

A large general population sample completed an n-back task online. Those who were in pain made more false alarms than those who were pain free.
Keywords: Cognition, Attention, Working memory, Updating, Internet study
Abstract
Pain captures attention, displaces current concerns, and prioritises escape and repair. This attentional capture can be measured by its effects on general cognition. Studies on induced pain, naturally occurring acute pain, and chronic pain all demonstrate a detrimental effect on specific tasks of attention, especially those that involve working memory. However, studies to date have relied on relatively small samples and/or one type of pain, thus restricting our ability to generalise to wider populations. We investigated the effect of pain on an n-back task in a large heterogeneous sample of 1318 adults. Participants were recruited from the general population and tested through the internet. Despite the heterogeneity of pain conditions, participant characteristics, and testing environments, we found a performance decrement on the n-back task for those with pain, compared with those without pain; there were significantly more false alarms on nontarget trials. Furthermore, we also found an effect of pain intensity; performance was poorer in participants with higher intensity compared with that in those with lower intensity pain. We suggest that the effects of pain on attention found in the laboratory occur in more naturalistic settings. Pain is common in the general population, and such interruption may have important, as yet uninvestigated, consequences for tasks of everyday cognition that involve working memory, such as concentration, reasoning, motor planning, and prospective memory.
1. Introduction
Beyond debate is the function of pain to alter behaviour by imposing an alarming motivational priority of escape, avoidance, or succour.16 What is debatable is the “cost” of attentional capture by pain. Pain is a quotidian experience.25,26 Perhaps equally common is the natural repair of attention in the maintenance of coherent behaviour. Pain is part of a general danger detection system. To be interrupted by pain is normal. Therefore, perhaps also normal is the fast recovery from interruption. Maybe, we are so good at recovery that such aversive interruption does not affect performance, except in the laboratory. Equally possible, however, is that pain has a cost so common that it goes largely unrecognised.
The effects of pain on cognition have been documented with laboratory-induced pain, naturally occurring acute pain, and chronic pain.1,6,9–12,15,18,20–22,24,28 For example, Moore et al.21 compared the performance of healthy participants on 7 different aspects of attention when participants were pain free and during heat pain induction. They found that pain disrupted working memory updating, attention switching, and divided attention. Similar effects have been found with naturally occurring menstrual pain18 and headache pain.22 A meta-analysis revealed that chronic pain results in less accurate responses on tests of complex executive function and set shifting and slower responses on inhibition, complex executive function, and set-shifting tasks.4
Although there have been many small-sample observations, missing are data from large, heterogeneous, and naturalistic samples of the general population. Most studies on pain-related interference have homogenous samples and tightly controlled laboratory conditions. While these characteristics are essential in establishing effects, it is now necessary to investigate whether the effects of pain on cognition are stable across different groups and in more naturalistic settings, sacrificing control over pain induction for scale, heterogeneity, and self-reported pain experience. Our aim was to investigate the effect of pain on working memory in a large heterogeneous general population sample recruited and tested on the internet, with participants experiencing a variety of pain states (eg, transient, acute, chronic, no pain) (see Ref. 5 for a similar method). If the effects of pain on working memory are reliable and significant in day-to-day life, we would expect to see them even in less controlled environments such as this.
We predicted that participants who were in pain at the time of the study would have lower accuracy and slower reaction times (RTs) on a working memory task than pain-free individuals. We included sex and age in this analysis to investigate the generalisability of the effects across the sample. Given that women report a greater impact of pain on their lives than do men,17 women may also show larger effects of pain on attention. Furthermore, we predicted that within the pain group, high-intensity pain would be associated with lower accuracy and slower RTs than low-intensity pain. We also examined the effect of the type of pain that participants experienced and whether it was acute or chronic.
2. Methods
2.1. Participants
A general population sample was recruited to complete a letter n-back task and a series of questionnaires online. The inclusion criteria were that participants had to be aged 18 or over and with access to an internet-enabled laptop or desktop computer. We did not restrict or control recruitment in any other way. One thousand five hundred participants were accessed through Amazon Mechanical Turk (MTurk; www.MTurk.com). MTurk is an open online marketplace for recruiting individuals to complete tasks for a small fee and can be used to obtain high-quality reliable research data quickly and inexpensively.7,23 Participants recruited through MTurk were paid $1 for their participation. Previous research suggests that participants recruited through MTurk are often internally motivated.7 An additional 199 participants were accessed through forums, websites, and pain-related discussion groups that hosted a link to the web experiment. Participants recruited outside of MTurk did not receive $1 for their participation. At the end of the study, participants were provided with links to other websites where they could complete similar tasks in the form of games, to discourage repeat submissions.
Of the 1699 participant entries, 20 participants were identified as having 2 submissions each. In these cases, only the first submission was included, and the 20 duplicate submissions were excluded. This left 1679 unique data submissions. Of these 1679 submissions, 15 were from individuals who did not give consent to take part and did not progress past the information and consent page. One further participant reported their age as 17 and was excluded. Participants who indicated that they did not want to seriously participate (N = 18) and those who did not report whether or not they were currently in pain (an additional 8 participants) were also excluded, leaving a total of 1637 participants. Sociodemographic and pain-related information of this sample is presented in Tables 1 and 2.
