

Abstract
Context:
Psychological comorbidities are prevalent in coal miners with chronic obstructive pulmonary disease (COPD) and contribute to the severity of the disease reducing their health status. Yoga has been shown to alleviate depression and anxiety associated with other chronic diseases but in COPD not been fully investigated.
Aim:
This study aimed to evaluate the role of yoga on health status, depression, and anxiety in coal miners with COPD.
Materials and Methods:
This was a randomized trial with two study arms (yoga and control), which enrolled 81 coal miners, ranging from 36 to 60 years with stage II and III stable COPD. Both groups were either on conventional treatment or combination of conventional care with yoga program for 12 weeks.
Results:
Data were collected through standardized questionnaires; COPD Assessment Test, Beck Depression Inventory and State and Trait Anxiety Inventory at the beginning and the end of the intervention. The yoga group showed statistically significant (P < 0.001) improvements on all scales within the group, all significantly different (P < 0.001) from changes observed in the controls. No significant prepost changes were observed in the control group (P > 0.05).
Conclusion:
Yoga program led to greater improvement in physical and mental health status than did conventional care. Yoga seems to be a safe, feasible, and effective treatment for patients with COPD. There is a need to conduct more comprehensive, high-quality, evidence-based studies to shed light on the current understanding of the efficacy of yoga in these chronic conditions and identify unanswered questions.
Keywords: Anxiety, COPD assessment test, chronic obstructive pulmonary disease, depression, yoga
INTRODUCTION
Chronic obstructive pulmonary disease (COPD) is a complex, treatment-resistant disease with multiple comorbidities, depression, and anxiety being the two of the most important and least treated among them.[1] Other than cigarette smoking, there is an increasing evidence of occupational exposures as a major risk factor for COPD[2,3] found the prevalence of COPD in nonsmoking coal miners was 19% in a study. Depression and anxiety increasingly affect the psychological well-being of working populations,[4] coal miners being more susceptible due to highly risky and stressful working environments.[5] Prior studies have documented association of depression and anxiety among COPD patients[6,7,8,9] more than non-COPD individuals.[10] Clinically significant symptoms of depression were found in around half COPD patients[11,12] while the prevalence of anxiety has been estimated at 40%.[13,14,15] About one-third of COPD sufferers is afflicted by both.[16] The presence of these comorbid symptoms significantly contributes to the impaired health status in patients with COPD[17,18] irrespective of the degree of airflow limitation.[19] Therefore, optimizing the health status is an important goal in COPD management.[20] In a systematic review, it has been reported that comprehensive pulmonary rehabilitation benefits in a reduction in short-term depression and anxiety.[21] Limited evidence is available on the effect of mindfulness-based treatments such as yoga for the management of depression and anxiety in COPD patients.
Yoga is a way of life, mainly has four primary components: Physical postures to develop strength and flexibility, breathing exercises to enhance respiratory functioning, deep relaxation techniques to cultivate the ability to release anxiety, and meditation/mindfulness practices to promote emotion and stress regulation skills.[22] Psychosomatic ailments arise due to a disturbance in the mind.[23] The level of documented evidence of yoga's psychophysiological benefits for depression and anxiety is progressively increasing.[24,25,26,27,28,29,30,31,32] Similarly, some research has been conducted on yoga's application to COPD[33,34,35,36,37] but no study has been published assessing the effect of yoga on coal miners, for whom the condition is a major work-related health hazard. Hence, this study was aimed to evaluate the effects of a 12 weeks program of the Integrated Approach of Yoga Therapy (IAYT) on health status, depression, and anxiety of COPD in coal miners compared to controls on conventional care, based on the hypothesis that it would improve the health status by decreasing depression and anxiety symptoms. IAYT is a combination of breathing practices, physical postures, pranayama, kriya, meditation, relaxation techniques, and lectures.[22] Its therapeutic applications as a supplementary therapy for chronic health conditions in asthma,[38] cancer,[39] diabetes,[40] schizophrenia,[41] and low back pain[42] are well established.
MATERIALS AND METHODS
Participants
Eighty-one male nonsmoking coal miners with ages ranging from 36 years to 60 years were recruited for the study. They were all present coal miners of Rampur Colliery, Odisha. A total of 279 coal miners were screened, of whom 36 declined to sign the informed consent form. Rest 243 underwent clinical examination, of these 162 met any one of exclusion criteria and finally 81 registered for the trial and were randomized into two groups, yoga and waitlist controls. Figure 1 depicts the flow diagram of the study, showing screening, enrollment, intervention, assessments, and analysis.
Figure 1.

Flow of participants over study period
Inclusion criteria
The inclusion criteria were as follows: Physician diagnosed COPD with spirometric evidence of chronic airflow limitation (forced expiratory volume in 1 s/forced vital capacity, post bronchodilator <0.70), Global initiative for Obstructive Lung Disease (GOLD) stage I and II COPD;[1] clinically stable for at least 3 months; literate to complete the questionnaires.
Exclusion criteria
Exclusion criteria were: Prior experience of yoga; recent COPD exacerbation; cognitive impairment; myocardial infarction or recurrent angina within the previous 6 months; hospitalization within 3 months; and respiratory tract infection within 1 month of enrollment.
Informed consent
The aim of the study was conveyed to those agreeing to participate in the study; signed informed consent was obtained from all participants prior to baseline assessment.
