

Abstract
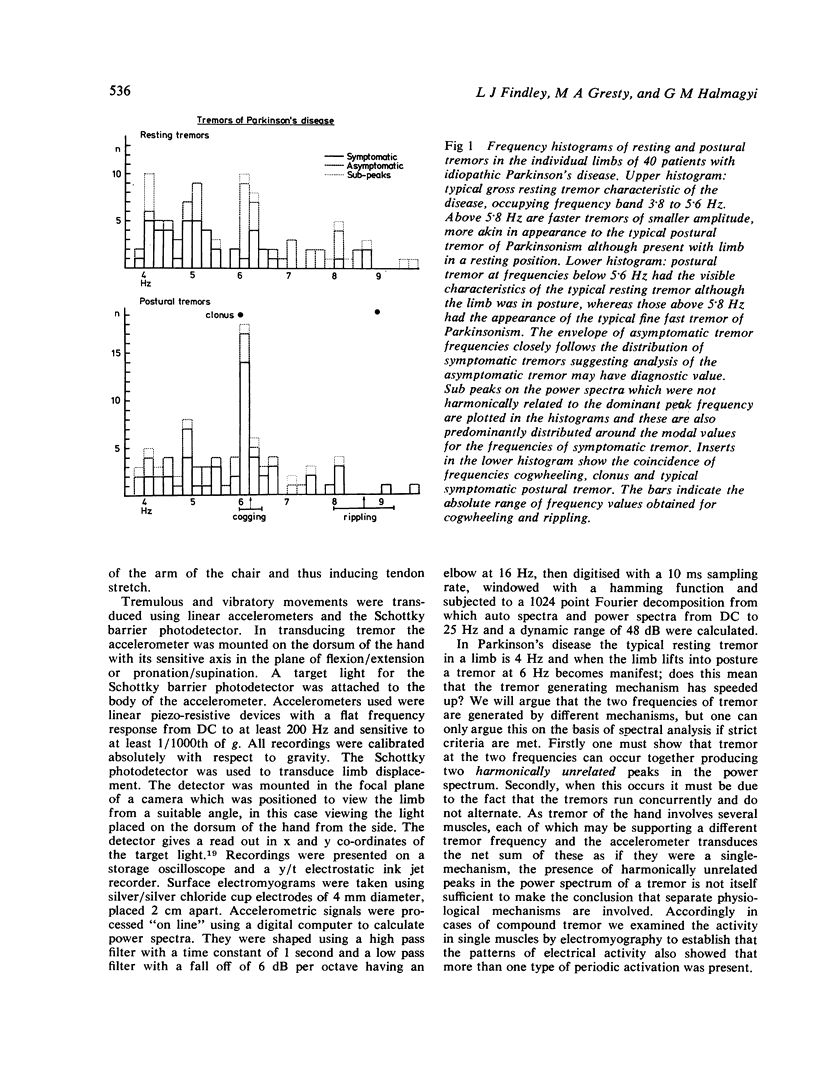
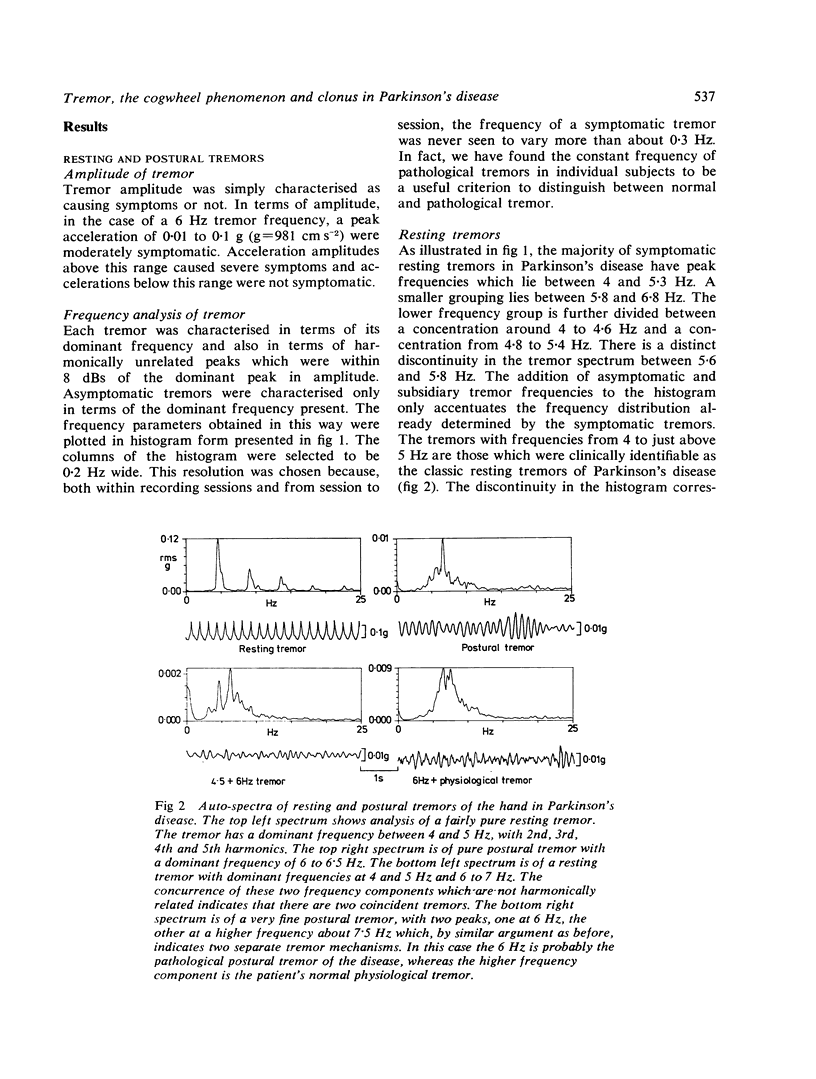
Resting and postural tremor, intention and action tremor, clonus and the cogwheel phenomenon in Parkinson's disease have been characterised in terms of frequency content using spectral analysis. Typical resting tremor ranged in peak frequency from 4 to 5.3 HZ with tremor in each individual varying only by 0.2 to 0.3 HZ. The peak frequency of postural tremor ranged between 6 and 6.2 HZ. Intention tremor appeared to be an exaggeration of postural tremor. Clonus evoked by active or passive stretch at the wrist had a frequency of 6 HZ and appeared to be a continuation of postural tremor. The cogwheel phenomenon was found at frequencies between 6 and 6.5 HZ and between 7.5 to 9 HZ. Action tremor was indistinguishable from the cogwheel phenomenon. Some patients had either a symptomatic resting tremor with a concurrent 6 HZ component of smaller amplitude or a symptomatic postural tremor with a 4-5 HZ component of smaller amplitude. These combinations would produce two peaks in the power spectrum. When this occurred EMG studies showed that individual muscles had two types of rhythmical activation suggesting that the tremors have separate mechanisms. Likewise some patients had a symptomatic 6 HZ tremor on posture with a second peak at 8-10 HZ in the physiological band. Therefore, the 6 HZ postural tremor is not an exaggeration of physiological tremor. On the basis of wave form and frequency similarities postural tremor, the low frequency type of active or passive cogwheeling, intention tremor and clonus possibly involve a common spinal mechanism. Higher frequency cogwheel phenomenon and action tremor may be an exaggeration of physiological tremor. More than 80% of patients with Parkinson's disease manifest tremors at both 4-5 HZ and 6 HZ. This combination would appear to be the strongest objective criterion for the diagnosis of basal ganglia disease.
