

Abstract
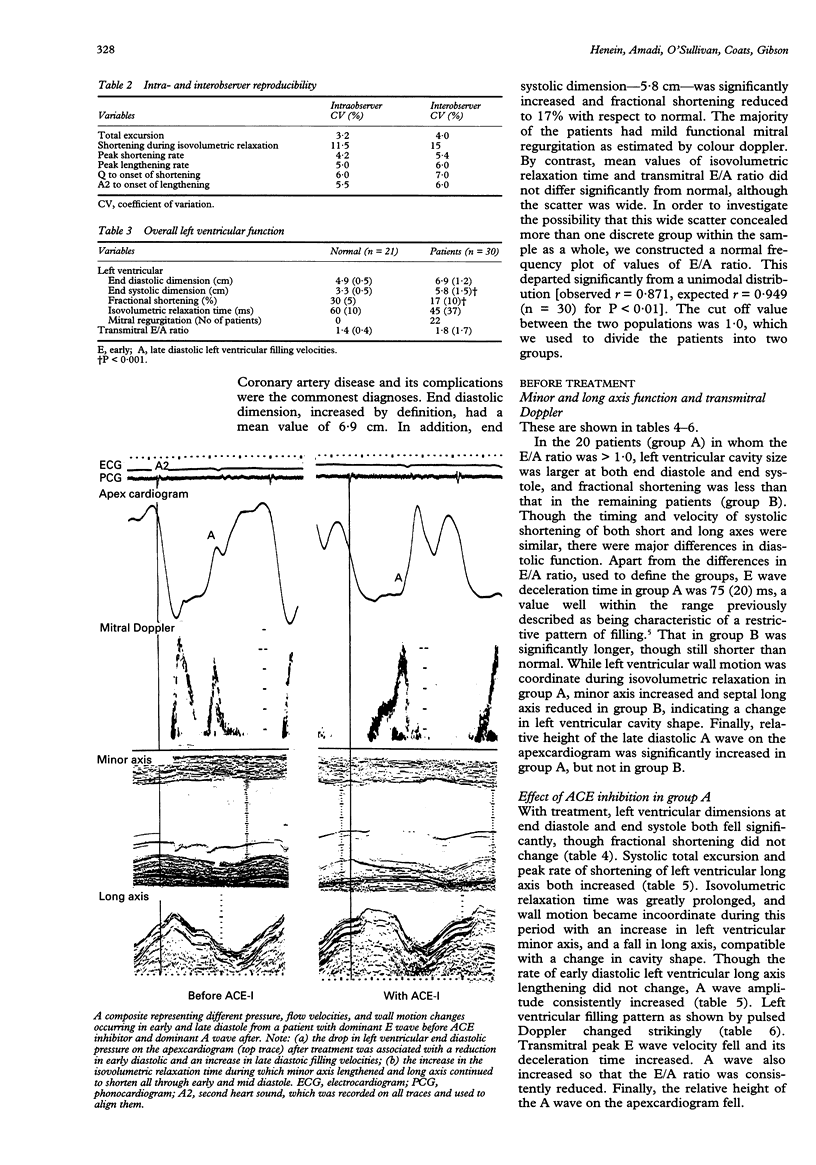
OBJECTIVE: To assess the effect of ACE-inhibition on left ventricular filling and wall motion in patients with a clinical diagnosis of heart failure. DESIGN: Prospective examination of left ventricular systolic and diastolic function using M mode echocardiography and pulsed and continuous wave Doppler before and three weeks after starting an ACE inhibitor. SETTING: A tertiary referral centre for cardiac disease equipped with non-invasive facilities. SUBJECTS: 30 outpatients with a clinical diagnosis of heart failure in whom treatment with an ACE inhibitor was started; age 61 (SD 11) years; 27 male; 3 female; 21 healthy controls of similar age. RESULTS: Left ventricular cavity was dilated both at end systole and end diastole, and fractional shortening reduced. Although mean isovolumetric relaxation time (IVRT) and transmitral E (early) to A (late) filling velocity (E/A) ratio were not different from normal, a value of 1.0 on the normal frequency plot of the E/A ratio divided the patients bimodally into two groups: 20 patients (group A) with E/A ratio > 1.0 and 10 patients (group B) < 1.0. In group A patients, IVRT was short as was transmitral E wave deceleration time compared to normal (P < 0.001), fulfilling the criteria of restrictive left ventricular physiology. Left ventricular wall motion during IVRT was coordinate and left ventricular end diastolic pressure was raised on the apex-cardiogram (P < 0.001). In group B, E wave deceleration time was longer, relaxation incoordinate, and apexcardiogram normal. With an ACE inhibitor: in group A, left ventricular dimensions fell at end diastole (P < 0.05) and end systole (P < 0.01) but fractional shortening did not change; long axis total excursion (P < 0.01) and peak rate of shortening (P < 0.05) both increased; IVRT increased (P < 0.001) with the appearance of markedly incoordinate wall motion, minor axis lengthening, and long axis shortening (P < 0.001 for both); A wave amplitude also consistently increased (P < 0.001); finally, transmitral E wave velocity fell and A wave velocity increased. ACE inhibition did not alter any of the left ventricular minor and long axis or transmitral Doppler variables in patients in group B. CONCLUSIONS: Patients with a clinical diagnosis of heart failure differ in their presentation and response to ACE inhibition according to baseline haemodynamics. In restrictive left ventricular physiology, ACE inhibition reduces cavity size and prolongs IVRT, compatible with a fall in left atrial pressure. At the same time, ventricular relaxation becomes very delayed and incoordinate, greatly reducing early diastolic left ventricular filling velocity. Thus ACE inhibition unmasks major diastolic abnormalities in patients with restrictive left ventricular disease.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Ader R., Chatterjee K., Ports T., Brundage B., Hiramatsu B., Parmley W. Immediate and sustained hemodynamic and clinical improvement in chronic heart failure by an oral angiotensin-converting enzyme inhibitor. Circulation. 1980 May;61(5):931–937. doi: 10.1161/01.cir.61.5.931. [DOI] [PubMed] [Google Scholar]
