

Abstract
Background:
Carpal tunnel syndrome (CTS) considers the most common compression neuropathy, which nerve conduction studies (NCSs) used for its detection routinely and universally. This study was performed to determine the value of the median TLI and other NCS variables and to investigate their sensitivity and specificity in the diagnosis of CTS.
Materials and Methods:
The study was carried out among 100 hands of healthy volunteers and 50 hands of patients who had a positive history of paresthesia and numbness in upper extremities. Information including age, gender, and result of sensory and motor nerve conduction velocity (MNCV), peak latency difference of median and ulnar nerves of fourth digit (M4-U4 peak latency difference), and TLI were recorded for analysis. Sensitivity and specificity of electro diagnostic parameters in the diagnosis of CTS was investigated.
Results:
Normal range of the median nerve TLI was 0.43 ± 0.077. There was no significant difference between two groups for MNCV means (P = 0. 45). Distal sensory latency and distal motor latency (DML) of median nerve and fourth digit median-ulnar peak latency differences (PM4-PU4) for CTS group was significantly higher (P < 0.001) and mean for sensory nerve conduction velocity was significantly higher in control group (P < 0.001). The most sensitive electrophysiological finding in CTS patients was median TLI (82%), but the most specific one was DML (98%).
Conclusion:
Although in early stages of CTS, we usually expect only abnormalities in the sensory studies, but TLI may better demonstrate the effect on median nerve motor fiber even in mild cases of CTS.
Keywords: Carpal tunnel syndrome, median nerve, nerve conduction study, terminal latency index
INTRODUCTION
The hand is a mirror of human brain function. Hand reflects human feeling and sensation and conformity between hand and feeling provide a tool for expressing issues and connecting to others.[1] One of the problems can cause the complications of hand function considers carpal tunnel syndrome (CTS). CTS is the most common form of entrapment neuropathies, which occurs due to median nerve compression in the wrist, and could last months or even years. CTS symptoms and signs include numbness, tingling, and paresthesia or the intermittent pain of thumb, index finger or middle finger, which results in severe functional disorders as consequences of the sensory complications.[2,3] Recent evidences were presented high incidence of the condition and related complications for the patients, in order to properly assess nerve function during the primary stages of disease development and ascertaining the patient condition, the need for sensitive and repetitive tests are felt. In this regard and for detection of many diseases such as CTS and due to complications occurs during surgery in nerve electrical activities, an electrical diagnosis such as nerve conduction study (NCS) is applicable.[4,5,6] Unfortunately, until now there is no consensus among researchers regarding what qualifies the number and the type of NCSs to better ascertain of neurophysiological diagnosis of potential CTS in order to select the most practical parameters among NCS parameters to ascertain of CTS definite incidence.[5] The electrodiagnostic parameters sensitivity for CTS diagnosis in the previous published studies were reported in wide ranges. Sensitivity of distal motor latency (DML) of median nerve was 20–81%,[7] sensory latency wrist-digit sensitivity was 40–100%[8] and fourth digit median-ulnar peak latency differences (PM4-PU4) was 56–100%.[9] Terminal latency index (TLI) of the median nerve considers a parameter, which displays the existence abnormality in the distal segment of peripheral nerves that is calculated by the formula,[10] with a normal range of ≥0.34.[2] A previous study have been reported that by calculating residual latency it was possible to determine the effect on median nerve motor fibers in early CTS diagnosis, as similar as TLI.[11] Although assessment of TLI provide additional information about distal nerve segments, especially in patients with high clinical suspicion of CTS but without abnormality in the routine NCS, determination of this index requiring no additional electrical stimulation, so that it may help to early diagnosis of CTS.
MATERIALS AND METHODS
This is a cross-sectional study, which was carried out from March 2013 to October 2013 among 100 hands of healthy volunteers and 50 hands of patients with signs and symptoms that suggested CTS. It was performed in Electrodiagnosis Center of Alzahra Hospital of Isfahan University of Medical Sciences, after explaining the procedure, and taking written consent. The participant's age were between 20 and 70 years old, which were divided into two groups: Patients and control groups. Subjects were selected by simple random sampling. The groups were divided subsequently into two age subgroups; 20–40 and 40–70 years old.
