°C for 120 min. Restorations were then cooled to room temperature. Copings were then rechecked for fit with the corresponding samples. Copings were also prepared by a single technician of respective labs to reduce operative bias.
Figure 3.
Computer aided milling in IN LAB MCXL
Luting and embedding of samples
Copings were then luted using type 1 glass ionomer cement (GC Co., Tokyo Japan). After luting, samples were held with hand pressure for 5 min[17] [Figure 4]. Moulds [Figure 5] were prepared using putty for embedding the samples in the clear self-cure acrylic resin (DPI Co.; Mumbai, Maharashtra, India). Putty Molds for the blocks were half filled with self-cure acrylic and samples were placed on the resin and moulds were completely filled with self-cure clear acrylic resin, taking care not to incorporate any air bubbles. After material cures, the embedded blocks were sectioned longitudinally using a diamond disc (Edenta Co.; Switzerland) under running water coolant.
Figure 4.

Luting of sample with finger pressure
Figure 5.

Mold with embedded sliced sample
Measurement of discrepancies
The sliced sample was then viewed under × 100 stereomicroscope (Hitachi HV C10; Japan). The images were stored digitally. Digital images were analyzed using ImageScope software [Figure 6] (Aperio Healthcare Solutions, Vista, CA, USA) for measuring marginal fit and internal adaptation at 15 points measured on each sample.[18,19] Known axial wall length of 4 mm was used to calibrate the readings obtained from samples. Marginal fit was seen along internal and external margins. Internal adaptation was seen along five points each along the mesial wall, distal wall and occlusal surface. Total of 15 points were measured and readings were tabulated[19] [Figure 7]. The normality of the data was checked by Kolmogrov–Smirov test, and found to be normal and unpaired t-test analysis was done.
Figure 6.
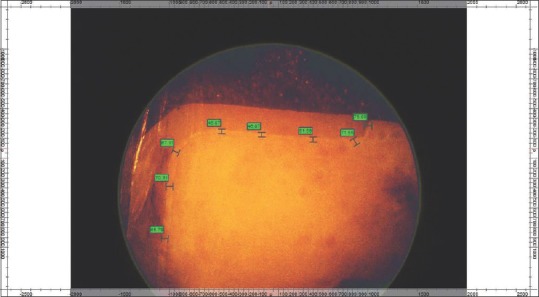
Zone of margins under magnification in ImageScope software
Figure 7.
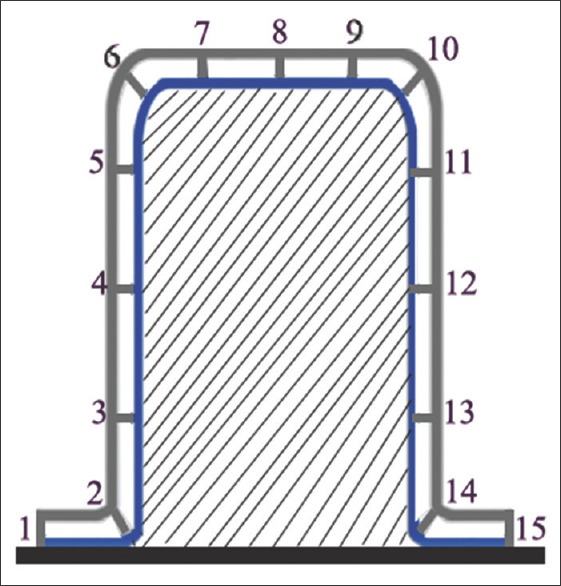
Schematic representation of 15 points measured
RESULTS
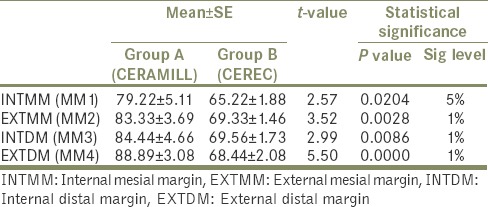
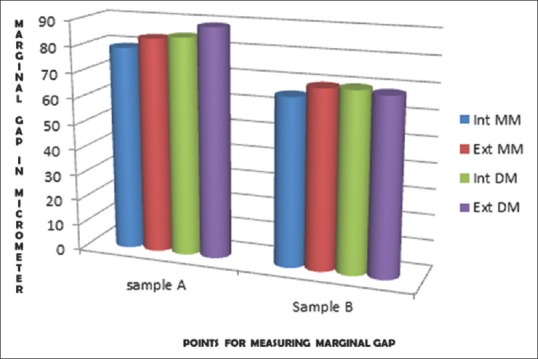
Mean marginal discrepancy was measured along mesial and distal margins on internal and external surface [Figure 8]. Mesial marginal discrepancy on the external surface for CEREC-In Lab MCXL and CERAMILL is 83.33 μm and 69.33 μm, respectively. A mesial marginal discrepancy on the internal surface for CEREC-In Lab MCXL and CERAMILL is 79.22 μm and 65.22 μm respectively. Distal marginal discrepancy on the external surface for CEREC-In Lab MCXL and CERAMILL is 88.89 μm and 68.44 μm respectively. Distal marginal discrepancy on the internal surface for CEREC-In Lab MCXL and CERAMILL is 84.44 μm and 69.56 μm. The overall P value for the marginal discrepancy is 0.008, which is statistically significant [Table 1].
