

Abstract
BACKGROUND:
Pulmonary rehabilitation (PR) programs proven to be one of the most effective treatment options for respiratory diseases; yet, they are not well-established in hospitals in Saudi Arabia.
AIM:
To determine the main barriers for setting up PR programs in Saudi Arabia.
METHODS:
A cross-sectional study was conducted in the Eastern Province of Saudi Arabia. Health care providers involved in treatment of chronic obstructive pulmonary disease (COPD) patients were recruited from 22 general government hospitals. Data were collected using questionnaires: Full version if they had heard about PR before the study, and a short version if they had not heard about PR before.
RESULTS:
A total of 123 health care providers were recruited (physicians [n = 44], nurses [n = 49], and respiratory therapists/technicians [n = 30]). Only 3.2% of the recruited health care providers had heard about PR programs before. According to the health care providers, the main barriers for setting up PR programs were a lack of (1) hospital capacity (75.6%), (2) trained health care providers (72.4%), and (3) funds (48.0%). There were significant differences in barriers reported by the health care providers. Compared to physicians, nurses were more likely to nominate the PR costs as a barrier (18.0% vs. 38.8%; P < 0.05).
CONCLUSION:
There is a worrisome lack of knowledge regarding content and benefits of PR programs among Saudi health care providers treating COPD patients. These findings imply that improving awareness and increasing education of the health care providers regarding PR will be required before PR can be more widely implemented as an integral treatment modality for patients with COPD in Saudi Arabia.
Keywords: Barriers, chronic obstructive, general, hospitals, pulmonary disease, rehabilitation, Saudi Arabia
Chronic obstructive pulmonary disease (COPD) is a leading cause of morbidity and mortality worldwide.[1] In 2012, more than 3 million people worldwide died of COPD, accounting for 6% of total deaths.[2] The global burden of disease study estimates that by 2020 COPD will become the third leading cause of death worldwide.[1]
In Saudi Arabia, the prevalence of COPD is 2.4% among the general population and 14.2% among smokers over 40 years of age.[3,4,5] These prevalence rates are comparable to rates in the Middle East countries (3.6% among the general population) and in Turkey (18.1% among smoking population).[3,5] In 2014, the fifth leading cause of death in Saudi Arabia was chest diseases.[6] Evidence shows that smoking is the main risk factor for the development and progression of COPD.[3] At present, the smoking rate in Saudi Arabia is estimated at 27.9%,[7] and there is evidence that the rate of smoking is steadily increasing among Saudis.[7] The prevalence of COPD is therefore expected to rise further in Saudi Arabia, not only because of exposure to smoking, but also outdoor air pollution, desert dust, wars (e.g., chemical weapons), childhood respiratory infections, and lack of physical activity.[8,9]
Studies have shown that patients with COPD tend to be physically inactive in daily life.[9] A relationship exists between decreasing level of physical activity and poor quality of life, increased health care utilization and reduced survival.[9] The prevalence of physical inactivity in Saudi Arabia is high.[10] This is illustrated by the fact that 96.1% of the Saudi males and 98.5% of the Saudi females do not meet the recommended physical activity levels compared to 64% of the males and 60% of the females in Australia.[10,11] This low level of physical activity of patients with COPD in Saudi Arabia is likely to contribute further to the mortality and health care burden associated with COPD in this country.[9]
Many studies and guidelines have recommended pulmonary rehabilitation (PR) programs as an integral and essential management option for respiratory diseases such as COPD.[1,12,13] PR is defined as “a comprehensive intervention based on a thorough patient assessment followed by patient-tailored therapies that include but are not limited to exercise training, education, and behavior change, designed to improve the physical and psychological condition of people with the chronic respiratory disease and to promote the long-term adherence to health-enhancing behaviors.”[12] High-level evidence shows that PR decreases dyspnea, anxiety levels, depression levels, and hospitalization rates and that it increases exercise capacity, physical activity, and quality of life.[12,14] Currently, there are no PR programs in hospitals in the Eastern Province of Saudi Arabia[15] and to the best of our knowledge, there is only one tertiary hospital (The King Abdulaziz Medical City in Riyadh, Central Province) that offers a program in Saudi Arabia.[16] Therefore, the number of patients with COPD that can access PR in Saudi Arabia is extremely low.[16] Implementation of more PR programs that meet international criteria throughout Saudi Arabia is therefore highly recommended.[13,16,17,18]
In this study, we explored the reasons why PR is not a part of usual COPD management in Saudi Arabia. Barriers for setting up PR programs were identified by health care professionals who treat and provide care for patients with COPD in Saudi Arabia. Moreover, we ascertained the opinions of these health care providers in relation to reasons that would prevent patients with COPD from participating in PR programs if they were to be offered.