Full text
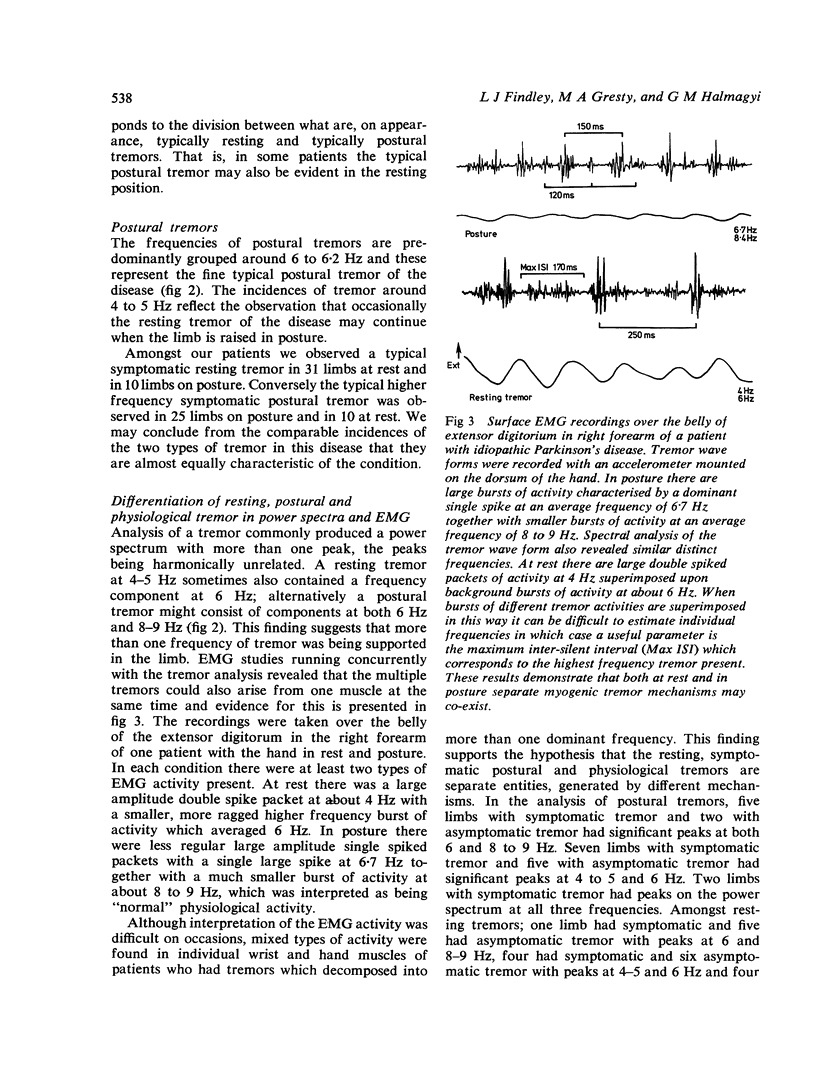
PDF
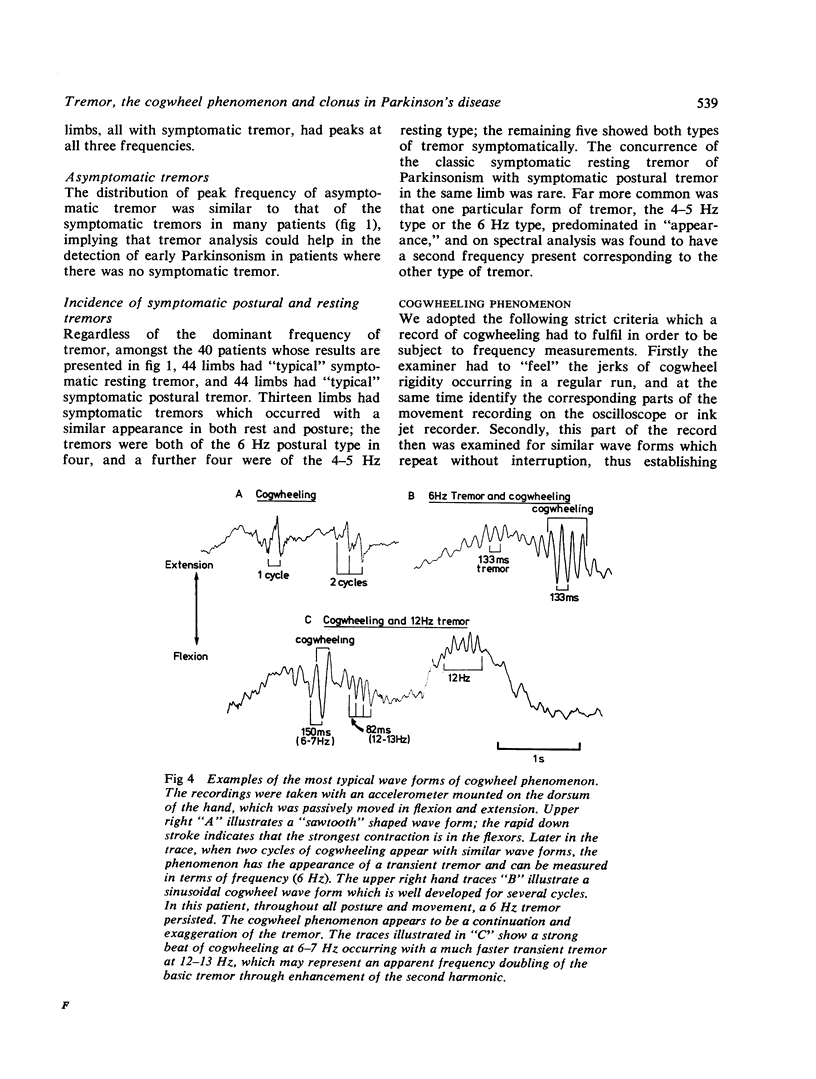
Selected References