Design
This is a randomized, waitlist control, single-blind clinical trial in which 81 participants were assigned to two groups (yoga and control) using a computer generated random number table obtained from http://www.randomizer.org. Numbered opaque envelopes were used to implement the random allocation to conceal the sequence until interventions were assigned.
Study protocol
At enrollment, medical, exposure histories, pulmonary symptoms, and information about current pharmacological treatments were obtained, and clinical examinations performed by a specialist physician. Comorbid diagnoses were established from clinical histories and examination findings, supported by reviews of available medical records. The yoga group practiced a set of integrated yoga practices specially designed for COPD for 90 min daily, 6 days/week for 12 weeks. Participants of control group continued conventional therapy, completing all assessments at the same times as the yoga group; they were offered yoga at the end of the study. All participants were asked to refrain from participating in any other yoga classes during the study period.
Blinding and masking
Double blinding is not considered possible for yoga interventions, where participants and trainer can recognize group assignment. However, giving and scoring the assessments were masked wherever feasible. The statistician responsible for randomization, and subsequent data analysis was not involved in administering the intervention and was thus blind to the source of the data. The clinical psychologist who administered and scored the psychological questionnaires and the staff, who carried out assessments, were blind to membership of the intervention groups. Coded answer sheets were analyzed only after the study's completion.
Study approval
The study was approved by the Institution Ethics Committee (Swami Vivekananda Yoga University, Bangalore) through RES/IEC/28/2014 in accordance with the Helsinki Declaration.
Intervention
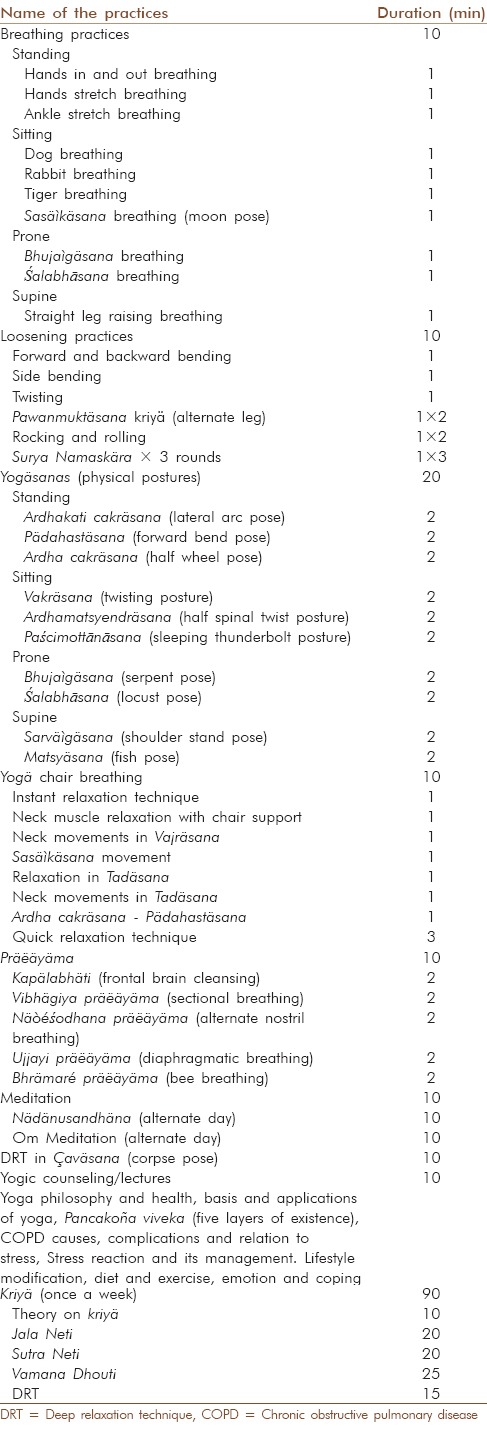
The IAYT module was developed by Swami Vivekananda Yoga Anusandhana Samasthana specifically for COPD. It included simple and safe practices at physical, mental, emotional, and intellectual levels. The yoga practice protocol was designed in consultation with S-VYASA's Medical Director. The daily schedule is detailed in Table 1.
Table 1.
Integrated approach of yoga therapy for chronic obstructive pulmonary disease used in this study
Assessments
Assessments were made on both groups before and after the 12 weeks of intervention. The following questionnaires were completed by all participants.
COPD assessment test
COPD Assessment Test (CAT) is a short questionnaire developed for assessing and monitoring COPD in routine clinical practice. It provides a valid, reliable, and standardized measure of the impact of COPD on a patient's health and well-being.[43,44] It consists of 8 items rated using a Likert-type scale of 0–5, providing a score out of 40, higher scores representing the poorer quality of life (QoL). Despite the small number of items, it covers a broad range of effects on patients’ health. It takes less time to complete than other health-related QoL questionnaires.[45] CAT is sensitive to changes in disease progression over time and to the effectiveness of treatments.[46,47] Internal consistency is excellent with Cronbach's α =0.88 and test-retest reliability good in stable patients (ICCC = 0. 8).[43]
Beck depression inventory
All participants completed the Beck Depression Inventory (BDI), 2nd edition.[48] BDI-II is a self-report questionnaire of 21 items scored from 0 to 3. It is designed to assess depressive symptoms experienced within the previous 2 weeks. It has high internal consistency (Cronbach's α =0.92); mean test-retest reliability is 0.72.[49] BDI-II scores range from 0 to 63, with categorical depression ratings of “minimal” (0–13), “mild” (14–19), “moderate” (20–28), and “severe” (29–63). BDI is considered a valid measure of depressed mood for diverse populations.
