

Abstract
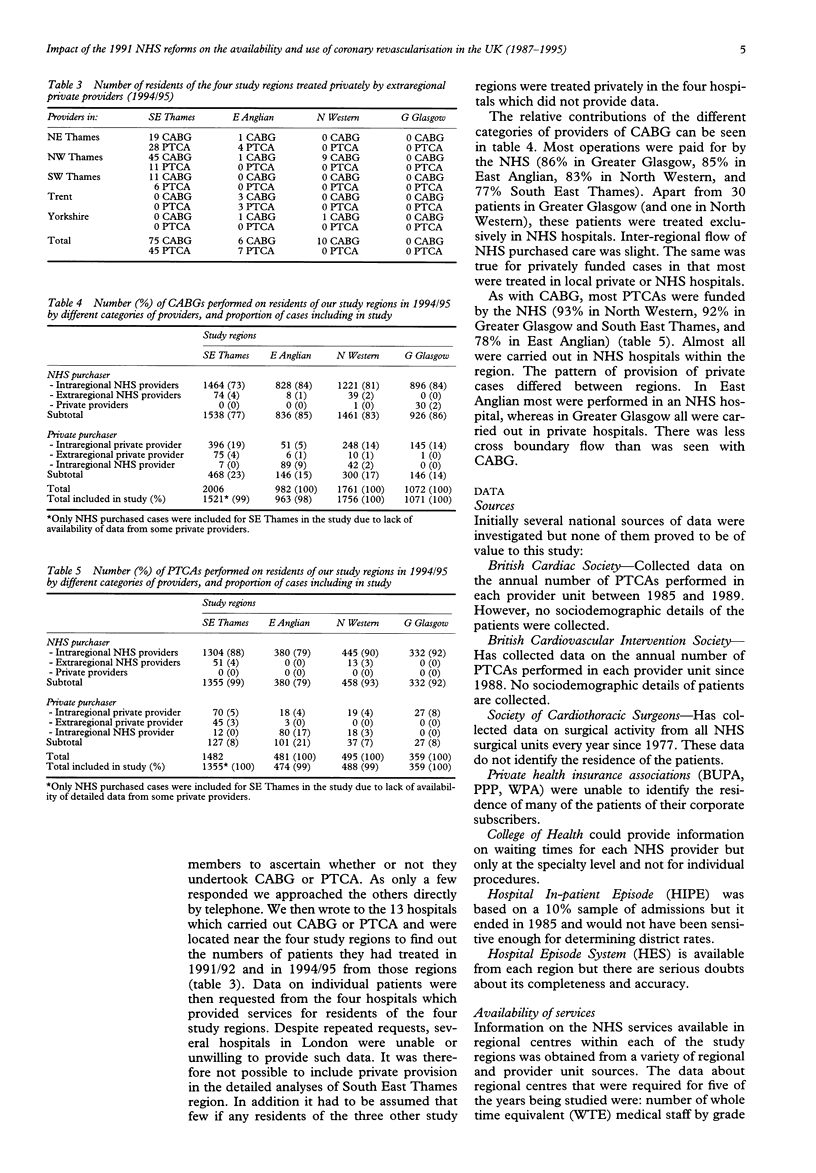
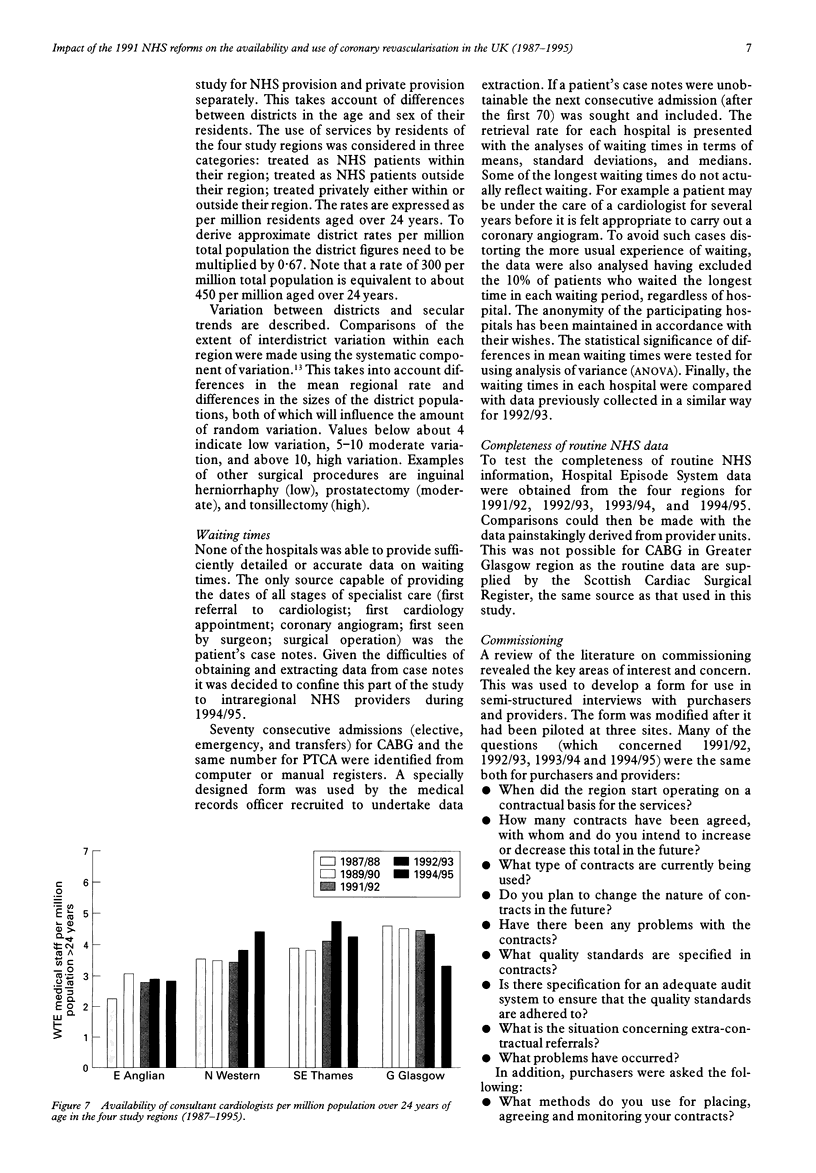
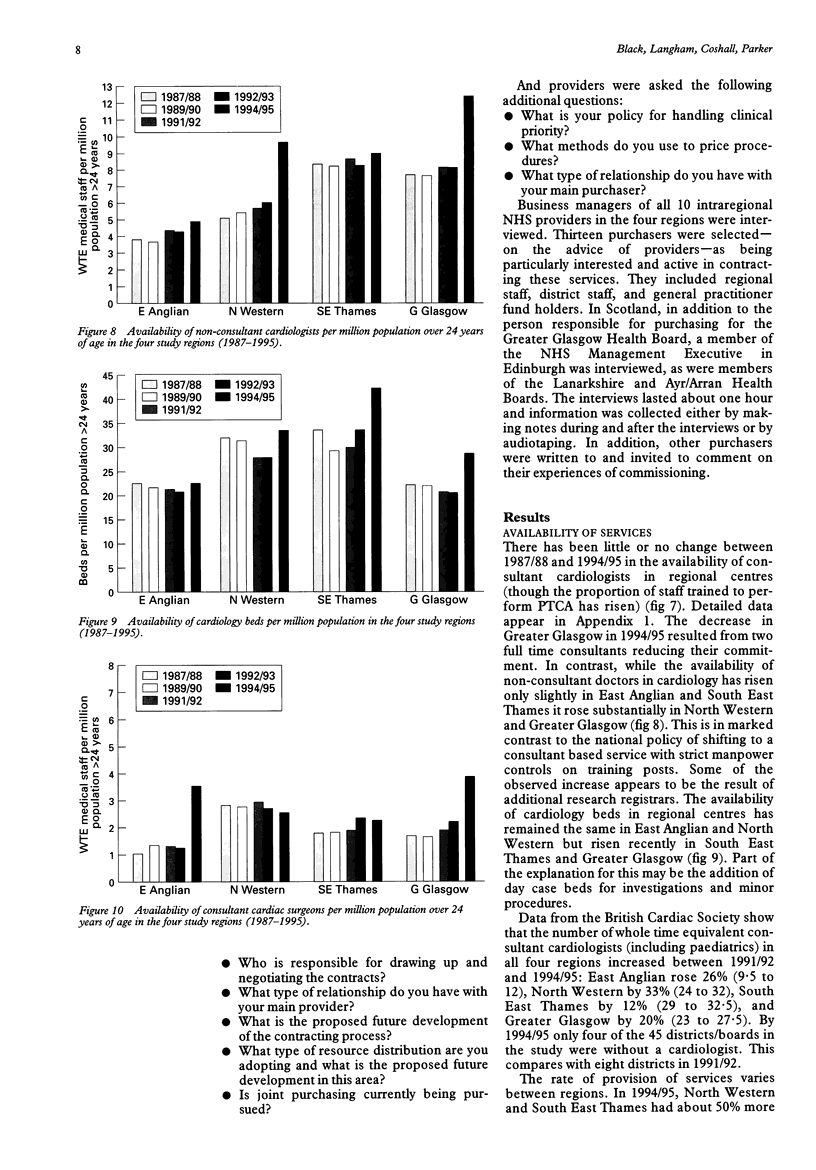
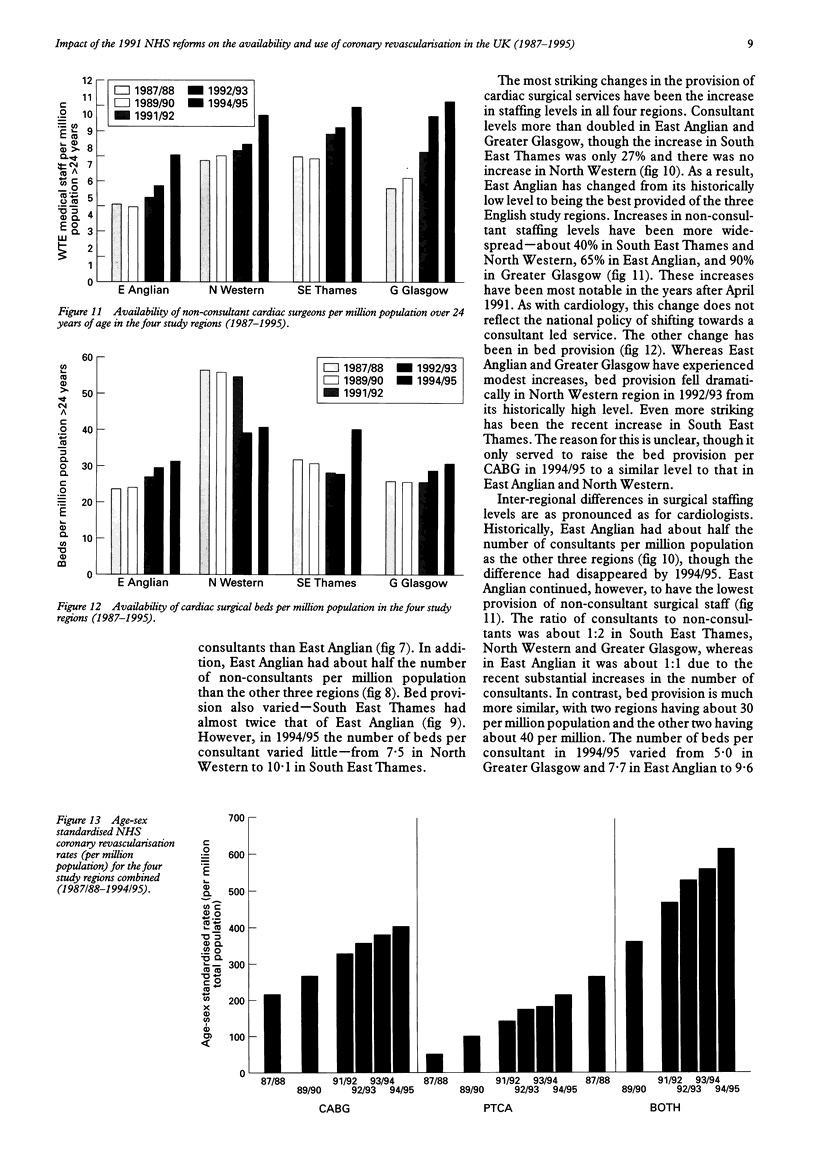
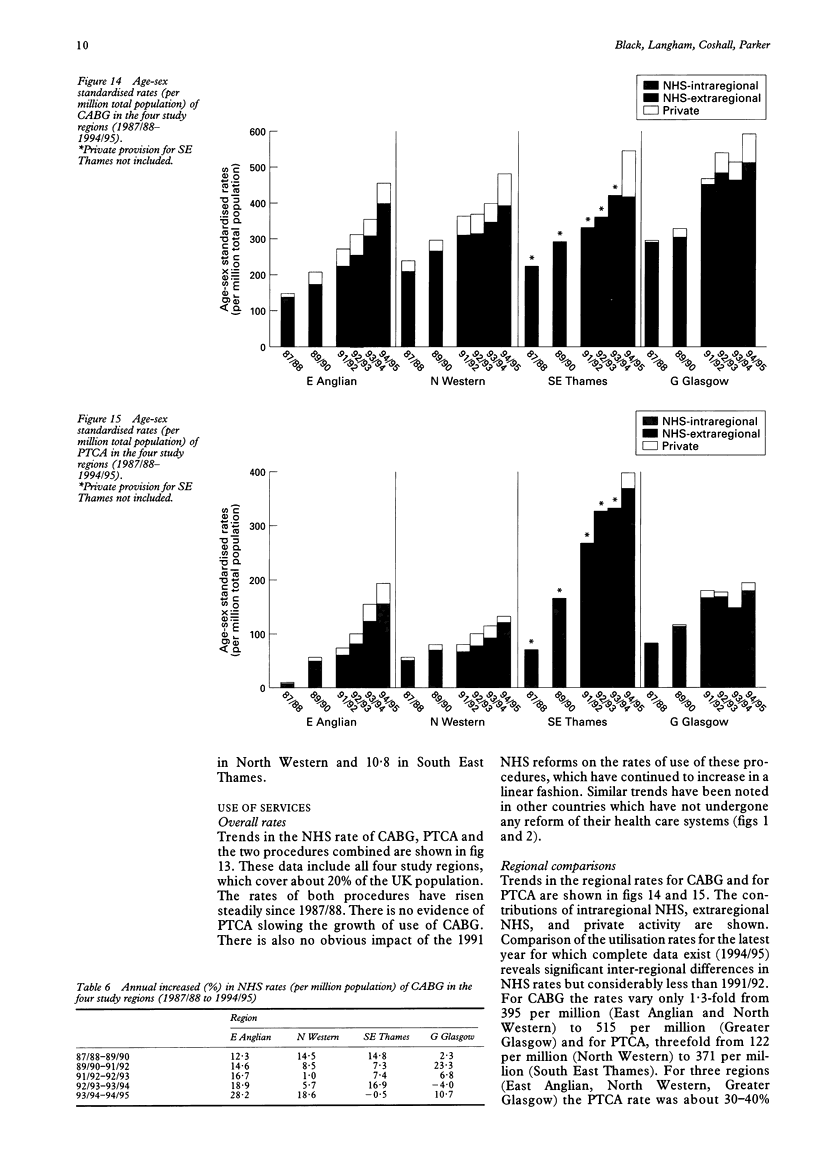
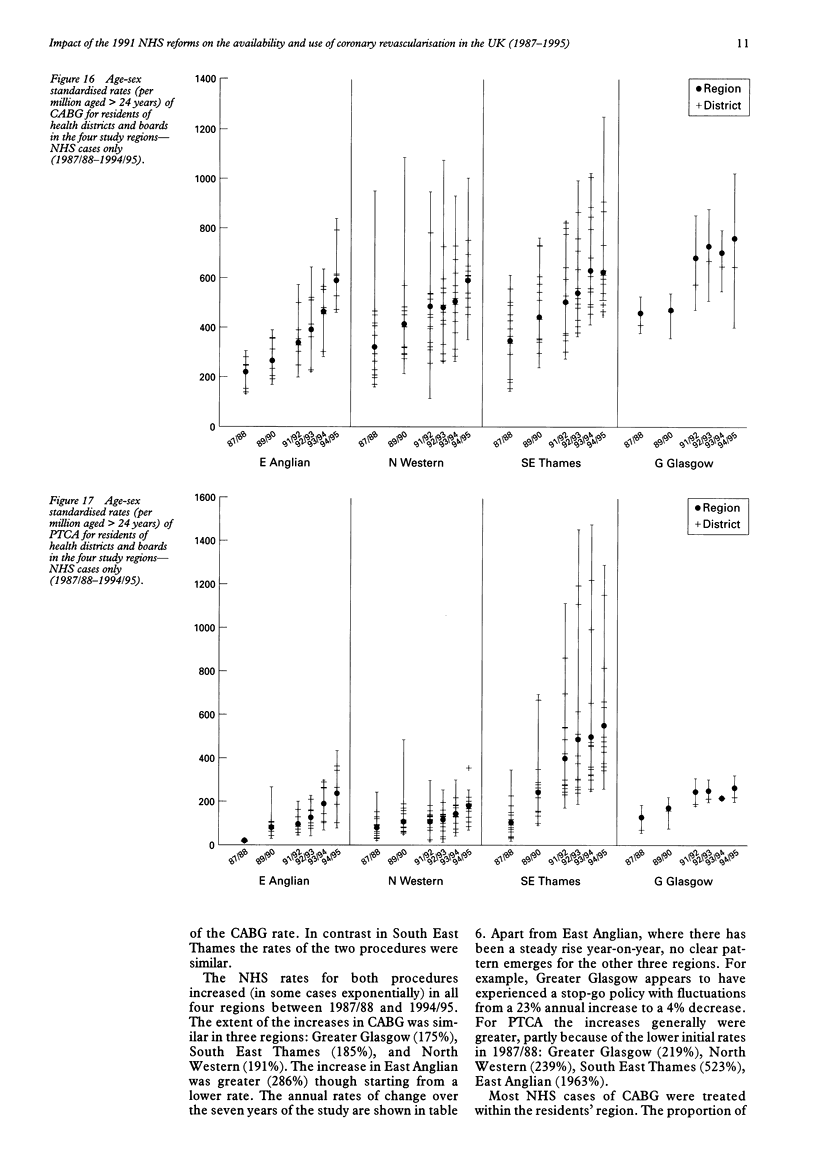
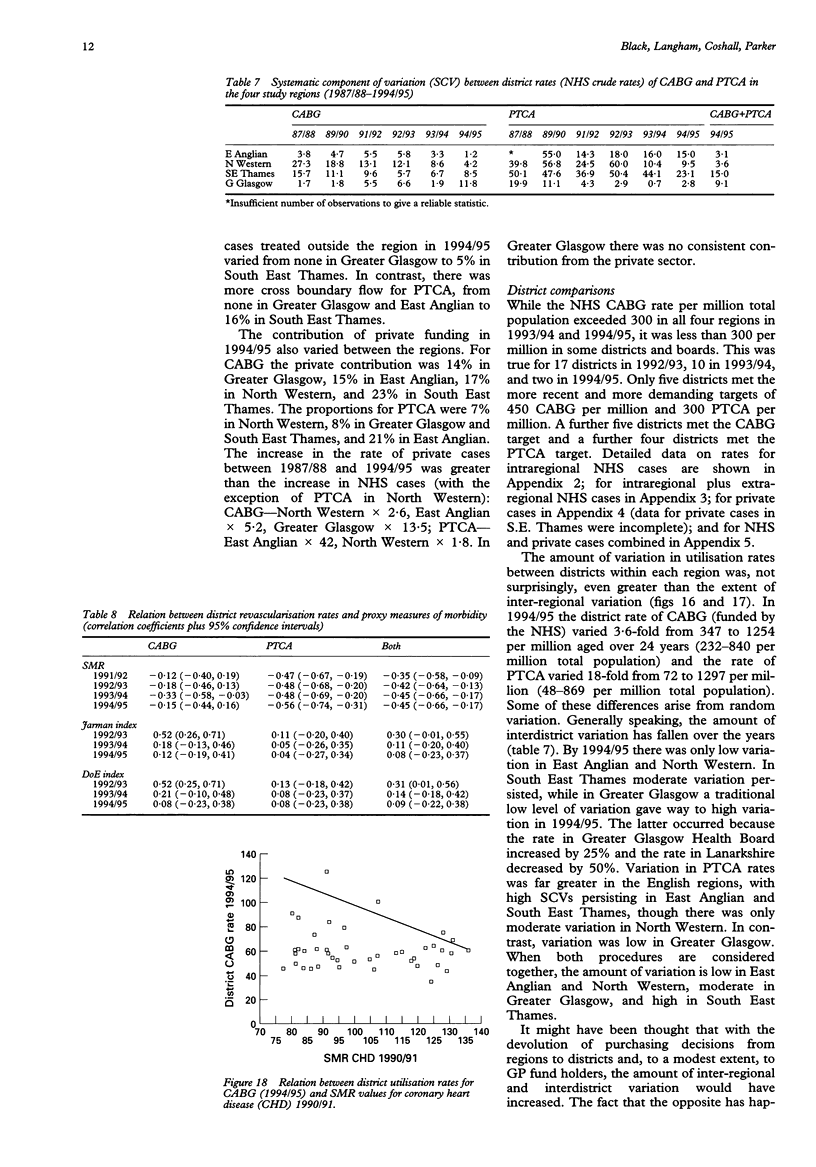
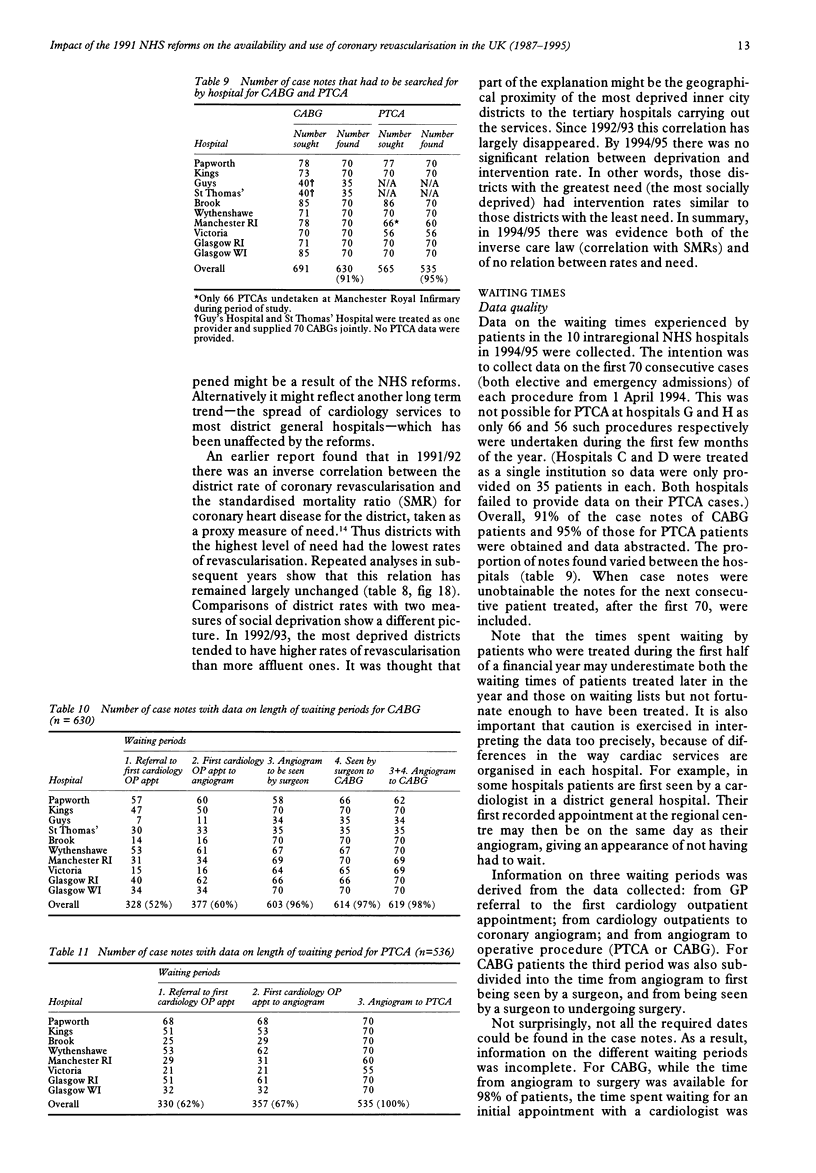
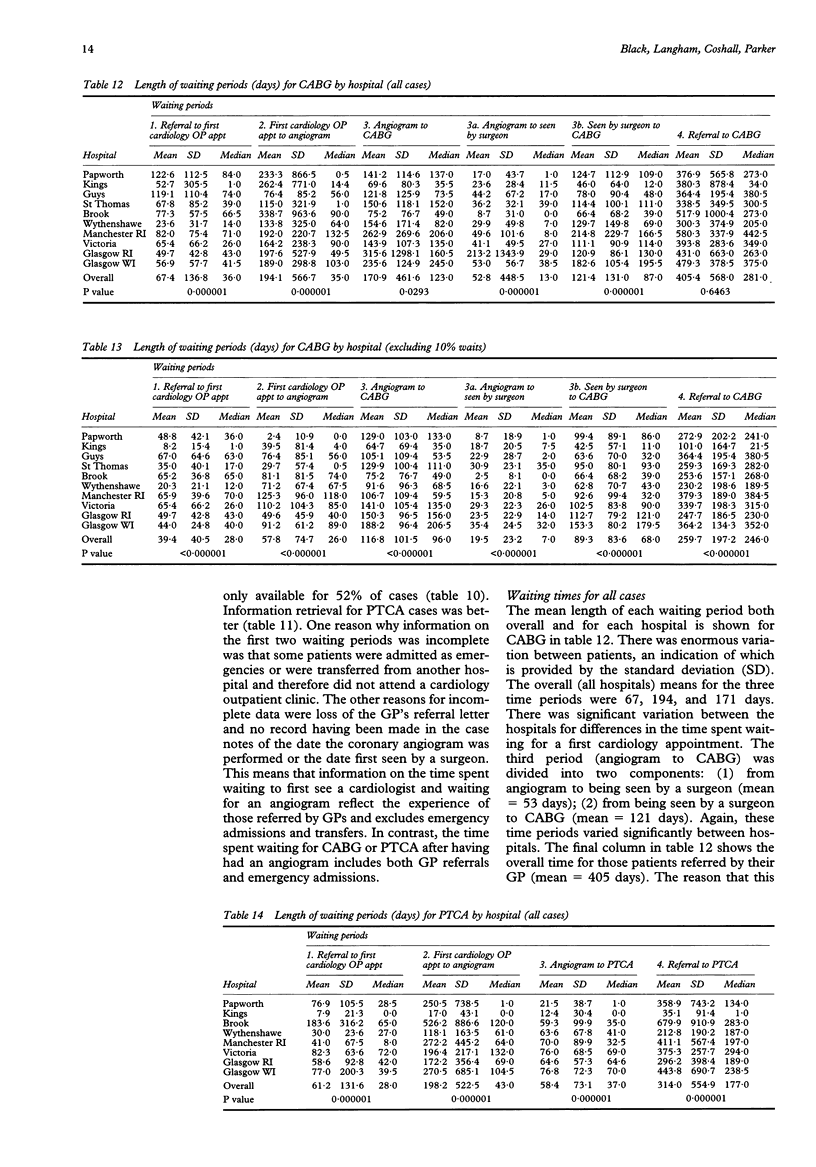