Methods
A cross-sectional study was conducted from April to August 2013 in the Eastern Province of Saudi Arabia. Health care providers were selected from all 22 general government hospitals (Eastern area: n = 14, Al-Ahsa area: n = 5, and Hafar Al-Batin area: n = 3).[15] To be eligible, health care providers needed to (a) have access to evaluate, treat, and provide care for patients with COPD and (b) have experience with patients with COPD with a minimum of 10 cases/year.
The research protocol was approved by the Southern Adelaide Clinical Human Research Ethics Committee, Flinders Medical Centre Ethics Committee, Institutional Review Board at Ministry of Health (MOH) in Saudi Arabia, and Institutional Review Board at King Fahd Hospital University in Saudi Arabia. All participants signed an informed consent form.
The researcher (MA) first contacted the directors of the Departments of Internal Medicine Physiotherapy, Respiratory Care, Psychiatry, Nutrition, and Nursing in order to obtain permission to conduct interviews with the health care providers who had access to evaluate, treat, and provide care for patients with COPD.
All eligible health care providers were asked in a face to face interview “Have you heard of a pulmonary rehabilitation program?” Health care providers who answered “yes” were asked to complete a full version of our PR questionnaire in order to evaluate the barriers for setting up PR (see online repository). If the health care providers and the directors answered “no,” the researcher provided standardized information about PR in order to familiarize them with PR [Box 1] and they were asked to complete a short version of our PR questionnaire (online repository). Health care providers were asked to complete the questionnaires within a week.
Box 1.
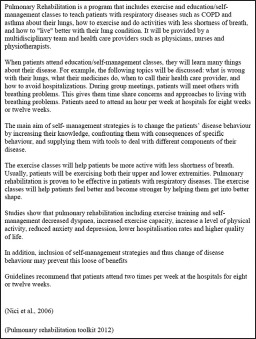
Information about pulmonary rehabilitation program
Questionnaires
The PR questionnaire was in the English language because this is the official language in Saudi hospitals. Barriers were predefined and based mostly on a systematic review[19] that described factors associated with uptake and completion of PR for people with COPD.
The full version of the questionnaire, provided to the health care providers who were familiar with PR, was divided into two parts. The first part (questions 1–4) evaluated their knowledge about PR programs. Another 13 questions were directed toward (1) the structure of the offered PR program, (2) perceived barriers for setting up a PR program, and (3) perceived preventers of participation in a PR program by COPD patients.
A short version of the PR questionnaire was provided to the health care providers who were not familiar with PR. It included standardized information about PR, four questions evaluating the perceived barriers associated with setting up a PR program and preventers of PR program participation by COPD patients.
After analyzing the questionnaires, we felt that health care providers could not distinguish between two barriers listed, namely “lack of hospital capacity” and “lack of hospital rooms.” These barriers were therefore retrospectively combined in one barrier “lack of hospital capacity.”
Statistical analysis
All data were entered into the Statistical Package for Social Sciences version 19 (IBM Corporation, Armonk, NY, USA). Analyses were mostly descriptive. Continuous variables were summarized by calculating the mean and the standard deviation. Nominal data were given as proportions.
Chi-square tests were performed to determine associations and significance between variables. Statistical significance was reported when P < 0.05.