Patients who had a positive history of paresthesia and paining upper extremities (in three lateral and radial half of fourth digits) and 2 of 3 sign suggesting CTS (1 Tinel's sign: Paresthesia that radiating in a median nerve distribution with tapping on the wrist over the median nerve, [2] median compression test: Pressure over the proximal edge of the carpal ligament [proximal wrist crease]) with thumbs causes paresthesia to develop or increase in the median nerve distribution, (3) Phalen's test: Paresthesia that radiating in a median nerve distribution within 60s of sustained flexion of the wrist were included as CTS group.[1]
The control group was persons who had neither signs nor symptoms of neurologic abnormalities of upper extremities in their history and physical examination.
Exclusion criteria were any history of hereditary polyneuropathies (e.g., Charcot-Marie-Tooth), acquired polyneuropathies (e.g., diabetic polyneuropathy), surgery or local steroid injections for CTS and patients who had any scar formation or history of fracture at the sites of stimulation or recording.[1]
A normal room temperature (mean: 25°C) and a skin temperature of over 31°C (32–34°C) were maintained and the study was performed with surface stimulation electrode using constant current and surface bar recording electrodes.[2]
Cadwell EMG machine was used for this study. For obtaining the median nerve compound motor action potential (CMAP), the active electrode (E-I) was located on the abductor pollicis brevis motor point with the reference electrode (E-II) placed distally, stimulation has been made 8 cm proximally at wrist. A second stimulus was applied to the median nerve at the antecubital fossa. Using a supramaximal impulse for both stimulation sites, the CMAP recorded, and forearm NCV was obtained. For antidromic median nerve sensory action potential (SNAP), the E-I recording electrode was located on the second or third digit just distal to the metacarpophalangeal (MCP) joint region and the E-II electrode placed at least 4 cm more distal on the respective digit. The median nerve is excited 7 cm[1] and 14 cm proximal to E-I at wrist again with a supramaximal current intensity.[2] For antidromic fourth digit, the E-I recording electrode was located on the fourth digit just distal to the MCP joint and the E-II electrode placed at least 4 cm more distal on the fourth digit. The median and ulnar nerves are stimulated 14 cm proximal to E-I at wrist again with a supramaximal current intensity. The difference between two distal sensory latency (DSL) (M4-U4 peak latency difference) is bases for diagnosis.[12]
The TLI is calculated as follows: Terminal distance ÷ (proximal conduction mm velocity m/s × distal latency ms). A value of 0.34 or greater is considered normal.
For the median nerve.[4,8] The instrument settings for median CMAP assessment were an amplifier sensitivity of 1,000 µV/div, a sweep of 2 or 5 ms/div and it was changed to an amplifier sensitivity of 10–20 µV/div and a sweep of 1 or 2 ms/div for SNAP recordings.
Information including age, gender, and results of CMAP and SNAP of the median nerve (as explained previously) and M4-U4 peak latency difference, was recorded for analysis.
Statistical analysis
The SPSS version 20 was used square test was used for the comparison of nominal data. Sensitivity and specificity of variables were based on receiver operating characteristic (ROC) curve analysis. to calculate the average values and standard deviation. Independent Student t-test was used for comparison of mean values among study groups. Comparison between the averages NCS values of the CTS and control groups also were performed by independent Student's t-test. Chi-square test was used for the comparison of nominal data. Sensitivity and specificity of variables were based on receiver operating characteristic (ROC) curve analysis.
RESULTS
A total number of 50 hands with CTS (42 women, 8 men) and 100 healthy controls (72 women, 28 men) were investigated after taking anamnesis and performing the neurological and electrophysiological examination. No significant difference was found between the mean ages of the CTS (44.4 ± 10.7 years) and the control groups (44.2 ± 12.1 years) (P > 0.05).
Mean for TLI of the median nerve for CTS group was 0.375 ± 0.08 and for the control group was 0.43 ± 0.07 which shows a significantly lower mean for CTS group compared to control group (P < 0.05). Independent t-test showed no significant difference between the two groups for motor nerve conduction velocity means (P = 0. 45). However, DSL and DML and PM4-PU4 for CTS group was significantly higher compared to control group (P < 0.001) and mean for sensory nerve conduction velocity (SNCV) variable was significantly higher in control group compare to CTS group (P < 0.001) [Table 1].
Table 1.