Table 1.
Sociodemographic characteristics of the sample.
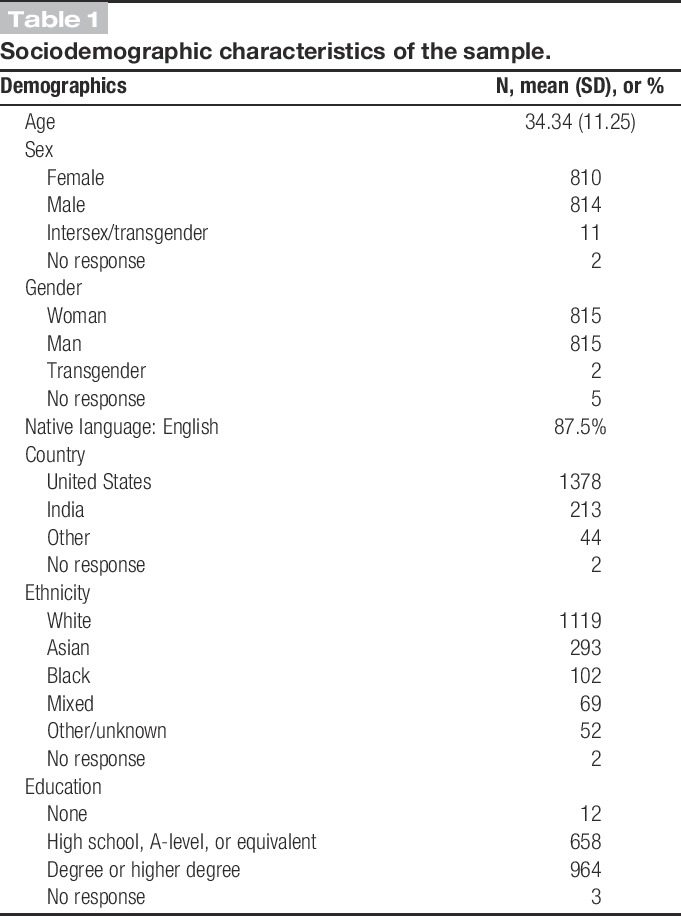
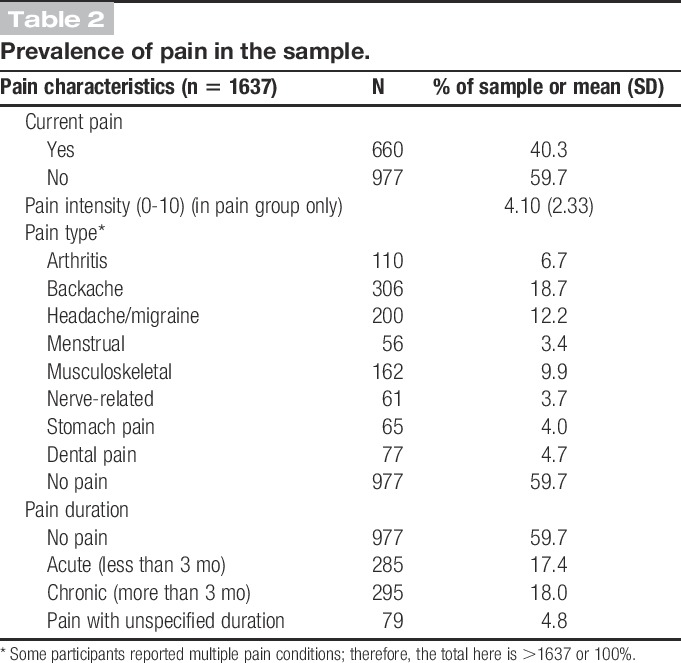
Table 2.
Prevalence of pain in the sample.
2.2. Measures
2.2.1. Seriousness check
The use of seriousness checks in online research is recommended to improve data validity by identifying nonserious submissions.3 Therefore, before completing the experiment, participants were asked to indicate whether they were seriously participating or just browsing the study pages. To further confirm whether participants had taken participation seriously, participants were also asked to report whether they had answered the questions honestly (yes [N = 1462], mostly yes [N = 56], mostly no [N = 4], no [N = 1], missing data [N = 111]) at the end of the experiment.
2.2.2. Demographics
Participants were asked to provide demographic information including age, sex, native language, country of residence, ethnicity, and level of education.
2.2.3. Pain status
To ascertain current pain, participants were asked to indicate whether or not they were currently in any pain and the intensity of this pain on a 21-point scale labelled 0 “no pain at all” to 10 “pain could not be worse” (with non-numbered midpoints available between each number). Participants were asked to indicate the type(s) of pain they were experiencing by selecting any applicable items from a list or entering any other condition in a free text box. They were also asked to report the duration of their current pain using a free text box, and responses were coded as acute (<3 months) or chronic (>3 months). These data are summarised in Table 2. Some details about pain diagnosis, analgesic treatment, and coping mechanisms were also requested. However, because of the study being conducted online, we aimed to keep it as short as possible and we did not assess non-pain-related health factors.
