

Abstract
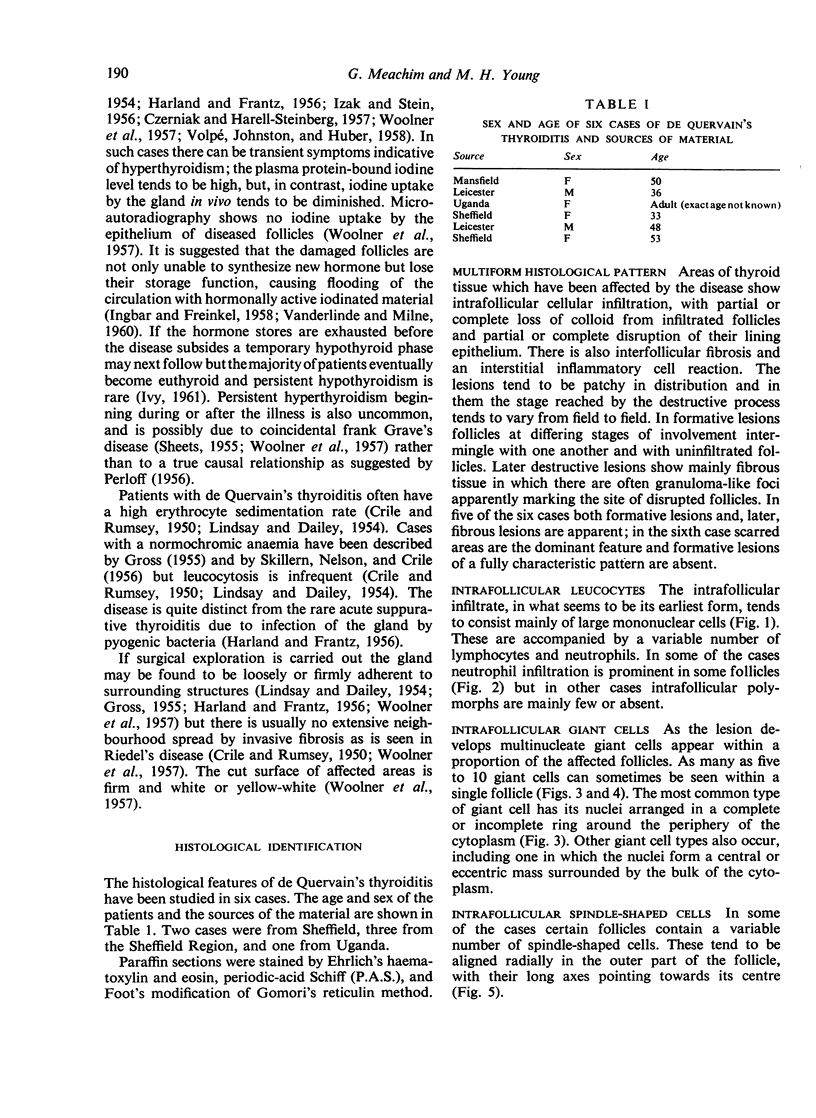
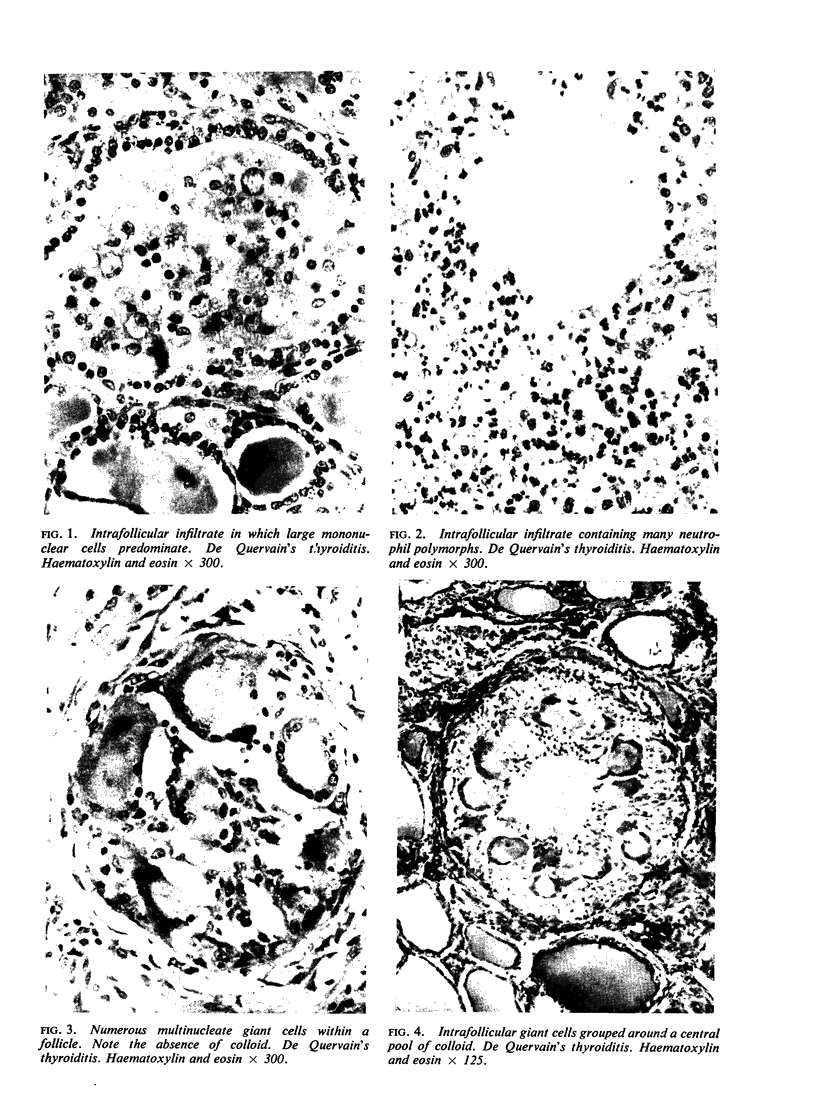
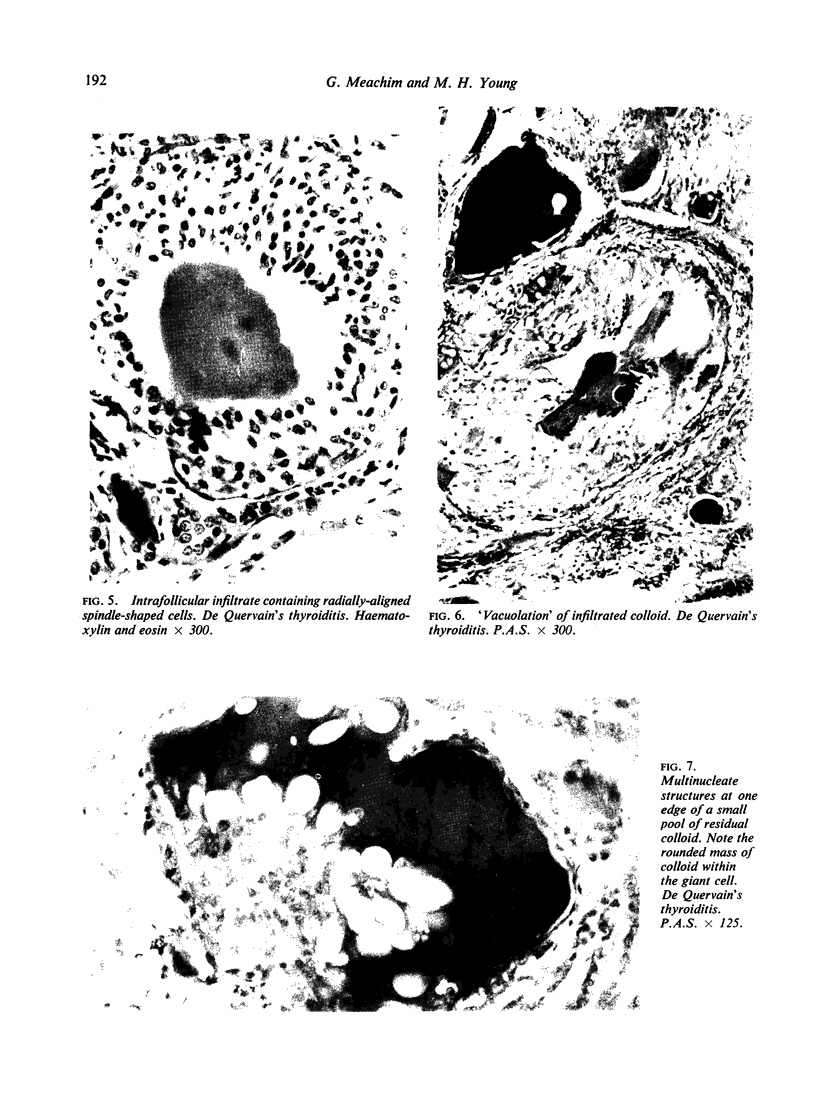
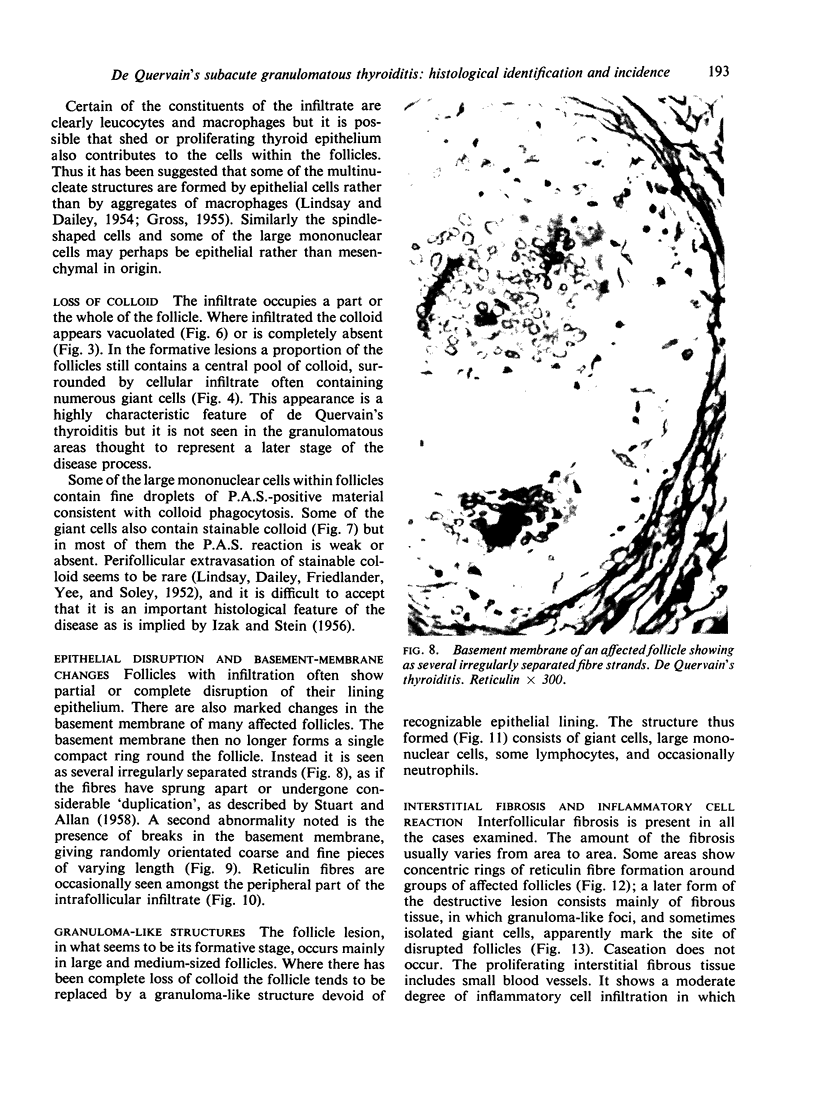
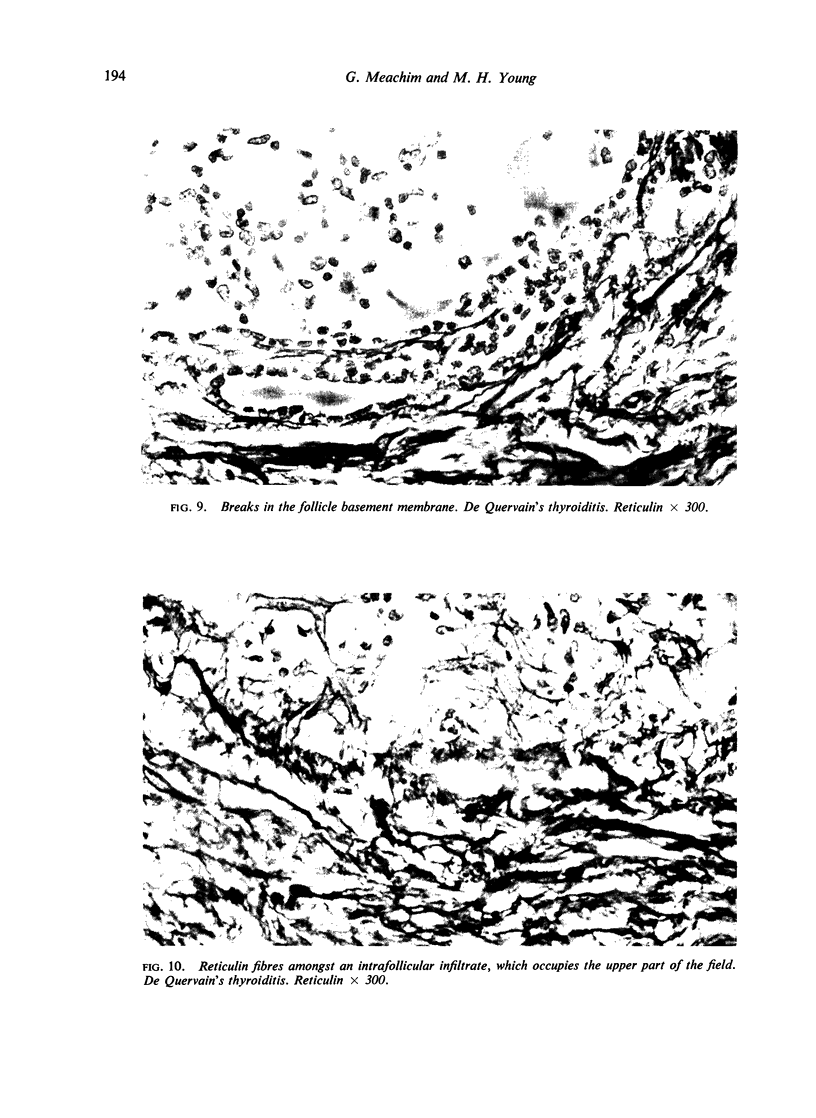
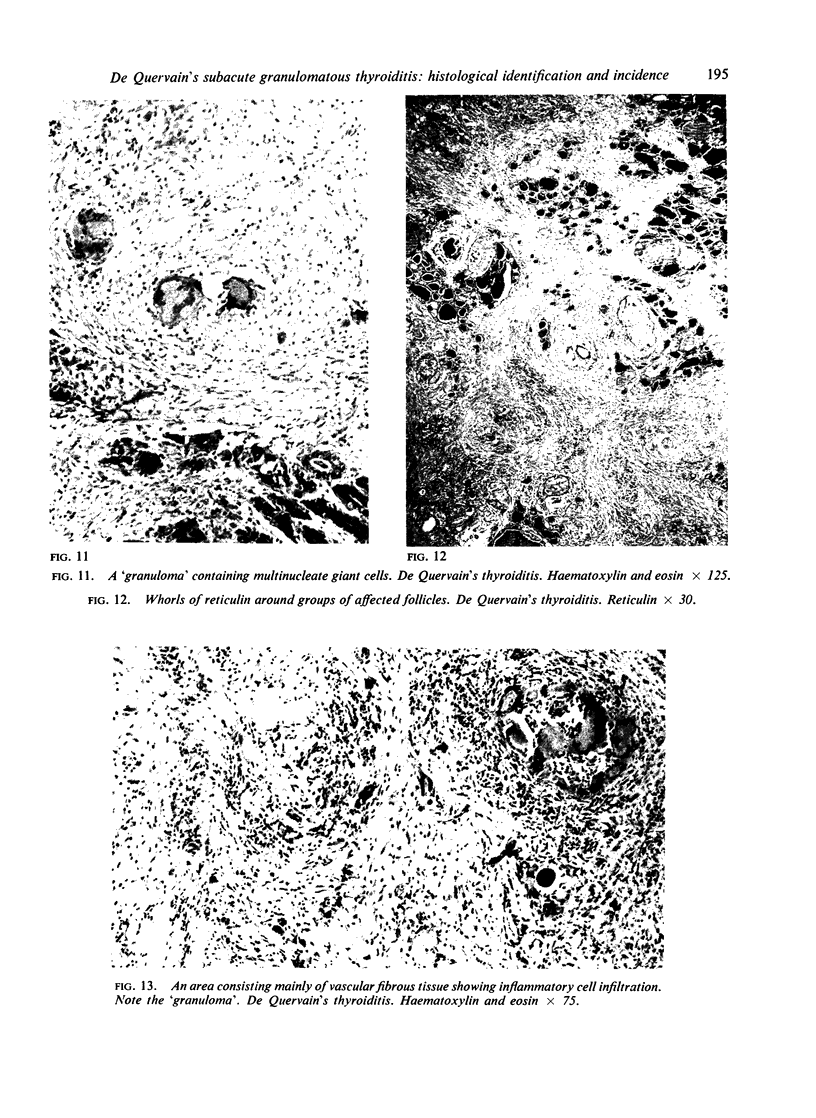
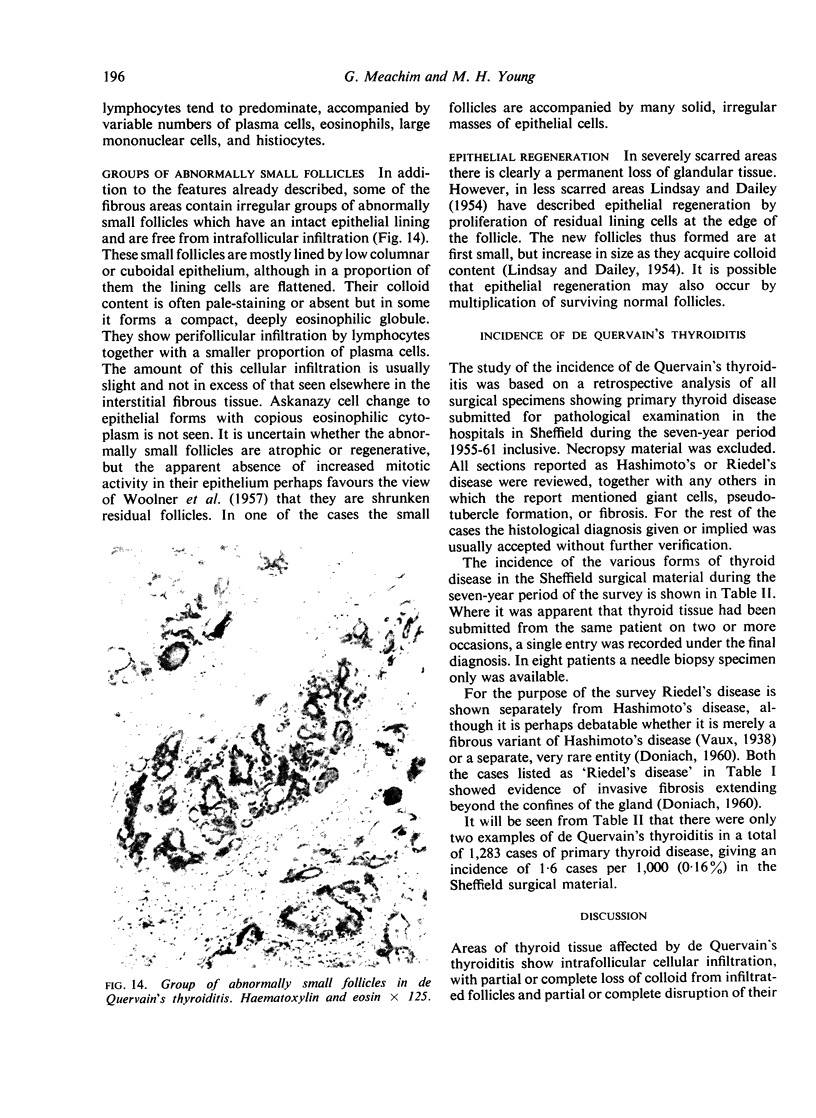
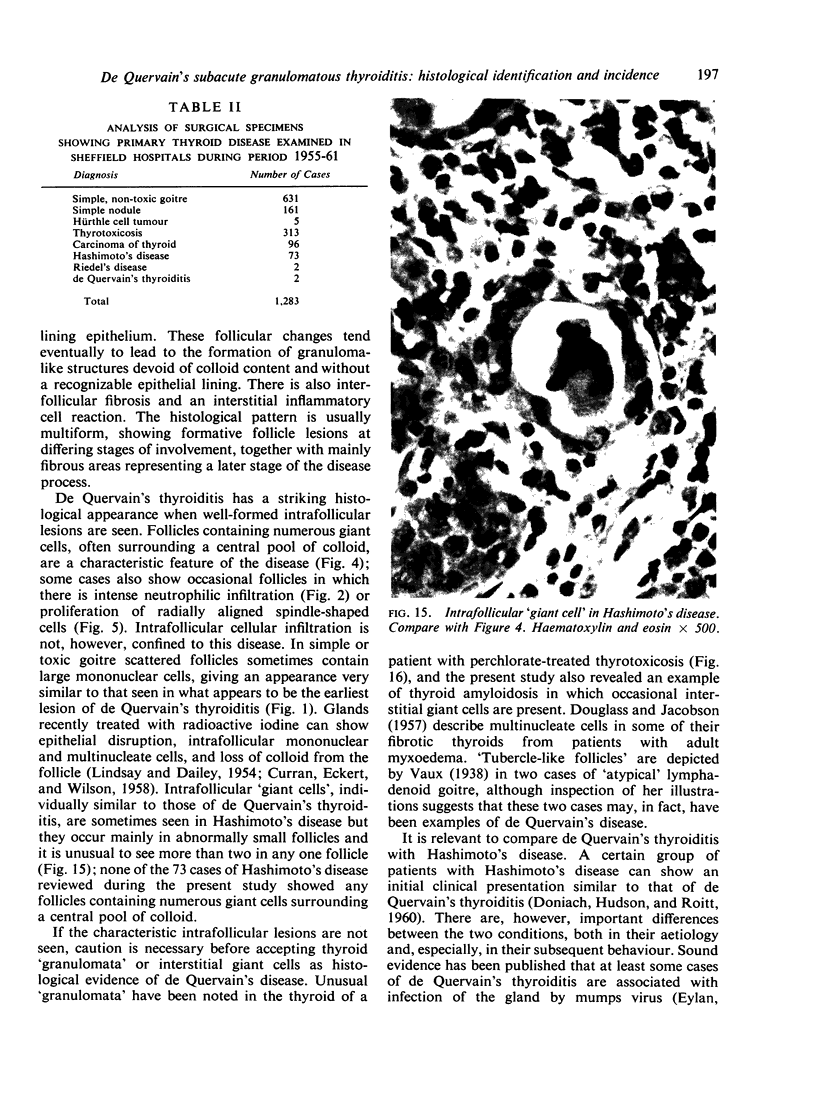
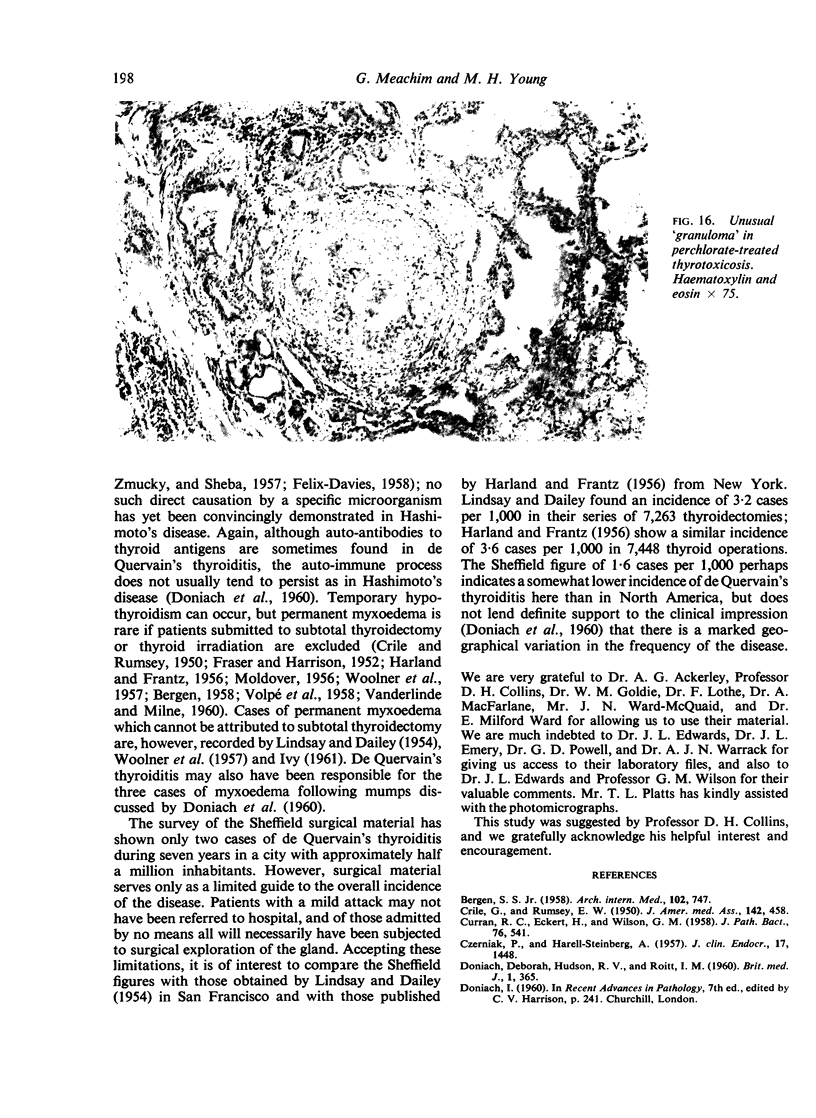
The histological features of de Quervain's subacute granulomatous thyroiditis are described, on the basis of a study of six specimens. This condition, unlike Hashimoto's disease, rarely causes permanent hypothyroidism; its histological