

Abstract
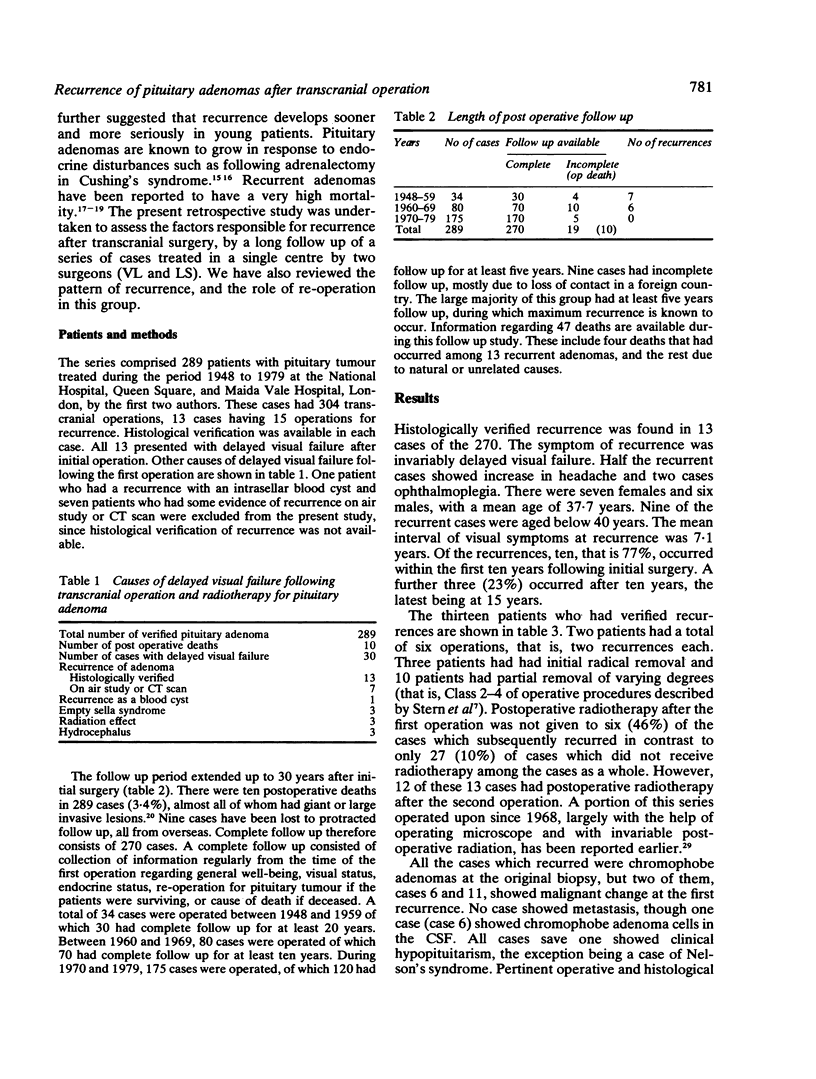
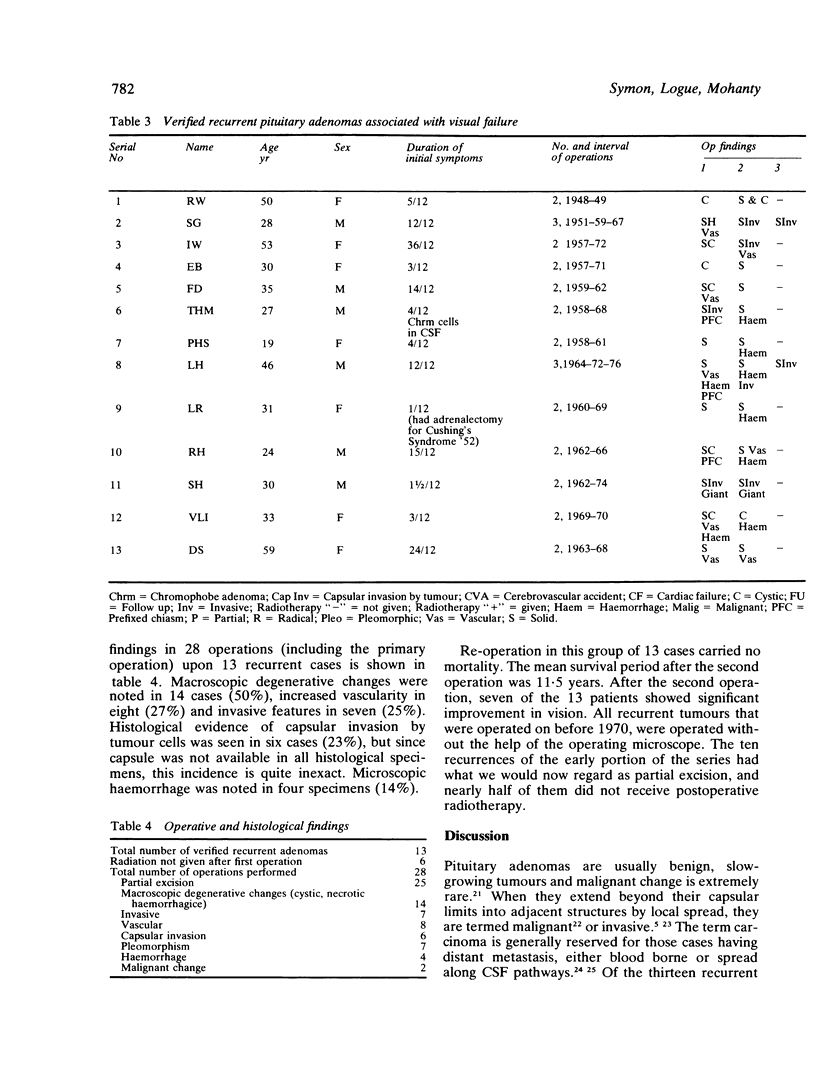
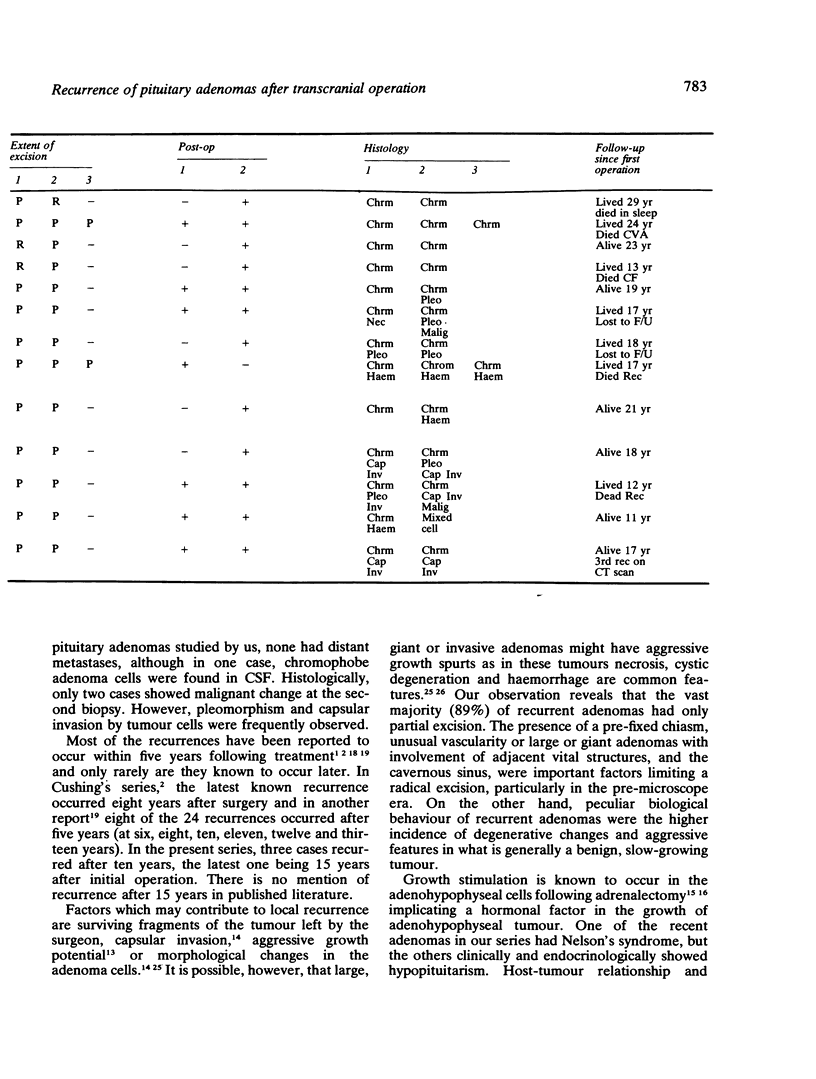
A series of 289 pituitary adenomas operated upon transcranially have been assessed for the frequency of recurrence. Ten patients died in the postoperative period, and nine patients have been lost to follow up. Follow up data is therefore available in a series of 270 cases for a period extending up to 30 years after the initial operation. There have been 13 histologically verified recurrences (4.8%), and a further six cases are known from CT scan or air study evidence to have residual or recurrent tumour which has not necessitated re-exploration. The total recurrence or residual tumour rate could therefore be regarded as 7.4%. The large majority (77%) of recurrences have been within 10 years of the first operation, and the rest between 10 and 20 years. Histologically, all were chromophobe adenomas, and the average age of their initial presentation was lower than the peak incidence of pituitary adenoma as a whole. Two patients showed frank malignant change in the second biopsy. In recurrent tumours, most had had only subtotal excision with some macroscopic evidence of invasion or degeneration, such as cystic change, haemorrhage or necrosis. Microscopic evidence of aggressive growth and capsular invasion by tumour cells also was relatively frequent. Postoperative radiotherapy decreased and delayed recurrence, although the vast majority of cases in the series received radiotherapy. Surgery for recurrence appeared an effective method of treatment, and no patient died following repeated operation. Initial transcranial excision in more recent years using the operating microscope followed by uniform radiotherapy, appears to have considerably reduced the already small recurrence rate of pituitary adenoma.