2.2.4. n-back task
The n-back task is a measure of working memory updating that has been shown to be sensitive to the effects of experimental pain6,21 and naturally occurring pain.18,22 The current experiment used a 2-back version of the n-back task. During this task, participants were presented with a stream of 90 letters (all of the consonants were included except “Y”), which appeared one at a time in the centre of their computer monitor. The letters were capitalised and appeared in black Arial font on a white background. The size of the letters was 20% of the monitor height. Each letter was presented for 500 milliseconds, followed by a 1500-millisecond blank screen. Participants were instructed to report whether the letter currently on screen matched the letter presented 2 letters back; they indicated their response using 2 separate keys (0 and 1) on their computer keyboard. The task included 30 target stimuli and 60 nontarget stimuli presented in a random order.
2.2.5. Experience of cognitive intrusion of pain
Participants completed the Experience of Cognitive Intrusion of Pain Scale2 to measure the phenomenology of cognitive intrusion from pain. These data are not relevant to our current research questions and are reported elsewhere.2
2.2.6. Environment
Participants were not instructed to complete the study under any specific conditions, but they were asked a series of questions regarding the environment in which they completed it. They were asked to indicate where they completed the study (home [N = 1376], work [N = 112], internet cafe [N = 8], library [N = 17], public transport [N = 1], outdoors [N = 3], other [N = 4]), whether they were interrupted during the study (no [N = 1404], once [N = 106], a few times [N = 24], repeatedly [N = 4]), and the amount of noise in their environment on a scale of 0 (silent) to 10 (very noisy; M = 1.36, SD = 1.89).
2.3. Procedure
The study was approved by the Departments of Psychology and Health Ethics Boards at the University of Bath. Participants were directed to the study web pages through MTurk, pain discussion forums, or other online advertisements. The study was presented to participants using Inquisit 4 Web,14 which provides millisecond accuracy for stimulus presentation and response timing.13 Minimum system requirements are needed to be able to run the programme, including Windows XP or Mac OS X 10.6, Pentium 166 MHz processor, 10 MB of available hard disk space, and DirectX-compatible Super VGA graphics system. The study began with an information and consent page. Participants were required to check a box and click next if they consented to take part or to exit the programme if they did not consent. Participants who gave consent then completed the following sections in order: questions on demographics, pain questions, Experience of Cognitive Intrusion of Pain Scale, n-back task, and environment questions. Finally, participants saw a debrief page and received a completion code for the MTurk payment system. The experiment took approximately 10 to 15 minutes to complete, and responses were anonymous. Participants were able to withdraw at any time.
2.4. Analysis
Sex differences in the prevalence of pain were investigated using a χ2 test. The relationship between age and pain prevalence was investigated using a logistic regression analysis. The relationship between pain and n-back task performance (measured by number of hits, number of correct rejections, hit RTs, and correct rejection RTs) was investigated with 3 analyses: (1) an examination of the main and interactive effects of pain, sex, and age on n-back performance using a 2 (Pain: present, absent) × 2 (Sex: female, male) analysis of covariance with age as a covariate; (2) a correlation between pain intensity and n-back accuracies and RTs within the pain group; (3) an investigation of the effects of pain type and duration on n-back performance using a 6 (Pain Group: arthritis only, backache only, headache and migraine only, musculoskeletal pain only, multiple pain conditions, and “other” pain conditions) × 2 (Pain Duration: acute, chronic) analysis of variance (ANOVA) (age and sex are not included here due to small cell sizes).
3. Results
3.1. Environmental effects and data cleaning
Of the 1637 participants who started the study, 94 did not complete the n-back task. For the remaining 1543 participants who did complete the n-back task, the relationship between task performance and participants' environments was investigated using 2 regression models with 5 independent variables: noise, interruptions, location (eg, home, work), honesty, and effort, one model to predict number of hits and one to predict number of correct rejections. Number of hits was significantly predicted by the model, R2 = 0.044, F(5,1503) = 13.70, P < 0.001, and 3 predictors were significant: interruptions, β = −0.093, P = 0.001, honesty, β = −0.100, P < 0.001, and effort, β = 0.124, P < 0.001. Number of hits was not predicted by noise, β = 0.049, P = 0.095, or location, β = −0.017, P = 0.515. Number of correct rejections was also significantly predicted by the model, R2 = 0.037, F(5,1503) = 11.41, P < 0.001, and the same 3 predictors were significant: interruptions, β = −0.073, P = 0.010, honesty, β = −0.108, P < 0.001, and effort, β = 0.096, P = 0.001. Again, correct rejections were not predicted by noise, β = 0.018, P = 0.528, or location, β = 0.042, P = 0.097.
