

Abstract
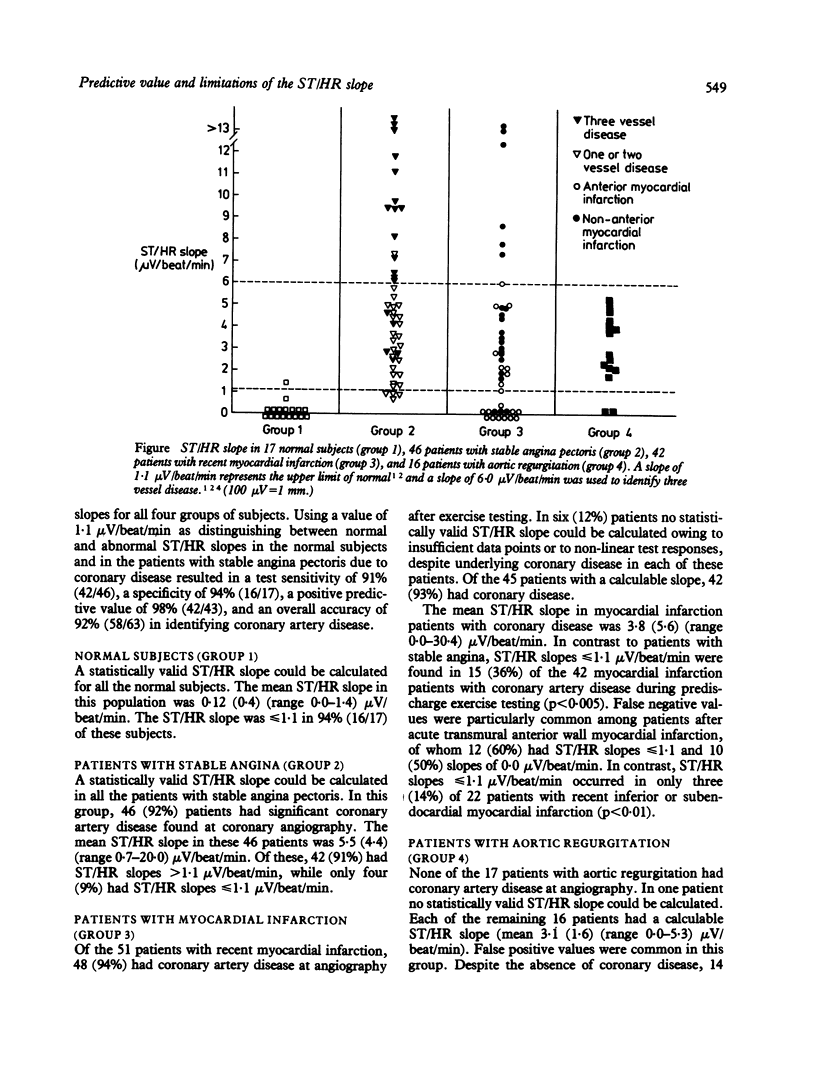
To assess the value and predictive limitations of the exercise ST/HR slope, exercise test results were compared in 50 patients with stable angina and in 17 normal subjects with those in two groups known to have a high prevalence of inaccurate electrocardiographic responses to exercise. The last two groups included 51 patients tested within three weeks of acute myocardial infarction and 17 with important aortic regurgitation but no coronary disease. Of the normal subjects, 16 (94%) had ST/HR values less than or equal to 1 X 1 microV/beat/min. Of those with stable angina pectoris, 42 of 46 (91%) patients with coronary artery disease had ST/HR slopes ranging from 1 X 2 to 20 X 0 microV/beat/min, with false negative findings (slopes less than or equal to 1 X 1 microV/beat/min) in only four (9%). In contrast, of those with recent myocardial infarction, 15 of 42 (36%) with coronary disease had false negative slopes, including 12 of 20 (60%) with anterior wall injury. Of those with aortic regurgitation, conversely, 14 of 16 (88%) patients with calculable ST/HR slopes had values greater than 1 X 1 microV/beat/min despite the absence of coronary disease. Despite the accuracy of the test in patients with stable angina, false negative results are common in those after recent myocardial infarction, and false positive results occur often in those with abnormal volume loading due to aortic regurgitation.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Aronow W. S., Harris C. N. Treadmill exercise test in aortic stenosis and mitral stenosis. Chest. 1975 Oct;68(4):507–509. doi: 10.1378/chest.68.4.507. [DOI] [PubMed] [Google Scholar]
- Balcon R., Brooks N., Layton C. Correlation of heart rate/ST slope and coronary angiographic findings. Br Heart J. 1984 Sep;52(3):304–307. doi: 10.1136/hrt.52.3.304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Borer J. S., Bacharach S. L., Green M. V., Kent K. M., Epstein S. E., Johnston G. S. Real-time radionuclide cineangiography in the noninvasive evaluation of global and regional left ventricular function at rest and during exercise in patients with coronary-artery disease. N Engl J Med. 1977 Apr 14;296(15):839–844. doi: 10.1056/NEJM197704142961503. [DOI] [PubMed] [Google Scholar]
- Bruce R. A., Kusumi F., Hosmer D. Maximal oxygen intake and nomographic assessment of functional aerobic impairment in cardiovascular disease. Am Heart J. 1973 Apr;85(4):546–562. doi: 10.1016/0002-8703(73)90502-4. [DOI] [PubMed] [Google Scholar]
- Castellanet M. J., Greenberg P. S., Ellestad M. H. Comparison of S-T segment changes on exercise testing with angiographic findings in patients with prior myocardial infarction. Am J Cardiol. 1978 Jul;42(1):29–35. doi: 10.1016/0002-9149(78)90980-3. [DOI] [PubMed] [Google Scholar]