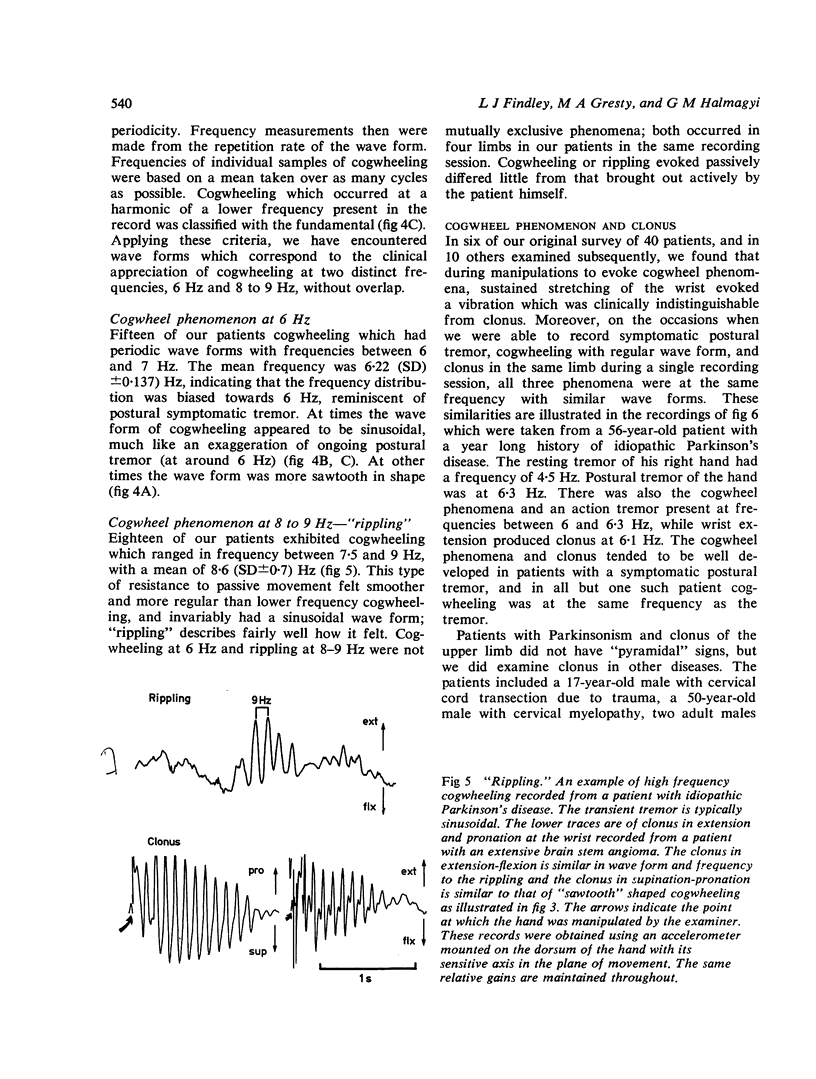
These references are in PubMed. This may not be the complete list of references from this article.