Based on these findings, participants were excluded if they reported that they were interrupted from their environment during the study a few times or constantly (N = 28), if they reported that they did not answer the study questions honestly (N = 5), if they rated their effort on the n-back task as lower than 5 of 10 (N = 14), if they did not provide answers to these questions (N = 12), or if their performance on the n-back task was not significantly above chance level on both target and nontarget trials, suggesting that they did not understand the task, were guessing, were responding randomly, or were simply unable to perform the task (N = 166). To test for bias in which participants performed above chance level, we examined the demographic characteristics of participants who were significantly above chance level on the n-back task and those who were not using χ2 tests. There was no evidence of dependency between above chance performance and presence/absence of pain, χ2(1) = 0.04, P = 0.851, or between above chance performance and type of pain, χ2(6) = 11.00, P = 0.089. However, above chance performance did differ by sex, χ2(1) = 6.48, P = 0.011, with more males (90.8%) than females (86.6%) scoring above chance level. Participants who did not perform significantly above chance rated their effort on the n-back task as 9.20 of 10 and those who scored above chance level rated their effort as 9.33 of 10, which were not significantly different, t(1482) = 1.51, P = 0.132, d = 0.11. Of note, participants who were in pain and those who were not were similar in the amount of effort they reported dedicating to the n-back task, t(1316) = 1.26, P = 0.207, d = 0.07, background noise, t(1316) = 0.09, P = 0.929, d = 0.01, interruptions, t(1316) = 0.89, P = 0.374, d = 0.08, and honesty, t(1316) = 1.39, P = 0.165, d = 0.12.
These exclusion criteria left 1318 participants for the analysis, 534 of whom were in pain and 784 of whom were not in pain. For analyses including Sex, we limited the sample to participants reporting that they were male or female and excluded those reporting that they were intersex or transgender due to small cell counts. For these analyses, the sample size was 1308, with 530 participants in pain and 778 participants not in pain.
The RT data were screened for extreme values. There were no anticipation RTs (shorter than 300 milliseconds). Because response times had an upper limit of 2500 milliseconds, none were removed from the upper end. For trials where a participant failed to respond (8.55% of all trials), their RT was removed and their accuracy was coded as incorrect. Mean RTs for each participant were also examined for outliers. This led to 9 participants being excluded from the analyses of hit RTs and 13 being excluded from the analyses of correct rejection RTs. However, these participants' accuracy data were retained. As such, the sample size for RT analyses was slightly smaller than for accuracy analyses.
3.2. Demographics and pain prevalence
Demographics for the final sample are presented in Table 1, and pain characteristics of the sample are presented in Table 2. Sex differences in the prevalence of pain were investigated using a χ2 test, which revealed that, as expected,17 more women (49%) than men (33%) reported that they were in pain, χ2(1) = 33.94, P < 0.001. Within the group of participants who were in pain, there was no sex difference for the intensity of pain reported, t(528) = 1.37, P = 0.171 (males: M = 7.47, SD = 4.60; females: M = 8.02, SD = 4.51).
A logistic regression also showed that pain was more common in older participants than in younger participants, Wald = 30.45, Exp(B) = 1.03, P < 0.001. For every 1-year increase in age, participants were 1.03 times more likely to report pain.
3.3. n-back task performance
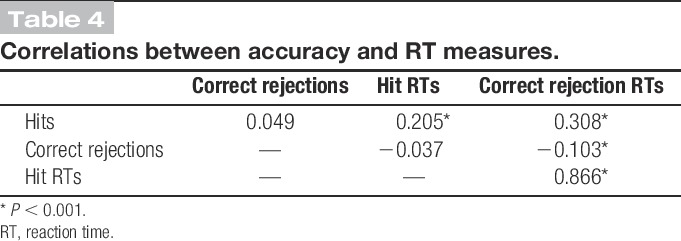
Table 3 shows mean accuracy and RTs for each type of trial (target and nontarget) and each type of response (target hits, target misses, nontarget correct rejections, and nontarget false alarms) in the pain and no pain groups. Table 4 shows the correlations between the 4 outcome measures used below. The number of hits and correct rejections that participants scored were not correlated. Next, we present the analyses of the relationship between pain and performance on the n-back task.
Table 3.
Mean accuracy and RT scores on the n-back task in the pain and no pain groups.

Table 4.
Correlations between accuracy and RT measures.
3.3.1. Effects of pain, sex, and age on number of hits
For number of hits, there were no significant main effects or interactions (all Ps > 0.084).
3.3.2. Effects of pain, sex, and age on number of correct rejections
For number of correct rejections, there was a main effect of Pain, F(1,1299) = 5.99, P = 0.015,  = 0.005, with participants who reported pain scoring lower (M = 85.12%, SD = 17.83%) than those who reported no pain (M = 88.50%, SD = 14.62%) (Fig. 1). There was a significant interaction between Sex and Age, F(1,1299) = 4.98, P = 0.026,
= 0.005, with participants who reported pain scoring lower (M = 85.12%, SD = 17.83%) than those who reported no pain (M = 88.50%, SD = 14.62%) (Fig. 1). There was a significant interaction between Sex and Age, F(1,1299) = 4.98, P = 0.026,  = 0.004. In women, there was a significant negative correlation between age and number of correct rejections, r(635) = 0.12, P = 0.003, whereas in men, there was no correlation between age and number of correct rejections, r(672) < 0.001, P = 1.00, and these correlations were significantly different, z = −2.17, P = 0.030. All other effects were nonsignificant; pain did not interact with sex or age.
= 0.004. In women, there was a significant negative correlation between age and number of correct rejections, r(635) = 0.12, P = 0.003, whereas in men, there was no correlation between age and number of correct rejections, r(672) < 0.001, P = 1.00, and these correlations were significantly different, z = −2.17, P = 0.030. All other effects were nonsignificant; pain did not interact with sex or age.