State trait anxiety inventory
State and Trait Anxiety Inventory (STAI) is a reliable, valid, and widely used measure of anxiety for clinical practice and research, with a high degree of internal consistency.[50] Cronbach's α is 0.85 for the total scores.[51] It includes separate measures of state anxiety and trait anxiety each comprising 20 items rated on a 4 point scale from 0 to 3 which range from 20, minimum, to 80, maximum. Form S evaluates state anxiety, how subjects, feel “at this moment;” while Form T assesses trait anxiety, how the respondent feels “most of the time.” In India, its reliability and validity are well established following extensive use in adult populations. State anxiety reflects subjective and transitory emotional states characterized by consciously perceived feelings of nervousness, tension, worries, and apprehension, and heightened autonomic nervous system activity. In contrast, trait anxiety refers to relatively stable individual differences in anxiety proneness as a personality attribute that denotes general tendency to respond with anxiety to perceived threats in the environment.
Data collection
Clinical and demographic information were collected using medical records and study-specific forms. Adherence and compliance were monitored through the use of daily patient diaries and attendance records kept by the yoga instructors. No make-up sessions were provided for missed classes. All participants were instructed to continue their routine daily activities during the 12-week intervention period but were asked not to start a new yoga or exercise regimen on their own during that time. A feedback form was used to assess enjoyment and helpfulness of the yoga intervention, and to ask whether participants would recommend it to others.
Statistical analysis
Data were analyzed using SPSS version 18.0 (IBM Corporation, USA). Within group changes and between group treatment effects associated with participation in the yoga intervention were evaluated using Chi-square tests for categorical data and paired t-tests and independent sample t-tests for continuous data. P < 0.05 was considered significant.
RESULTS
Descriptive features
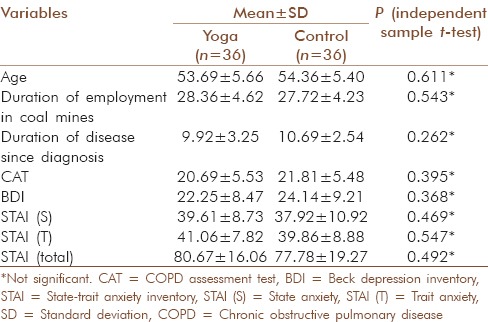
The study population initially consisted of 81 coal miners with COPD. Five and four participants dropped out of yoga and control group, respectively, for personal reasons unrelated to the study, giving a final sample size of 72 (36 in each group). Total participants in GOLD stage II category were 52.8% in yoga and 58.3% in controls, and in GOLD stage III 47.2% in yoga and 41.7% in controls. Demographic variables of patient's average age, duration of employment in coal mines, and duration of disease since diagnosis were comparable as were initial test scores at baseline (all P > 0.05) [Table 2].
Table 2.
Baseline characteristics of participants in both yoga and control group
COPD assessment test
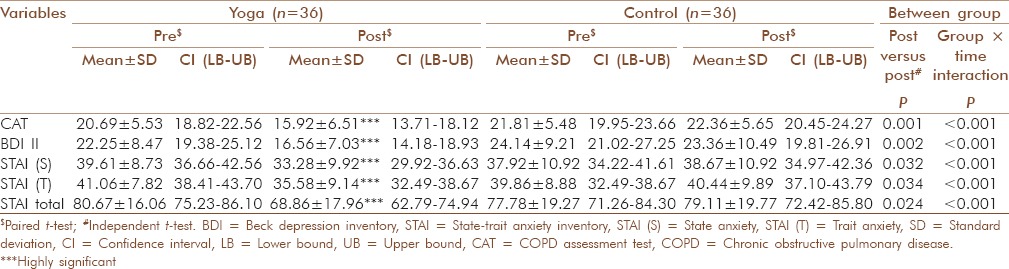
The practice of yoga for 12 weeks has significantly lowered the CAT scores (P < 0.001) in the yoga group, indicating better health status, whereas no significant difference was observed in the control group (P = 0.294). The results further revealed that the change occurred in the yoga group was 23.05% and in the control group was − 2.52%. Between-group differences were statistically significant (P < 0.001, independent t-test) [Table 3].
Table 3.
Change scores within yoga and control, and difference between groups with 95% CI
Beck depression inventory
In both the groups, mean depression scores were reduced, but the magnitude of change is statistically significant and higher (P < 0.001, 25.53%) in the yoga group as compared to the control group (P = 0.095, 3.23%). In addition, significant group mean differences were observed between yoga and control group's post intervention scores (P = 0.002) [Table 3].
State and trait anxiety inventory
The yoga group showed significantly lower scores in both state and trait anxiety (P < 0.001), but controls showed no significant change (P = 0.192 and P = 0.383, respectively). State anxiety decreased by 15.98% in yoga and increased by 1.98% in controls. A similar trend was observed in trait anxiety also. It decreased by 13.35% in yoga and increased by 1.46% in controls. Independent t-tests gave statistically significant differences between groups at posttest, P = 0.032 and P = 0.034, respectively. Overall anxiety score was significantly reduced by 14.64% within the yoga group (P < 0.001), whereas and there was slight increase by 1.71% (P = 0.054) reported in the control group [Table 3].
