

Abstract
Candida osteoarticular infections are being reported with increasing frequency, possibly due to an expanding population at risk. However, Candida costochondritis is uncommon. We report two cases of Candida costochondritis in patients who presented with subacute-onset chest wall swelling and whose only identifiable risk factor was a history of recent intravenous drug use.
Keywords: Candida costochondritis, Invasive candidiasis, Intravenous drug use
Introduction
Candida species commonly colonize the gut and skin of humans but are also capable of causing significant infections in susceptible hosts [1]. Osteoarticular infection is a serious and increasingly reported form of invasive candidiasis [2], [3]. However, Candida costochondritis, once commonly described in injecting drug users with disseminated candidiasis, has rarely been reported in the last two decades. Two cases of Candida costochondritis in patients who had recently injected heroin are reported herein and serve as a reminder that this remains a clinically relevant infection.
Case reports
Patient 1
A 35-year-old male presented with a one-month history of painful chest wall swelling, subjective fever, anorexia and unintended weight loss. He had a history intravenous drug use (IVDU), last injecting heroin 2 months earlier. On examination, there was a firm, smooth 5 cm × 10 cm swelling over the right lower ribs anteriorly. The lesion was tender to palpation and fixed to underlying structures; overlying skin was indurated and mildly erythematous. A firm, tender lymph node was palpable in the right axilla. Laboratory findings included normocytic anemia (hemoglobin 11.7 g/dL; normal range 13.0–18.0 g/dL), mildly elevated C-reactive protein (CRP) concentration (27 mg/L; normal range <5 mg/L) and erythrocyte sedimentation rate (ESR) (32 mm/h; normal range 0–14 mm/h). Hepatitis C virus antibody was positive; human immunodeficiency virus antigen/antibody test was negative. There was no growth from three sets of blood cultures. Chest computed tomography (CT) demonstrated a soft tissue mass arising from the right seventh costochondral junction with erosion of the costal cartilage and communication with a 5.0 cm × 1.3 cm fluid collection superficial to the liver (Fig. 1).
Fig. 1.
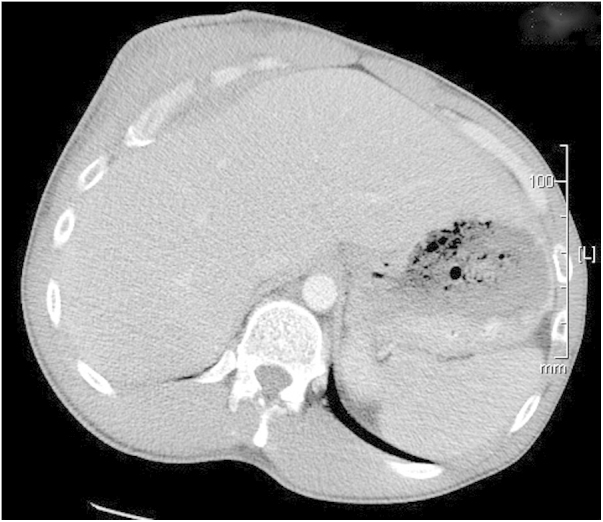
Chest computed tomography of Patient 1, showing a soft tissue mass arising from the right seventh costochondral junction with erosion of the costal cartilage and communication with an extra-capsular perihepatic fluid collection.
While awaiting percutaneous biopsy, the mass became fluctuant and discharged thick purulent material. An aspirate, immediately obtained for microscopy and culture, demonstrated pus cells and scanty growth of Candida albicans. Surgical debridement was performed and C. albicans was cultured from intra-operative specimens; susceptibility of the isolate to fluconazole was assumed due to very low rates of fluconazole resistance among C. albicans isolates in our region. Histopathological examination of the specimen demonstrated suppurative, noncaseating, granulomatous inflammation with no organisms seen on routine or special stains. The patient commenced fluconazole 400 mg orally daily for Candida costochondritis. Within three months, the chest wall swelling had resolved and he had gained weight. Antifungal therapy was ceased after 6 months and the patient has remained asymptomatic in follow up for over 6 months.