Figure 1.
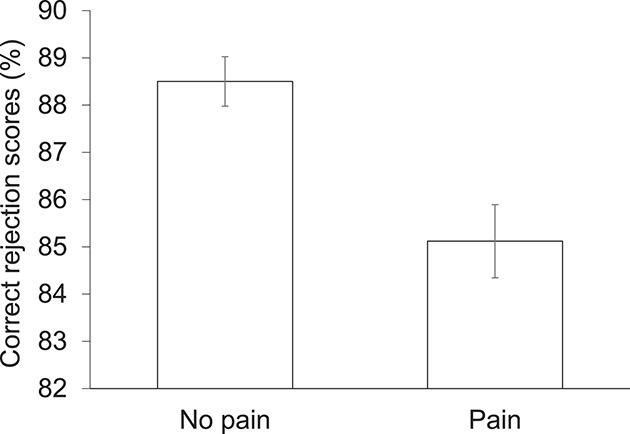
Correct rejection scores in the pain and no pain groups. Error bars reflect ±1 SEM.
Overall, participants in pain were more likely to mistake nontargets for targets (ie, have more false alarms). This could be because they genuinely believed they were targets or it could be that participants in pain were more likely to select the “target” option when unsure. To discriminate between these hypotheses, we compared RTs for false alarms on nontarget trials with RTs for hits on target trials using a 2 (Trial Type) × 2 (Pain) ANOVA. To support the first hypothesis, we would expect the RTs to be similar across trial types in participants with pain. To support the second hypothesis, we would expect RTs for false alarms to be longer than RTs for hits in participants with pain. Our analysis revealed a main effect of Trial Type on RTs, F(1,1200) = 6.66, P = 0.010,  = 0.006, with false alarms (M = 1222, SD = 217) taking longer than hits (M = 1210, SD = 180) (note that the sample size here is slightly smaller than that in other RT analyses because some participants did not make any false alarms, meaning they did not have a false alarm RT score). There was no main effect of pain, F(1,1200) = 2.43, P = 0.120. There was a marginally significant interaction between Trial Type and Pain, F(1,1200) = 2.94, P = 0.087,
= 0.006, with false alarms (M = 1222, SD = 217) taking longer than hits (M = 1210, SD = 180) (note that the sample size here is slightly smaller than that in other RT analyses because some participants did not make any false alarms, meaning they did not have a false alarm RT score). There was no main effect of pain, F(1,1200) = 2.43, P = 0.120. There was a marginally significant interaction between Trial Type and Pain, F(1,1200) = 2.94, P = 0.087,  = 0.002, which was due to longer RTs for false alarms (M = 1216, SD = 219) than for hits (M = 1199, SD = 175) in participants without pain, t(706) = 3.17, P = 0.002, d = 0.09, and no difference in RTs for false alarms (M = 1226, SD = 207) and for hits (M = 1223, SD = 180) in participants with pain, t(494) = 0.62, P = 0.537, d = 0.02. This suggests that in the absence of pain, participants hesitate before making false alarms, but in the presence of pain, they do not. In other words, participants in pain may be more likely to genuinely mistake nontargets for targets than those without pain, although the 2-way interaction did not quite reach significance.
= 0.002, which was due to longer RTs for false alarms (M = 1216, SD = 219) than for hits (M = 1199, SD = 175) in participants without pain, t(706) = 3.17, P = 0.002, d = 0.09, and no difference in RTs for false alarms (M = 1226, SD = 207) and for hits (M = 1223, SD = 180) in participants with pain, t(494) = 0.62, P = 0.537, d = 0.02. This suggests that in the absence of pain, participants hesitate before making false alarms, but in the presence of pain, they do not. In other words, participants in pain may be more likely to genuinely mistake nontargets for targets than those without pain, although the 2-way interaction did not quite reach significance.
3.3.3. Effects of pain, sex, and age on hit reaction times
For hit RTs, there was a significant main effect of Age, F(2,1284) = 48.32, P < 0.001,  = 0.036, with RTs increasing as age increased, r(1292) = 0.23, P < 0.001. There was a significant main effect of sex, with women's RTs (M = 1215.76, SD = 179) being longer than those of men (M = 1202.29, SD = 186). Finally, there was an interaction between Sex and Age, F(1,1284) = 6.43, P = 0.011,
= 0.036, with RTs increasing as age increased, r(1292) = 0.23, P < 0.001. There was a significant main effect of sex, with women's RTs (M = 1215.76, SD = 179) being longer than those of men (M = 1202.29, SD = 186). Finally, there was an interaction between Sex and Age, F(1,1284) = 6.43, P = 0.011,  = 0.005, which was due to a stronger positive correlation between age and hit RTs in women, r(631) = 0.31, P < 0.001, then in men, r(661) = 0.13, P = 0.001, z = 3.44, P < 0.001. All other effects were nonsignificant.
= 0.005, which was due to a stronger positive correlation between age and hit RTs in women, r(631) = 0.31, P < 0.001, then in men, r(661) = 0.13, P = 0.001, z = 3.44, P < 0.001. All other effects were nonsignificant.
