

Abstract
Triceps tendon tear is one of the least commonly recognized major tendon tears. Bilateral triceps tendon tears are especially rare. We present a case of simultaneous complete tears of bilateral triceps tendons secondary to a fall. The anatomy, etiology, image findings, and current literature are discussed.
Abbreviations: MRI, magnetic resonance imaging
Case report
A 42-year-old man with a prior history of anabolic steroid use presented to his primary physician one day after falling on both elbows while playing football. On physical examination, he had mild tenderness and a palpable defect over the olecranons bilaterally. He had full strength on extension; however, he complained of weakness and pain in both arms.
Initially, three view radiographs of both elbows showed a 1-cm ossific fragment in the posterior soft tissue located approximately 4 cm proximal to the posterior aspect of the olecranon. The margins of the fractured fragments were not corticated and thus appeared to be acute. Soft-tissue swelling was also appreciated on the posterior aspect of both arms. These findings indicated bilateral enthesophyte fracture with proximal retraction, suggestive of bilateral partial or complete avulsion/tear of the triceps tendon (Fig. 1).
Figure 1.

42-year-old male with bilateral triceps tendon tear. A. Lateral view of the right elbow B. Lateral view of the left elbow. Black arrows depict ossific fragment and origin of avulsion. White arrows represent soft-tissue swelling.
Subsequent fat-saturated proton-density-weighted MRI of the right (Fig. 2) and left (Fig. 3) elbow revealed bilateral full-thickness tears of the triceps tendons, with extensive edema within the myotendinous portions and surrounding hemorrhage.
Figure 2.
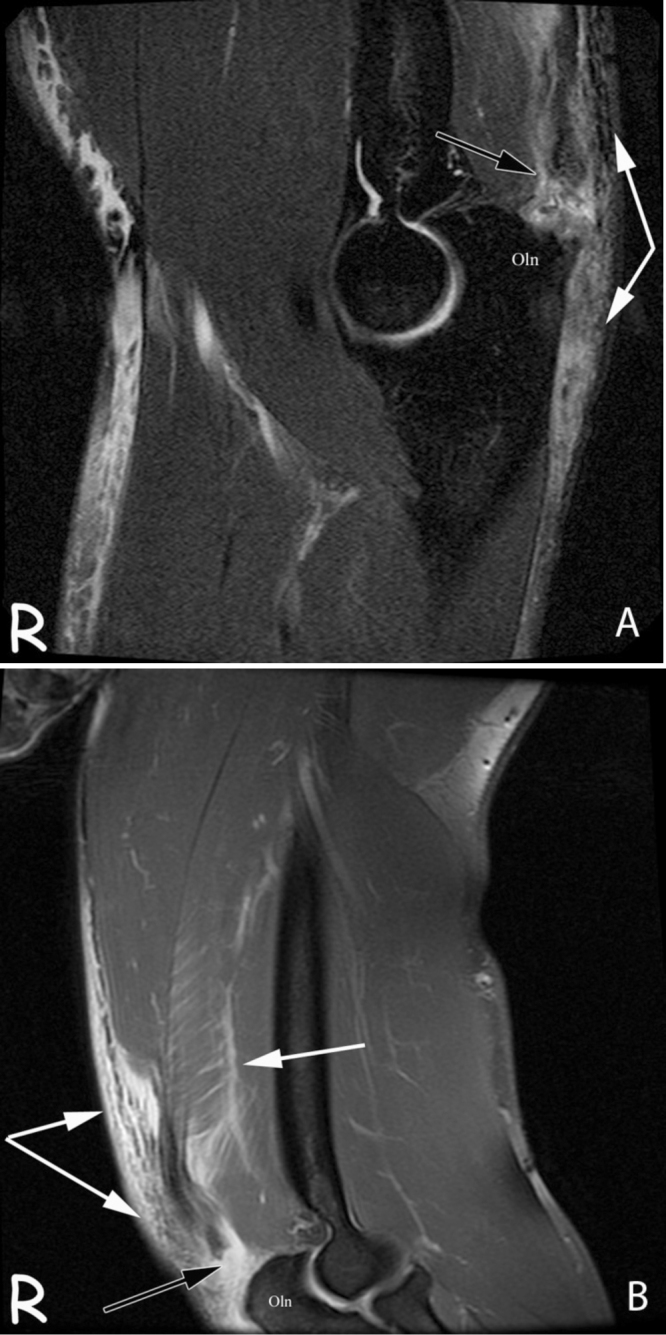
42-year-old male with bilateral triceps tendon tear. A. Sagittal, fat-saturated proton-density-weighted MRI of the right elbow. B. Coronal, fat-saturated proton-density-weighted MRI of the right elbow. Black arrows represent the most distal portion of the triceps tendon. White arrows represent surrounding hemorrhage and edema. Oln = olecranon.