Patient 2
A 49-year-old female presented with a two-month history of two painful chest wall swellings, lethargy and anorexia. There was no documented fever or weight loss. Her medical history was notable for IVDU and hepatitis C virus infection with spontaneous clearance. She last injected heroin 4 months earlier. On examination, she exhibited firm, tender chest wall swellings over the left lower parasternal region and the right eighth rib anteriorly. Overlying skin was indurated but not erythematous. There was no palpable lymphadenopathy. Serum CRP concentration and ESR were elevated at 28.5 mg/L and 32 mm/h respectively. Chest CT demonstrated two heterogeneous masses, one over the left seventh costal cartilage, adjacent to the xiphisternum, measuring 3.5 cm in greatest diameter and one arising from the right eighth costochondral junction measuring 4.5 cm; there was cartilaginous erosion associated with the latter.
Percutaneous biopsy of the right-sided lesion was performed and culture of the specimen produced scanty growth of C. albicans. There was no growth from blood cultures and no features of infective endocarditis on transthoracic echocardiography. The patient commenced fluconazole 400 mg orally daily. Due to limited response after 1 month, surgical resection of both chest wall lesions was performed. Histopathological examination of the surgical specimens demonstrated a mixed inflammatory infiltrate but no granulomas. The specimens were received in formalin and could not be cultured. Surgical resection was followed by rapid resolution of symptoms. The patient completed 6 months of fluconazole without incident and remains well over 6 months after ceasing therapy.
Discussion
Candida osteoarticular infection is a serious form of invasive candidiasis associated with significant morbidity. Most infections arise from hematogenous seeding during candidemia, with the remainder due to direct inoculation or contiguous spread following trauma or surgery [1], [2], [3]. Reports of Candida osteoarticular infection may reflect rising prevalence of risk factors associated with candidemia: two recent literature reviews reported high rates of major surgery, broad-spectrum antimicrobial use, immunosuppression, central venous access devices, parenteral nutrition, and IVDU among patients with Candida osteomyelitis [2], [3].
The earliest reported cases of Candida costochondritis occurred following thoracic surgery [4], with the first IVDU-associated report published in 1981.[5] Collignon subsequently described a distinctive syndrome of eye lesions, skin lesions, osteomyelitis, and costochondritis due to C. albicans in patients who had recently injected heroin [6]; later studies implicated Candida-contaminated lemon juice used to dissolve brown heroin (a base that is poorly water-soluble) [7]. Outbreaks of invasive candidiasis among injecting drug users in Europe in the 1980s were notable for high rates of costochondritis [8], but there have been few reports of Candida costochondritis since, possibly reflecting changes in drug availability and injecting practices.
The clinical and diagnostic features of Candida costochondritis have been described only in small series [8], [9], [10]. Patients present with insidious onset of a mildly painful chest wall swelling. The mass is usually firm, but longstanding lesions may become fluctuant or discharge. Constitutional symptoms are variable but fever >38 °C is rarely recorded. Candida infection at other sites is common, necessitating thorough physical assessment; skin, eyes, bones and joints are the most frequently affected sites. Markers of inflammation such as leukocyte count, CRP concentration and ESR are usually modestly elevated. Multiple blood cultures should be performed to exclude candidemia, but Candida is infrequently cultured from the blood at the time of diagnosis. The role of echocardiography is uncertain unless candidemia is proven. CT of the chest with intravenous contrast may show a mass arising from the costochondral junction, erosion of the adjacent cartilage or rib, invasion of the surrounding soft tissues or formation of a sinus. Imaging also helps differentiate infection from other causes of chest wall swelling such as tumors. Percutaneous or open biopsy is the diagnostic test of choice with specimens submitted for histopathology as well as routine bacterial, fungal and mycobacterial stains and cultures. Histopathological examination of biopsied tissue may demonstrate mixed inflammatory cell infiltrate, noncaseating granulomas and fungal elements. C. albicans is the species most commonly identified in culture [8], [9], [10].
Prolonged antifungal therapy is the mainstay of treatment for Candida costochondritis. The choice of agent, route of administration and duration are determined by antimicrobial sensitivity, the severity of infection and potential toxicity. Adjunctive surgical debridement or resection is frequently required to achieve cure [11].