3.3.4. Effects of pain, sex, and age on correct rejection reaction times
For correct rejection RTs, there was a significant main effect of Age, F(2,1274) = 47.79, P < 0.001,  = 0.036, with RTs increasing as age increased, r(1282) = 0.22, P < 0.001. There was a significant main effect of sex, with women's RTs (M = 1161, SD = 167) being longer than those of men (M = 1154, SD = 173). Finally, there was an interaction between Sex and Age, F(1,1274) = 5.39, P = 0.020,
= 0.036, with RTs increasing as age increased, r(1282) = 0.22, P < 0.001. There was a significant main effect of sex, with women's RTs (M = 1161, SD = 167) being longer than those of men (M = 1154, SD = 173). Finally, there was an interaction between Sex and Age, F(1,1274) = 5.39, P = 0.020,  = 0.004, which was due to a stronger positive correlation between age and hit RTs in women, r(622) = 0.30, P < 0.001, then in men, r(660) = 0.13, P = 0.001, z = 3.43, P < 0.001. All other effects were nonsignificant.
= 0.004, which was due to a stronger positive correlation between age and hit RTs in women, r(622) = 0.30, P < 0.001, then in men, r(660) = 0.13, P = 0.001, z = 3.43, P < 0.001. All other effects were nonsignificant.
3.3.5. Pain intensity and n-back scores
To examine the influence of pain intensity on n-back performance, we ran a series of correlations between pain intensity and n-back scores within the pain group. There was no relationship between pain intensity and number of hits, r(534) = −0.07, P = 0.132, but there was a significant relationship between pain intensity and number of correct rejections, r(534) = −0.16, P < 0.001. The more intense participants reported their pain to be, the fewer correct rejections (and more false alarms) they made. There was no relationship between pain intensity and hit RTs, r(534) = 0.003, P = 0.949, or correct rejection RTs, r(534) = 0.03, P = 0.558.
3.3.6. n-back performance in different pain conditions and pain durations
Pain reduced the number of correct rejections that participants made, and this effect was correlated with pain intensity. Next, we investigated the effects of the type and duration of pain that participants reported on their n-back performance, using a 6 (Pain Group: arthritis only, backache only, headache and migraine only, musculoskeletal pain only, multiple pain conditions, and other pain conditions) × 2 (Pain Duration: acute, chronic) ANOVA, within those reporting pain. There were no main effects and no interactions for Pain Type or Duration for number of hits, number of correct rejections, hit RTs, or correct rejection RTs, all Ps > 0.143.
4. Discussion
Pain reduces working memory performance. Participants in pain at the time of the study made more errors, more often falsely identifying letters as seen when they had not been presented. This effect of accuracy was consistent across sex and age but sensitive to the intensity of pain experienced; the more intense the pain, the more false alarms participants made. Performance did not significantly differ depending on the type of pain, classified largely by location, or the chronicity of pain.
Of interest here is the specificity of the effects. Pain disrupted working memory by increasing the chance of wrongly identifying nontargets as targets, an effect exacerbated by intensity. A similar pattern of results was found in the study of menstrual pain by Keogh et al.18 using the same n-back task and in the study of headache and migraine by Kuhajda et al.20 using a word recognition test 1 to 7 days after encoding. If pain-related increases in false alarms occur consistently for both working memory and longer-term memory, its impact on day-to-day life is potentially extensive. However, Moore et al.22 found a different effect on n-back performance in their study of headache pain; accuracy for targets but not nontargets was reduced when participants were in pain. This inconsistency is difficult to reconcile. It cannot be explained simply by the type of pain studied (which was the same in Moore et al. and Kuhadja et al.) or the type of task used (which was the same in Moore et al. and Keogh et al.). However, it could be the specific combination of headache and n-back task that produces a reduction in the number of hits. To investigate this possibility, we ran an additional analysis to compare the number of hits in participants with headache pain (N = 45) vs menstrual pain (N = 9). This analysis was hindered by a small number of participants with menstrual pain and no other pain conditions, and although the comparison was not significant, t(52) = 1.75, P = 0.086, participants with headache had 11% fewer hits than participants with menstrual pain. Taken together, these findings suggest that headache specifically impairs working memory for targets, whereas pain in general increases false alarms in working and longer-term memory. Further investigation is needed to confirm this.
We tested between 2 hypotheses of the higher number of false alarms in participants with pain; either participants believed that nontargets were targets, in which case their RTs should be similar for false alarms and hits, or participants were more likely to select the target option when they were unsure, in which case we expected RTs for false alarms to be longer than RTs for hits, due to hesitation. The latter seemed to be the case in participants without pain, but we found no difference in RTs for hits and false alarms for participants with pain. This suggests that participants who are in pain may be genuinely mistaking nontargets for targets. However, the interaction between trial type and pain did not achieve significance, and these hypotheses should be investigated further in future research.
