

Abstract
Attacks of Prinzmetal's variant form of angina pectoris are spontaneous, recur cyclically, and present unequivocal electrocardiographic alterations: they are ideal for a detailed haemodynamic study.
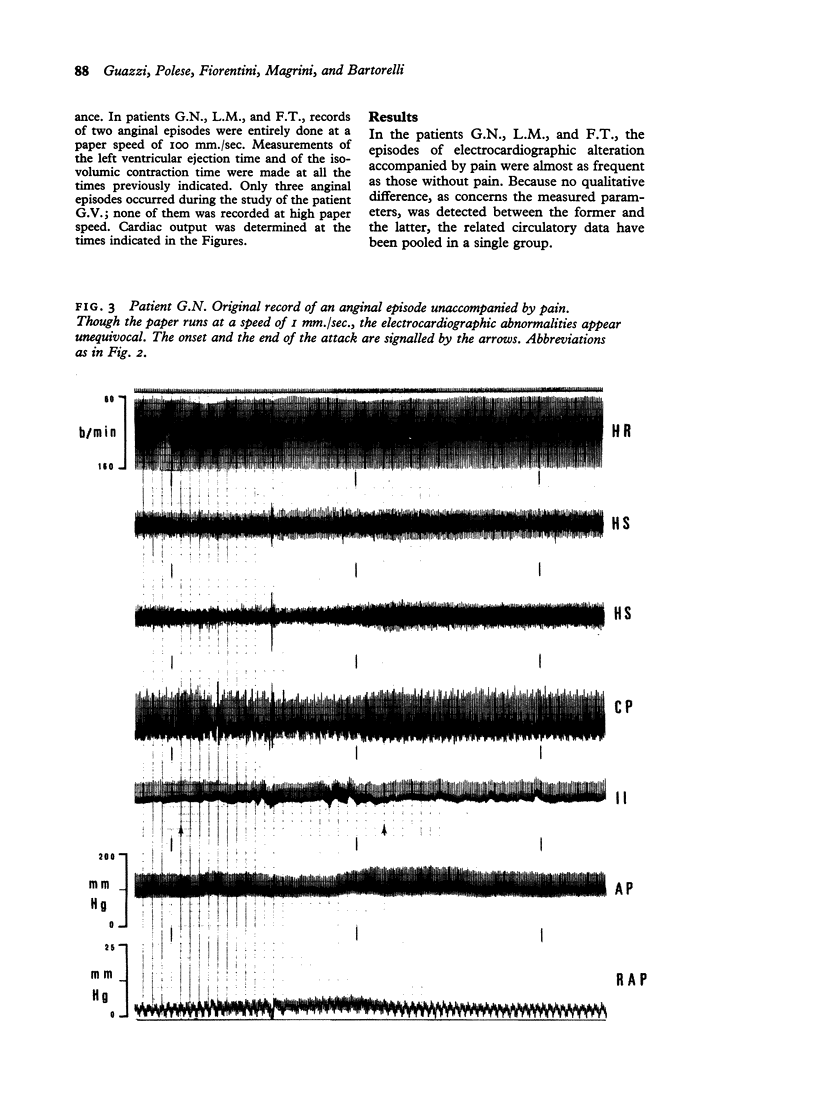
Four patients with this form of angina were investigated. In each of them episodes occurred of electrocardiographic abnormalities either accompanied or unaccompanied by pain. During the same session, the cardiogram, heart rate, arterial pressure, and right atrial pressure were continuously recorded during periods ranging from 5 to 7 hours in each patient. Cardiac output was measured at selected times. Left ventricular ejection time, isovolumic contraction time, mean rate of isovolumic pressure development, and mean systolic ejection rate were also determined.