Values of the various nerve conduction parameters of median nerve in CTS and normal groups
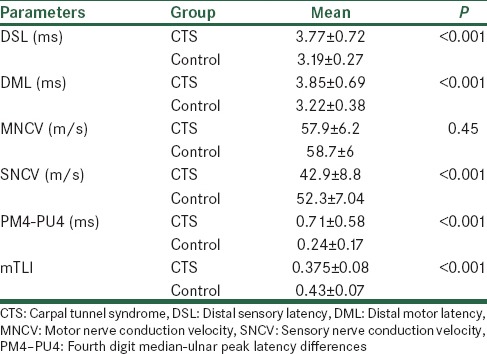
Table 2 shows the sensitivity, specificity, of electrophysiological diagnostic tests for the CTS patients.
Table 2.
Sensitivity and specificity of nerve conduction variables for median nerve in CTS patients
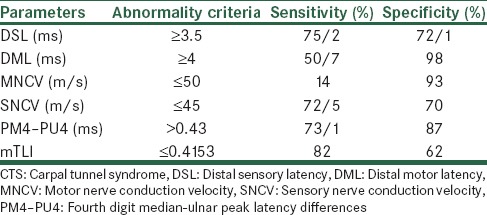
The most sensitive electrophysiological finding in CTS patients was mTLI (82%), but the most specific one was DML (98%) [Table 2].
Given that the area under the curve (AUC) is more than 70%, therefore, mTLI is able to distinguish between two groups and has diagnostic reliability. mTLI cut-off point for distinguishing between two groups was 0.4153.
In the next step, the ROC curve was distinguished the diagnostic reliability between two study groups, CTS group, and a control group; which according to 79.8% AUC of PM4-PU4, it has been recognized that this parameter had more AUC than mTLI (73.9%), hence PM4-PU4 had better reliability for diagnostic purposes [Figure 1].
Figure 1.

Receiver operating characteristic curve diagram for assessing the diagnostic legitimacy of mTLI and peak latency difference of median and ulnar nerves of the fourth digit for distinguishing between carpal tunnel syndrome group and control group
DISCUSSION
Our results showed regardless of the high sensitivity of mTLI for CTS detection, but PM4-PU4 has better diagnostic reliability compare to mTLI, according to the AUC of the ROC respectively. In a prospective study were published by Uzar et al. showed highest sensitivity was obtained for 3 following parameters: Median DSL (mDSL) 91.5%, PM4-PU4 91.5%, mTLI 90.1%. In all CTS patients with prolonged mMDL values, and also in 22.6% with normal mMDL, mTLI was found to be lower than normal values. Compared with mMDL, the sensitivity of mTLI in the diagnosis of CTS was found to be higher but its specificity was lower. The electrophysiological findings with the highest sensitivity and specificity in the diagnosis of CTS among conventional NCS were mDSL, PM4-PU4 and motor SNCV.[1] In another study that were published by Aygül, et al., comparing common conventional and new electrophysiological techniques in CTS detection and their relation to body mass index, they concluded that two parameters show the highest sensitivity in CTS detection: M4-U4 peak latency difference 77% and mTLI 70.3%.[3] Kuntzer has found that while mTLI has high sensitivity but it bears low specificity.[9] Karata et al. (2000) noted that sensory and motor NCV of the median nerve (median mixed nerve conduction velocity) an mTLI had a highest diagnostic sensitivity.[13] In a prospective study by Simovic and Weinberg, they have been reported that the mean of mTLI in the CTS group was 0.25, but in control group this mean was estimated to be 0.44.[10] Furthermore, they have been reported that mTLI sensitivity was 81.5%.[14] In addition, in a study that was published by Shakouri et al. (2006). Their results showed TLI in CTS group was 0.3 ± 0.05 and in the control group was estimated to be 0.42 ± 0.03 and its sensitivity was reported to be 73%.[15] In conclusion, it has been understood that TLI parameter is not a better parameter compare to NCS parameters for CTS detection.
CONCLUSION
Finally, if one obtain normal findings after performing the routine NCSs, especially if there is a clinical suspicious to CTS, we showed that use ofTLI parameter separately is not a better parameter compare to routine NCS parameters but combination of median TLI and PM4-PU4 can provide better predictor in the diagnosis of CTS.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
This study was supported by the Isfahan University of Medical Sciences (research project number 392304).