Multiple executive processes are involved in performing the n-back task: actively maintaining the previous n items, updating working memory with new items, rapidly binding items to their serial position, and inhibiting any interference from items that appeared not n-items back.8 It is unclear which of these processes could be responsible for the increase in false alarms in participants with pain. False alarms may result from incorrect updating of new items (ie, updating the working memory record with new letters that were not presented), incorrect binding of items to their serial position so that letters seen 1- or 3-back are incorrectly coded as being 2-back, or failure to inhibit interference from recently seen items that were not exactly n-items back. The latter explanation seems most likely because the former 2 would likely reduce the number of hits in addition to increasing the number of false alarms.
A major strength of this study is the size and diversity of our sample, which allowed us to examine the effects of types of pain and duration of pain on n-back performance. Neither type nor duration of pain had a significant effect on number of hits, number of correct rejections, hit RTs, or correct rejection RTs, which suggests that the effect of pain on working memory is general rather than specific to certain conditions.
We also investigated the role of sex and age in working memory disruption from pain. While 47% of women reported pain compared with 33% of men, there was no difference in pain intensity between the sexes and there were no interactions between pain and sex on task performance. This suggests that although females may be more susceptible to pain or more willing to report it, they do not differ broadly from men in terms of working memory disruption from pain. Our sample reported a wide range of ages (18-71 years), in contrast to the majority of pain and cognition research that tends to recruit samples with narrower age ranges, such as students (eg, 18,19,21,22,28). Sex and age interacted to affect number of correct rejections and RTs to both hits and correct rejections. In women, age was more strongly associated with a decline in accuracy and an increase in RTs than in men. Importantly, however, there were no interactions between age and pain on task performance, which suggests that the effects of pain on working memory are generalisable across the age range we examined and provides some reassurance that samples with limited age ranges in this field should not be a substantial cause for concern.
A limitation to this study is that a proportion of participants (11%) failed to perform above chance level on the n-back task. The online nature of the study meant that participants were not able to ask the researchers for clarifications if they were unsure how to perform the task. Importantly, we found no evidence that above chance performance was dependent on presence/absence of pain or type of pain. The online nature of the study also meant that we were limited in how many measures we could administer, and so we did not assess psychological traits such as catastrophising. Individual difference measures such as this have been studied extensively in the laboratory, and they were not relevant to our main aim here.
Of note is that the effect sizes we found were small; false alarms were 3.4% higher in participants with pain than in those without pain. For comparison, cocaine has been found to reduce hits on a 2-back task by 8%.27 However, the effect size we found here was comparable with that found in other pain studies. Keogh et al.18 found 2.5% more false alarms on a 2-back task in participants with menstrual pain, while Buhle and Wager6 found an approximately 4% decrease in hits on a 3-back task when participants experienced high heat pain induction compared with low heat. The small magnitude of the effect of pain on n-back performance is reassuring in a sense, but we should be careful not to dismiss the relevance of small effects on processes as important as working memory. In a complex situation such as driving, where multiple processes are reliant on working memory and multiple decisions are made every minute, 3% more errors could have very important consequences.
We have taken pain and attention research out of the laboratory and replicated previous findings, but future research should go further by examining the effect of everyday pain on tasks that more closely resemble the use of working memory in the real world, such as driving, cooking, or shopping. Our research has already begun to move in this direction. Keogh et al.19 investigated the effects of thermal pain induction on a complex computerised breakfast-making task and found impaired ability to multitask in participants experiencing pain. Further research in this direction should establish the extent of attentional disruption from pain in day-to-day life and investigate strategies people use to deal with this disruption.
In summary, we have conducted a novel large-scale internet study recruiting participants with a variety of painful conditions and shown that working memory is impaired in people with naturally occurring pain in the general population. This is the first study of pain and cognition to recruit such a large and diverse sample and to use the internet for recruitment and testing. Our findings represent further evidence that pain has a disruptive effect on working memory, and they suggest that the effect is reliable enough to be seen across a variety of pain conditions, intensities, and durations and in participants from multiple countries with a wide range of ages and testing environments. This not only provides convincing evidence that the effects of pain on working memory are robust but also demonstrates that it is feasible and worthwhile to conduct pain cognition research online.
Conflict of interest statement
The authors have no conflicts of interest to declare.
This research was supported by an unrestricted grant for research from Reckitt Benckiser Healthcare UK Ltd.