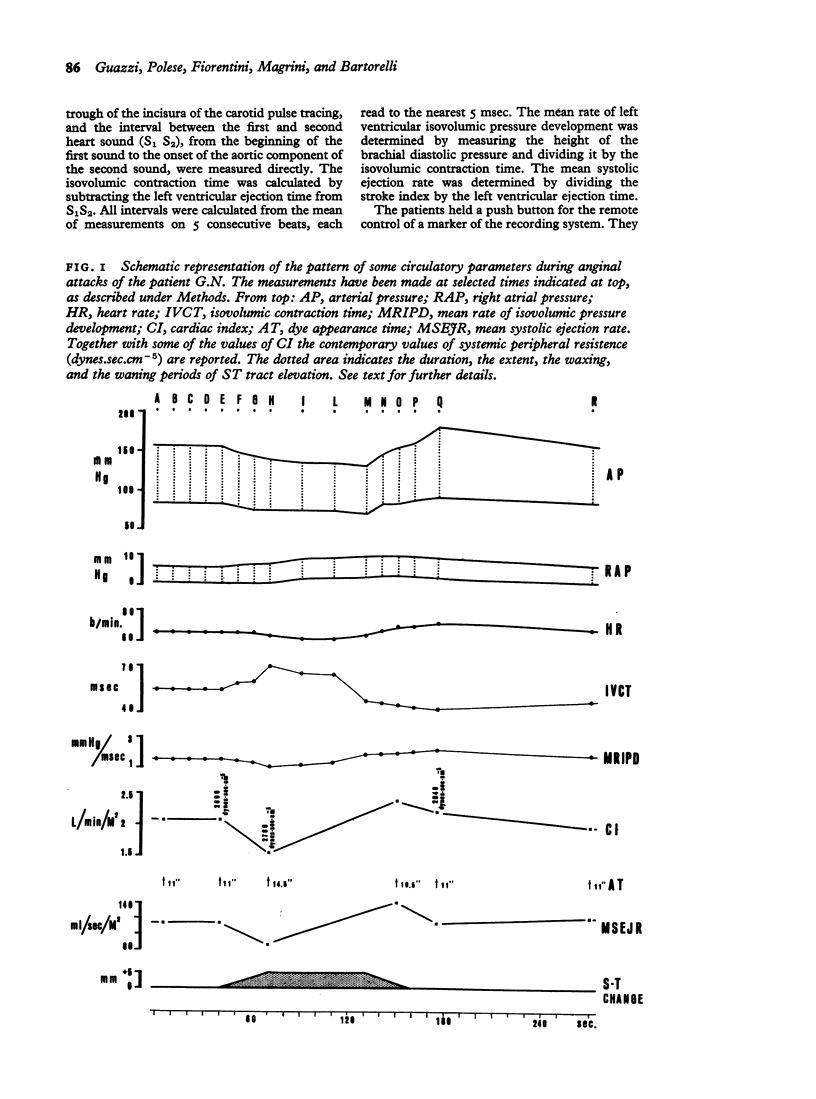
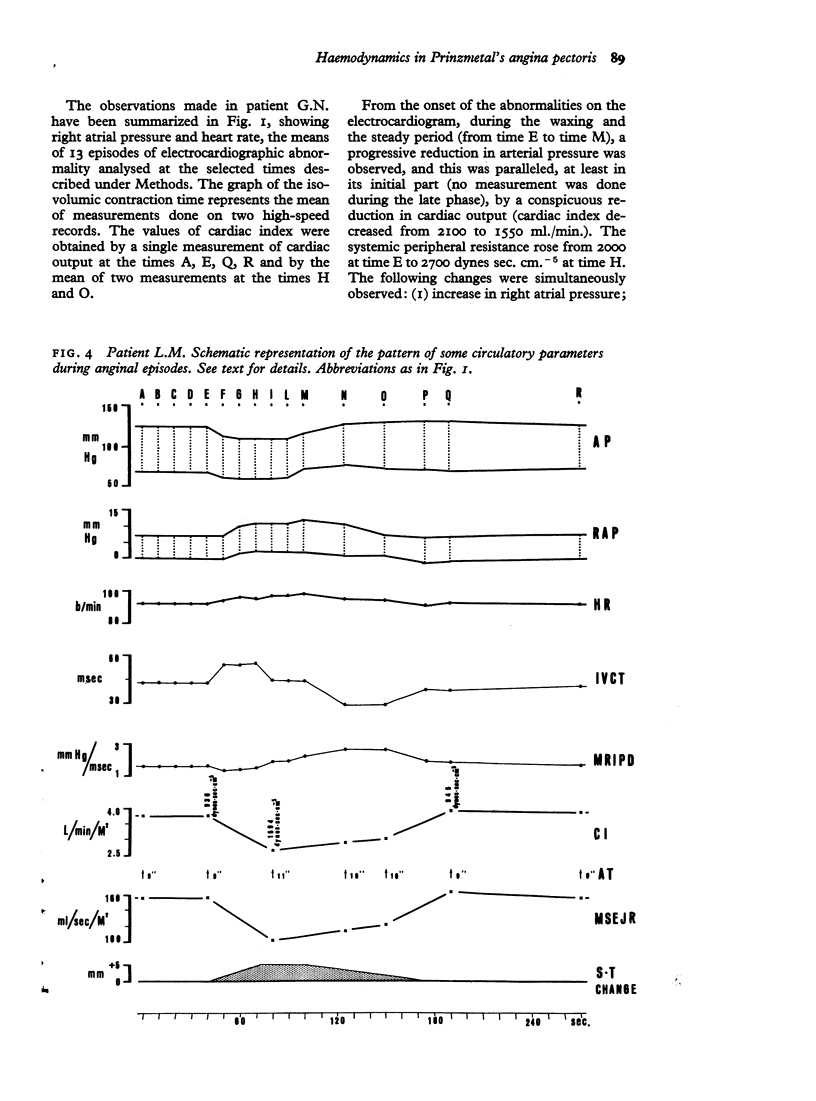
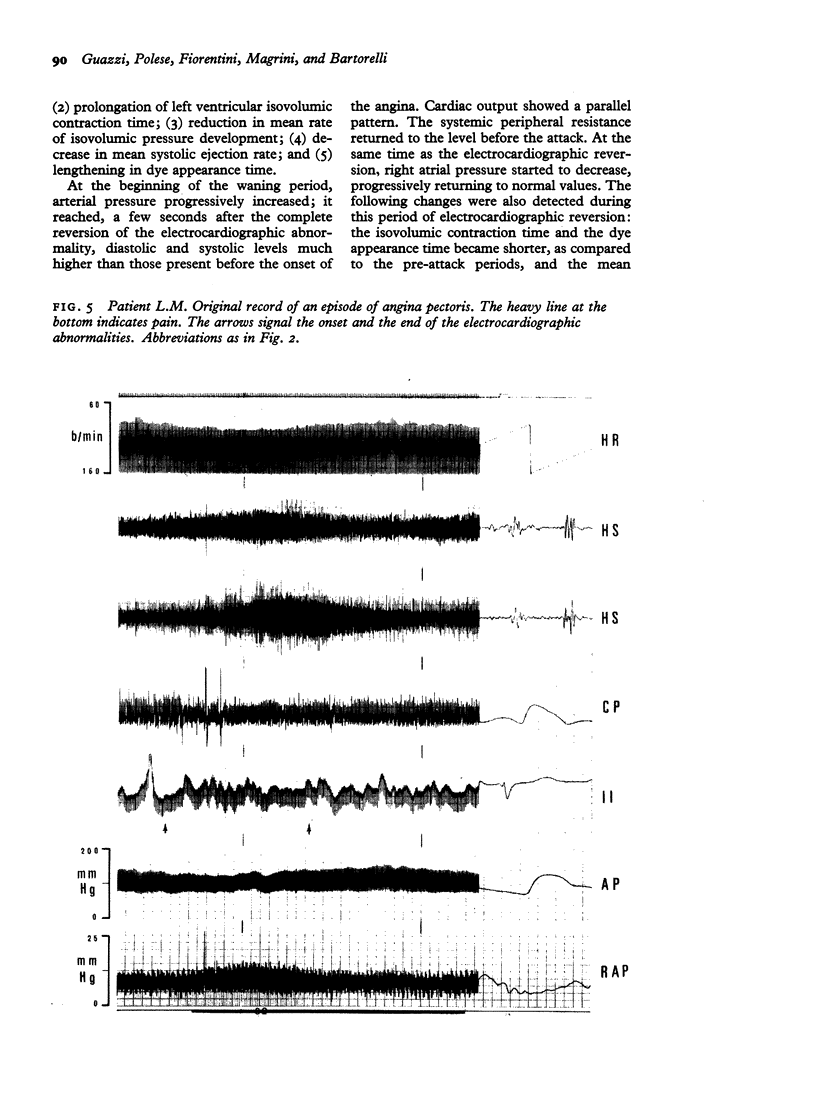
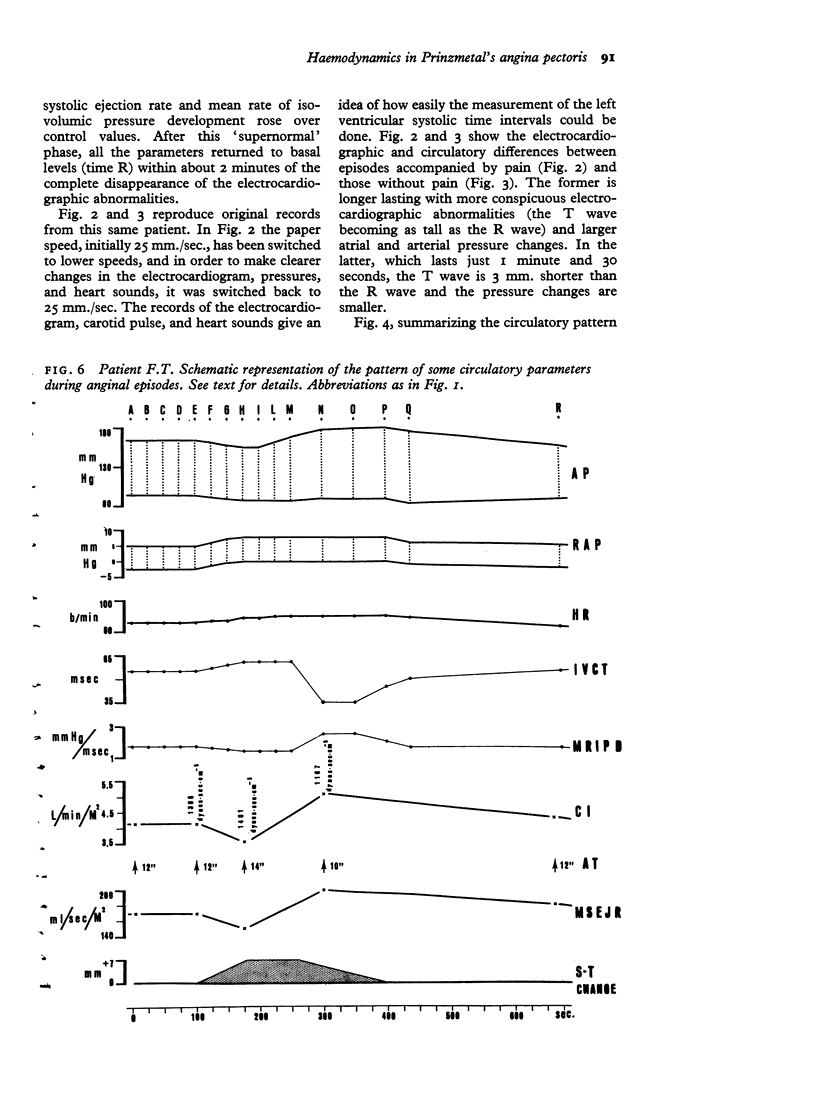
In the 38 recorded anginal episodes, no circulatory change preceded the cardiographic modifications. From the onset of the electrocardiographic abnormalities to the beginning of their reversion, the following circulatory events were observed: (1) obvious reduction of cardiac output; (2) arterial hypotension; (3) lengthening of isovolumic contraction time and mean rate of isovolumic pressure development; (5) reduction of mean systolic ejection rate. It is concluded: (1) that no circulatory factor interfering with work or oxygen consumption of the heart is responsible for eliciting these anginal episodes; (2) that conspicuous left ventricular impairment occurs during the increasing and steady period of the electrocardiographic abnormalities.