Results
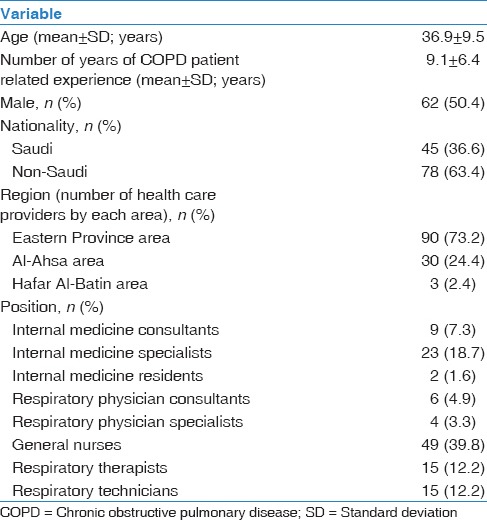
Of the 158 health care providers, 123 could be included (physicians n = 44 from 22 hospitals, nurses n = 49 from 8 hospitals, and respiratory therapists/technicians n = 30 from 3 hospitals). Six physicians, 15 nurses, and five respiratory therapists refused to participate because of lack of time. Six general physicians and three physiotherapists were excluded because they did not meet the study criteria [Figure 1]. Characteristics of the included health care providers are presented in Table 1. The majority of the health care providers were non-Saudis (n = 78; 63.4%).
Figure 1.
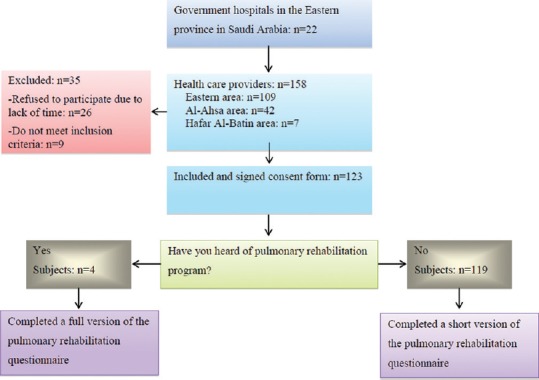
Flow diagram of health care provider's progress through the study
Table 1.
Characteristics of the health care providers (n=123)
Health care providers were categorized into three disciplines based on their specialties (physicians, nurses, and respiratory therapists/technicians). Table 2 presents the characteristics of each discipline. There is a significant difference between health care providers' disciplines in terms of number per region, age, gender, and years of experience. Physicians were enrolled from 21 hospitals, nurses were enrolled from eight hospitals, while respiratory therapists/technicians were enrolled from three hospitals. Only four participants (all physicians) had heard of PR and therefore completed a full version of the PR questionnaire, while 119 health care providers were not familiar with PR and completed the short version of PR questionnaire instead [Figure 1 and Table 2].
Table 2.
Characteristics of the health care providers’ disciplines (n=123)
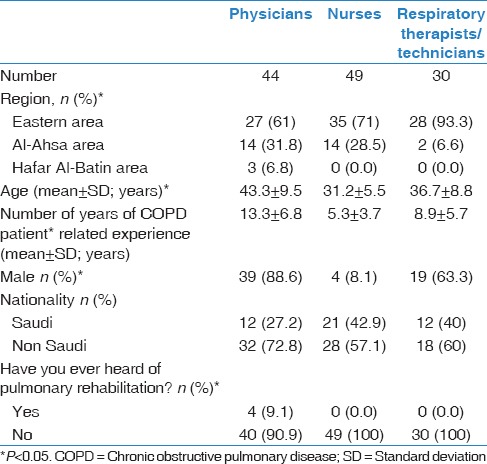
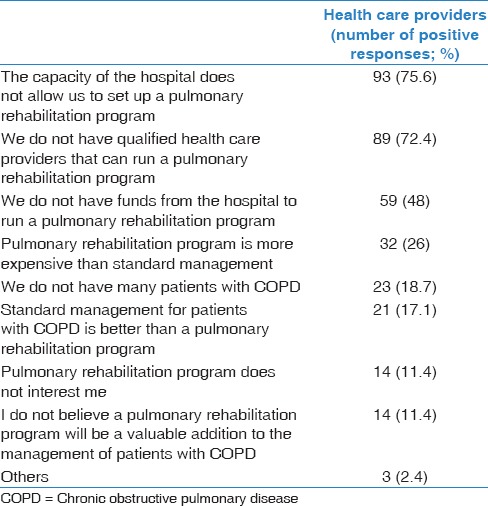
Table 3 shows the perceived barriers for setting up PR program in hospitals in the Eastern Province of Saudi Arabia according to the health care providers. The most reported barrier was “The capacity of the hospital does not allow us to set up a pulmonary rehabilitation program” (reported by 75.6% of health care providers). “We do not have qualified health care providers that can run a pulmonary rehabilitation program” was also reported frequently (72.4%), followed by “We do not have funds from the hospital to run a pulmonary rehabilitation program” (48%).