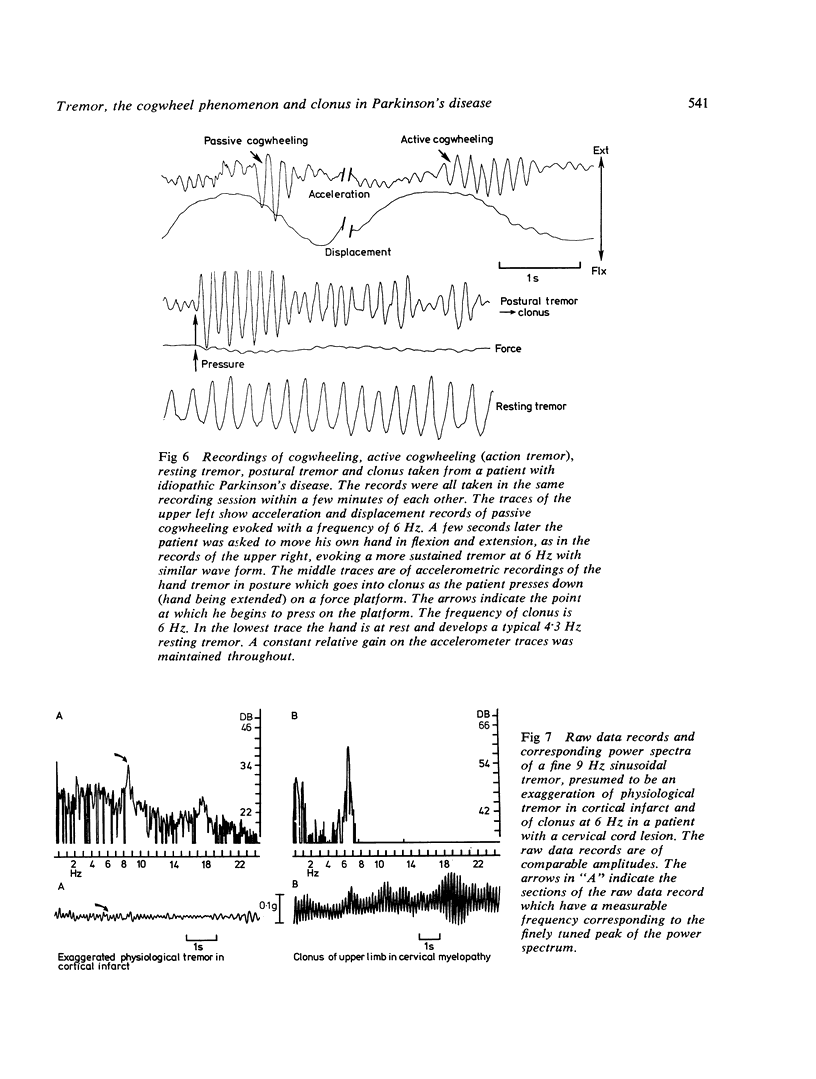
- Aronson N. I. Neurophysiology of tremor. J Neurosurg. 1966 Jan;24(1 Suppl):207–209. [PubMed] [Google Scholar]
- Dimitrijevic M. R., Nathan P. W., Sherwood A. M. Clonus: the role of central mechanisms. J Neurol Neurosurg Psychiatry. 1980 Apr;43(4):321–332. doi: 10.1136/jnnp.43.4.321. [DOI] [PMC free article] [PubMed] [Google Scholar]
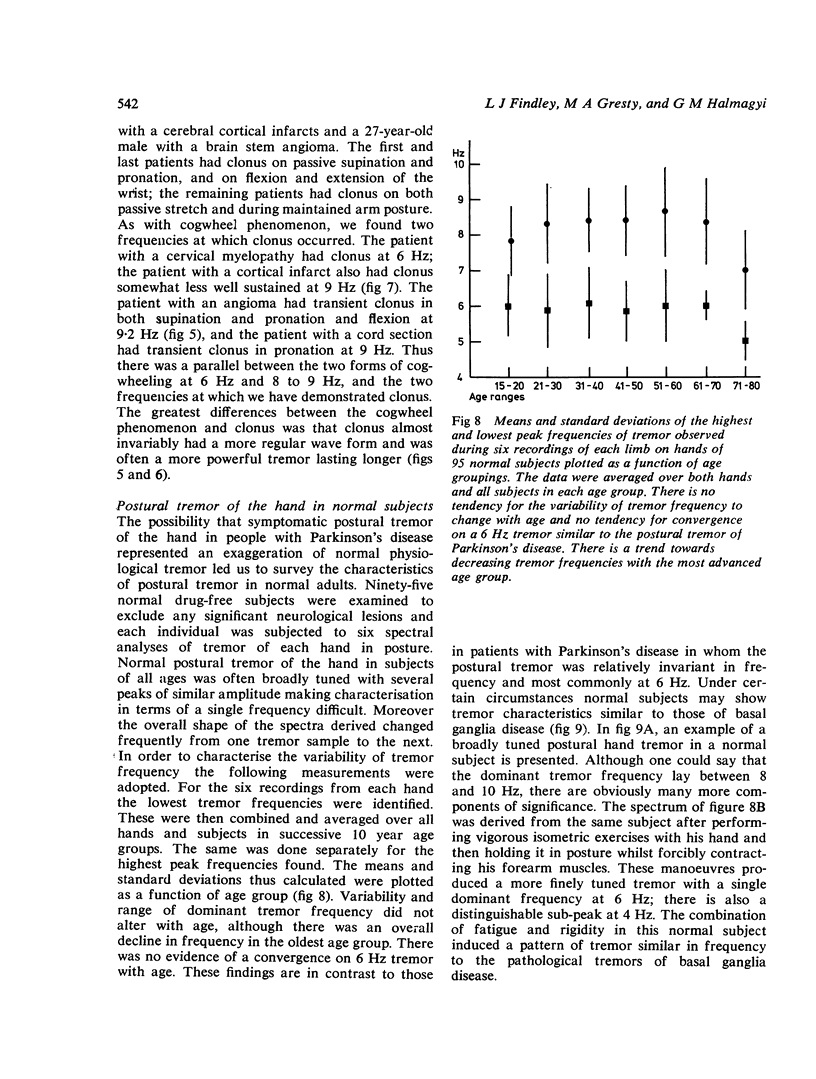
- EHRINGER H., HORNYKIEWICZ O. [Distribution of noradrenaline and dopamine (3-hydroxytyramine) in the human brain and their behavior in diseases of the extrapyramidal system]. Klin Wochenschr. 