Candida costochondritis, once a commonly reported manifestation of disseminated candidiasis in intravenous drug users, has rarely been reported in the last 20 years. We report two cases of Candida costochondritis that highlight the typical presentation of this infection and serve as a reminder of its ongoing clinical relevance. The presumed mechanism of infection in our patients was hematogenous seeding following self-injection of Candida-contaminated narcotics. For reasons that are unclear, injecting drug users seem to be at increased risk of developing costochondritis following candidemia and clinicians should be aware of this as a potential presentation. Surgical debridement and prolonged antifungal therapy leads to favorable outcomes.
Conflict of interest
The authors have no conflicts of interest to declare in relation to this manuscript.
Ethical approval
Written informed consent was obtained from the patients for publication of these case reports and the accompanying image. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Acknowledgements
The authors would like to acknowledge the Illawarra Shoalhaven Local Health District Research Unit for financial assistance in publishing this article.
References
- 1.Kullberg B.J., Arendrup M.C. Invasive candidiasis. N Engl J Med. 2015;373:1445–1456. doi: 10.1056/NEJMra1315399. [DOI] [PubMed] [Google Scholar]
- 2.Slenker A.K., Keith S.W., Horn D.L. Two hundred and eleven cases of Candida osteomyelitis: 17 case reports and a review of the literature. Diagn Microbiol Infect Dis. 2012;73:89–93. doi: 10.1016/j.diagmicrobio.2012.02.004. [DOI] [PubMed] [Google Scholar]
- 3.Gamaletsou M.N., Kontoyiannis D.P., Sipsas N.V., Moriyama B., Alexander E., Roilides E. Candida osteomyelitis: analysis of 207 pediatric and adult cases (1970–2011) Clin Infect Dis. 2012;55:1338–1351. doi: 10.1093/cid/cis660. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Williams C.D., Cunningham J.N., Falk E.A., Isom O.W., Chase R.N., Spencer F.C. Chronic infection of the costal cartilages after thoracic surgical procedures. J Thorac Cardiovasc Surg. 1973;66:592–598. [PubMed] [Google Scholar]
- 5.Yap S., Ravitch M.M., Pataki K.I. En bloc chest wall resection for candidal costochondritis in a drug addict. Ann Thorac Surg. 1981;31:182–187. doi: 10.1016/s0003-4975(10)61540-8. [DOI] [PubMed] [Google Scholar]
- 6.Collignon P.J., Sorrell T.C. Disseminated candidiasis: evidence of a distinctive syndrome in heroin abusers. Br Med J. 1983;287:861–862. doi: 10.1136/bmj.287.6396.861. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Newton-John H.F., Wise K., Looke D.F. Role of the lemon in disseminated candidiasis of heroin abusers. Med J Aust. 1984;140:780–781. doi: 10.5694/j.1326-5377.1984.tb132597.x. [DOI] [PubMed] [Google Scholar]
- 8.Miro J.M., Brancos M.A., Abello R., Lomena F., Bisbe J., Ribalta T. Costochondral involvement in systemic candidiasis in heroin addicts: clinical, scintigraphic, and histologic features in 26 patients. Arthritis Rheum. 1988;31:793–797. doi: 10.1002/art.1780310616. [DOI] [PubMed] [Google Scholar]
- 9.Zapatero J., Lopez Longo J., Monteagudo I., Carreno L. Costal chondritis in heroin addicts: a comparative study with postsurgical chondritis. Br J Dis Chest. 1988;82:341–346. doi: 10.1016/0007-0971(88)90086-1. [DOI] [PubMed] [Google Scholar]
- 10.Gimferrer J.M., Callejas M.A., Sanchez-Lloret J., Carranza M., Catalan M., Freixinet J. Candida albicans costochondritis in heroin addicts. Ann Thorac Surg. 1986;41:89–90. doi: 10.1016/s0003-4975(10)64503-1. [DOI] [PubMed] [Google Scholar]
- 11.Pappas P.G., Kauffman C.A., Andes D., Benjamin D.K., Calandra T.F., Edwards J.E. Clinical practice guidelines for the management of candidiasis: 2009 update by the Infectious Diseases Society of America. Clin Infect Dis. 2009;48:503–535. doi: 10.1086/596757. [DOI] [PMC free article] [PubMed] [Google Scholar]