- Devereux R. B. Echocardiography: state of the art--1984. Cardiology. 1984;71(2-3):118–135. doi: 10.1159/000173658. [DOI] [PubMed] [Google Scholar]
- Elamin M. S., Boyle R., Kardash M. M., Smith D. R., Stoker J. B., Whitaker W., Mary D. A., Linden R. J. Accurate detection of coronary heart disease by new exercise test. Br Heart J. 1982 Oct;48(4):311–320. doi: 10.1136/hrt.48.4.311. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Elamin M. S., Mary D. A., Smith D. R., Linden R. J. Prediction of severity of coronary artery disease using slope of submaximal ST segment/heart rate relationship. Cardiovasc Res. 1980 Dec;14(12):681–691. doi: 10.1093/cvr/14.12.681. [DOI] [PubMed] [Google Scholar]
- Fox K. M. Exercise heart rate/ST segment relation. Perfect predictor of coronary disease. Br Heart J. 1982 Oct;48(4):309–310. doi: 10.1136/hrt.48.4.309. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goldschlager N., Selzer A., Cohn K. Treadmill stress tests as indicators of presence and severity of coronary artery disease. Ann Intern Med. 1976 Sep;85(3):277–286. doi: 10.7326/0003-4819-85-3-277. [DOI] [PubMed] [Google Scholar]
- Kardash M., Boyle R., Elamin M. S., Stoker J. B., Mary D. A., Linden R. J. Detection of severity of coronary artery disease by the ST segment/heart rate relationship in patients on beta-blocker therapy. Cardiovasc Res. 1982 Sep;16(9):508–515. doi: 10.1093/cvr/16.9.508. [DOI] [PubMed] [Google Scholar]
- Okin P. M., Kligfield P., Ameisen O., Goldberg H. L., Borer J. S. Improved accuracy of the exercise electrocardiogram: identification of three-vessel coronary disease in stable angina pectoris by analysis of peak rate-related changes in ST segments. Am J Cardiol. 1985 Feb 1;55(4):271–276. doi: 10.1016/0002-9149(85)90359-5. [DOI] [PubMed] [Google Scholar]
- Paine T. D., Dye L. E., Roitman D. I., Sheffield L. T., Rackley C. E., Russell R. O., Jr, Rogers W. J. Relation of graded exercise test findings after myocardial infarction to extent of coronary artery disease and left ventricular dysfunction. Am J Cardiol. 1978 Nov;42(5):716–723. doi: 10.1016/0002-9149(78)90089-9. [DOI] [PubMed] [Google Scholar]
- Quyyumi A. A., Raphael M. J., Wright C., Bealing L., Fox K. M. Inability of the ST segment/heart rate slope to predict accurately the severity of coronary artery disease. Br Heart J. 1984 Apr;51(4):395–398. doi: 10.1136/hrt.51.4.395. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Théroux P., Waters D. D., Halphen C., Debaisieux J. C., Mizgala H. F. Prognostic value of exercise testing soon after myocardial infarction. N Engl J Med. 1979 Aug 16;301(7):341–345. doi: 10.1056/NEJM197908163010701. [DOI] [PubMed] [Google Scholar]