Figure 8.
Marginal adaptation of samples A and B
Table 1.
Difference in marginal fit values of group A and group B in μm
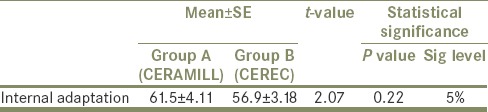
Internal adaptation was measured along 15 points. The averages of 15 points were calculated for every sample [Table 2]. The overall internal adaptation is 56.9 μm In Lab MCXL (sirona) and CERAMILL 61.5 μm (Aman). P =0.022 (P < 0.05) is relatively significant [Figure 9 and Table 3].
Table 2.
Average values of internal adaptation of group A and B samples in μm
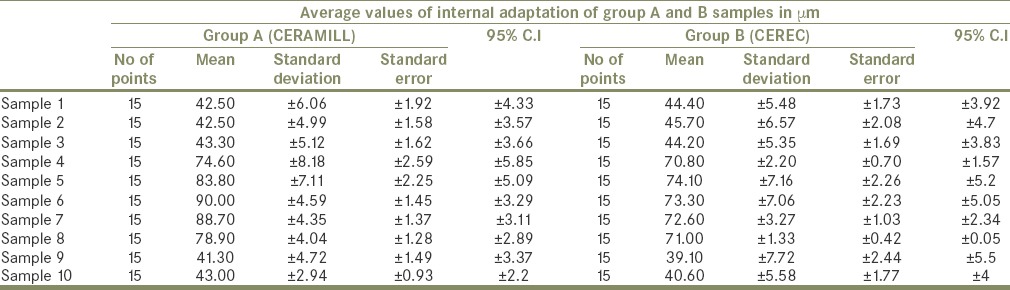
Figure 9.
Internal fit values of sample A and B
Table 3.
Difference in internal adaptation of samples group A and group B in μm
DISCUSSION
Contrepois et al.[20] in their systematic review on All ceramic crowns stated the three main factors, which determine the success of an all ceramic restoration namely, esthetic value, resistance to fracture and third being the marginal fit. The results of our study revealed the fact that “CEREC-In Lab MCXL copings had better adaptation than CERAMILL”, thereby rejecting our null hypothesis. Our study intended to check the marginal discrepancy and internal adaptation in commonly used CAD CAM systems. The marginal adaptation of CEREC-In Lab MCXL (68 μm) was found to be superior than CERAMILL (83 μm) (P < 0.005). The mean internal adaptation of CERAMILL is 61.5 μm and the mean internal adaptation of CEREC-In Lab MCXL is 56.9 μm and the difference is just 1.6 μm between the two systems. But, the statistical range (max value-min value) of the data obtained in the CERAMILL group 49 μm (90–41 μm) was greater than the CEREC-In Lab MCXL group 33 μm (74–39 μm), this result shows that CEREC-In Lab MCXL is definitely better than CERAMILL. The occlusal adaptation discrepancy between both the systems was mainly attributed to the construction of the optical image on scanning.[21] CEREC-In Lab MCXL used a red light scan with a fixed light source and adjustable object to capture different areas, which are not perfectly scanned during initial scanning. On the contrary, CERAMILL used a blue light in a closed chamber with the movable light source. Since the object is not movable in CERAMILL, scanning of CEREC-In Lab MCXL system proved to be better. Both CEREC-In Lab MCXL and CERAMILL used presintered blanks for fabrication of coping, which when sintered resulted in densely packed zirconia. The balance between the shrinkage of the presintered blanks and the final sintered zirconia (amount of shrinkage) was found to be a critical factor in determining the marginal fit and internal adaptation. Studies indicate that CEREC-In Lab MCXL systems have better balance during sintering and hence may be a reason to produce copings with a better fit.[12]
McLean and von Fraunhofer stated clinically accepted marginal discrepancy for all ceramic crown is 120 μm and marginal gap < 80 μm will not be visible in the oral environment.[8] No direct comparisons of CEREC-In Lab MCXL and CERAMILL with the same methodology have been reported in the literature. Only one previous study was reported in the literature with CERAMILL by Grenade et al.,[22] to check the marginal fit which was around 81 μm in their study and is nearly equal to our results (85 μm). However, Grenade et al.[22] tested only the marginal fit, whereas internal adaptation was not tested. Att et al.,[12] in their study reported that mean marginal discrepancy for CEREC-In Lab MCXL was 64 μm, which is in accordance with our study (68 μm).
