

Abstract
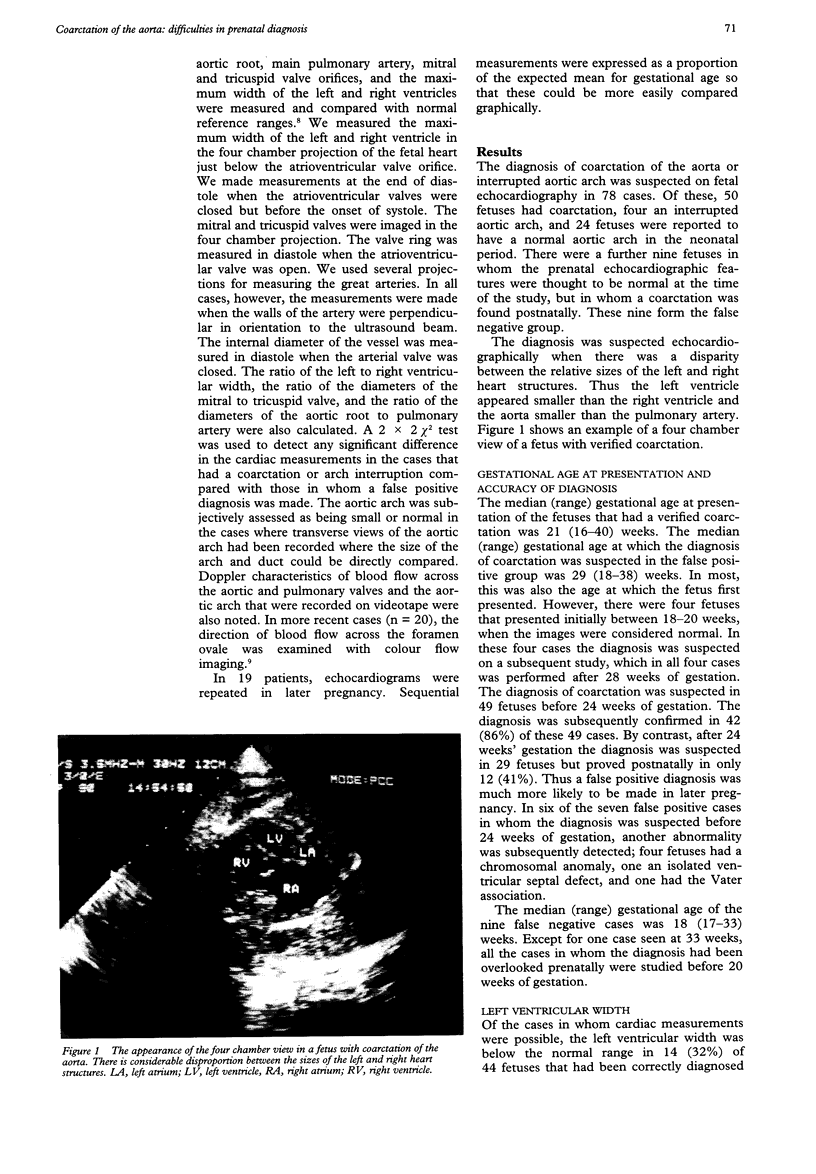
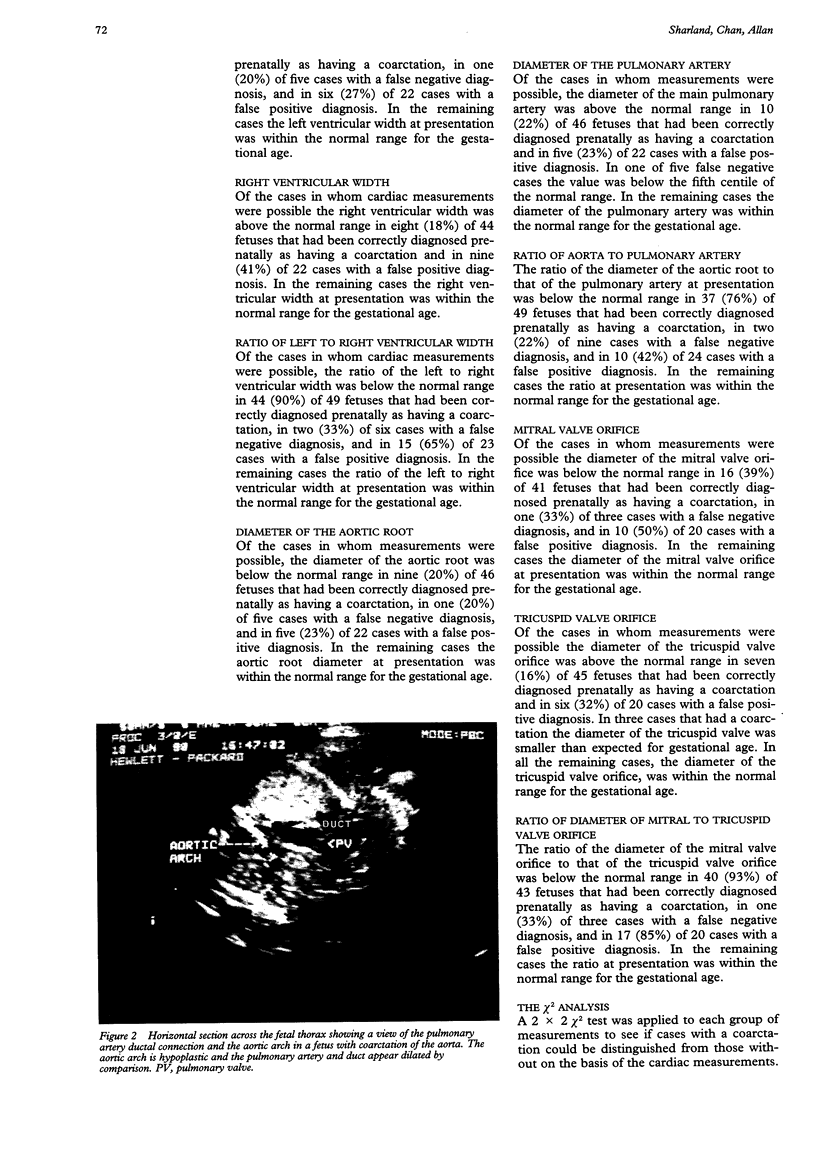
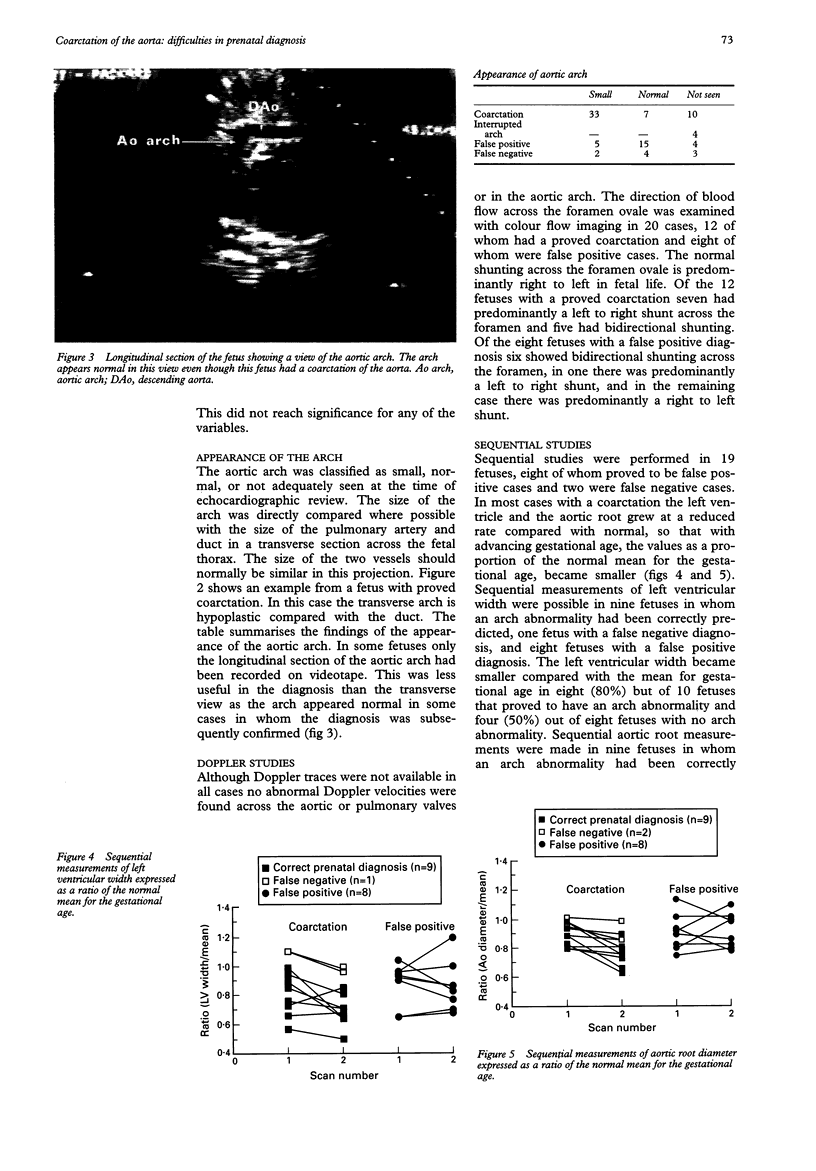
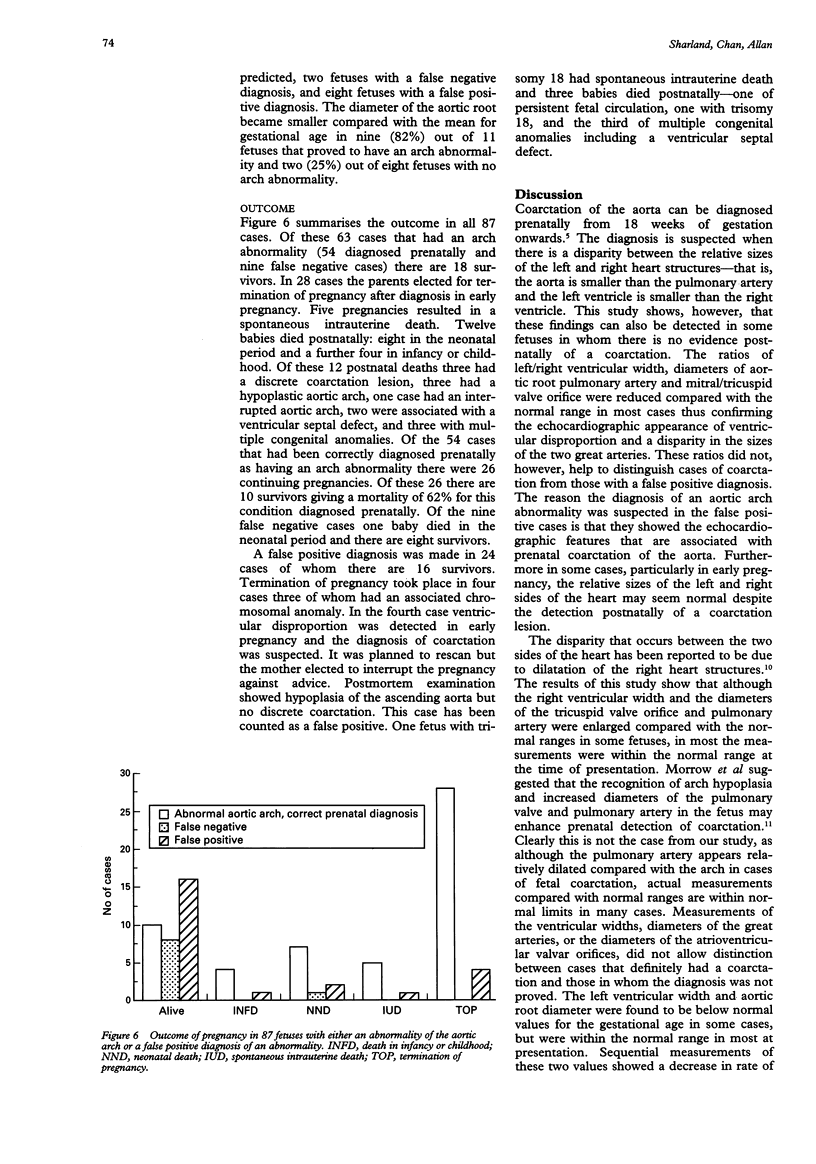
OBJECTIVE--To formulate echocardiographic criteria for the prenatal diagnosis of coarctation of the aorta. DESIGN--A retrospective study examining the echocardiograms of fetuses with a verified aortic arch abnormality and those in whom the diagnosis was suspected prenatally but was not subsequently confirmed. SETTING--Tertiary referral centre for fetal echocardiography. PATIENTS--87 fetuses in whom the diagnosis of coarctation was correctly made in 54, suspected but unproved in 24, and overlooked prenatally in nine. MAIN OUTCOME MEASURES--Measurements of left and right ventricular size, the diameters of the great arteries, the diameters of the left and right atrioventricular valvar orifices, the appearance of the aortic arch, and the direction of the flow of blood across the foramen ovale. RESULTS--Measurements of the ventricular widths, diameters of the great arteries, or the diameters of