Footnotes
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
References
- [1].Arntz A, Hopmans M. Underpredicted pain disrupts more than correctly predicted pain, but does not hurt more. Beh Res Ther 1998;36:1121–9. [DOI] [PubMed] [Google Scholar]
- [2].Attridge NF, Crombez G, Van Ryckeghem D, Keogh E, Eccleston C. The Experience of Cognitive Intrusion of Pain: scale development and validation. PAIN. Epub ahead of print, 9 June 2015. 10.1097/j.pain.0000000000000257. [DOI] [PMC free article] [PubMed]
- [3].Aust F, Diedenhofen B, Ullrish S, Musch J. Seriousness checks are useful to improve data validity in online research. Behav Res Methods 2013;45:527–35. [DOI] [PubMed] [Google Scholar]
- [4].Berryman C, Stanton TR, Bowering KJ, Tabor A, McFarlane A, Moseley GL. Do people with chronic pain have impaired executive function? A meta-analytical review. Clin Psychol Rev 2014;34:563–79. [DOI] [PubMed] [Google Scholar]
- [5].Bowering KJ, Butler DS, Fulton IJ, Moseley GL. Motor imagery in people with a history of back pain, current back pain, both, or neither. Clin J Pain 2014;30:1070–5. [DOI] [PubMed] [Google Scholar]
- [6].Buhle J, Wager TD. Performance-dependent inhibition of pain by an executive working memory task. PAIN 2010;149:19–26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].Buhrmester M, Kwang T, Gosling SD. Amazon's Mechanical Turk: a new source of inexpensive, yet high-quality, data? Perspect Psychol Sci 2011;6:3–5. [DOI] [PubMed] [Google Scholar]
- [8].Chatham CH, Herd SA, Brant AM, Hazy TE, Miyake A, O'Reilly R, Friedman NP. From an executive network to executive control: a computational model of the n-back task. J Cogn Neurosci 2011;23:3598–619. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [9].Crombez G, Eccleston C, Baeyens F, Eelen P. The disruptive nature of pain: an experimental investigation. Behav Res Ther 1996;34:911–18. [DOI] [PubMed] [Google Scholar]
- [10].Crombez G, Eccleston C, Baeyens F, Eelen P. Habituation and the interference of pain with task performance. PAIN 1997;70:149–54. [DOI] [PubMed] [Google Scholar]
- [11].Crombez G, Eccleston C, Baeyens F, Eelen P. Attentional disruption is enhanced by the threat of pain. Behav Res Ther 1998;36:195–204. [DOI] [PubMed] [Google Scholar]
- [12].Crombez G, Eccleston C, Van den Broeck A, Van Houdenhove B, Goubert L. The effects of catastrophic thinking about pain on attentional interference by pain: no mediation of negative affectivity in healthy volunteers and in patients with low back pain. Pain Res Manag 2002;7:31–9. [DOI] [PubMed] [Google Scholar]
- [13].De Clercq A, Crombez G, Buysse A, Roeyers H. A simple and sensitive method to measure timing accuracy. Behav Res Methods Instrum Comput 2003;35:109–15. [DOI] [PubMed] [Google Scholar]
- [14].Draine SC. Inquisit 4 Web [computer program]. Seattle, WA: Millisecond Software; 2013.
- [15].Eccleston C. Chronic pain and distraction: an experimental investigation into the role of sustained and shifting attention in the processing of chronic persistent pain. Behav Res Ther 1995;33:391–405. [DOI] [PubMed] [Google Scholar]
- [16].Eccleston C, Crombez G. Pain demands attention: a cognitive–affective model of the interruptive function of pain. Psychol Bull 1999;125:356–66. [DOI] [PubMed] [Google Scholar]
- [17].Keogh E. Sex differences in pain across the life course. In: Moore R, editor. Handbook of pain and palliative care: biobehavioral approaches for the life course, Chapter 21. New York: Springer, 2012. p. 347–66. [Google Scholar]
- [18].Keogh E, Cavill R, Moore DJ, Eccleston C. The effects of menstrual-related pain on attentional interference. PAIN 2014;155:821–7. [DOI] [PubMed] [Google Scholar]
- [19].Keogh E, Moore DJ, Duggan GB, Payne SJ, Eccleston C. The disruptive effects of pain on complex cognitive performance and executive control. PLoS One 2013;8:e83272. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [20].Kuhajda MC, Thorn BE, Klinger MR, Rubin NJ. The effect of headache pain on attention (encoding) and memory (recognition). PAIN 2002;97:213–21. [DOI] [PubMed] [Google Scholar]
- [21].Moore DJ, Keogh E, Eccleston C. The interruptive effect of pain on attention. Q J Exp Psychol (Hove). 2012;65:565–86. [DOI] [PubMed] [Google Scholar]
- [22].Moore DJ, Keogh E, Eccleston C. Headache impairs attentional performance. PAIN 2013;154:1840–5. [DOI] [PubMed] [Google Scholar]
- [23].Paolacci G, Chandler J, Ipeirotis PG. Running experiments on Amazon Mechanical Turk. Judgm Decis Mak 2010;5:411–19. [Google Scholar]
- [24].Smith A, Ayres P. The impact of persistent pain on working memory and learning. Educ Psychol Rev 2014;26:245–64. [Google Scholar]
- [25].Stewart WF, Ricci JA, Chee E, Morganstein D, Lipton R. Lost productive time and cost due to common pain conditions in the US workforce. JAMA 2003;290:2443–54. [DOI] [PubMed] [Google Scholar]
- [26].Stovner LJ, Andree C. Prevalence of headache in Europe: a review for the Eurolight project. J Headache Pain 2010;11:289–99. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [27].Tomasi D, Goldstein RZ, Telang F, Maloney T, Alia-Klein N, Caparelli EC, Volkow ND. Widespread disruption in brain activation patterns to a working memory task during cocaine abstinence. Brain Res 2007;1171:83–92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [28].Van Ryckeghem DML, Crombez G, Eccleston C, Liefooghe B, Van Damme S. The interruptive effect of pain in a multi-task environment: an experimental investigation. J Pain 2012;13:131–8. [DOI] [PubMed] [Google Scholar]