Table 3.
Barriers for setting up pulmonary rehabilitation program
Perceived barriers to setting up a PR program organized in accordance with the health care providers' disciplines are presented in Table 4. There were significant differences between the views of physicians, respiratory therapists/technicians, and nurses in terms of reporting barriers. For example, whereas almost all physicians (93%) saw the lack of trained health care providers as a barrier, well over half of the nurses (61%) and respiratory therapists/technicians (60%) considered this as a barrier. Most of the health care providers (91%) thought that patients with COPD would be willing to participate in a PR program if they were offered a place.
Table 4.
Barriers for setting up pulmonary rehabilitation program according to health care providers groups*
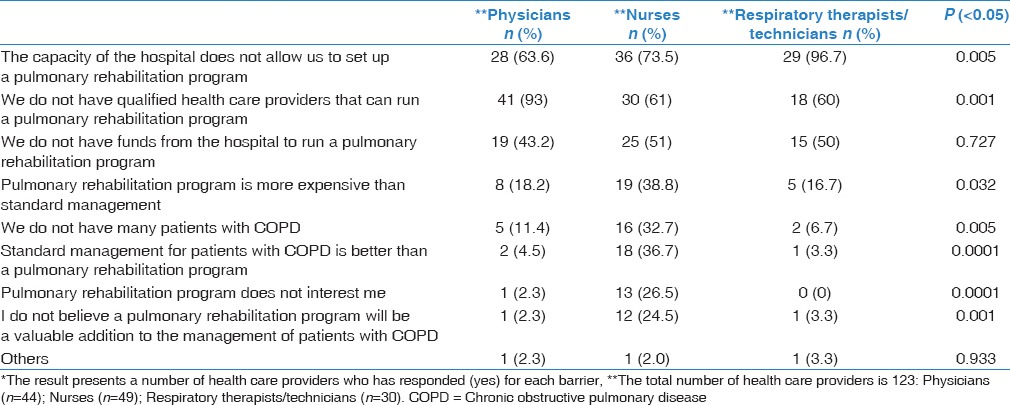
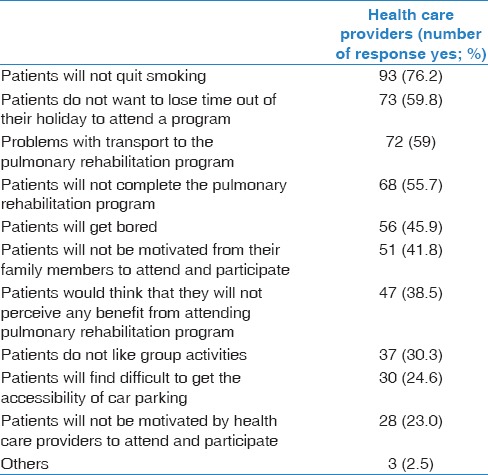
Table 5 displays health care providers' perceptions of barriers that may prevent patients with COPD from participating in a PR program. The main barriers reported by the health care providers included smoking status (76.2%), interruption to patient's routine (59.8%), lack of transportation (59%), patients will not complete the PR program (55.7%), patients will get bored (45.9%), lack of social/family support (41.8%), lack of perceived benefit (38.5%), and patients do not like group activities (30.3%).
Table 5.
