

Abstract
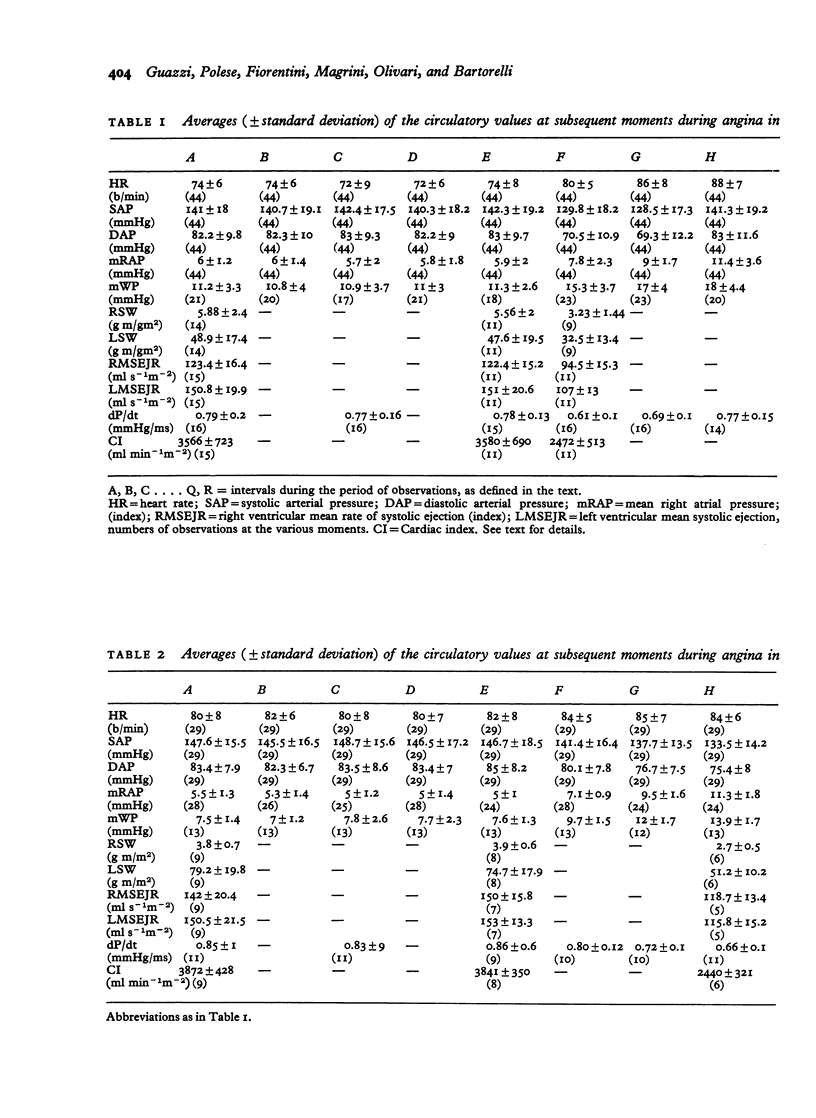
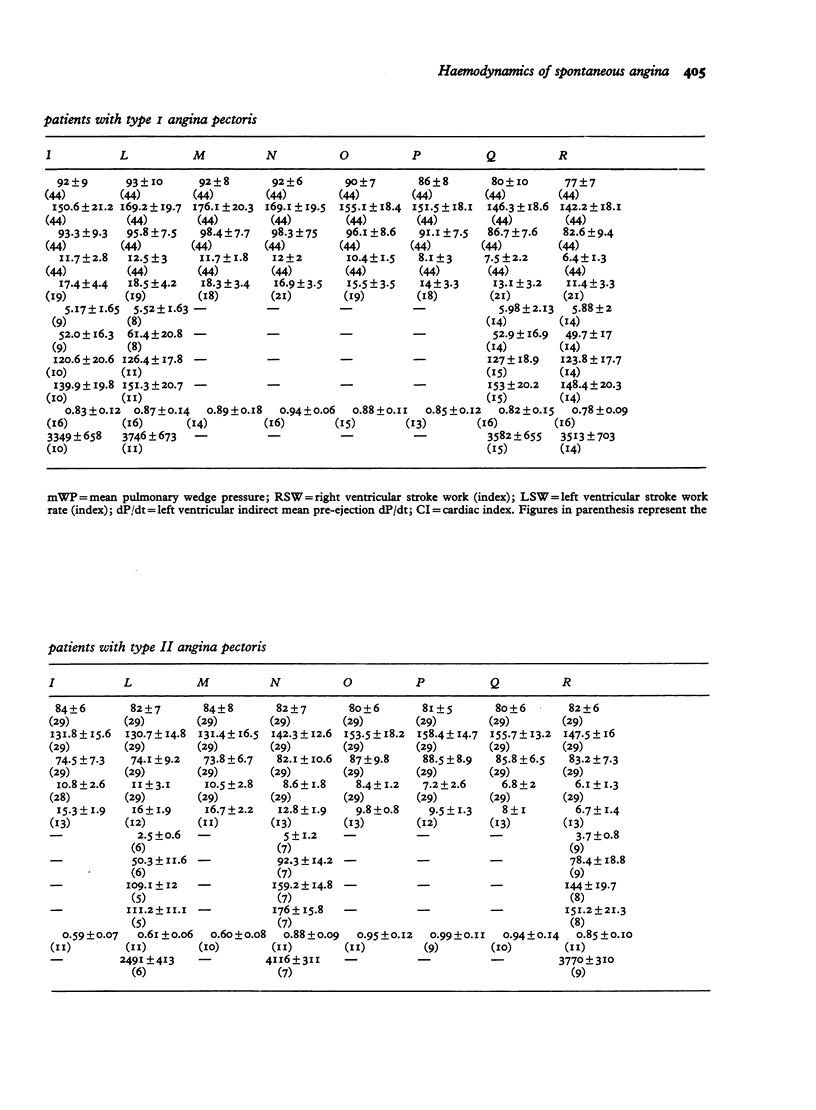
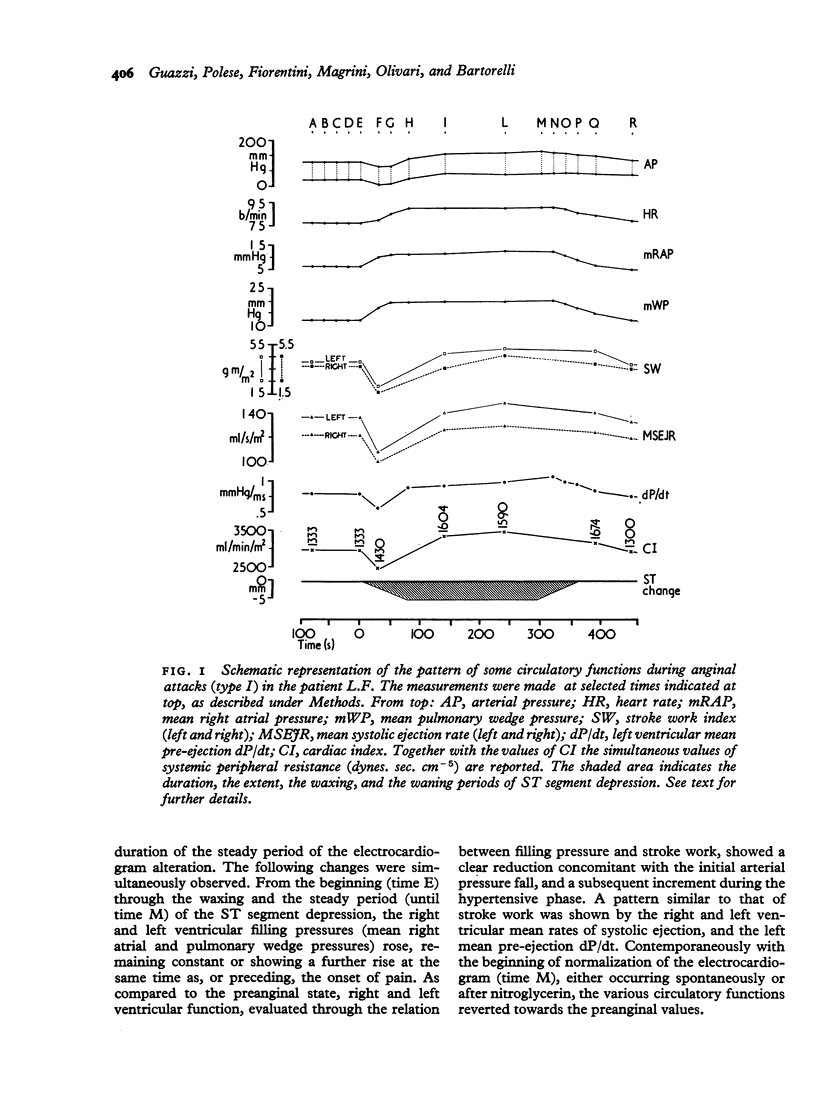
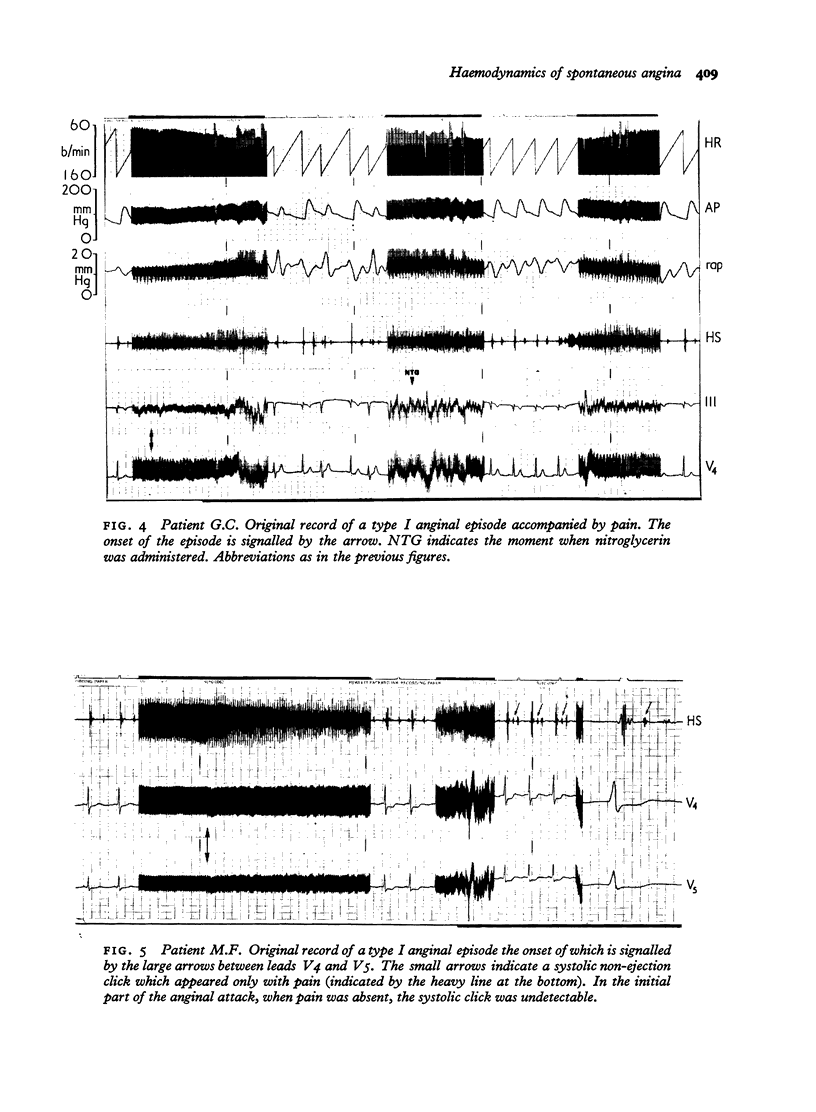
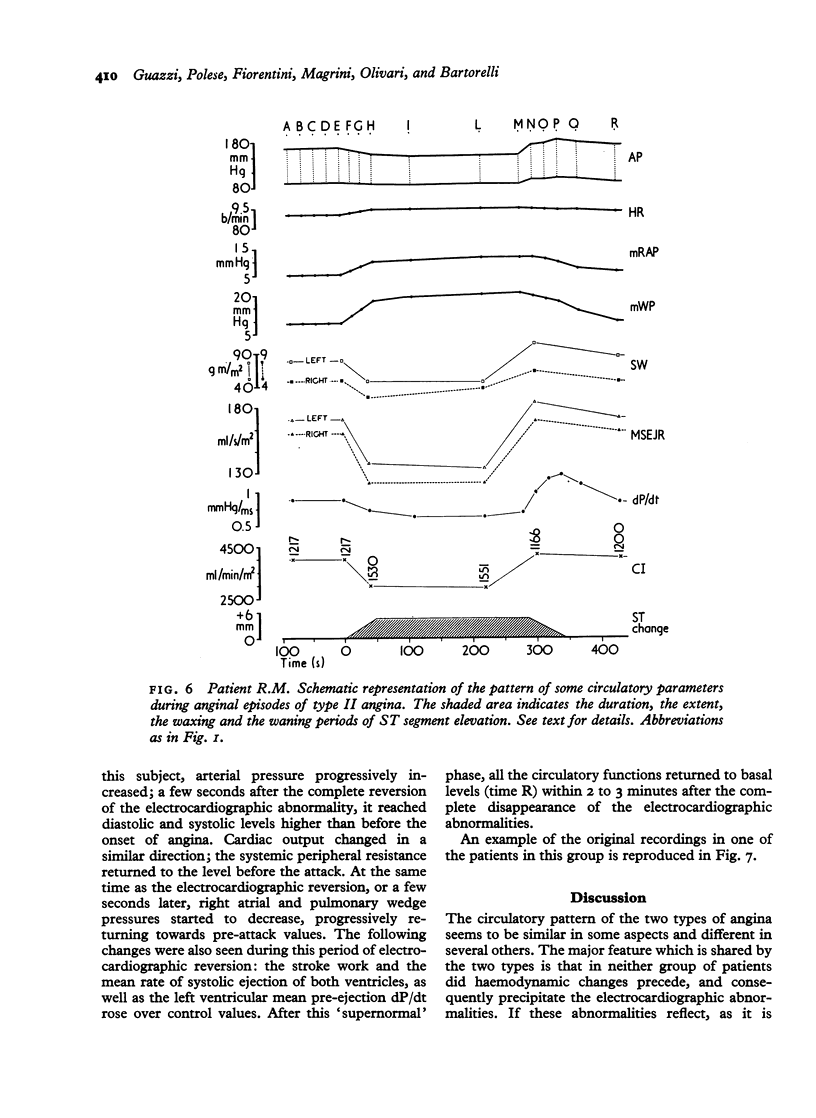
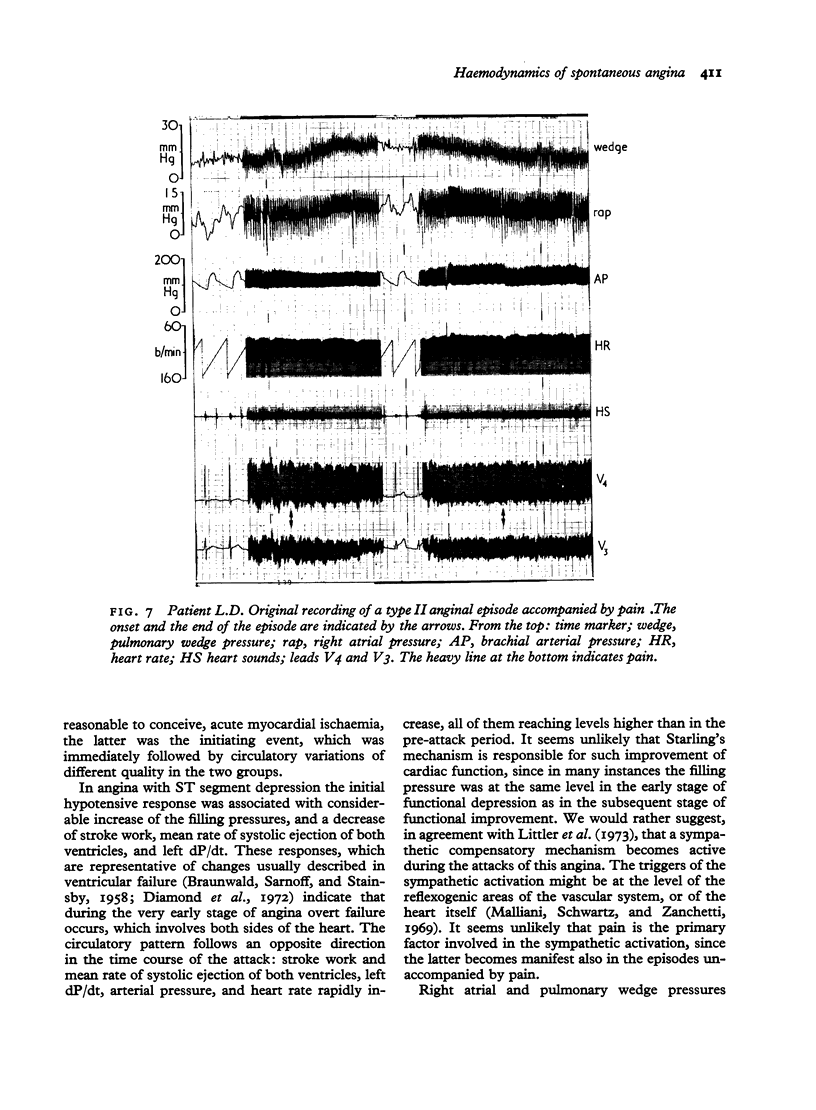
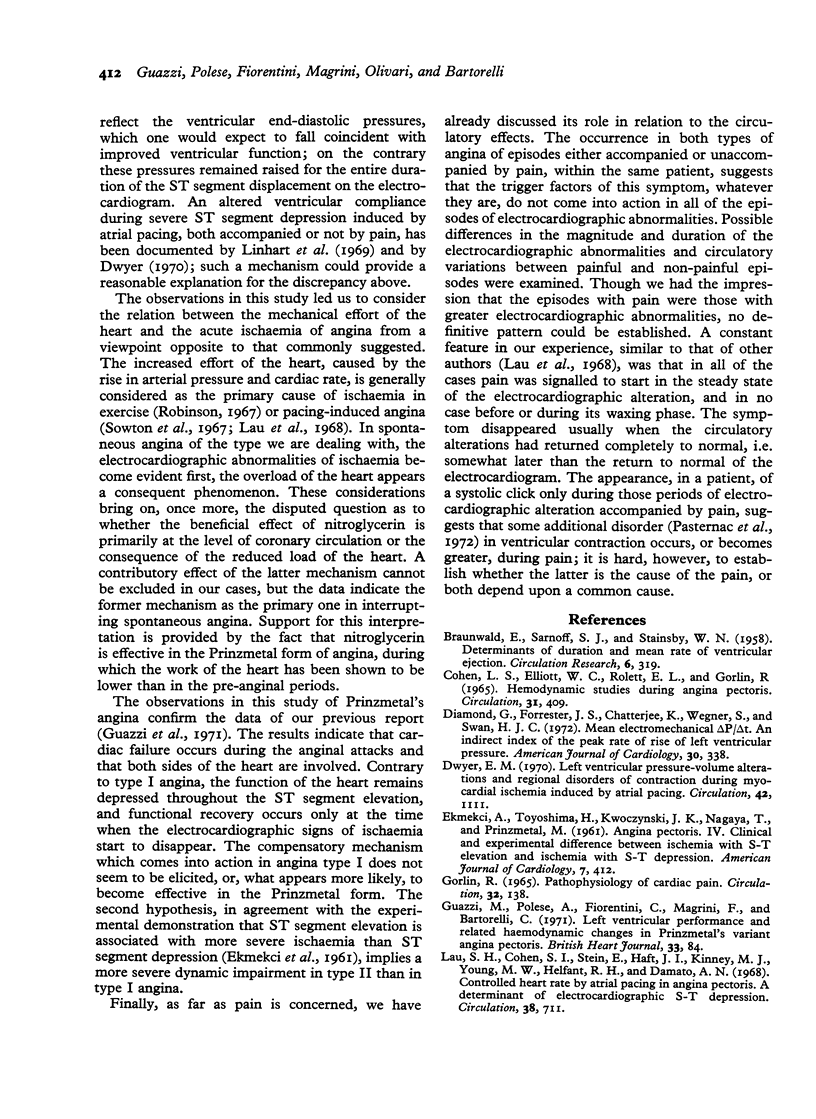
The function of both right and left sides of the heart was studied during spontaneous attacks of angina