

A 15-year-old Indian girl presented with dysphagia, oropharyngeal dystonic movements, brisk reflexes, and unsteadiness in tandem walking over years.
MRI revealed T2-weighted hyperintensity in the corpora striata (figure 1). Following treatment, imaging at 2 months and 2 years showed improvement in the corpus striatal hyperintensity with residual cystic damage (figure 2). Muscle biopsy was normal.
Figure 1. Coronal and axial T2-weighted MRI at presentation.
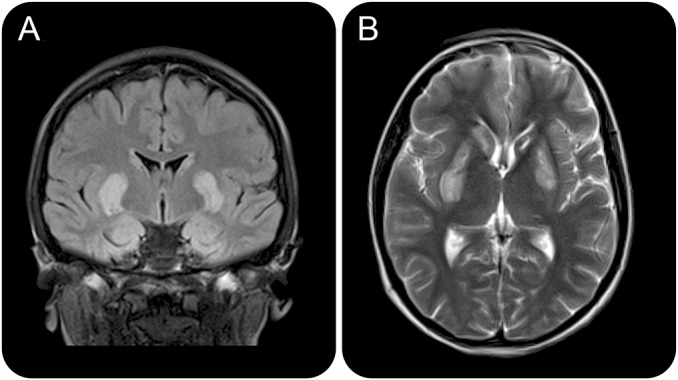
Coronal fluid-attenuated inversion recovery (A) and axial T2-weighted (B) MRI slices at presentation showing relatively symmetric hyperintensity in the corpora striata, and apparent cystic changes in the left head of caudate.
Figure 2. Coronal and axial T2-weighted MRI 2 months and 2 years after treatment.
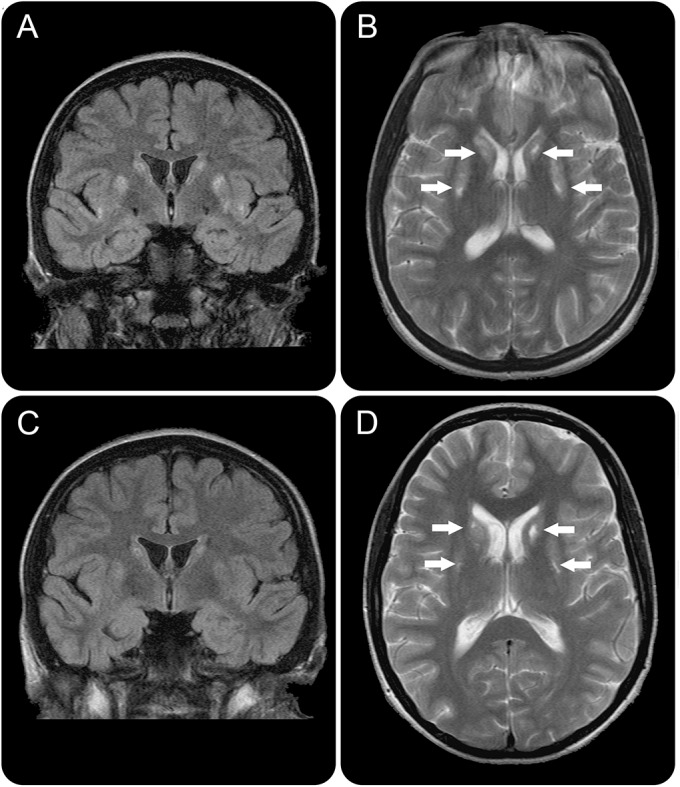
Coronal and Axial T2-weighted MRI slices showing symmetrical hyperintensities in the corpora striata at 2 months (A and B) and 2 years (C and D) after biotin and thiamine treatment, demonstrating a progressive reduction in the corpus striatal hyperintensity with residual small areas of cystic damage (white arrows).
Genetic testing confirmed biotin-responsive basal ganglia disease, which is secondary to mutations in the SLC19A3 thiamine transporter gene, usually in Middle Eastern and Indian patients.1,2 Untreated, it can progress to dystonia, quadriparesis, and coma.1 Biotin and thiamine therapy significantly improved the patient's clinical condition.2
Supplementary Material
Footnotes
Download teaching slides: Neurology.org
AUTHOR CONTRIBUTIONS
J.S.: study design and concept, analysis and interpretation of data/images, drafting the manuscript. R.L.: analysis and interpretation of data/images, drafting and revising the manuscript. I.D.: study design and concept, analysis and interpretation of data/images, drafting and revising the manuscript, study supervision.
STUDY FUNDING
No targeted funding reported.
DISCLOSURE
J. Schwarting and R. Lakshmanan report no disclosures relevant to the manuscript. I. Davagnanam is funded by the NIHR UCL/UCLH Biomedical Research Centre. Go to Neurology.org for full disclosures.
REFERENCES
- 1.Tabarki B, Al-Shafi S, Al-Shahwan S, et al. Biotin-responsive basal ganglia disease revisited: clinical, radiologic, and genetic findings. Neurology 2013;80:261–267. [DOI] [PubMed] [Google Scholar]
- 2.Tabarki B, Alfadhel M, AlShahwan S, Hundallah K, AlShafi S, AlHashem A. Treatment of biotin-responsive basal ganglia disease: open comparative study between the combination of biotin plus thiamine versus thiamine alone. Eur J Paediatr Neurol 2015;19:547–552. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.