Nakamura et al.[23] in his study concluded that when die spacer was set at 30 μm or 50 μm the marginal gap obtained usually is 53 μm to 67 μm. The study also reported CEREC-In Lab MCXL 3 CAD CAM system was better than PROCERA to produce coping with acceptable fit. Mously et al.[24] compared the marginal fit of heat pressed restorations and CAD CAM copings with 30 μm spacer thickness. IPS e max milling unit was used for lithium disilicate blanks. Heat pressed groups shown a marginal gap of 74.04 μm and 30 μm spacer CAD CAM group showed 90.03 μm. Herera et al.[25] conducted a study comparing marginal leakage in copings fabricated with PROCERA, KaVo, and CEREC-In Lab MCXL in lab systems. CEREC-In Lab MCXL in the lab produced copings with more marginal discrepancy 132.18 μm comparing to 62.58 μm PROCERA and KaVO 65.54 μm. Yucel et al.[26] compared marginal discrepancy of CEREC-In Lab MCXL 3, CELAY, IPS empress, IN CERAM crowns. The readings were measured on master steel die. CEREC-In Lab MCXL 3 Marginal gaps were recorded as 47.4 μm. CELAY system recorded with least value of 27.8 μm and in ceram system recorded with higher marginal values of 94.9 μm.
In order to assess the precision of fabrication of systems, in terms of marginal fit and internal adaptation, comparing the zirconia copings were found to be more reliable than on veneered zirconia copings since it is not influenced by veneering condition.[27] However, to check the clinical performance the veneered zirconia must be compared for the marginal fit and internal adaptation. The number of measured sites for internal adaptation was initially suggested to be taken as 50 points by Groten et al. in 2000, but his statement was contradicted by the works of Gassino et al.,[28] which stated that just 18 measure points were necessary for laboratory prepared abutments which were close to the number of points taken in our study.
Clinical inference in both the systems produced crown with acceptable marginal fit and internal adaptation. When comparing the marginal fit, 14 μm more gaps was found in CERAMILL which is less costlier than CEREC-In Lab MCXL. Even though the cost of CERAMILL is less and the marginal discrepancy is 14 μm but internal adaptation plays an important role in retention. Restorations may fail because of poor internal adaptation even after proper geometric preparation of tooth. The marginal discrepancies can be present in horizontal and vertical discrepancies. The horizontal discrepancies can be easily corrected with grinding while vertical discrepancies cannot be compensated as it is directly proportional to exposure of luting cements which lead to cement dissolution.[29]
Most of the previous studies on marginal fit was done using replica technique, but in order to eliminate those errors while replicating,[13] direct scanning of the typodont was performed which added to the strength of our study. Limitation of the study is that Contrepois et al.[20] has stated that the use of computer X-ray microtomography was recommended for further research on marginal fit. The result of any in vitro study has to be corroborated with clinical studies. To strengthen the validity of our results future randomized control trials comparing these two CAD CAM systems need to be studied.