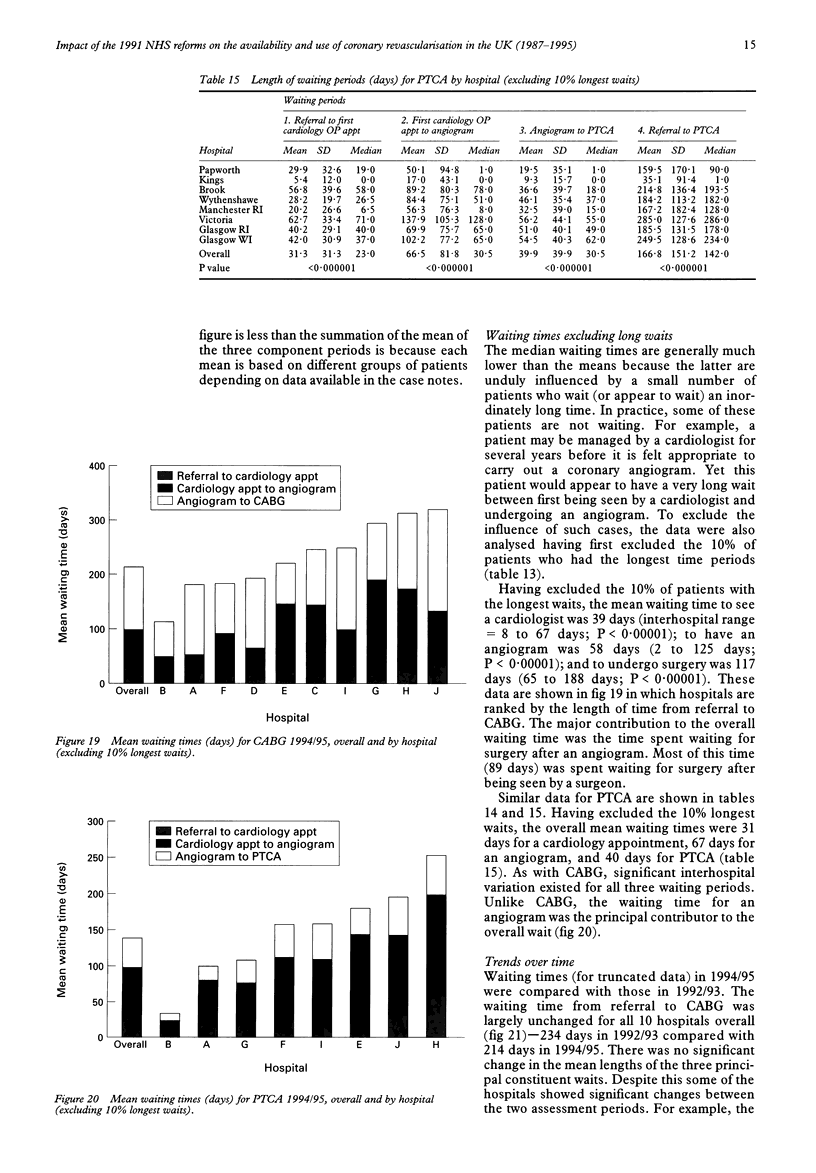
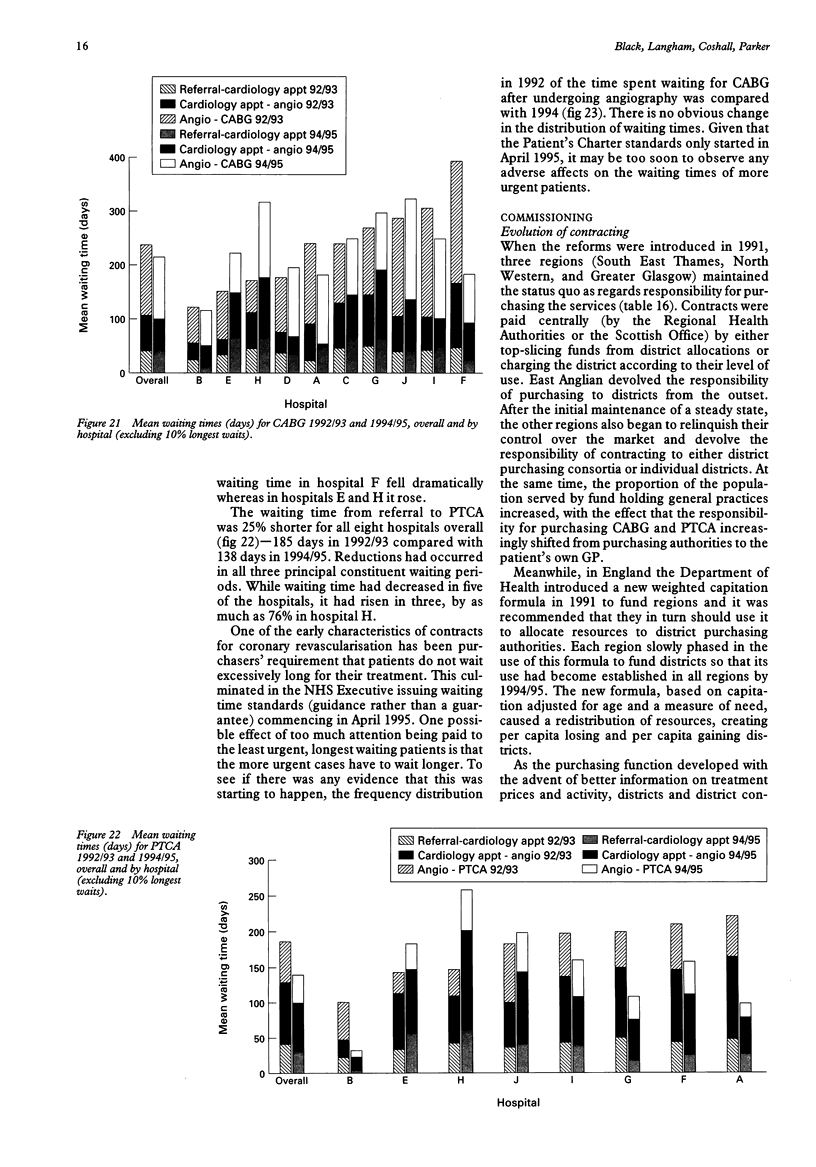
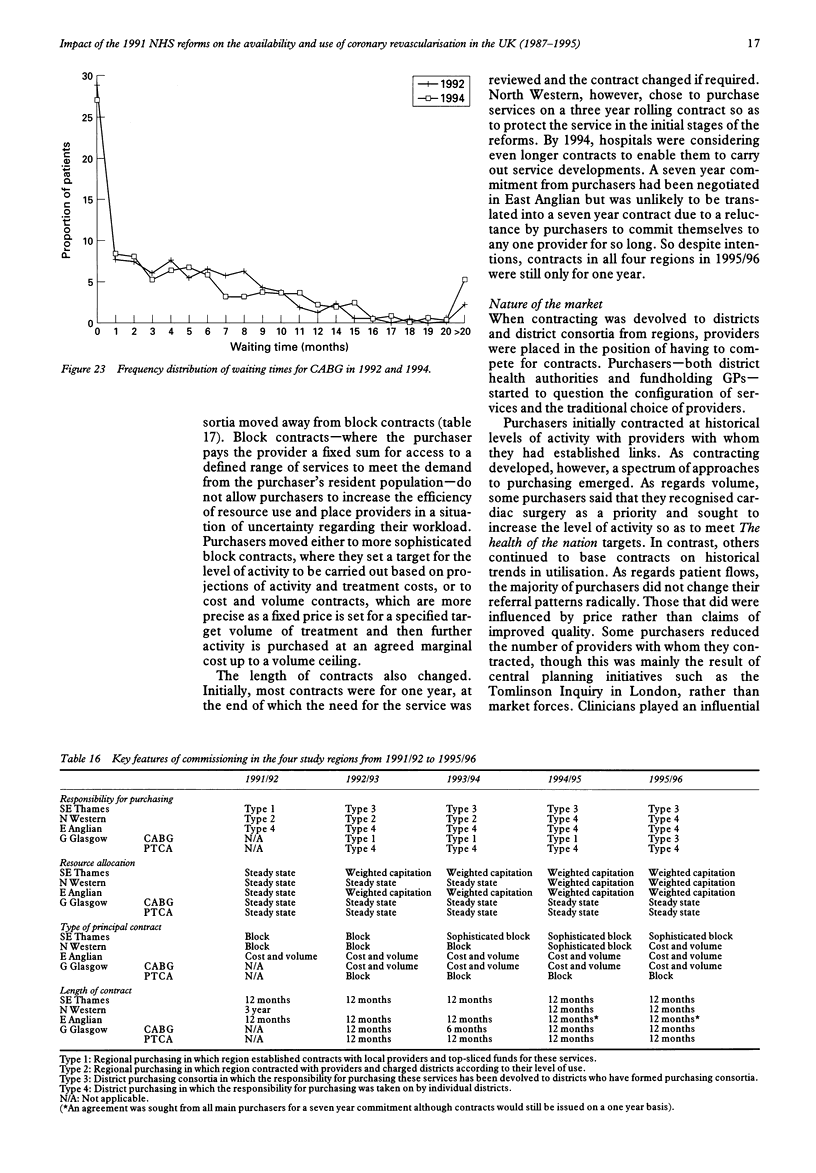
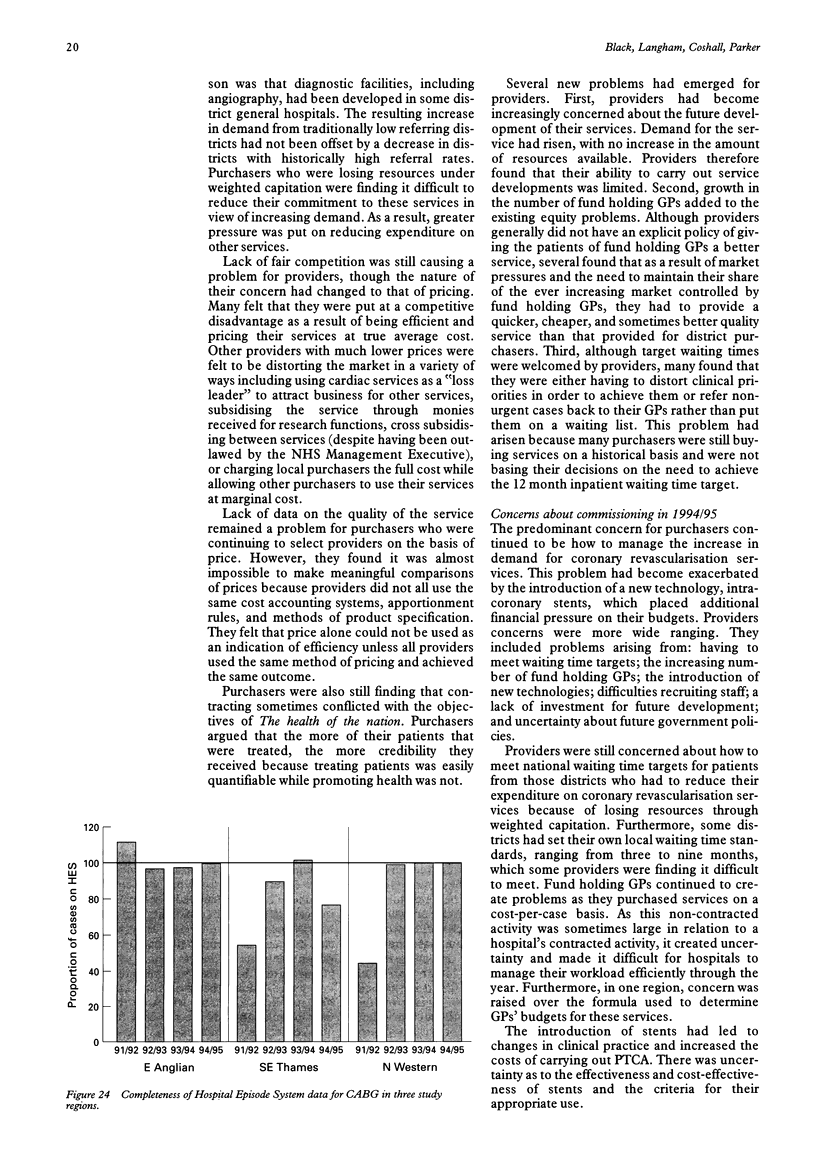
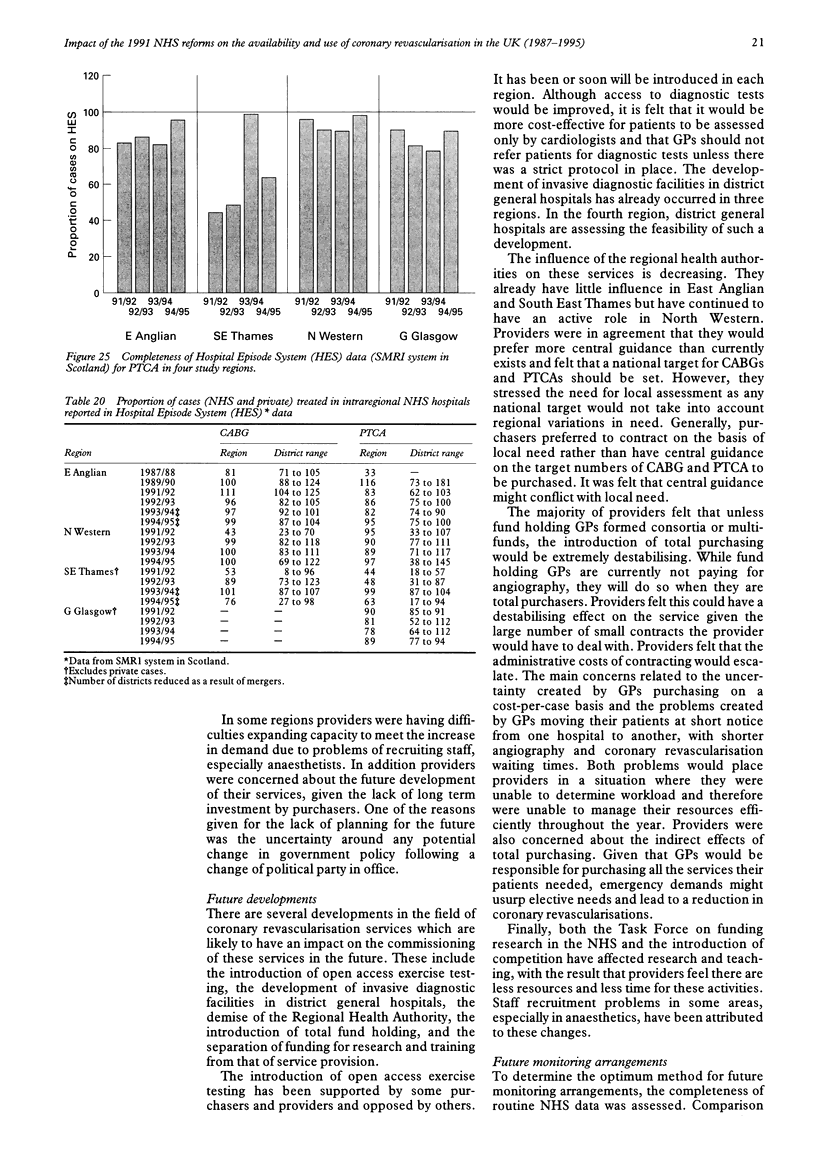
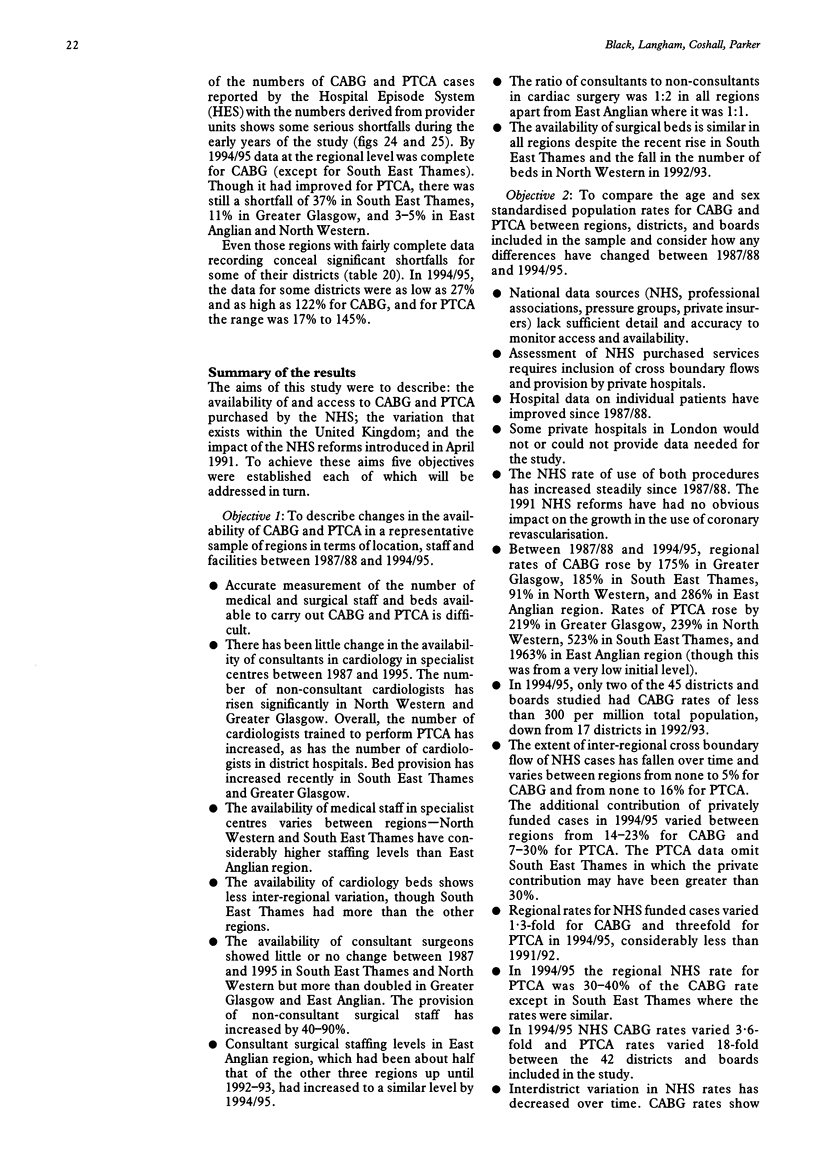
Objective—To describe changes in the availability, utilisation, and waiting times for coronary artery bypass grafting (CABG) and