- Appleton C. P., Hatle L. K., Popp R. L. Demonstration of restrictive ventricular physiology by Doppler echocardiography. J Am Coll Cardiol. 1988 Apr;11(4):757–768. doi: 10.1016/0735-1097(88)90208-2. [DOI] [PubMed] [Google Scholar]
- Cleland J. G., Bulpitt C. J., Falk R. H., Findlay I. N., Oakley C. M., Murray G., Poole-Wilson P. A., Prentice C. R., Sutton G. C. Is aspirin safe for patients with heart failure? Br Heart J. 1995 Sep;74(3):215–219. doi: 10.1136/hrt.74.3.215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Denolin H., Kuhn H., Krayenbuehl H. P., Loogen F., Reale A. The definition of heart failure. Eur Heart J. 1983 Jul;4(7):445–448. doi: 10.1093/oxfordjournals.eurheartj.a061500. [DOI] [PubMed] [Google Scholar]
- Fitzpatrick D., Nicholls M. G., Ikram H., Espiner E. A. Haemodynamic, hormonal, and electrolyte effects of enalapril in heart failure. Br Heart J. 1983 Aug;50(2):163–169. doi: 10.1136/hrt.50.2.163. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Henein M. Y., Gibson D. G. Abnormal subendocardial function in restrictive left ventricular disease. Br Heart J. 1994 Sep;72(3):237–242. doi: 10.1136/hrt.72.3.237. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Henein M. Y., Gibson D. G. Suppression of left ventricular early diastolic filling by long axis asynchrony. Br Heart J. 1995 Feb;73(2):151–157. doi: 10.1136/hrt.73.2.151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jones C. J., Raposo L., Gibson D. G. Functional importance of the long axis dynamics of the human left ventricle. Br Heart J. 1990 Apr;63(4):215–220. doi: 10.1136/hrt.63.4.215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Levine T. B., Franciosa J. A., Cohn J. N. Acute and long-term response to an oral converting-enzyme inhibitor, captopril, in congestive heart failure. Circulation. 1980 Jul;62(1):35–41. doi: 10.1161/01.cir.62.1.35. [DOI] [PubMed] [Google Scholar]
- Ng K. S., Gibson D. G. Relation of filling pattern to diastolic function in severe left ventricular disease. Br Heart J. 1990 Apr;63(4):209–214. doi: 10.1136/hrt.63.4.209. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nishimura R. A., Abel M. D., Housmans P. R., Warnes C. A., Tajik A. J. Mitral flow velocity curves as a function of different loading conditions: evaluation by intraoperative transesophageal Doppler echocardiography. J Am Soc Echocardiogr. 1989 Mar-Apr;2(2):79–87. doi: 10.1016/s0894-7317(89)80068-9. [DOI] [PubMed] [Google Scholar]
- Shen W. F., Tribouilloy C., Rey J. L., Baudhuin J. J., Boey S., Dufossé H., Lesbre J. P. Prognostic significance of Doppler-derived left ventricular diastolic filling variables in dilated cardiomyopathy. Am Heart J. 1992 Dec;124(6):1524–1533. doi: 10.1016/0002-8703(92)90067-6. [DOI] [PubMed] [Google Scholar]
- Stoddard M. F., Pearson A. C., Kern M. J., Ratcliff J., Mrosek D. G., Labovitz A. J. Influence of alteration in preload on the pattern of left ventricular diastolic filling as assessed by Doppler echocardiography in humans. Circulation. 1989 Jun;79(6):1226–1236. doi: 10.1161/01.cir.79.6.1226. [DOI] [PubMed] [Google Scholar]