Barriers that might prevent patients with chronic obstructive pulmonary disease from participating in a pulmonary rehabilitation program
Discussion
This study is the first to assess the barriers to setting up a PR program in Saudi Arabia.[15,17,20] The study results show that only a very small percentage of the Saudi health care providers know what PR is. Hospitals capacity, trained health care providers, and funds were seen by the health care providers as the main barriers to setting up a PR program. Reported barriers differed significantly between disciplines.
Lack of hospital capacity was reported as a barrier by more than half of the health care providers. However, PR can be provided within existing infrastructure and using incumbent health professionals in the hospitals.[21] Furthermore, it has been demonstrated that an outpatient PR program conducted in a small hospital was as effective as programs in a large hospital in COPD patients.[22] Studies have also suggested that PR can be effectively provided in an inpatient, community-based or home setting.[14,21,23,24,25,26] Hospitals in the Eastern Province of Saudi Arabia could therefore adopt any PR model that suits their resources.[14]
Lack of trained health care providers was defined as another major barrier for setting up a PR program. Studies show that Saudi Arabia, in general, suffers from a lack of health care providers, and limited disciplines are involved in COPD management in particular.[6,15,27] Moreover, the total number of chest physicians in Saudi Arabia is very low[6] and the number of specialized nurses (e.g., respiratory nurse practitioners) in Saudi Arabia is even lower.[6,15,28] This lack of health care providers may affect the quality of COPD care in Saudi Arabia.[15] The government could provide training incentives and facilitations encouraging upskilling of current health care providers and stimulating people to study medicine or health sciences and to specialize in respiratory diseases. The latter can be stimulated by offering high-quality education in Saudi universities or by sending students to overseas universities.
Similar to our data, lack of funds was also defined as an important barrier for setting up PR program and in keeping programs running in Australia.[29] Funding of health care services is a serious challenge for the MOH in Saudi Arabia because government-based health services are free for the population.[27] Whereas, spending more does not per definition mean a better quality of health care, the availability of funds is, however, one factor that influences the quality of health care systems.[30] It would be important to spite to the incorporation of PR as a core component of COPD care within any such funding system.
Our data show that barriers reported by health care providers differed significantly between disciplines. The fact that physicians had more years of experience in specifically managing COPD patients than nurses and respiratory therapists/technicians may have contributed to this difference. Another potential explanation is that all of the nurses participating in our study were general nurses and not specialized respiratory nurses.[15,28] It is therefore likely that nurses may have had limited knowledge about management of respiratory diseases. Increasing the nurse's level of education to the bachelor level is recommended in order to improve the quality of nursing care for patients in Saudi Arabia.[15,28,31,32] In addition, worryingly, between 10% and 20% of respondents considered PR would not be useful. This indicates that there is a need to improve the spread of understanding of the role and outcomes of PR among health care workers as well as administrators and government agencies in Saudi Arabia.
Previous studies in other countries and Saudi Arabia have reported that lack of knowledge and awareness of PR by primary care and specialist physicians were seen as one of the main barriers for setting up and referring to PR program.[15,29,33] Our data strongly support the view that there is a significant lack of knowledge by health care providers regarding PR programs and management of COPD in Saudi Arabia. This is exemplified by the fact that only four physicians in our sample had even heard of PR prior this study. In addition, only three disciplines were identified as being directly involved in COPD care in this study. This suggests that physicians may not be completely aware of optimal management of respiratory patients in general and the multidisciplinary approach in COPD management in particular. COPD guidelines recommend the involvement of other health care providers such as physiotherapists, mental health specialists (i.e., psychiatrist and psychologists), occupational therapists, respiratory nurses, and dieticians in COPD management.[1,13,21,34,35] Increasing awareness and improving information regarding PR is therefore recommended in order to implement PR programs and then to improve the referral rate,[15,33] which can be achieved by offering physicians and other health care providers short courses regarding PR program and management of COPD, seminars, education, and so forth.[15,33]
There is only one tertiary care center offering a PR program in the entire Saudi Arabia.[15,17,20] It is, however, possible that some private hospitals run PR programs, but they are often not well known by health care providers. It is very likely that barriers found in our study also apply to the rest of the Saudi Provinces because the Eastern Province is the largest and has a higher number of beds, funds, and health care providers.[6]
Instead of a cross-sectional design, we could also have chosen to use a structured interview method with health care providers to obtain more detailed data in this study. However, because of time constraints, the use of such a structured interview would most probably have led to the inclusion of fewer health care providers. Another study limitation was the limited participation of nurses in this study (only nurses from eight hospitals participated). Many nurses refused to participate due to a perceived lack of time. The small number of participating respiratory therapists/technicians (three hospitals) is not surprising because only five of the included government hospitals had employed respiratory therapists/technicians involved in COPD care.[15] Another limitation is that barriers that may prevent patients with COPD from participating in a PR program were obtained from health care providers and not the patients themselves, and we cannot be sure that these are the actual barriers. Our data are however in line with barriers mentioned in other studies that have assessed barrier for PR in patients with COPD.[19,36] Finally, barriers reported in this study may have been different if the health care providers had more knowledge regarding PR (and experience with PR) at the start of the study.