DISCUSSION
To the best of our knowledge, this is the first randomized-controlled study investigating physical and psychological health benefits associated with yoga practice on coal miners with COPD. The study evaluated the impact of yoga on their disease-specific health status, depression, and anxiety levels. Results suggested that IAYT practice facilitates improvements in health status and reduces self-reported depression and anxiety levels after 12 weeks of practice.
The results are consistent with previously reported interventions based on yoga, which demonstrated positive, beneficial effects on psychological and psychosocial factors in diverse conditions such as diabetes,[40] cancer,[52] CAD,[53] low back pain,[54] osteoarthritis of the knee,[55] and pregnancy.[56,57] It is reported in a study that pranayama (yogic breathing) mitigates posttraumatic stress disorder and depression.[58] Another study on patients who participated in education and stress management in addition to exercise training during a 12-week intervention reported reductions in depression and anxiety.[59]
A study reported that changes in depression and state and trait anxiety did not significantly differ between the two interventions (6 weeks of weekly yoga classes together with exercise, compared to a 6 weeks weekly group exercise) (GDS15, P = 0.749, STAI-S, P = 0.595, STAI-T, P = 0.407).[60] Another study has similarly obtained unclear effects following yoga intervention.[61]
The pathophysiology of depression and anxiety among COPD patient is complex and poorly understood. The physical, emotional, and social impact of COPD may cause a self-perpetuating cycle that has a severe impact on a patient's physical and mental health status.[21] It has been shown that high scores on perceived stress and anxiety are related to increase in hypothalamic-pituitary-adrenal (HPA) axis activity.[62] The effects of yoga in our results can be explained by reduction in levels of psychophysiological arousal via triggering neurohormonal mechanisms that suppress sympathetic activity,[63,64] balance in the autonomic nervous system responses,[65] alterations in neuroendocrine arousal[66,67] through better regulation of the HPA axis[68] resulting in reductions in stress and anxiety.[32] Better psychological health resulting from stress reduction might be due to relaxation techniques[69] which contribute to the observed improvements in CAT scores in our study. Thus, these psychological changes may explain the physiological changes observed as better outcomes seen in previous studies on integrated yoga in asthma.[38] Yoga unites body, mind, and spirit; and enhances attention by calming down the restless mind.[22] Thus, the deep physiological rest that is achieved by the components of pranayama, meditation, and other mindfulness practices incorporated in the integrated yoga program could be the major factors explaining observed benefits. Overall, antidepressant effects of yoga programs can be attributed to stress reduction.[70] Another study concluded the practice of meditation strengthens the mental resolve and hence decreases anxiety.[71] Yoga practices decrease parasympathetic nervous system and GABAergic activity that underlies stress-related disorders which result in amelioration of disease symptoms.[72] Reductions in psychological hyper-reactivity and emotional instability achieved by yoga may be due to reduced efferent vagal reactivity[73] already recognized as a main psychosomatic factor in asthma,[74] might have similar physiology in COPD also.
This study is the first of its kind to conclude that integrated yoga can act as an imperative line of therapy in the management of COPD in coal miners. The novel aspects of this study were (a) the randomized control design, (b) good sample size, (c) incorporation of integrated yoga approach, and (d) good compliance. A major constraint of the study is the lack of an active control group. It would have been valuable to include physiological measures of stress such as Galvanic Skin Response and Heart Rate Variability to overcome the subjectivity of self-report and to throw light on the mechanisms. In spite of the aforementioned limitations, significant results were manifested in a short time suggesting yoga therapy could be a non-pharmacological alternative for the management of COPD. The current state of understanding necessitates further assessment to evaluate benefits of yoga for COPD in diverse populations, especially associated with depression and anxiety followed over longer time periods. Robust effectiveness and implementation studies are required to determine whether yoga therapy can decrease medical utilization. In addition, the findings of this study may also provide evidence supporting the incorporation of yoga into standardized pulmonary rehabilitation programs as a practical adjunct to improve the management of psychosocial symptoms associated with COPD.
CONCLUSION
In this study, 12 weeks of integrated yoga enhanced health status and reduced depression and anxiety in coal miners with COPD. Any system that can bring symptomatic relief and improve different aspects of QoL of COPD patients merits incorporation into standard COPD treatments. Further research is warranted to confirm these preliminary findings and facilitate implementation in clinical settings.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
The authors would like to express gratitude Mr. Rajeev Lochan and Soubhagyalaxmi Mohanty for assisting with manuscript preparation. Thanks are due to Mr. Kunja Bihari Badhai, senior yoga instructor for his experienced support and advice. Also to Mr. Arjun Biswal for coordinating the program. Special thanks to Dr. R Nagarathna, who offered critical and thoughtful recommendations in the initial development of the program and Dr. Balaram Pradhan, Ph.D. for statistical analysis.
REFERENCES
- 1.GOLD. Global Strategy for the Diagnosis, Management and Prevention of Chronic Obstructive Pulmonary Disease. Global Initiative for Chronic Obstructive Lung Disease; 2015. [Last accessed on 2015 Mar 09]. Available from: http://www.goldcopd.org/uploads/users/files/GOLD_Report_2015.pdf .