pectoris at rest in 7 patients showing ST depression (type I) and 4 showing ST elevation (type II) during the attack. In none of the 44 type I attacks and 29 type II attacks which were recorded did circulatory changes; the latter were different in the two groups. Type I attacks showed: a) a brief fall in arterial pressure, accompanied by b) a rise of right atrial and pulmonary wedge pressures and c) a decrease of cardiac output, right and left stroke work, the mean rate of systolic ejection, and indirect left ventricular pre-ejection dP/dt. In the course of the attack a hypertensive phase followed, which was paralleled by an increase of heart rate, cardiac output, left and right stroke work, and mean systolic ejection rate, left dP/dt; right atrial pressure and wedge pressure remained raised. All of the circulatory functions started to revert towards the pre-attack levels coincident with the waning phase of the electrocardiographic alteration, the latter occurring either spontaneously or after nitroglycerin. Type II attacks for the entire duration of the electrocardiographic changes showed: a) a reduction of arterial pressure, cardiac output, right and left stroke work, mean systolic ejection rate, and left dP/dt, b) a rise of right atrial and wedge pressures, and c) quite small changes of heart rate. When the electrocardiogram started to revert to the pre-attack aspect, the cardiac function rapidly improved and, after a supernormal phase, returned to the basal levels in about 2 minutes. It is concluded: 1) that no circulatory factor interfering with the mechanical effort of the heart is responsible for eliciting spontaneous angina: 2) that in type I attacks right and left ventricular impairment occurs which recovers rapidly, possibly through a sympathetic compensation; 3) that in type II attachs dysfunction of both sides of the heart occurs and persists throughout the episode of electrocardiographic alteration; 4) that the dynamic impairment is probably more severe in type I than in type II angina.