percutaneous transluminal coronary angioplasty (PTCA) between 1987/88 and 1994/95 and to review commissioning of these services. Design—A series of cross sectional surveys and interviews with purchasers and providers. Setting—Four health regions in the United Kingdom. Patients—All residents aged 25 years or more who underwent coronary revascularisation. Results—There has been little change in the availability of consultants in cardiology in specialist centres, while the number of non-consultant cardiologists has risen significantly. The availability of consultant surgeons more than doubled in some regions, while non-consultant surgical staff increased by 40–90%. The NHS rate of use of both CABG and PTCA has increased steadily since 1987/88. In 1994/95, only two districts had CABG rates of less than 300 per million population. The additional contribution of privately funded cases varied between 14–23% for CABG and 7–30% for PTCA. Regional rates varied 1·3-fold for CABG and threefold for PTCA in 1994/95, while district rates of CABG varied 3·6-fold and PTCA 18-fold. Revascularisation rates were higher in districts with least need in 1991/92 and this persisted over the following three years. The overall waiting time for CABG (214 days) was largely unchanged from 1992/93 (234 days). The overall waiting time for PTCA (138 days) was 25% shorter than in 1992/93 (185 days). Prioritisation of patients waiting over a year had not yet adversely affected the waiting time of more urgent patients. Commissioning has faced a complex web of interconnected problems which, in general, caused more problems for purchasers than providers initially but which appear to be of increasing concern to providers. Conclusions—The 1991 NHS reforms had had no observable impact on the availability and use of coronary revascularisation by 1995. Continued monitoring is necessary to detect any delayed effect.
