

Essential thrombocytemia (ET) may occur in women of childbearing age. Pregnancy may therefore be a common issue in the clinical management of young women with ET.1,2
Previous studies have shown live birth rates of 50% to 70% and spontaneous abortion rates of 25% to 50%, mostly during the first-trimester.3–5 The pathogenesis of poor pregnancy outcome has not been fully clarified. Age, parity, thrombophilia, platelet count, leukocyte count, and hemoglobin level have not been found to be predictive of pregnancy outcome in ET;3–5 however, a 3.4-fold higher risk of fetal loss in women with ET than in healthy women has been shown.3 The effect of JAK2 V617F mutation is currently unclear, as it has been associated with an increased rate of pregnancy loss in 2 studies3,5 but not confirmed in others.4,6 Data regarding the impact of the other MPN-associated mutations are lacking.
Two recent papers demonstrated that most of the patients with sporadic ET wild type for both JAK2 and MPL carry somatic mutations of CALR.7,8 The clinical course of sporadic CALR mutated patients has been shown to be more indolent than that of JAK2 mutated cases.7,9,10
The impact of CALR mutations on pregnancy outcome in ET remains to be clarified. In this study we aimed to investigate the correlation between mutational status and pregnancy complications.
This study includes 155 pregnancies that occurred in 94 patients with ET who were diagnosed between 1982 and 2014 at the Department of Hematology Oncology, Fondazione IRCCS Policlinico San Matteo Pavia, and at the First Clinical Medicine of the University of Padova, and for whom at least one DNA sample to assess mutational status was available (DNA collected between 2002 and 2014). Some of these cases (49 out of 94 patients) have been reported in our previous paper.3 This study was approved by the local ethics committees. The procedures followed were in accordance with the Helsinki Declaration, and samples were obtained with patients written informed consent. Diagnosis of ET was made in accordance with the criteria in use at the time of the first observation, as previously described.9
All patients were screened for JAK2, CALR and MPL mutations with previously reported methods.7,9 The four genotypic subgroups (JAK2 mutated, CALR mutated, MPL mutated and triple-negative patients) were compared in terms of pregnancy outcome. Pregnancy complications included fetal loss (first, second or third-trimester miscarriage), intrauterine growth retardation (IUGR), and maternal complications (including thrombosis, bleeding, preeclampsia, gestational hypertension, gestational diabetes, abruptio placentae and intrahepatic cholestasis).
Categorical variables have been described as counts and relative frequencies (%) of each category. Quantitative variables have been summarized as median and range. The Fisher’s exact test was adopted to evaluate the association between categorical variables, while comparison of quantitative variables between two or more groups of patients was carried out by the non-parametric Wilcoxon rank-sum test or the Kruskal-Wallis analysis, respectively. An association between the occurrence of pregnancy complications and mutational status, year of pregnancy, age at pregnancy and use of aspirin was investigated via multivariate logistic regression, “correcting” standard errors to specify that pregnancies are independent across patients, but not within patients (repeated pregnancies in patients).
Of 94 ET patients, 59 (62.8%) carried JAK2 V617F mutation, 19 (20.2%) carried CALR mutations, 2 (2.1%) carried MPL mutations, and 14 (14.9%) were triple-negative.
When comparing hematological data at ET diagnosis, the hemoglobin value was the only hematological parameter that differed according to mutational status, being higher in JAK2 V617F mutated patients (median 14 g/dl, range 11.2–16) than in both CALR mutated patients (median 13 g/dl, range 11.5–14, P<0.001) and triple-negative patients (median 12.2 g/dl, range 8–14, P<0.001), thus confirming that which we previously reported.9
3 pregnancies were ended by voluntary abortion and were excluded from the analysis of pregnancy outcome. Overall, 72 out of 152 pregnancies (47.4%) were complicated: 46 (30%) by fetal loss (37 during the first-trimester, 6 during the second and 3 during the third), 18 (11.8%) by maternal complications, and 13 (8.6%) by IUGR. The distribution of complications according to mutational status is reported in Table 1.
Table 1.
Distribution of pregnancy complications according to mutational status.