- 2.Hu Y, Chen B, Yin Z, Jia L, Zhou Y, Jin T. Increased risk of chronic obstructive pulmonary diseases in coke oven workers: Interaction between occupational exposure and smoking. Thorax. 2006;61:290–5. doi: 10.1136/thx.2005.051524. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Yasin M, Beatty B, Folz RJ. Depression, COPD and Coal Worker's Pneumoconiosis (CWP) are common among kentucky coal miners evaluated for respiratory impairment. Am J Respir Crit Care Med. 2015;191:A4683. [Google Scholar]
- 4.Fan LB, Blumenthal JA, Watkins LL, Sherwood A. Work and home stress: Associations with anxiety and depression symptoms. Occup Med (Lond) 2015;65:110–6. doi: 10.1093/occmed/kqu181. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Liu L, Wang L, Chen J. Prevalence and associated factors of depressive symptoms among Chinese underground coal miners. Biomed Res Int 2014. 2014:987305. doi: 10.1155/2014/987305. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Laurin C, Lavoie KL, Bacon SL, Dupuis G, Lacoste G, Cartier A, et al. Sex differences in the prevalence of psychiatric disorders and psychological distress in patients with COPD. Chest. 2007;132:148–55. doi: 10.1378/chest.07-0134. [DOI] [PubMed] [Google Scholar]
- 7.Eisner MD, Blanc PD, Yelin EH, Katz PP, Sanchez G, Iribarren C, et al. Influence of anxiety on health outcomes in COPD. Thorax. 2010;65:229–34. doi: 10.1136/thx.2009.126201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Johansson R, Carlbring P, Heedman Å, Paxling B, Andersson G. Depression, anxiety and their comorbidity in the Swedish general population: Point prevalence and the effect on health-related quality of life. PeerJ. 2013;1:e98. doi: 10.7717/peerj.98. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Giardino ND, Curtis JL, Andrei AC, Fan VS, Benditt JO, Lyubkin M, et al. Anxiety is associated with diminished exercise performance and quality of life in severe emphysema: A cross-sectional study. Respir Res. 2010;11:29. doi: 10.1186/1465-9921-11-29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Felker B, Bush KR, Harel O, Shofer JB, Shores MM, Au DH. Added burden of mental disorders on health status among patients with chronic obstructive pulmonary disease. Prim Care Companion J Clin Psychiatry. 2010;12 doi: 10.4088/PCC.09m00858gry. pii: PCC.09m00858. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Yohannes AM, Baldwin RC, Connolly MJ. Depression and anxiety in elderly outpatients with chronic obstructive pulmonary disease: Prevalence, and validation of the BASDEC screening questionnaire. Int J Geriatr Psychiatry. 2000;15:1090–6. doi: 10.1002/1099-1166(200012)15:12<1090::aid-gps249>3.0.co;2-l. [DOI] [PubMed] [Google Scholar]
- 12.Lacasse Y, Rousseau L, Maltais F. Prevalence of depressive symptoms and depression in patients with severe oxygen-dependent chronic obstructive pulmonary disease. J Cardiopulm Rehabil. 2001;21:80–6. doi: 10.1097/00008483-200103000-00004. [DOI] [PubMed] [Google Scholar]
- 13.Kunik ME, Roundy K, Veazey C, Souchek J, Richardson P, Wray NP, et al. Surprisingly high prevalence of anxiety and depression in chronic breathing disorders. Chest. 2005;127:1205–11. doi: 10.1378/chest.127.4.1205. [DOI] [PubMed] [Google Scholar]
- 14.Yohannes AM, Willgoss TG, Baldwin RC, Connolly MJ. Depression and anxiety in chronic heart failure and chronic obstructive pulmonary disease: Prevalence, relevance, clinical implications and management principles. Int J Geriatr Psychiatry. 2010;25:1209–21. doi: 10.1002/gps.2463. [DOI] [PubMed] [Google Scholar]
- 15.Willgoss TG, Yohannes AM. Anxiety disorders in patients with COPD: A systematic review. Respir Care. 2013;58:858–66. doi: 10.4187/respcare.01862. [DOI] [PubMed] [Google Scholar]
- 16.Panagioti M, Scott C, Blakemore A, Coventry PA. Overview of the prevalence, impact, and management of depression and anxiety in chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2014;9:1289–306. doi: 10.2147/COPD.S72073. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Ng TP, Niti M, Tan WC, Cao Z, Ong KC, Eng P. Depressive symptoms and chronic obstructive pulmonary disease: Effect on mortality, hospital readmission, symptom burden, functional status, and quality of life. Arch Intern Med. 2007;167:60–7. doi: 10.1001/archinte.167.1.60. [DOI] [PubMed] [Google Scholar]
- 18.Gudmundsson G, Gislason T, Janson C, Lindberg E, Hallin R, Ulrik CS, et al. Risk factors for rehospitalisation in COPD: Role of health status, anxiety and depression. Eur Respir J. 2005;26:414–9. doi: 10.1183/09031936.05.00078504. [DOI] [PubMed] [Google Scholar]