Keywords: coronary revascularisation, trends, geographical variation, commissioning
Full text
PDF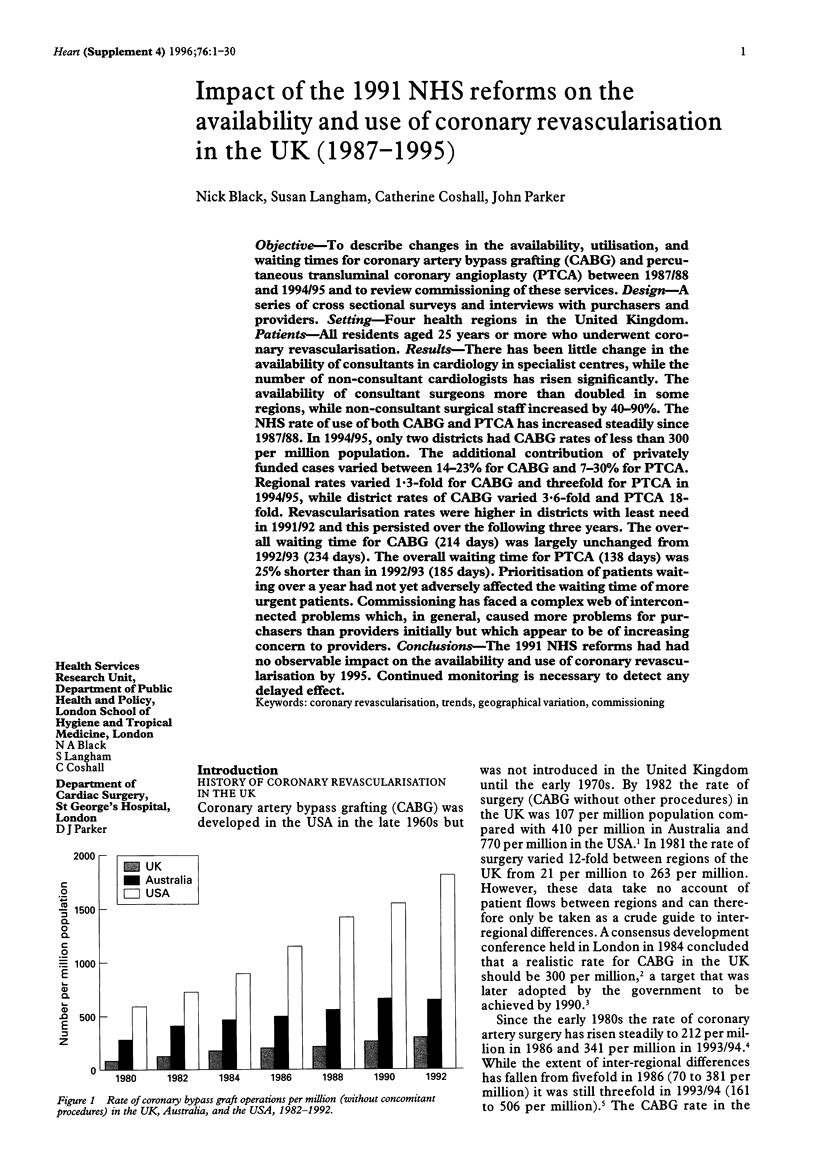



Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Black N., Langham S., Petticrew M. Coronary revascularisation: why do rates vary geographically in the UK? J Epidemiol Community Health. 1995 Aug;49(4):408–412. doi: 10.1136/jech.49.4.408. [DOI] [PMC free article] [PubMed] [Google Scholar]
- English T. A., Bailey A. R., Dark J. F., Williams W. G. The UK cardiac surgical register, 1977-82. Br Med J (Clin Res Ed) 1984 Nov 3;289(6453):1205–1208. doi: 10.1136/bmj.289.6453.1205. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hubner P. J. Cardiac interventional procedure in the United Kingdom during 1990. The British Cardiovascular Intervention Society. Br Heart J. 1992 Oct;68(4):434–436. doi: 10.1136/hrt.68.10.434. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hubner P. J. Cardiac interventional procedures in the United Kingdom in 1989. Br Heart J. 1991 Dec;66(6):469–471. doi: 10.1136/hrt.66.6.469. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McPherson K., Wennberg J. E., Hovind O. B., Clifford P. Small-area variations in the use of common surgical procedures: an international comparison of New England, England, and Norway. N Engl J Med. 1982 Nov 18;307(21):1310–1314. doi: 10.1056/NEJM198211183072104. [DOI] [PubMed] [Google Scholar]
- Wilson R., Allen P. Medical and dental staffing prospects in the NHS in England and Wales 1993. Health Trends. 1994;26(3):70–79. [PubMed] [Google Scholar]