Figure 3.
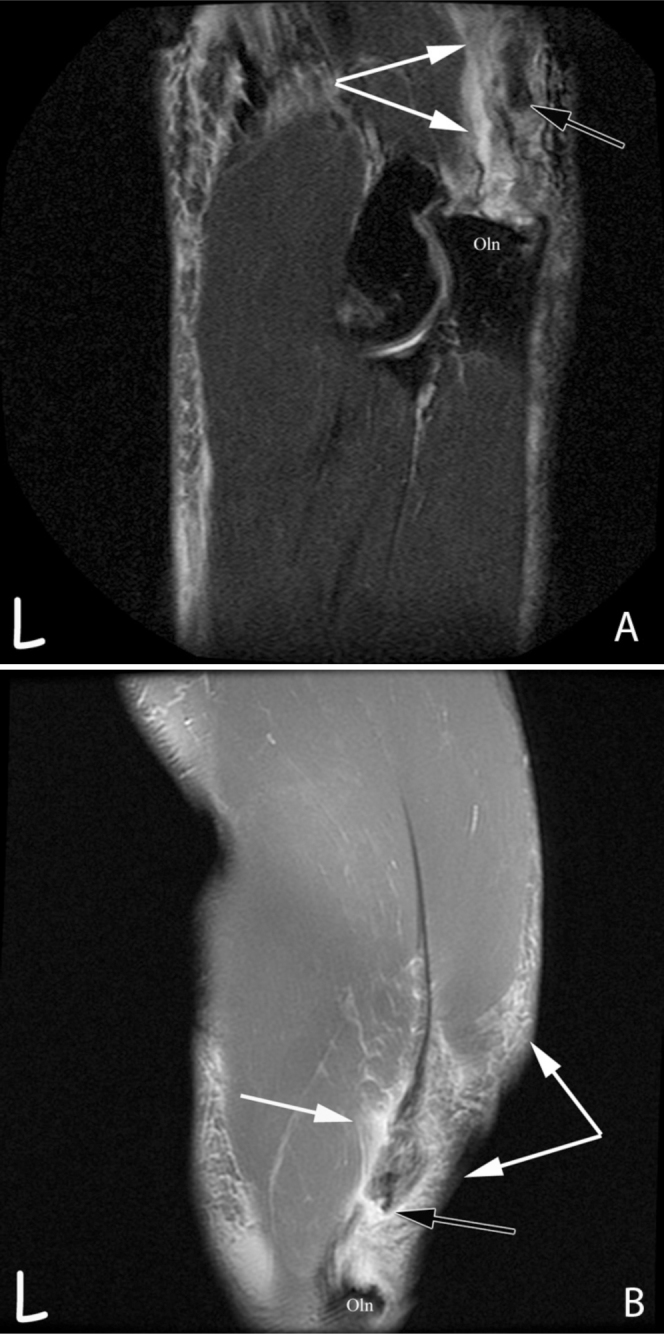
42-year-old male with bilateral triceps tendon tear. A. Sagittal, fat-saturated proton-density-weighted MRI of the left elbow. B. Coronal, fat-saturated proton-density-weighted MRI of the left elbow. Black arrows represent the most distal portion of the triceps tendon. White arrows represent surrounding hemorrhage and edema. Oln = olecranon.