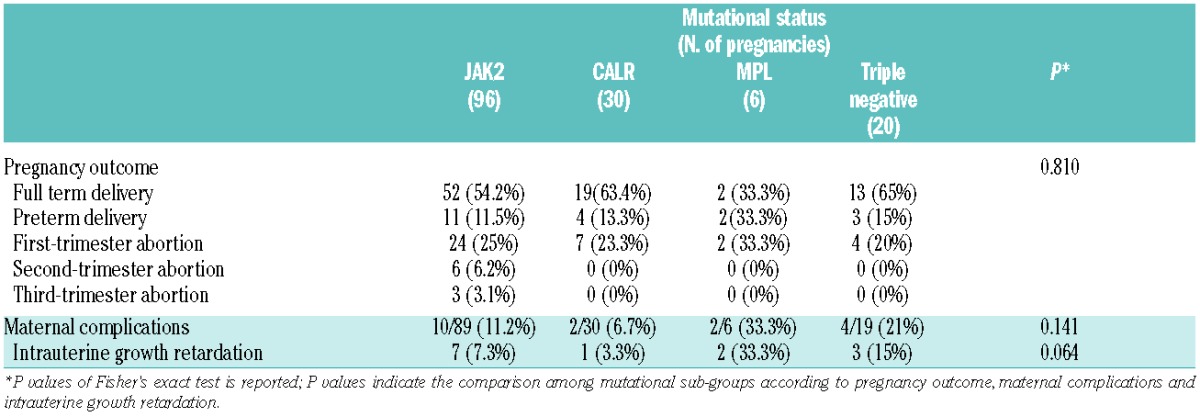
We did not find a correlation between mutation status and the rate of fetal losses (Fisher’s exact test P=0.52) or the rate of pregnancy complications, including both fetal and maternal complications (Fisher’s exact test P=0.134). This result did not confirm our previous observation that identified the JAK2 V617F mutation as an independent predictor of pregnancy complications.3 Of note, in our previous paper we could assess patients mutational status in only the 49 cases for whom a DNA sample was available,3 compared to the whole cohort of 94 patients in the current study. The absence of a role for the JAK2 V617F mutation in pregnancy outcome has already been reported both in MPN4 and in women with a history of recurrent miscarriage without a diagnosis of MPN.11
When we restricted the analysis to late pregnancy losses, a relationship with JAK2 V617F mutation (P=0.027) was found: second and third-trimester miscarriage occurred in 9.4% of JAK2 V617F pregnancies vs. none in MPL/CALR/triple-negative pregnancies. It is known that JAK2 V617F mutation is associated with a higher risk of thrombosis.12 In MPN pregnancies the prothrombotic state may affect the remodeling of maternal spiral arteries essential for adequate blood delivery to the placenta. In pregnancy the placental circulation changes from a low-flow high-resistance system to a high-flow low-resistance system. The JAK2 V617F mutation might contribute to placental hypoperfusion due to vascular thrombotic occlusion, thus impairing the process of spiral arteries remodeling during the second and third-trimester. This would account for the late pregnancy losses observed in JAK2 V617F mutated patients
To investigate the role of other potential predictors of pregnancy complications, we performed a multivariate analysis considering calendar year (before or after July 2007, the year of our previous paper on pregnancy in ET3), mutational status (CALR vs. JAK2/MPL/triple-negative), age at pregnancy and use of aspirin. In multivariate analysis we found that the occurrence of pregnancy before 2007 correlated with a poorer outcome (OR=2.5, 95%CI: 1.1–5.4, P=0.021), and the presence of CALR mutations showed a trend toward a lower rate of pregnancy complications (OR=0.4, 95%CI: 0.2–1.0, P=0.060), while no association was found with either age at pregnancy (OR=1.0, 95%CI: 0.9–1.1, P=0.645) or use of aspirin (OR=0.9, 95%CI: 0.4–2.0, P=0.709)(Figure 1). The improvement of pregnancy outcome after 2007 might be explained by better medical care with regard to pregnancies in more recent years.
Figure 1.
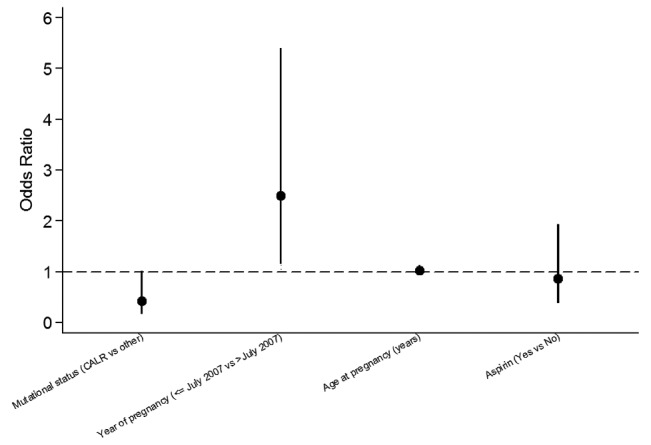
Odds ratios for the prevalence of risk factors in patients with pregnancy complications. ORs were 0.4 (95%CI: 0.2–1.0) for mutational status, 2.5 (95%CI: 1.1–5.4) for year of pregnancy, 1.0 (95%CI: 0.9–1.1) for age at pregnancy, and 0.9 (95%CI: 0.4–2.0) for use of aspirin. The occurrence of pregnancy before 2007 was a significant risk factor for pregnancy complications. The presence of CALR mutations showed a trend toward a lower rate of pregnancy complications.