identification is thus of practical importance. Areas of thyroid affected by the disease show intrafollicular cellular infiltration, with partial or complete loss of colloid from infiltrated follicles, partial or complete disruption of their lining epithelium, and abnormalities of the basement membrane. These changes tend eventually to lead to replacement of the damaged follicle by a granuloma-like structure devoid of colloid content and without a recognizable epithelial lining. The disease also causes interfollicular fibrosis and an interstitial inflammatory cell reaction. The histological pattern is typically multiform. Formative follicle lesions present a striking appearance, aiding recognition of the disease. Some follicles contain numerous giant cells, often grouped around a central pool of residual colloid; others may contain a considerable proportion of neutrophil polymorphs or show radially aligned spindle-shaped cells.
A study has also been made of the incidence of de Quervain's thyroiditis in surgical material in Sheffield during the seven year period 1955-61. Only two examples were found in a total of 1,282 cases of primary thyroid disease, an incidence of 1·6 per 1,000 (0·16%); there is, however, reason to believe that the overall clinical incidence is higher than that indicated by the surgical figures.
Full text
PDF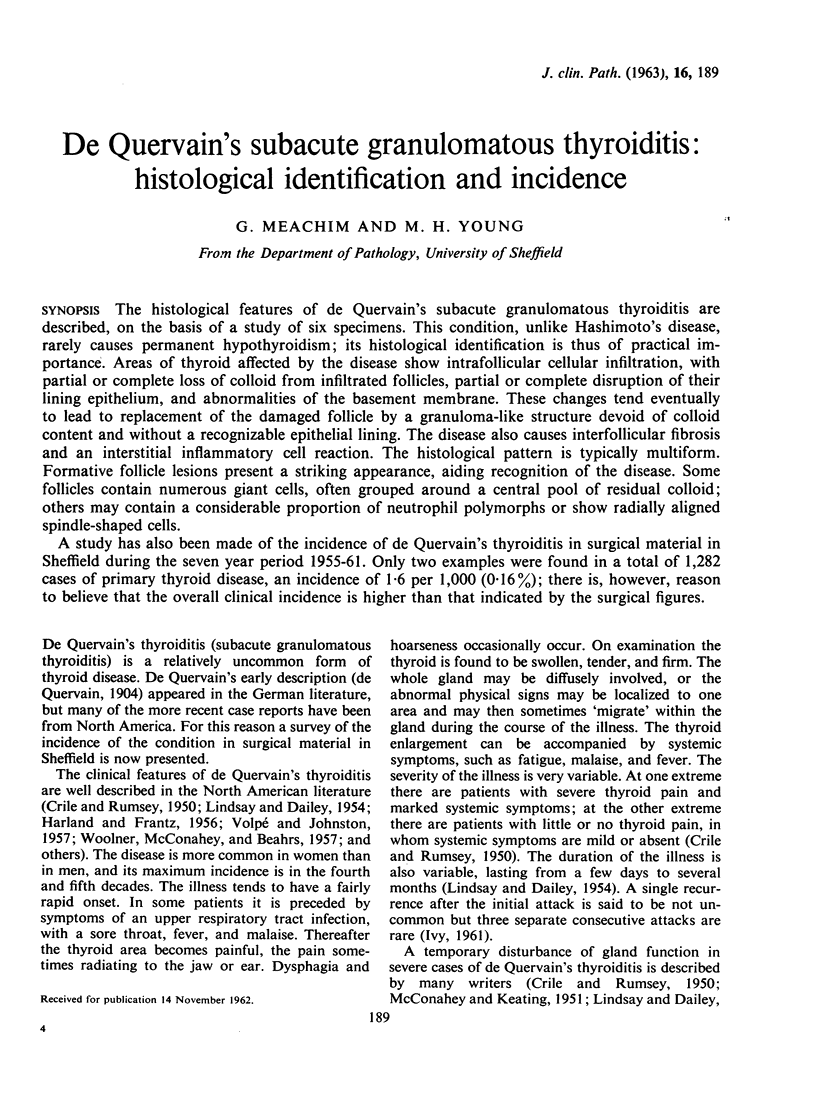
Images in this article





Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- CRILE G., Jr, NELSON H. E., SKILLERN P. G. Some new observations on subacute thyroiditis. J Clin Endocrinol Metab. 1956 Nov;16(11):1422–1432. doi: 10.1210/jcem-16-11-1422. [DOI] [PubMed] [Google Scholar]
- CRILE G., Jr, RUMSEY E. W. Subacute thyroiditis. J Am Med Assoc. 1950 Feb 18;142(7):458-62, illust. doi: 10.1001/jama.1950.02910250006002. [DOI] [PubMed] [Google Scholar]