The patient underwent bilateral open triceps tendon repair without complication 15 days after sustaining injury.
Discussion
The insertion and composition of the triceps tendon has been closely investigated in the recent literature. Cadaveric and imaging studies have grossly identified a bilaminar triceps tendon consisting of a deep and superficial tendon (1, 2). The deep tendon is suspected to arise from the medial head, while the superficial tendon arises from the joining of the lateral and long heads (1, 2). Histologically, however, the deep and superficial tendons are not discernable at the insertion on the olecranon process, suggesting that the two tendons may unite before insertion (3). Anatomic variation of the tendon has also been demonstrated (4).
In a limited number of cases, ultrasound has been able to differentiate complete from partial triceps tendon tear, but its ability to localize tears has not been fully studied (5). Thus, MRI remains the imaging modality of choice when evaluating tendons. Due to low free-water content, tendons are often best visualized on T1 and proton-density-weighted imaging (6).
In a review of over 800 elbow MRIs, Koplas et al. cited a 3.8% prevalence of triceps tendon tear (7). This is an increase over the previously documented <1% prevalence from a study performed in 1959 (8). The authors attributed their findings to higher level of anatomic detail provided by modern MRI. Further, triceps tear was clinically suspected in only 43% of their positive cases, suggesting that triceps tears may not be as rare as once thought. Of note, they reported no cases of simultaneous bilateral tear (7).
Risk factors for tear of the triceps tendon include renal failure, repeated local steroid injections, and (most relevant to our case) anabolic steroid use (9, 10, 11). The use of anabolic steroids has been reported to induce structural alterations of tendons, making them more susceptible to tear (12). Mechanisms of injury include fall, direct blow, and weight lifting (9, 10). Triceps tendon tear is commonly associated with avulsion at the site of olecranon insertion, which may be visualized on plain radiography (13).
A handful of case reports on triceps tendon tear have been published, but to our knowledge, only one other case of simultaneous bilateral tear has been documented in a patient without systemic illness. That case involved a body builder performing a bench press with 165-pound dumbbells in each hand, resulting in incomplete rupture with bony avulsion of both triceps. MRI, however, was not possible due to the patient’s body habitus, and ultrasound was used to confirm the diagnosis. Conservative management afforded nearly full recovery at 41 weeks (14).
There is general agreement that surgical repair is the most appropriate management for complete tear of the triceps. However, debate continues over proper management of partial tears (9). The low prevalence of the injury has yielded very few large case series to evaluate treatment options. In a study of 19 professional football players with triceps tendon tears, the authors recommended nonoperative treatment for tears involving less than 75% of the triceps tendon (10). Further evidence may be required before a definite treatment course can be suggested.
In conclusion, triceps tendon rupture should be included in the differential diagnosis for patients presenting with posterior pain and swelling of the elbow. Bilateral triceps tendon tear is exceedingly rare but can be evaluated on the basis of risk factors, physical examination, and imaging. Plain radiography can identify bony avulsion. However, MRI remains the imaging modality of choice for proper evaluation of the tendon and surrounding soft tissue. Complete tears should be repaired surgically, but opinion is divided regarding treatment of partial tears.
Footnotes
Published: October 10, 2011
References
- 1.Madsen M, Marx RG, Millett PJ, Rodeo SA, Sperling JW, Warren RF. Surgical anatomy of the triceps brachii tendon: Anatomical study and clinical correlation. Am J Sports Med. 2006 Nov;34(11):1839–1843. doi: 10.1177/0363546506288752. [PubMed] [DOI] [PubMed] [Google Scholar]
- 2.Belentani C, Pastore D, Wangwinyuvirat M. Triceps brachii tendon: anatomic-MR imaging study in cadavers with histologic correlation. Skeletal Radiol. 2009 Feb;38(2):171–175. doi: 10.1007/s00256-008-0605-6. [PubMed] [DOI] [PubMed] [Google Scholar]
- 3.Chamseddine AH, Jawish RM, Alasiry AA, Zein HK. Ruptures and avulsions of the distal tendon of the triceps brachii. Eur J Orthop Surg Traumatol. DOI 10.1007/s00590-011-0818-6.