Conclusion and Recommendation
PR is highly efficacious in improving health status, activity levels, and health care utilizations for people with COPD. Knowledge regarding PR, however, is very limited among health care providers who are involved in COPD care in Saudi Arabia. Several barriers were identified by health care providers. These barriers should be further explored and if necessary targeted in the near future to increase awareness and knowledge regarding PR by health care providers as a crucial first step to facilitate implementation of PR programs in Saudi hospitals.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
We gratefully acknowledge the Ministry of Education in Saudi Arabia, the Saudi Arabian Cultural Mission in Australia, University of Dammam, and of course all participants who were involved in our study.
References
- 1.Vestbo J, Hurd SS, Agustí AG, Jones PW, Vogelmeier C, Anzueto A, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2013;187:347–65. doi: 10.1164/rccm.201204-0596PP. [DOI] [PubMed] [Google Scholar]
- 2.Chronic obstructive pulmonary disease (COPD): World Health Organization. 2015. [Last updated 2015 Jan 01; cited 2015 Jul 01]. Available from: http://www.who.int/mediacentre/factsheets/fs315/en/
- 3.Al Ghobain M. The prevalence of chronic obstructive pulmonary disease in Saudi Arabia: Where do we stand? Ann Thorac Med. 2011;6:185–6. doi: 10.4103/1817-1737.84770. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Al Ghobain M, Al-Hajjaj MS, Wali SO. Prevalence of chronic obstructive pulmonary disease among smokers attending primary healthcare clinics in Saudi Arabia. Ann Saudi Med. 2011;31:129–33. doi: 10.4103/0256-4947.77485. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Tageldin MA, Nafti S, Khan JA, Nejjari C, Beji M, Mahboub B, et al. Distribution of COPD-related symptoms in the Middle East and North Africa: Results of the BREATHE study. Respir Med. 2012;106 Suppl 2:S25–32. doi: 10.1016/S0954-6111(12)70012-4. [DOI] [PubMed] [Google Scholar]
- 6.Kingdom of Saudi Arabia: Ministry of Health; 2014. [Last accessed on 2015 Nov 21]. Statistics Year Book. Ministry of Health Portal. Available from: http://www.moh.gov.sa/Ministry/Statistics/Book/Pages/default.aspx . [Google Scholar]
- 7.Khattab A, Javaid A, Iraqi G, Alzaabi A, Ben Kheder A, Koniski ML, et al. Smoking habits in the Middle East and North Africa: Results of the BREATHE study. Respir Med. 2012;106(Suppl 2):S16–24. doi: 10.1016/S0954-6111(12)70011-2. [DOI] [PubMed] [Google Scholar]
- 8.Waness A, El-Sameed YA, Mahboub B, Noshi M, Al-Jahdali H, Vats M, et al. Respiratory disorders in the middle east: A review. Respirology. 2011;16:755–66. doi: 10.1111/j.1440-1843.2011.01988.x. [DOI] [PubMed] [Google Scholar]
- 9.Cindy Ng LW, Mackney J, Jenkins S, Hill K. Does exercise training change physical activity in people with COPD? A systematic review and meta-analysis. Chron Respir Dis. 2012;9:17–26. doi: 10.1177/1479972311430335. [DOI] [PubMed] [Google Scholar]
- 10.Al-Nozha MM, Al-Hazzaa HM, Arafah MR, Al-Khadra A, Al-Mazrou YY, Al-Maatouq MA, et al. Prevalence of physical activity and inactivity among Saudis aged 30-70 years. A population-based cross-sectional study. Saudi Med J. 2007;28:559–68. [PubMed] [Google Scholar]
- 11.Physical Activity in Australia: A Snapshot, 2007-08 Australian Bureau of Statistics website Australian Bureau of Statistics. 2012. [Last updated 2011 Sep 09; cited 2012 Jul 24]. Available from: http://www.abs.gov.au/ausstats/abs@.nsf/Lookup/4835.0.55.001main+features32007-08 .