As the electrocardiogram started reverting to the pre-attack aspect, cardiac performance rapidly improved and, after a `supernormal' phase, returned in about 2 minutes to basal levels. It is possible that this phase is dependent on a temporary sympathetic compensatory mechanism.
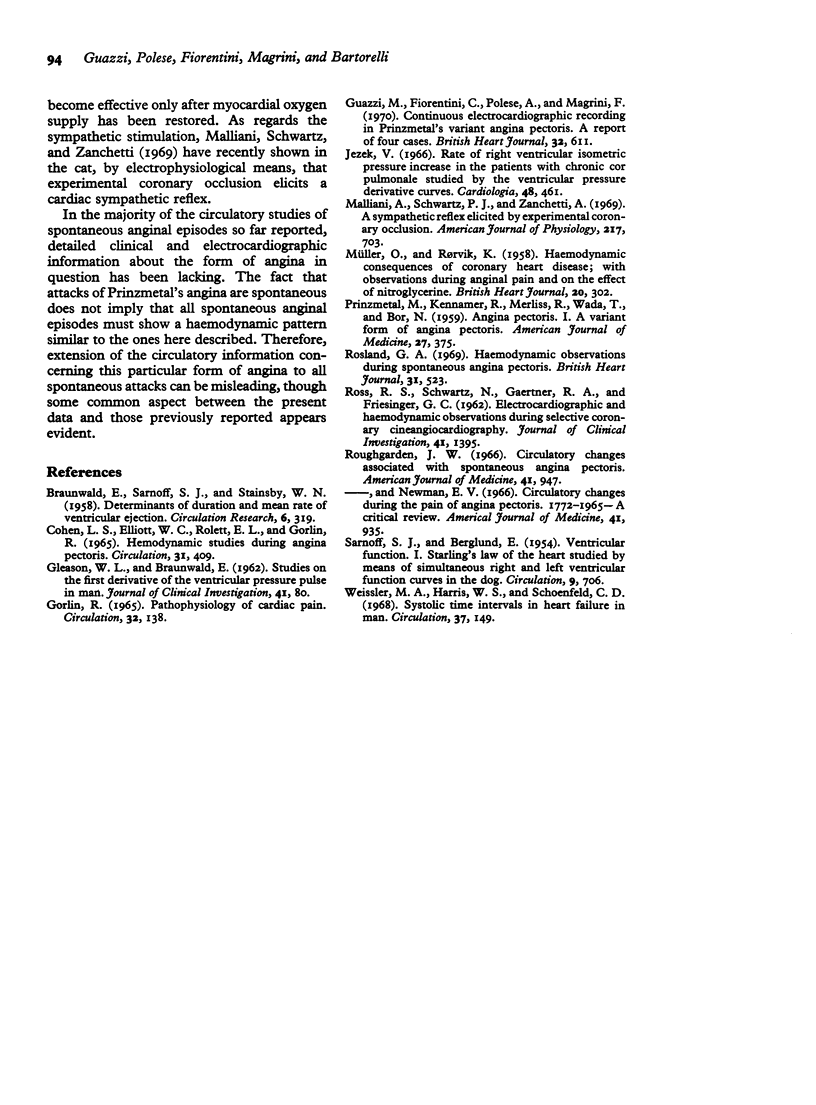
No significant qualitative differences were detected between the circulatory pattern of various anginal episodes. The difference was mainly quantitative and the magnitude of the haemodynamic changes correlated well with the degree of the electrocardiographic abnormalities. Pain, when present, seemed just a concomitant symptom not significantly interfering with the circulatory changes associated with the episodes of this form of angina pectoris.
Full text
PDF
Images in this article

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- BRAUNWALD E., SARNOFF S. J., STAINSBY W. N. Determinants of duration and mean rate of ventricular ejection. Circ Res. 1958 May;6(3):319–325. doi: 10.1161/01.res.6.3.319. [DOI] [PubMed] [Google Scholar]
- COHEN L. S., ELLIOTT W. C., ROLETT E. L., GORLIN R. HEMODYNAMIC STUDIES DURING ANGINA PECTORIS. Circulation. 1965 Mar;31:409–416. doi: 10.1161/01.cir.31.3.409. [DOI] [PubMed] [Google Scholar]