Full text
PDF

Images in this article

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- BRAUNWALD E., SARNOFF S. J., STAINSBY W. N. Determinants of duration and mean rate of ventricular ejection. Circ Res. 1958 May;6(3):319–325. doi: 10.1161/01.res.6.3.319. [DOI] [PubMed] [Google Scholar]
- COHEN L. S., ELLIOTT W. C., ROLETT E. L., GORLIN R. HEMODYNAMIC STUDIES DURING ANGINA PECTORIS. Circulation. 1965 Mar;31:409–416. doi: 10.1161/01.cir.31.3.409. [DOI] [PubMed] [Google Scholar]
- Diamond G., Forrester J. S., Chatterjee K., Wegner S., Swan H. J. Mean electromechanical P- t: an indirect index of the peak rate of rise of left ventricular pressure. Am J Cardiol. 1972 Sep;30(4):338–342. doi: 10.1016/0002-9149(72)90562-0. [DOI] [PubMed] [Google Scholar]
- Dwyer E. M., Jr Left ventricular pressure-volume alterations and regional disorders of contraction during myocardial ischemia induced by atrial pacing. Circulation. 1970 Dec;42(6):1111–1122. doi: 10.1161/01.cir.42.6.1111. [DOI] [PubMed] [Google Scholar]
- EKMEKCI A., TOYOSHIMA H., KWOCZYNSKI J. K., NAGAYA T., PRINZMETAL M. Angina pectoris. IV. Clinical and experimental difference between ischemia with S-T elevation and ischemia with S-T depression. Am J Cardiol. 1961 Mar;7:412–426. doi: 10.1016/0002-9149(61)90485-4. [DOI] [PubMed] [Google Scholar]
- GORLIN R. PATHOPHYSIOLOGY OF CARDIAC PAIN. Circulation. 1965 Jul;32:138–148. doi: 10.1161/01.cir.32.1.138. [DOI] [PubMed] [Google Scholar]
- Lau S. H., Cohen S. I., Stein E., Haft J. I., Kinney M. J., Young M. W., Helfant R. H., Damato A. N. Controlled heart rate by atrial pacing in angina pectoris. A determinant of electrocardiographic S-T depression. Circulation. 1968 Oct;38(4):711–720. doi: 10.1161/01.cir.38.4.711. [DOI] [PubMed] [Google Scholar]
- Linhart J. W., Hildner F. J., Barold S. S., Listejw, Samet P. Left heart hemodynamics during angina pectoris induced by atrial pacing. Circulation. 1969 Oct;40(4):483–492. doi: 10.1161/01.cir.40.4.483. [DOI] [PubMed] [Google Scholar]
- MULLER O., RORVIK K. Haemodynamic consequences of coronary heart disease with observations during anginal pain and on the effect of nitroglycerine. Br Heart J. 1958 Jul;20(3):302–310. doi: 10.1136/hrt.20.3.302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Malliani A., Schwartz P. J., Zanchetti A. A sympathetic reflex elicited by experimental coronary occlusion. Am J Physiol. 1969 Sep;217(3):703–709. doi: 10.1152/ajplegacy.1969.217.3.703. [DOI] [PubMed] [Google Scholar]
- PRINZMETAL M., KENNAMER R., MERLISS R., WADA T., BOR N. Angina pectoris. I. A variant form of angina pectoris; preliminary report. Am J Med. 1959 Sep;27:375–388. doi: 10.1016/0002-9343(59)90003-8. [DOI] [PubMed] [Google Scholar]
- Pasternac A., Gorlin R., Sonnenblick E. H., Haft J. I., Kemp H. G. Abnormalities of ventricular motion induced by atrial pacing in coronary artery disease. Circulation. 1972 Jun;45(6):1195–1205. doi: 10.1161/01.cir.45.6.1195. [DOI] [PubMed] [Google Scholar]
- Robinson B. F. Relation of heart rate and systolic blood pressure to the onset of pain in angina pectoris. Circulation. 1967 Jun;35(6):1073–1083. doi: 10.1161/01.cir.35.6.1073. [DOI] [PubMed] [Google Scholar]
- Rosland G. A. Haemodynamic observations during spontaneous angina pectoris. Br Heart J. 1969 Jul;31(4):523–525. doi: 10.1136/hrt.31.4.523. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sowton G. E., Balcon R., Cross D., Frick M. H. Measurement of the angina threshold using atrial pacing. A new technique for the study of angina pectoris. Cardiovasc Res. 1967 Oct;1(4):301–307. doi: 10.1093/cvr/1.4.301. [DOI] [PubMed] [Google Scholar]
- Swan H. J., Ganz W., Forrester J., Marcus H., Diamond G., Chonette D. Catheterization of the heart in man with use of a flow-directed balloon-tipped catheter. N Engl J Med. 1970 Aug 27;283(9):447–451. doi: 10.1056/NEJM197008272830902. [DOI] [PubMed] [Google Scholar]
- Weissler A. M., Harris W. S., Schoenfeld C. D. Systolic time intervals in heart failure in man. Circulation. 1968 Feb;37(2):149–159. doi: 10.1161/01.cir.37.2.149. [DOI] [PubMed] [Google Scholar]