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- BAKAY L. The results of 300 pituitary adenoma operations (Prof. Herbert Olivecrona's series). J Neurosurg. 1950 May;7(3):240–255. doi: 10.3171/jns.1950.7.3.0240. [DOI] [PubMed] [Google Scholar]
- COLBY M. Y., Jr, KEARNS T. P. Radiation therapy of pituitary adenomas with associated visual impairment. Proc Staff Meet Mayo Clin. 1962 Jan 3;37:15–24. [PubMed] [Google Scholar]
- Clark K. Surgery for the recurrent pituitary adenoma. Clin Neurosurg. 1980;27:309–314. doi: 10.1093/neurosurgery/27.cn_suppl_1.309. [DOI] [PubMed] [Google Scholar]
- ECHOLS D. H. Experience with surgical treatment in twenty cases of pituitary adenomas. J Neurosurg. 1958 Jul;15(4):447–454. doi: 10.3171/jns.1958.15.4.0447. [DOI] [PubMed] [Google Scholar]
- EPSTEIN J. A., EPSTEIN B. S., MOLHO L., ZIMMERMAN H. M. CARCINOMA OF THE PITUITARY GLAND WITH METASTASES TO THE SPINAL CORD AND ROOTS OF THE CAUDA EQUINA. J Neurosurg. 1964 Oct;21:846–853. doi: 10.3171/jns.1964.21.10.0846. [DOI] [PubMed] [Google Scholar]
- GERMAN W. J., FLANIGAN S. PITUITARY ADENOMAS: A FOLLOW-UP STUDY OF THE CUSHING SERIES. Clin Neurosurg. 1964;10:72–81. doi: 10.1093/neurosurgery/10.cn_suppl_1.72. [DOI] [PubMed] [Google Scholar]
- HORRAX G., HARE H. F., POPPEN J. L., HURXTHAL L. M., YOUNGHUSBAND O. Z. Chromophobe pituitary tumors. II. Treatment. J Clin Endocrinol Metab. 1952 Jun;12(6):631–641. doi: 10.1210/jcem-12-6-631. [DOI] [PubMed] [Google Scholar]
- Jefferson G. Extrasellar Extensions of Pituitary Adenomas: (Section of Neurology). Proc R Soc Med. 1940 May;33(7):433–458. [PMC free article] [PubMed] [Google Scholar]