- 4.Athwal GS, McGill RJ, Rispoli DM. Isolated avulsion of the medial head of the triceps tendon: An anatomic study and arthroscopic repair in 2 cases. Arthroscopy. 2009 Sep;25(9):983–988. doi: 10.1016/j.arthro.2009.02.020. [PubMed] [DOI] [PubMed] [Google Scholar]
- 5.Tagliafico A, Gandolfo N, Michaud J, Perez MM, Palmieri F, Martinoli C. Ultrasound demonstration of distal triceps tendon tears. Eur J Radiol. 2011 Mar 18 doi: 10.1016/j.ejrad.2011.03.012. [PubMed] [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 6.Tiger E, Mayer DP, Glazer R. Complete avulsion of the triceps tendon: MRI diagnosis. Comput Med Imaging Graph. 1993 Jan-Feb;17(1):51–54. doi: 10.1016/0895-6111(93)90074-w. [PubMed] [DOI] [PubMed] [Google Scholar]
- 7.Koplas MC, Schneider E, Sundaram M. Prevalence of triceps tendon tears on MRI of the elbow and clinical correlation. Skeletal Radiol. 2011 May;40(5):587–594. doi: 10.1007/s00256-010-1043-9. [PubMed] [DOI] [PubMed] [Google Scholar]
- 8.Anzel SH, Covey KW, Weiner AD, Lipscomb PR. Disruption of muscles and tendons; an analysis of 1,014 cases. Surgery. 1959 Mar;45(3):406–414. [PubMed] [PubMed] [Google Scholar]
- 9.Harris PC, Atkinson D, Moorehead JD. Bilateral partial rupture of triceps tendon: case report and quantitative assessment of recovery. Am J Sports Med. 2004 Apr-May;32(3):787–792. doi: 10.1177/0363546503258903. [PubMed] [DOI] [PubMed] [Google Scholar]
- 10.Mair SD, Isbell WM, Gill TJ, Schlegel TF, Hawkins RJ. Triceps tendon ruptures in professional football players. Am J Sports Med. 2004 Mar;32(2):431–434. doi: 10.1177/0095399703258707. [PubMed] [DOI] [PubMed] [Google Scholar]
- 11.Sollender JL, Rayan GM, Barden GA. Triceps tendon reupture in weight lifters. J Sholder Elbow Surg. 1998 Mar-Apr;7(2):151–153. doi: 10.1016/s1058-2746(98)90227-0. [PubMed] [DOI] [PubMed] [Google Scholar]
- 12.Cope MR, Ali A, Bayliss NC. Biceps rupture in body builders: three case reports of rupture of the long head of the biceps at the tendon-labrum junction. J Shoulder Elbow Surg. 2004 Sep-Oct;13(5):580–582. doi: 10.1016/j.jse.2004.03.003. [PubMed] [DOI] [PubMed] [Google Scholar]
- 13.Tarsney FF. Rupture and avulsion of the triceps. Clin Orthop Relat Res. 1972 Mar-Apr;83:177–183. doi: 10.1097/00003086-197203000-00033. [PubMed] [DOI] [PubMed] [Google Scholar]
- 14.Harris PC, Atkinson D, Moorehead JD. Bilateral partial rupture of triceps tendon: Case report and quantitative assessment of recovery. Am J Sports Med. 2004 Apr-May;32(3):787–792. doi: 10.1177/0363546503258903. [PubMed] [DOI] [PubMed] [Google Scholar]