1960 Dec 15;38:1236–1239. doi: 10.1007/BF01485901. [DOI] [PubMed] [Google Scholar]
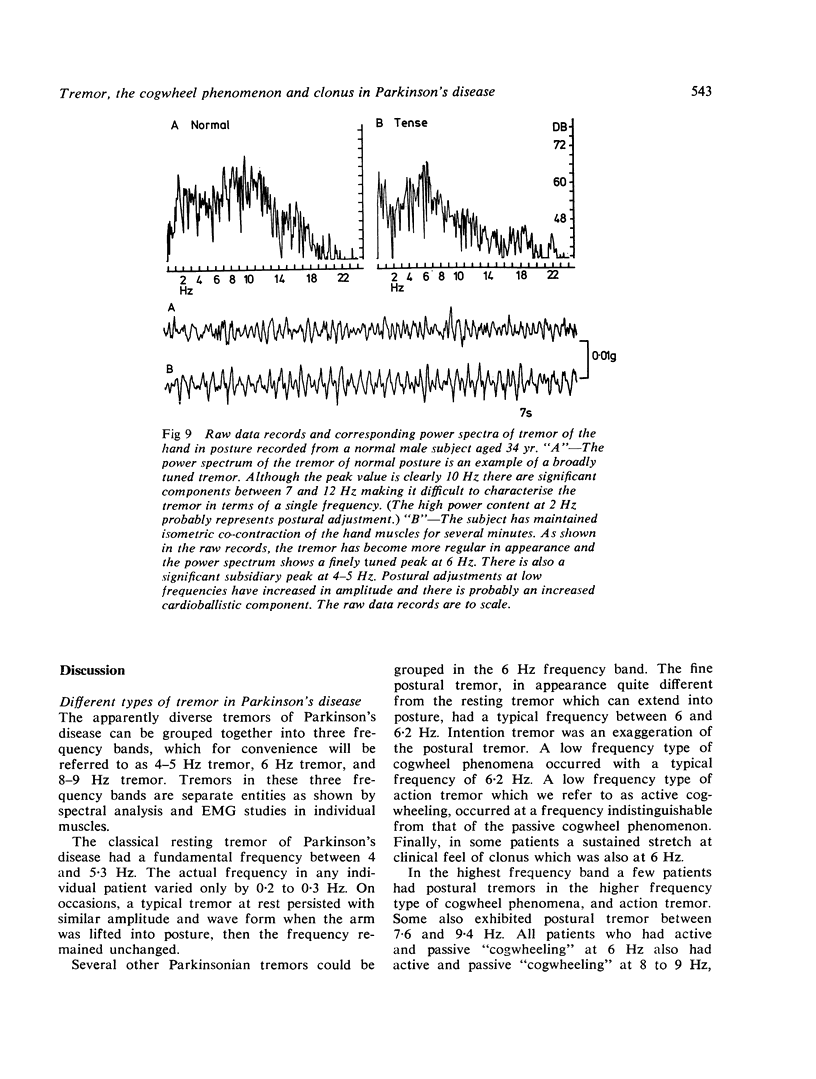
- Findley L. J., Gresty M. A., Halmagyi M. G. A novel method of recording arm movements. A survey of common abnormalities. Arch Neurol. 1981 Jan;38(1):38–42. doi: 10.1001/archneur.1981.00510010064011. [DOI] [PubMed] [Google Scholar]
- LANCE J. W., SCHWAB R. S., PETERSON E. A. Action tremor and the cogwheel phenomenon in Parkinson's disease. Brain. 1963 Mar;86:95–110. doi: 10.1093/brain/86.1.95. [DOI] [PubMed] [Google Scholar]
- MATTHEWS P. B., RUSHWORTH G. The selective effect of proCaine on the stretch reflex and tendon jerk of soleus muscle when applied to its nerve. J Physiol. 1957 Feb 15;135(2):245–262. doi: 10.1113/jphysiol.1957.sp005707. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marsden C. D., Meadows J. C., Lange G. W., Watson R. S. The relation between physiological tremor of the two hands in healthy subjects. Electroencephalogr Clin Neurophysiol. 1969 Aug;27(2):179–185. doi: 10.1016/0013-4694(69)90171-0. [DOI] [PubMed] [Google Scholar]