the atrioventricular valvar orifices, did not allow clear distinction between cases that definitely had a coarctation and those in whom the diagnosis was unproved. The appearance of the aortic arch, particularly in the horizontal projection, was more helpful in distinguishing cases of coarctation, although this also was not always diagnostic. A predominantly left to right shunt across the foramen ovale was detected more often in cases with a substantiated coarctation (58%) than in those with an unproved diagnosis (12%). CONCLUSIONS--The most severe forms of coarctation are associated with relative hypoplasia of the left heart structures compared with the right and a correct diagnosis can be made in early pregnancy. The milder forms of coarctation, however, are consistent with a normal early fetal echocardiogram. In late pregnancy it may be impossible to exclude coarctation categorically as the right heart structures may appear larger than the left in the normal fetus. Thus although a combination of echocardiographic features can correctly identify aortic arch anomalies in the fetus, none either alone or in combination, could clearly distinguish between real and false positive cases, particularly in late gestation.
Full text
PDF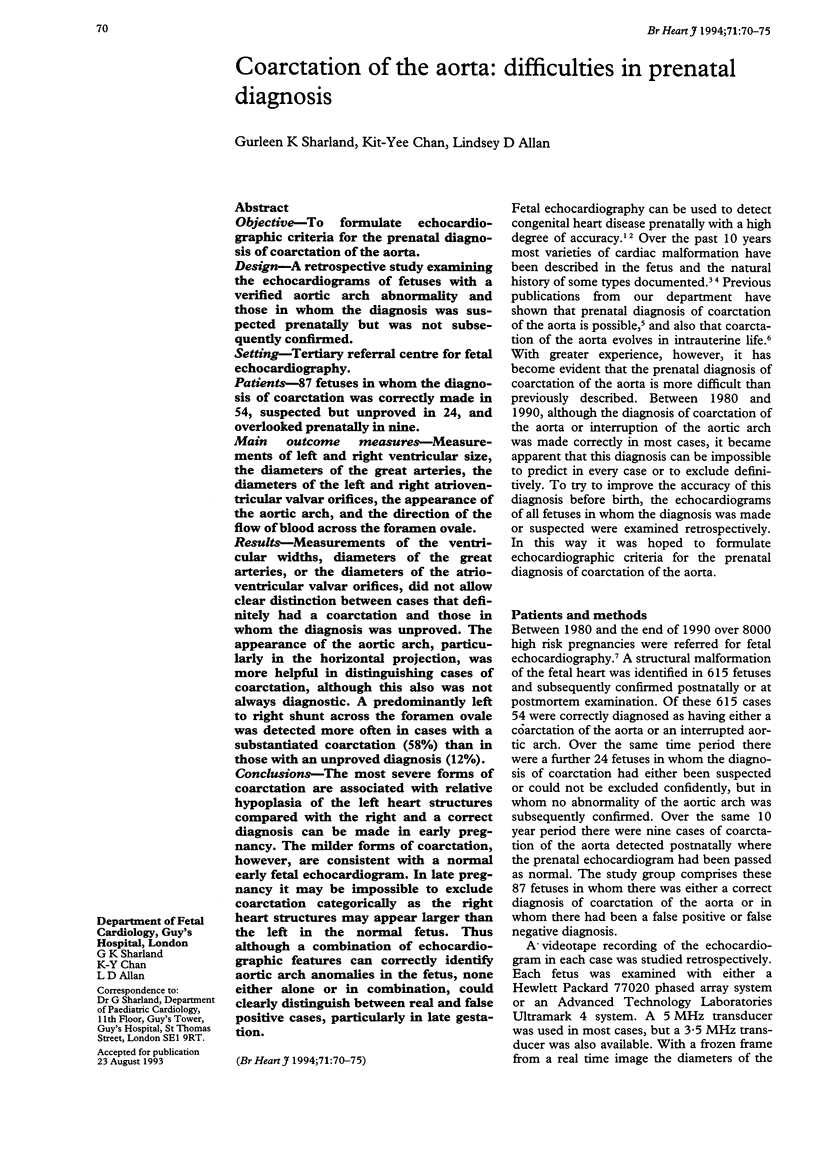
Images in this article

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Allan L. D., Chita S. K., Anderson R. H., Fagg N., Crawford D. C., Tynan M. J. Coarctation of the aorta in prenatal life: an echocardiographic, anatomical, and functional study. Br Heart J. 1988 Mar;59(3):356–360. doi: 10.1136/hrt.59.3.356. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Allan L. D., Crawford D. C., Anderson R. H., Tynan M. J. Echocardiographic and anatomical correlations in fetal congenital heart disease. Br Heart J. 1984 Nov;52(5):542–548. doi: 10.1136/hrt.52.5.542. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Allan L. D., Crawford D. C., Tynan M. Evolution of coarctation of the aorta in intrauterine life. Br Heart J. 1984 Oct;52(4):471–473. doi: 10.1136/hrt.52.4.471. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Allan L. D., Sharland G. K., Chita S. K., Lockhart S., Maxwell D. J. Chromosomal anomalies in fetal congenital heart disease. Ultrasound Obstet Gynecol. 1991 Jan 1;1(1):8–11. doi: 10.1046/j.1469-0705.1991.01010008.x. [DOI] [PubMed] [Google Scholar]
- Allan L. D., Sharland G., Tynan M. J. The natural history of the hypoplastic left heart syndrome. Int J Cardiol. 1989 Dec;25(3):341–343. doi: 10.1016/0167-5273(89)90226-x. [DOI] [PubMed] [Google Scholar]
- Copel J. A., Cullen M., Green J. J., Mahoney M. J., Hobbins J. C., Kleinman C. S. The frequency of aneuploidy in prenatally diagnosed congenital heart disease: an indication for fetal karyotyping. Am J Obstet Gynecol. 1988 Feb;158(2):409–413. doi: 10.1016/0002-9378(88)90166-4. [DOI] [PubMed] [Google Scholar]
- Feit L. R., Copel J. A., Kleinman C. S. Foramen ovale size in the normal and abnormal human fetal heart: an indicator of transatrial flow physiology. Ultrasound Obstet Gynecol. 1991 Sep 1;1(5):313–319. doi: 10.1046/j.1469-0705.1991.01050313.x. [DOI] [PubMed] [Google Scholar]