- 12.Spruit MA, Singh SJ, Garvey C, ZuWallack R, Nici L, Rochester C, et al. An official American Thoracic Society/European Respiratory Society statement: Key concepts and advances in pulmonary rehabilitation. Am J Respir Crit Care Med. 2013;188:e13–64. doi: 10.1164/rccm.201309-1634ST. [DOI] [PubMed] [Google Scholar]
- 13.Khan JH, Lababidi HM, Al-Moamary MS, Zeitouni MO, Al-Jahdali HH, Al-Amoudi OS, et al. The saudi guidelines for the diagnosis and management of COPD. Ann Thorac Med. 2014;9:55–76. doi: 10.4103/1817-1737.128843. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.McCarthy B, Casey D, Devane D, Murphy K, Murphy E, Lacasse Y. Pulmonary rehabilitation for chronic obstructive pulmonary disease. Cochrane Libr. 2015;2:CD003793. doi: 10.1002/14651858.CD003793.pub3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Alsubaiei ME, Cafarella PA, Frith PA, McEvoy RD, Effing TW. Current care services provided for patients with COPD in the Eastern Province in Saudi Arabia: A descriptive study. Int J Chron Obstruct Pulmon Dis. 2015;10:2379–91. doi: 10.2147/COPD.S89456. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Al Moamary MS. Health care utilization among chronic obstructive pulmonary disease patients and the effect of pulmonary rehabilitation. Med Princ Pract. 2010;19:373–8. doi: 10.1159/000316376. [DOI] [PubMed] [Google Scholar]
- 17.Al-Moamary MS. Experience with pulmonary rehabilitation program in a tertiary care center in Saudi Arabia. Saudi Med J. 2008;29:271–6. [PubMed] [Google Scholar]
- 18.Al Moamary MS. Impact of a pulmonary rehabilitation programme on respiratory parameters and health care utilization in patients with chronic lung diseases other than COPD. East Mediterr Health J. 2012;18:120–6. doi: 10.26719/2012.18.2.120. [DOI] [PubMed] [Google Scholar]
- 19.Keating A, Lee A, Holland AE. What prevents people with chronic obstructive pulmonary disease from attending pulmonary rehabilitation? A systematic review. Chron Respir Dis. 2011;8:89–99. doi: 10.1177/1479972310393756. [DOI] [PubMed] [Google Scholar]
- 20.Al Moamary MS, Alorainy H, Al-Hajjaj MS. Pulmonary rehabilitation: A regional perspective evidenced-based review. Ann Thorac Med. 2014;9:3–7. doi: 10.4103/1817-1737.124408. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Jenkins S, Hill K, Cecins NM. State of the art: How to set up a pulmonary rehabilitation program. Respirology. 2010;15:1157–73. doi: 10.1111/j.1440-1843.2010.01849.x. [DOI] [PubMed] [Google Scholar]
- 22.Ward JA, Akers G, Ward DG, Pinnuck M, Williams S, Trott J, et al. Feasibility and effectiveness of a pulmonary rehabilitation programme in a community hospital setting. Br J Gen Pract. 2002;52:539–42. [PMC free article] [PubMed] [Google Scholar]
- 23.Hernández MT, Rubio TM, Ruiz FO, Riera HS, Gil RS, Gómez JC. Results of a home-based training program for patients with COPD. Chest. 2000;118:106–14. doi: 10.1378/chest.118.1.106. [DOI] [PubMed] [Google Scholar]