- CURRAN R. C., ECKERT H., WILSON G. M. The thyroid gland after treatment of hyperthyroidism by partial thyroidectomy or iodine 131. J Pathol Bacteriol. 1958 Oct;76(2):541–560. doi: 10.1002/path.1700760224. [DOI] [PubMed] [Google Scholar]
- CZERNIAK P., HARELL-STEINBERG A. The chronology of events in the development of subacute thyroiditis, studied by radioactive iodine. J Clin Endocrinol Metab. 1957 Dec;17(12):1448–1453. doi: 10.1210/jcem-17-12-1448. [DOI] [PubMed] [Google Scholar]
- DONIACH D., HUDSON R. V., ROITT I. M. Human auto-immune thyroiditis: clinical studies. Br Med J. 1960 Feb 6;1(5170):365–373. doi: 10.1136/bmj.1.5170.365. [DOI] [PMC free article] [PubMed] [Google Scholar]
- EYLAN E., ZMUCKY R., SHEBA C. Mumps virus and subacute thyroiditis; evidence of a causal association. Lancet. 1957 May 25;272(6978):1062–1063. doi: 10.1016/s0140-6736(57)91438-1. [DOI] [PubMed] [Google Scholar]
- INGBAR S. H., FREINKEL N. Thyroid function and the metabolism of iodine in patients with subacute thyroiditis. AMA Arch Intern Med. 1958 Feb;101(2):339–346. doi: 10.1001/archinte.1958.00260140171026. [DOI] [PubMed] [Google Scholar]