- 19.Agusti A, Calverley PM, Celli B, Coxson HO, Edwards LD, Lomas DA, et al. Characterisation of COPD heterogeneity in the ECLIPSE cohort. Respir Res. 2010;11:122. doi: 10.1186/1465-9921-11-122. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Vestbo J, Hurd SS, Agustí AG, Jones PW, Vogelmeier C, Anzueto A, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2013;187:347–65. doi: 10.1164/rccm.201204-0596PP. [DOI] [PubMed] [Google Scholar]
- 21.Pumar MI, Gray CR, Walsh JR, Yang IA, Rolls TA, Ward DL. Anxiety and depression-Important psychological comorbidities of COPD. J Thorac Dis. 2014;6:1615–31. doi: 10.3978/j.issn.2072-1439.2014.09.28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Nagarathna R, Nagendra HR. 2nd ed. Bangalore: Swami Vivekananda Yoga Prakashan; 2013. Integrated Approach of Yoga Therapy for Positive Health. [Google Scholar]
- 23.Rajesh SK, Ilavarasu JV, Srinivasan TM, Nagendra HR. Stress and its expression according to contemporary science and ancient indian wisdom: Perseverative cognition and the pañca kosas. Mens Sana Monogr. 2014;12:139–52. doi: 10.4103/0973-1229.130323. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Shapiro D, Cook IA, Davydov DM, Ottaviani C, Leuchter AF, Abrams M. Yoga as a complementary treatment of depression: Effects of traits and moods on treatment outcome. Evid Based Complement Alternat Med. 2007;4:493–502. doi: 10.1093/ecam/nel114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Davis K, Goodman SH, Leiferman J, Taylor M, Dimidjian S. A randomized controlled trial of yoga for pregnant women with symptoms of depression and anxiety. Complement Ther Clin Pract. 2015;21:166–72. doi: 10.1016/j.ctcp.2015.06.005. [DOI] [PubMed] [Google Scholar]
- 26.Duan-Porter W, Coeytaux RR, McDuffie J, Goode A, Sharma P, Mennella H, et al. EEvidence map of yoga for depression, anxiety and post-traumatic stress disorder. J Phys Act Health. 2015 doi: 10.1123/jpah.2015-0027. Epub ahead of print. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Doria S, de Vuono A, Sanlorenzo R, Irtelli F, Mencacci C. Anti-anxiety efficacy of Sudarshan Kriya Yoga in general anxiety disorder: A multicomponent, yoga based, breath intervention program for patients suffering from generalized anxiety disorder with or without comorbidities. J Affect Disord. 2015;184:310–7. doi: 10.1016/j.jad.2015.06.011. [DOI] [PubMed] [Google Scholar]
- 28.Jacquart J, Miller KM, Radossi A, Haime V, Macklin E, Gilburd D, et al. The effectiveness of a community-based, mind-body group for symptoms of depression and anxiety. Adv Mind Body Med. 2014;28:6–13. [PubMed] [Google Scholar]
- 29.Forfylow AL. Integrating yoga with psychotherapy: A complimentary treatment for anxiety and depression. Can J Couns Psychother. 2011;45:132–50. [Google Scholar]
- 30.Uebelacker LA, Epstein-Lubow G, Gaudiano BA, Tremont G, Battle CL, Miller IW. Hatha yoga for depression: Critical review of the evidence for efficacy, plausible mechanisms of action, and directions for future research. J Psychiatr Pract. 2010;16:22–33. doi: 10.1097/01.pra.0000367775.88388.96. [DOI] [PubMed] [Google Scholar]
- 31.Telles S, Gaur V, Balkrishna A. Effect of a yoga practice session and a yoga theory session on state anxiety. Percept Mot Skills. 2009;109:924–30. doi: 10.2466/pms.109.3.924-930. [DOI] [PubMed] [Google Scholar]
- 32.Hoge EA, Bui E, Marques L, Metcalf CA, Morris LK, Robinaugh DJ, et al. Randomized controlled trial of mindfulness meditation for generalized anxiety disorder: Effects on anxiety and stress reactivity. J Clin Psychiatry. 2013;74:786–92. doi: 10.4088/JCP.12m08083. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Desveaux L, Lee A, Goldstein R, Brooks D. Yoga in the management of chronic disease: A systematic review and meta-analysis. Med Care. 2015;53:653–61. doi: 10.1097/MLR.0000000000000372. [DOI] [PubMed] [Google Scholar]
- 34.Donesky-Cuenco D, Nguyen HQ, Paul S, Carrieri-Kohlman V. Yoga therapy decreases dyspnea-related distress and improves functional performance in people with chronic obstructive pulmonary disease: A pilot study. J Altern Complement Med. 2009;15:225–34. doi: 10.1089/acm.2008.0389. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Fulambarker A, Farooki B, Kheir F, Copur AS, Srinivasan L, Schultz S. Effect of yoga in chronic obstructive pulmonary disease. Am J Ther. 2012;19:96–100. doi: 10.1097/MJT.0b013e3181f2ab86. [DOI] [PubMed] [Google Scholar]