REFERENCES
- 1.Uzar E, Tamam Y, Acar A, Yucel Y, Palanci Y, Cansever S, et al. Sensitivity and specificity of terminal latency index and residual latency in the diagnosis of carpal tunnel syndrome. Eur Rev Med Pharmacol Sci. 2011;15:1078–84. [PubMed] [Google Scholar]
- 2.Dumitru D, Zwartz MJ. Focal peripheral neuropathies. In: Dumitru D, Amato AA, Zwarts M, editors. Electrodiagnostic Medicine. 2nd ed. Philadelphia: Hanley & Belfus; 2002. pp. 195–201. [Google Scholar]
- 3.Aygül R, Ulvi H, Kotan D, Kuyucu M, Demir R. Sensitivities of conventional and new electrophysiological techniques in carpal tunnel syndrome and their relationship to body mass index. J Brachial Plex Peripher Nerve Inj. 2009;4:12. doi: 10.1186/1749-7221-4-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ogura T, Akiyo N, Kubo T, Kira Y, Aramaki S, Nakanishi F. The relationship between nerve conduction study and clinical grading of carpal tunnel syndrome. J Orthop Surg (Hong Kong) 2003;11:190–3. doi: 10.1177/230949900301100215. [DOI] [PubMed] [Google Scholar]
- 5.Smith NJ. Nerve conduction studies for carpal tunnel syndrome: Essential prelude to surgery or unnecessary luxury? J Hand Surg Br. 2002;27:83–5. doi: 10.1054/jhsb.2001.0669. [DOI] [PubMed] [Google Scholar]
- 6.Rosén I. Neurophysiological diagnosis of the carpal tunnel syndrome: Evaluation of neurographic techniques. Scand J Plast Reconstr Surg Hand Surg. 1993;27:95–101. doi: 10.3109/02844319309079790. [DOI] [PubMed] [Google Scholar]
- 7.Scelsa SN, Herskovitz S, Bieri P, Berger AR. Median mixed and sensory nerve conduction studies in carpal tunnel syndrome. Electroencephalogr Clin Neurophysiol. 1998;109:268–73. doi: 10.1016/s0924-980x(98)00018-6. [DOI] [PubMed] [Google Scholar]
- 8.Jablecki CK, Andary MT, So YT, Wilkins DE, Williams FH. Literature review of the usefulness of nerve conduction studies and electromyography for the evaluation of patients with carpal tunnel syndrome. AAEM Quality Assurance Committee. Muscle Nerve. 1993;16:1392–414. doi: 10.1002/mus.880161220. [DOI] [PubMed] [Google Scholar]
- 9.Kuntzer T. Carpal tunnel syndrome in 100 patients: Sensitivity, specificity of multi-neurophysiological procedures and estimation of axonal loss of motor, sensory and sympathetic median nerve fibers. J Neurol Sci. 1994;127:221–9. doi: 10.1016/0022-510x(94)90076-0. [DOI] [PubMed] [Google Scholar]
- 10.Simovic D, Weinberg DH. Terminal latency index in the carpal tunnel syndrome. Muscle Nerve. 1997;20:1178–80. doi: 10.1002/(sici)1097-4598(199709)20:9<1178::aid-mus14>3.0.co;2-p. [DOI] [PubMed] [Google Scholar]
- 11.Khosrawi S, Dehghan F. Determination of the median nerve residual latency values in the diagnosis of carpal tunnel syndrome in comparison with other electrodiagnostic parameters. J Res Med Sci. 2013;18:934–8. [PMC free article] [PubMed] [Google Scholar]
- 12.Johnson EW, Kukla RD, Wongsam PE, Piedmont A. Sensory latencies to the ring finger: Normal values and relation to carpal tunnel syndrome. Arch Phys Med Rehabil. 1981;62:206–8. [PubMed] [Google Scholar]
- 13.Karata M, Sozay S, Bayramo LU. Terminal latency index and residual latency in Carpal Tunnel Syndrome. Romatizma. 2000;15:105–11. [Google Scholar]
- 14.Simovic D, Weinberg DH. The median nerve terminal latency index in carpal tunnel syndrome: A clinical case selection study. Muscle Nerve. 1999;22:573–7. doi: 10.1002/(sici)1097-4598(199905)22:5<573::aid-mus4>3.0.co;2-a. [DOI] [PubMed] [Google Scholar]
- 15.Shakouri SK, Eftekhar Sadat B, Salekzamani Y, Taheragdam A, Abedi F. Determination of terminal latency index in carpal tunnel syndrome. Med J Tabriz Univ Med Sci. 2006;28:3. [Google Scholar]