- IZAK G., STEIN Y. Subacute non-suppurative thyroiditis; treatment with cortisone and corticotrophin. Lancet. 1956 Feb 4;270(6910):225–226. doi: 10.1016/s0140-6736(56)91150-3. [DOI] [PubMed] [Google Scholar]
- LINDSAY S., DAILEY M. E., FRIEDLANDER J., YEE G., SOLEY M. H. Chronic thyroiditis: a clinical and pathologic study of 354 patients. J Clin Endocrinol Metab. 1952 Dec;12(12):1578–1600. doi: 10.1210/jcem-12-12-1578. [DOI] [PubMed] [Google Scholar]
- LINDSAY S., DAILEY M. E. Granulomatous or giant cell thyroiditis; a clinical and pathologic study of thirty-seven patients. Surg Gynecol Obstet. 1954 Feb;98(2):197–212. [PubMed] [Google Scholar]
- MOLDOVER A. Subacute thyroiditis; report of three cases treated with cortisone. AMA Arch Intern Med. 1956 Sep;98(3):322–327. doi: 10.1001/archinte.1956.00250270066007. [DOI] [PubMed] [Google Scholar]
- STUART A. E., ALLAN W. S. The significance of basement-membrane changes in thyroid disease. Lancet. 1958 Dec 6;2(7058):1204–1206. doi: 10.1016/s0140-6736(58)92356-0. [DOI] [PubMed] [Google Scholar]
- WOOLNER L. B., McCONAHEY W. M., BEAHRS O. H. Granulomatous thyroiditis (De Quervain's thyroiditis). J Clin Endocrinol Metab. 1957 Oct;17(10):1202–1221. doi: 10.1210/jcem-17-10-1202. [DOI] [PubMed] [Google Scholar]