- 36.Santana MJ, S-Parrilla J, Mirus J, Loadman M, Lien DC, Feeny D. An assessment of the effects of Iyengar yoga practice on the health-related quality of life of patients with chronic respiratory diseases: A pilot study. Can Respir J. 2013;20:e17–23. doi: 10.1155/2013/265406. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Soni R, Munish K, Singh K, Singh S. Study of the effect of yoga training on diffusion capacity in chronic obstructive pulmonary disease patients: A controlled trial. Int J Yoga. 2012;5:123–7. doi: 10.4103/0973-6131.98230. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Nagarathna R, Nagendra HR. Yoga for bronchial asthma: A controlled study. Br Med J (Clin Res Ed) 1985;291:1077–9. doi: 10.1136/bmj.291.6502.1077. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Chandwani KD, Perkins G, Nagendra HR, Raghuram NV, Spelman A, Nagarathna R, et al. Randomized, controlled trial of yoga in women with breast cancer undergoing radiotherapy. J Clin Oncol. 2014;32:1058–65. doi: 10.1200/JCO.2012.48.2752. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.McDermott KA, Rao MR, Nagarathna R, Murphy EJ, Burke A, Nagendra RH, et al. Ayoga intervention for type 2 diabetes risk reduction: A pilot randomized controlled trial. BMC Complement Altern Med. 2014;14:212. doi: 10.1186/1472-6882-14-212. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Duraiswamy G, Thirthalli J, Nagendra HR, Gangadhar BN. Yoga therapy as an add-on treatment in the management of patients with schizophrenia – A randomized controlled trial. Acta Psychiatr Scand. 2007;116:226–32. doi: 10.1111/j.1600-0447.2007.01032.x. [DOI] [PubMed] [Google Scholar]
- 42.Tekur P, Chametcha S, Hongasandra RN, Raghuram N. Effect of yoga on quality of life of CLBP patients: A randomized control study. Int J Yoga. 2010;3:10–7. doi: 10.4103/0973-6131.66773. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Jones PW, Harding G, Berry P, Wiklund I, Chen WH, Kline Leidy N. Development and first validation of the COPD Assessment Test. Eur Respir J. 2009;34:648–54. doi: 10.1183/09031936.00102509. [DOI] [PubMed] [Google Scholar]
- 44.Jones PW, Brusselle G, Dal Negro RW, Ferrer M, Kardos P, Levy ML, et al. Properties of the COPD assessment test in a cross-sectional European study. Eur Respir J. 2011;38:29–35. doi: 10.1183/09031936.00177210. [DOI] [PubMed] [Google Scholar]
- 45.Ringbaek T, Martinez G, Lange P. A comparison of the assessment of quality of life with CAT, CCQ, and SGRQ in COPD patients participating in pulmonary rehabilitation. COPD. 2012;9:12–5. doi: 10.3109/15412555.2011.630248. [DOI] [PubMed] [Google Scholar]
- 46.Mackay AJ, Donaldson GC, Patel AR, Jones PW, Hurst JR, Wedzicha JA. Usefulness of the chronic obstructive pulmonary disease assessment test to evaluate severity of COPD exacerbations. Am J Respir Crit Care Med. 2012;185:1218–24. doi: 10.1164/rccm.201110-1843OC. [DOI] [PubMed] [Google Scholar]
- 47.Dodd JW, Hogg L, Nolan J, Jefford H, Grant A, Lord VM, et al. The COPD assessment test (CAT): Response to pulmonary rehabilitation. A multicentre, prospective study. Thorax. 2011;66:425–9. doi: 10.1136/thx.2010.156372. [DOI] [PubMed] [Google Scholar]
- 48.Beck AT, Steer RA, Brown GK. San Antonio, TX: Psychological Corporation; 1996. Manual for the beck depression inventory-II. [Google Scholar]
- 49.Dozois DJ, Covin R. The Beck Depression Inventory. II (BDI-II), Beck Hopelessness Scale (BHS), and Beck Scale for Suicide Ideation (BSS) In: Hersen M, Hilsenroth MJ, Segal DL, editors. Comprehensive Handbook of Psychological Assessment. Personality Assessment and Psychopathology. New York: John Wiley & Sons Inc; 2004. pp. 50–69. [Google Scholar]
- 50.Spielberger CD, Gorsuch RL, Lushene RE. Palo Alto, CA: Consulting Psychologists; 1970. The State-Trait Anxiety Inventory (Test Manual) [Google Scholar]
- 51.Vitasari P, Wahab MN, Herawan T, Othman A, Sinnadurai SK. Re-test of State Trait Anxiety Inventory (STAI) among engineering students in Malaysia: Reliability and validity tests. Procedia Soc Behav Sci. 2011;15:3843–8. [Google Scholar]
- 52.Rao RM, Raghuram N, Nagendra HR, Usharani MR, Gopinath KS, Diwakar RB, et al. Effects of an integrated yoga program on self-reported depression scores in breast cancer patients undergoing conventional treatment: A randomized controlled trial. Indian J Palliat Care. 2015;21:174–81. doi: 10.4103/0973-1075.156486. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Raghuram N, Parachuri VR, Swarnagowri MV, Babu S, Chaku R, Kulkarni R, et al. Yoga based cardiac rehabilitation after coronary artery bypass surgery: One-year results on LVEF, lipid profile and psychological states – A randomized controlled study. Indian Heart J. 2014;66:490–502. doi: 10.1016/j.ihj.2014.08.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Tekur P, Nagarathna R, Chametcha S, Hankey A, Nagendra HR. A comprehensive yoga programs improves pain, anxiety and depression in chronic low back pain patients more than exercise: An RCT. Complement Ther Med. 2012;20:107–18. doi: 10.1016/j.ctim.2011.12.009. [DOI] [PubMed] [Google Scholar]