- Jezek V. Rate of right ventricular isometric pressure increase in the patients with chronic cor pulmonale studied by the ventricular pressure derivative curves. Cardiologia. 1966;48(5):461–470. [PubMed] [Google Scholar]
- MULLER O., RORVIK K. Haemodynamic consequences of coronary heart disease with observations during anginal pain and on the effect of nitroglycerine. Br Heart J. 1958 Jul;20(3):302–310. doi: 10.1136/hrt.20.3.302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Malliani A., Schwartz P. J., Zanchetti A. A sympathetic reflex elicited by experimental coronary occlusion. Am J Physiol. 1969 Sep;217(3):703–709. doi: 10.1152/ajplegacy.1969.217.3.703. [DOI] [PubMed] [Google Scholar]
- PRINZMETAL M., KENNAMER R., MERLISS R., WADA T., BOR N. Angina pectoris. I. A variant form of angina pectoris; preliminary report. Am J Med. 1959 Sep;27:375–388. doi: 10.1016/0002-9343(59)90003-8. [DOI] [PubMed] [Google Scholar]
- Rosland G. A. Haemodynamic observations during spontaneous angina pectoris. Br Heart J. 1969 Jul;31(4):523–525. doi: 10.1136/hrt.31.4.523. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roughgarden J. W. Circulatory changes associated with spontaneous angina pectoris. Am J Med. 1966 Dec;41(6):947–961. doi: 10.1016/0002-9343(66)90052-0. [DOI] [PubMed] [Google Scholar]
- Roughgarden J. W., Newman E. V. Circulatory changes during the pain of angina pectoris. 1772-1965--a critical review. Am J Med. 1966 Dec;41(6):935–946. doi: 10.1016/0002-9343(66)90051-9. [DOI] [PubMed] [Google Scholar]
- SARNOFF S. J., BERGLUND E. Ventricular function. I. Starling's law of the heart studied by means of simultaneous right and left ventricular function curves in the dog. Circulation. 1954 May;9(5):706–718. doi: 10.1161/01.cir.9.5.706. [DOI] [PubMed] [Google Scholar]
- Weissler A. M., Harris W. S., Schoenfeld C. D. Systolic time intervals in heart failure in man. Circulation. 1968 Feb;37(2):149–159. doi: 10.1161/01.cir.37.2.149. [DOI] [PubMed] [Google Scholar]