CONCLUSION
The marginal adaptation of CEREC-In Lab MCXL (68 μm) is found to be superior than CERAMILL (83 μm) (P < 0.05)
Both the CEREC-In Lab MCXL and CERAMILL copings demonstrated internal adaptation and marginal fit within the acceptable clinical range
When corroborating both the internal adaptation and marginal fit, CEREC-In Lab MCXL was found to be better than CERAMILL.
Footnotes
Source of Support: Nil
Conflict of Interest: None.
REFERENCES
- 1.Krishna J, Kumar S, Savadi RV. Evolution of metal free ceramics. J Indian Prosthodont Soc. 2009;9:70–5. [Google Scholar]
- 2.Conrad HJ, Seong WJ, Pesun IJ. Current ceramic materials and systems with clinical recommendations: A systematic review. J Prosthet Dent. 2007;98:389–404. doi: 10.1016/S0022-3913(07)60124-3. [DOI] [PubMed] [Google Scholar]
- 3.Haselton DR, Diaz-Arnold AM, Hillis SL. Clinical assessment of high-strength all-ceramic crowns. J Prosthet Dent. 2000;83:396–401. doi: 10.1016/s0022-3913(00)70033-3. [DOI] [PubMed] [Google Scholar]
- 4.Gemalmaz D, Ergin S. Clinical evaluation of all-ceramic crowns. J Prosthet Dent. 2002;87:189–96. doi: 10.1067/mpr.2002.120653. [DOI] [PubMed] [Google Scholar]
- 5.Sailer I, Fehér A, Filser F, Gauckler LJ, Lüthy H, Hämmerle CH. Five-year clinical results of zirconia frameworks for posterior fixed partial dentures. Int J Prosthodont. 2007;20:383–8. [PubMed] [Google Scholar]
- 6.Sailer I, Fehér A, Filser F, Lüthy H, Gauckler LJ, Schärer P, et al. Prospective clinical study of zirconia posterior fixed partial dentures: 3-year follow-up. Quintessence Int. 2006;37:685–93. [PubMed] [Google Scholar]
- 7.Jacobs MS, Windeler AS. An investigation of dental luting cement solubility as a function of the marginal gap. J Prosthet Dent. 1991;65:436–42. doi: 10.1016/0022-3913(91)90239-s. [DOI] [PubMed] [Google Scholar]
- 8.Gonzalo E, Suárez MJ, Serrano B, Lozano JF. A comparison of the marginal vertical discrepancies of zirconium and metal ceramic posterior fixed dental prostheses before and after cementation. J Prosthet Dent. 2009;102:378–84. doi: 10.1016/S0022-3913(09)60198-0. [DOI] [PubMed] [Google Scholar]
- 9.Schaefer O, Watts DC, Sigusch BW, Kuepper H, Guentsch A. Marginal and internal fit of pressed lithium disilicate partial crowns in vitro: A three-dimensional analysis of accuracy and reproducibility. Dent Mater. 2012;28:320–6. doi: 10.1016/j.dental.2011.12.008. [DOI] [PubMed] [Google Scholar]
- 10.Kohorst P, Junghanns J, Dittmer MP, Borchers L, Stiesch M. Different CAD/CAM-processing routes for zirconia restorations: Influence on fitting accuracy. Clin Oral Investig. 2011;15:527–36. doi: 10.1007/s00784-010-0415-9. [DOI] [PubMed] [Google Scholar]
- 11.Mörmann WH. The evolution of the CEREC system. J Am Dent Assoc. 2006;137(Suppl):7S–13. doi: 10.14219/jada.archive.2006.0398. [DOI] [PubMed] [Google Scholar]
- 12.Att W, Komine F, Gerds T, Strub JR. Marginal adaptation of three different zirconium dioxide three-unit fixed dental prostheses. J Prosthet Dent. 2009;101:239–47. doi: 10.1016/S0022-3913(09)60047-0. [DOI] [PubMed] [Google Scholar]
- 13.Baig MR, Tan KB, Nicholls JI. Evaluation of the marginal fit of a zirconia ceramic computer-aided machined (CAM) crown system. J Prosthet Dent. 2010;104:216–27. doi: 10.1016/S0022-3913(10)60128-X. [DOI] [PubMed] [Google Scholar]
- 14.Olivera AB, Saito T. The effect of die spacer on retention and fitting of complete cast crowns. J Prosthodont. 2006;15:243–9. doi: 10.1111/j.1532-849X.2006.00113.x. [DOI] [PubMed] [Google Scholar]
- 15.Psillakis JJ, McAlarney ME, Wright RF, Urquiola J, MacDonald DE. Effect of evaporation and mixing technique on die spacer thickness: A preliminary study. J Prosthet Dent. 2001;85:82–7. doi: 10.1067/mpr.2001.113028. [DOI] [PubMed] [Google Scholar]
- 16. [Last cited on 2015 Mar 30]. Available from: http://www.td.sirona.com/pdf/6359801.pdf .