The trend for a lower risk of pregnancy complications observed in CALR mutated ET is in line with previous studies reporting a lower risk of thrombosis in CALR mutated ET compared to JAK2 mutated ET.9,10 When also including the thrombophilic status (available in only 110 pregnancies), the multivariate analysis confirmed that pregnancy before 2007 correlated with a poorer outcome (OR=3.9, 95% CI:1.5–9.7, P=0.004); the presence of CALR mutations maintained a trend (OR=0,3 95%CI: 0.1–1.0, P=0.060) toward a lower rate of pregnancy complications, while no association was found with age at pregnancy (OR=1.0, 95%CI: 0.9–1.2, P=0.470), use of aspirin (OR=0.8, 95%CI: 0.3–2.3, P=0.711) or thrombophilic status (OR=2.0, 95%CI: 0.8–5, P=0.161).
In conclusion, the presence of JAK2 V617F mutation is associated with late pregnancy losses, whereas the presence of CALR mutations is associated with a trend to a better outcome. In addition, pregnancies occurring in the last decade showed a lower risk of pregnancy complications, suggesting an improvement in our medical care of pregnancies.
Acknowledgments
A special thank to Dr. Laura Tassi and prof. Giorgio Lo Russo for their technical support.
Footnotes
Funding: the Authors would like to thank Associazione Italiana per la Ricerca sul Cancro (AIRC) for the grant Special Program “Molecular Clinical Oncology 5 per mille” AGIMM (AIRC Gruppo Italiano Malattie Mieloproliferative) (project #1005) to MC and the grant “my first AIRC grant” (MFAG-2014-15672) to ER; and the Italian Ministry of Health for the grant GR-2010-2312855 to ER.
Information on authorship, contributions, and financial & other disclosures was provided by the authors and is available with the online version of this article at www.haematologica.org.
References
- 1.Harrison C. Pregnancy and its management in the Philadelphia negative myeloproliferative diseases. Br J Haematol 2005;129(3):293–306. [DOI] [PubMed] [Google Scholar]
- 2.Griesshammer M, Struve S, Harrison CM. Essential thrombocythemia/polycythemia vera and pregnancy: the need for an observational study in Europe. Semin Thromb Hemost 2006;32(4):422–429. [DOI] [PubMed] [Google Scholar]
- 3.Passamonti F, Randi ML, Rumi E, et al. Increased risk of pregnancy complications in patients with essential thrombocythemia carrying the JAK2 (617V>F) mutation. Blood 2007;110(2):485–489. [DOI] [PubMed] [Google Scholar]
- 4.Gangat N, Wolanskyj AP, Schwager S, Tefferi A. Predictors of pregnancy outcome in essential thrombocythemia: a single institution study of 63 pregnancies. Eur J Haematol 2009;82(5):350–353. [DOI] [PubMed] [Google Scholar]
- 5.Melillo L, Tieghi A, Candoni A, et al. Outcome of 122 pregnancies in essential thrombocythemia patients: A report from the Italian registry. Am J Hematol 2009;84(10):636–640. [DOI] [PubMed] [Google Scholar]
- 6.Randi ML, Bertozzi I, Rumi E, et al. Pregnancy complications predict thrombotic events in young women with essential thrombocythemia. Am J Hematol 2014;89(3):306–309. [DOI] [PubMed] [Google Scholar]
- 7.Klampfl T, Gisslinger H, Harutyunyan AS, et al. Somatic mutations of calreticulin in myeloproliferative neoplasms. N Engl J Med 2013; 369(25):2379–2390. [DOI] [PubMed] [Google Scholar]
- 8.Nangalia J, Massie CE, Baxter EJ, et al. Somatic CALR mutations in myeloproliferative neoplasms with nonmutated JAK2. N Engl J Med 2013;369(25):2391–2405. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Rumi E, Pietra D, Ferretti V, et al. JAK2 or CALR mutation status defines subtypes of essential thrombocythemia with substantially different clinical course and outcomes. Blood 2014;123(10):1544–1551. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Rotunno G, Mannarelli C, Guglielmelli P, et al. Impact of calreticulin mutations on clinical and hematological phenotype and outcome in essential thrombocythemia. Blood 2014;123(10):1552–1555. [DOI] [PubMed] [Google Scholar]
- 11.Dahabreh IJ, Jones AV, Voulgarelis M, et al. No evidence for increased prevalence of JAK2 V617F in women with a history of recurrent miscarriage. Br J Haematol 2009;144(5):802–803. [DOI] [PubMed] [Google Scholar]
- 12.Barbui T, Finazzi G, Carobbio A, et al. Development and validation of an International Prognostic Score of thrombosis in World Health Organization-essential thrombocythemia (IPSET-thrombosis). Blood 2012;120(26):5128–5133. [DOI] [PubMed] [Google Scholar]