- MARGUTH F., NOVER A. MORPHOLOGIE UND KLINIK DER HYPOPHYSENADENOM-REZIDIVE. Acta Neurochir (Wien) 1964;11:716–730. doi: 10.1007/BF01402143. [DOI] [PubMed] [Google Scholar]
- Mohanty S., Tandon P. N., Banerji A. K., Prakash B. Haemorrhage into pituitary adenomas. J Neurol Neurosurg Psychiatry. 1977 Oct;40(10):987–991. doi: 10.1136/jnnp.40.10.987. [DOI] [PMC free article] [PubMed] [Google Scholar]
- NELSON D. H., MEAKIN J. W., THORN G. W. ACTH-producing pituitary tumors following adrenalectomy for Cushing's syndrome. Ann Intern Med. 1960 Mar;52:560–569. doi: 10.7326/0003-4819-52-3-560. [DOI] [PubMed] [Google Scholar]
- RAY B. S. SURGERY OF RECURRENT INTRACRANIAL TUMORS. Clin Neurosurg. 1964;10:1–30. doi: 10.1093/neurosurgery/10.cn_suppl_1.1. [DOI] [PubMed] [Google Scholar]
- Ray B. S., Patterson R. H., Jr Surgical experience with chromophobe adenomas of the pituitary gland. J Neurosurg. 1971 Jun;34(6):726–729. doi: 10.3171/jns.1971.34.6.0726. [DOI] [PubMed] [Google Scholar]
- Spark R. F., Dickstein G., Pallotta J. Complete remission of acromegaly with medical treatment. JAMA. 1979 Feb 9;241(6):573–575. [PubMed] [Google Scholar]
- Stern W. E., Batzdorf U. Intracranial removal of pituitary adenomas. An evaluation of varying degree of excision from partial to total. J Neurosurg. 1970 Nov;33(5):564–573. doi: 10.3171/jns.1970.33.5.0564. [DOI] [PubMed] [Google Scholar]
- Symon L., Jakubowski J. Transcranial management of pituitary tumours with suprasellar extension. J Neurol Neurosurg Psychiatry. 1979 Feb;42(2):123–133. doi: 10.1136/jnnp.42.2.123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wirth F. P., Schwartz H. G., Schwetschenau P. R. Pituitary adenomas: factors in treatment. Clin Neurosurg. 1974;21:8–25. doi: 10.1093/neurosurgery/21.cn_suppl_1.8. [DOI] [PubMed] [Google Scholar]