- 17.White SN, Yu Z, Kipnis V. Effect of seating force on film thickness of new adhesive luting agents. J Prosthet Dent. 1992;68:476–81. doi: 10.1016/0022-3913(92)90414-6. [DOI] [PubMed] [Google Scholar]
- 18.Sorensen JA. A standardized method for determination of crown margin fidelity. J Prosthet Dent. 1990;64:18–24. doi: 10.1016/0022-3913(90)90147-5. [DOI] [PubMed] [Google Scholar]
- 19.Holmes JR, Bayne SC, Holland GA, Sulik WD. Considerations in measurement of marginal fit. J Prosthet Dent. 1989;62:405–8. doi: 10.1016/0022-3913(89)90170-4. [DOI] [PubMed] [Google Scholar]
- 20.Contrepois M, Soenen A, Bartala M, Laviole O. Marginal adaptation of ceramic crowns: A systematic review. J Prosthet Dent. 2013;110:447–54.e10. doi: 10.1016/j.prosdent.2013.08.003. [DOI] [PubMed] [Google Scholar]
- 21.Martins LM, Lorenzoni FC, Melo AO, Silva LM, Oliveira JL, Oliveira PC, et al. Internal fit of two all-ceramic systems and metal-ceramic crowns. J Appl Oral Sci. 2012;20:235–40. doi: 10.1590/S1678-77572012000200019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Grenade C, Mainjot A, Vanheusden A. Fit of single tooth zirconia copings: Comparison between various manufacturing processes. J Prosthet Dent. 2011;105:249–55. doi: 10.1016/S0022-3913(11)60040-1. [DOI] [PubMed] [Google Scholar]
- 23.Nakamura T, Dei N, Kojima T, Wakabayashi K. Marginal and internal fit of Cerec 3 CAD/CAM all-ceramic crowns. Int J Prosthodont. 2003;16:244–8. [PubMed] [Google Scholar]
- 24.Mously HA, Finkelman M, Zandparsa R, Hirayama H. Marginal and internal adaptation of ceramic crown restorations fabricated with CAD/CAM technology and the heat-press technique. J Prosthet Dent. 2014;112:249–56. doi: 10.1016/j.prosdent.2014.03.017. [DOI] [PubMed] [Google Scholar]
- 25.Herera M, Catalan A, Flores M, Martinez A. Marginal discrepancy and microleakage in crown-copings fabricated by three CAD/CAM systems: An in vitro study. Open J Stomatol. 2012;2:163–9. [Google Scholar]
- 26.Yucel MT, Aynekat F, Avunduk M. In vitro evaluation of the marginal fit of different all-ceramic crowns. J Dent Sci. 2013;8:225–30. [Google Scholar]
- 27.Martínez-Rus F, Suárez MJ, Rivera B, Pradíes G. Evaluation of the absolute marginal discrepancy of zirconia-based ceramic copings. J Prosthet Dent. 2011;105:108–14. doi: 10.1016/S0022-3913(11)60009-7. [DOI] [PubMed] [Google Scholar]
- 28.Gassino G, Barone Monfrin S, Scanu M, Spina G, Preti G. Marginal adaptation of fixed prosthodontics: A new in vitro 360-degree external examination procedure. Int J Prosthodont. 2004;17:218–23. [PubMed] [Google Scholar]
- 29.Ng J, Ruse D, Wyatt C. A comparison of the marginal fit of crowns fabricated with digital and conventional methods. J Prosthet Dent. 2014;112:555–60. doi: 10.1016/j.prosdent.2013.12.002. [DOI] [PubMed] [Google Scholar]