- Kleinman C. S., Hobbins J. C., Jaffe C. C., Lynch D. C., Talner N. S. Echocardiographic studies of the human fetus: prenatal diagnosis of congenital heart disease and cardiac dysrhythmias. Pediatrics. 1980 Jun;65(6):1059–1067. [PubMed] [Google Scholar]
- Morrow W. R., Huhta J. C., Murphy D. J., Jr, McNamara D. G. Quantitative morphology of the aortic arch in neonatal coarctation. J Am Coll Cardiol. 1986 Sep;8(3):616–620. doi: 10.1016/s0735-1097(86)80191-7. [DOI] [PubMed] [Google Scholar]
- Sharland G. K., Allan L. D. Normal fetal cardiac measurements derived by cross-sectional echocardiography. Ultrasound Obstet Gynecol. 1992 May 1;2(3):175–181. doi: 10.1046/j.1469-0705.1992.02030175.x. [DOI] [PubMed] [Google Scholar]
- Sharland G. K., Chita S. K., Allan L. D. The use of colour Doppler in fetal echocardiography. Int J Cardiol. 1990 Aug;28(2):229–236. doi: 10.1016/0167-5273(90)90065-d. [DOI] [PubMed] [Google Scholar]
- Sharland G. K., Chita S. K., Allan L. D. Tricuspid valve dysplasia or displacement in intrauterine life. J Am Coll Cardiol. 1991 Mar 15;17(4):944–949. doi: 10.1016/0735-1097(91)90877-c. [DOI] [PubMed] [Google Scholar]