- 24.Maltais F, Bourbeau J, Shapiro S, Lacasse Y, Perrault H, Baltzan M, et al. Effects of home-based pulmonary rehabilitation in patients with chronic obstructive pulmonary disease: A randomized trial. Ann Intern Med. 2008;149:869–78. doi: 10.7326/0003-4819-149-12-200812160-00006. [DOI] [PubMed] [Google Scholar]
- 25.van Wetering CR, Hoogendoorn M, Mol SJ, Rutten-van Mölken MP, Schols AM. Short- and long-term efficacy of a community-based COPD management programme in less advanced COPD: A randomised controlled trial. Thorax. 2010;65:7–13. doi: 10.1136/thx.2009.118620. [DOI] [PubMed] [Google Scholar]
- 26.Goldstein RS, Gort EH, Stubbing D, Avendano MA, Guyatt GH. Randomised controlled trial of respiratory rehabilitation. Lancet. 1994;344:1394–7. doi: 10.1016/s0140-6736(94)90568-1. [DOI] [PubMed] [Google Scholar]
- 27.Almalki M, Fitzgerald G, Clark M. Health care system in Saudi Arabia: An overview. East Mediterr Health J. 2011;17:784–93. doi: 10.26719/2011.17.10.784. [DOI] [PubMed] [Google Scholar]
- 28.Almalki M, FitzGerald G, Clark M. The nursing profession in Saudi Arabia: An overview. Int Nurs Rev. 2011;58:304–11. doi: 10.1111/j.1466-7657.2011.00890.x. [DOI] [PubMed] [Google Scholar]
- 29.Pulmonary Rehabilitation Survey. Report. The Australian Lung Foundation website Stollznow Research, 2007 July, 2007. Report No.: 71 109 407 141 [Google Scholar]
- 30.Akala FA, El-Saharty S. Public-health challenges in the Middle East and North Africa. The Lancet. 2006;367:961–4. doi: 10.1016/S0140-6736(06)68402-X. [DOI] [PubMed] [Google Scholar]
- 31.Al Thagafi H. Change of Attitudes Towards the Nursing Profession for a Sample of Saudi Youth Through a Counselling Program: Experimental Study on a Sample of Students. Naif Arab University for Security Sciences. 2006 [Google Scholar]
- 32.Al-Freihi H, editor. A Meeting with the Secretary-general of the Saudi Commission for Health Specialties. Health Forum. 2009 [Google Scholar]
- 33.Johnston KN, Young M, Grimmer KA, Antic R, Frith PA. Barriers to, and facilitators for, referral to pulmonary rehabilitation in COPD patients from the perspective of Australian general practitioners: A qualitative study. Prim Care Respir J. 2013;22:319–24. doi: 10.4104/pcrj.2013.00062. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Abramson M, Crockett A, Frith P. The COPD-X plan: Australian and New Zealand guidelines for the management of chronic obstructive pulmonary disease. Med J Aust. 2003;178:1. doi: 10.5694/j.1326-5377.2003.tb05213.x. [DOI] [PubMed] [Google Scholar]
- 35.Nici L, Donner C, Wouters E, Zuwallack R, Ambrosino N, Bourbeau J, et al. American Thoracic Society/European Respiratory Society statement on pulmonary rehabilitation. Am J Respir Crit Care Med. 2006;173:1390–413. doi: 10.1164/rccm.200508-1211ST. [DOI] [PubMed] [Google Scholar]
- 36.Hayton C, Clark A, Olive S, Browne P, Galey P, Knights E, et al. Barriers to pulmonary rehabilitation: Characteristics that predict patient attendance and adherence. Respir Med. 2013;107:401–7. doi: 10.1016/j.rmed.2012.11.016. [DOI] [PubMed] [Google Scholar]