- 55.Ebnezar J, Nagarathna R, Yogitha B, Nagendra HR. Effect of integrated yoga therapy on pain, morning stiffness and anxiety in osteoarthritis of the knee joint: A randomized control study. Int J Yoga. 2012;5:28–36. doi: 10.4103/0973-6131.91708. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Satyapriya M, Nagarathna R, Padmalatha V, Nagendra HR. Effect of integrated yoga on anxiety, depression & well being in normal pregnancy. Complement Ther Clin Pract. 2013;19:230–6. doi: 10.1016/j.ctcp.2013.06.003. [DOI] [PubMed] [Google Scholar]
- 57.Newham JJ, Wittkowski A, Hurley J, Aplin JD, Westwood M. Effects of antenatal yoga on maternal anxiety and depression: A randomized controlled trial. Depress Anxiety. 2014;31:631–40. doi: 10.1002/da.22268. [DOI] [PubMed] [Google Scholar]
- 58.Descilo T, Vedamurtachar A, Gerbarg PL, Nagaraja D, Gangadhar BN, Damodaran B, et al. Effects of a yoga breath intervention alone and in combination with an exposure therapy for post-traumatic stress disorder and depression in survivors of the 2004 South-East Asia tsunami. Acta Psychiatr Scand. 2010;121:289–300. doi: 10.1111/j.1600-0447.2009.01466.x. [DOI] [PubMed] [Google Scholar]
- 59.de Godoy DV, de Godoy RF. A randomized controlled trial of the effect of psychotherapy on anxiety and depression in chronic obstructive pulmonary disease. Arch Phys Med Rehabil. 2003;84:1154–7. doi: 10.1016/s0003-9993(03)00239-9. [DOI] [PubMed] [Google Scholar]
- 60.Chan W, Immink MA, Hillier S. Yoga and exercise for symptoms of depression and anxiety in people with poststroke disability: A randomized, controlled pilot trial. Altern Ther Health Med. 2012;18:34–43. [PubMed] [Google Scholar]
- 61.Kirkwood G, Rampes H, Tuffrey V, Richardson J, Pilkington K. Yoga for anxiety: A systematic review of the research evidence. Br J Sports Med. 2005;39:884–91. doi: 10.1136/bjsm.2005.018069. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.van Eck M, Berkhof H, Nicolson N, Sulon J. The effects of perceived stress, traits, mood states, and stressful daily events on salivary cortisol. Psychosom Med. 1996;58:447–58. doi: 10.1097/00006842-199609000-00007. [DOI] [PubMed] [Google Scholar]
- 63.Vempati RP, Telles S. Yoga-based guided relaxation reduces sympathetic activity judged from baseline levels. Psychol Rep. 2002;90:487–94. doi: 10.2466/pr0.2002.90.2.487. [DOI] [PubMed] [Google Scholar]
- 64.Ray US, Mukhopadhyaya S, Purkayastha SS, Asnani V, Tomer OS, Prashad R, et al. Effect of yogic exercises on physical and mental health of young fellowship course trainees. Indian J Physiol Pharmacol. 2001;45:37–53. [PubMed] [Google Scholar]
- 65.Telles S, Nagarathna R, Nagendra HR, Desiraju T. Physiological changes in sports teachers following 3 months of training in Yoga. Indian J Med Sci. 1993;47:235–8. [PubMed] [Google Scholar]
- 66.Harte JL, Eifert GH, Smith R. The effects of running and meditation on beta-endorphin, corticotropin-releasing hormone and cortisol in plasma, and on mood. Biol Psychol. 1995;40:251–65. doi: 10.1016/0301-0511(95)05118-t. [DOI] [PubMed] [Google Scholar]
- 67.West J, Otte C, Geher K, Johnson J, Mohr DC. Effects of Hatha yoga and African dance on perceived stress, affect, and salivary cortisol. Ann Behav Med. 2004;28:114–8. doi: 10.1207/s15324796abm2802_6. [DOI] [PubMed] [Google Scholar]
- 68.Pascoe MC, Bauer IE. A systematic review of randomised control trials on the effects of yoga on stress measures and mood. J Psychiatr Res. 2015;68:270–82. doi: 10.1016/j.jpsychires.2015.07.013. [DOI] [PubMed] [Google Scholar]
- 69.Manzoni GM, Pagnini F, Castelnuovo G, Molinari E. Relaxation training for anxiety: A ten-years systematic review with meta-analysis. BMC Psychiatry. 2008;8:41. doi: 10.1186/1471-244X-8-41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Deberry S, Davis S, Reinhard KE. A comparison of meditation-relaxation and cognitive/behavioral techniques for reducing anxiety and depression in a geriatric population. J Geriatr Psychiatry. 1989;22:231–47. [PubMed] [Google Scholar]
- 71.Telles S, Nagarathna R, Nagendra HR. Autonomic changes while mentally repeating two syllables – One meaningful and the other neutral. Indian J Physiol Pharmacol. 1998;42:57–63. [PubMed] [Google Scholar]
- 72.Streeter CC, Gerbarg PL, Saper RB, Ciraulo DA, Brown RP. Effects of yoga on the autonomic nervous system, gamma-aminobutyric-acid, and allostasis in epilepsy, depression, and post-traumatic stress disorder. Med Hypotheses. 2012;78:571–9. doi: 10.1016/j.mehy.2012.01.021. [DOI] [PubMed] [Google Scholar]
- 73.Raghuraj P, Ramakrishnan AG, Nagendra HR, Telles S. Effect of two selected yogic breathing techniques of heart rate variability. Indian J Physiol Pharmacol. 1998;42:467–72. [PubMed] [Google Scholar]
- 74.Nagendra HR, Nagarathna R. An integrated approach of yoga therapy for bronchial asthma: A 3-54-month prospective study. J Asthma. 1986;23:123–37. doi: 10.3109/02770908609077486. [DOI] [PubMed] [Google Scholar]