

Abstract
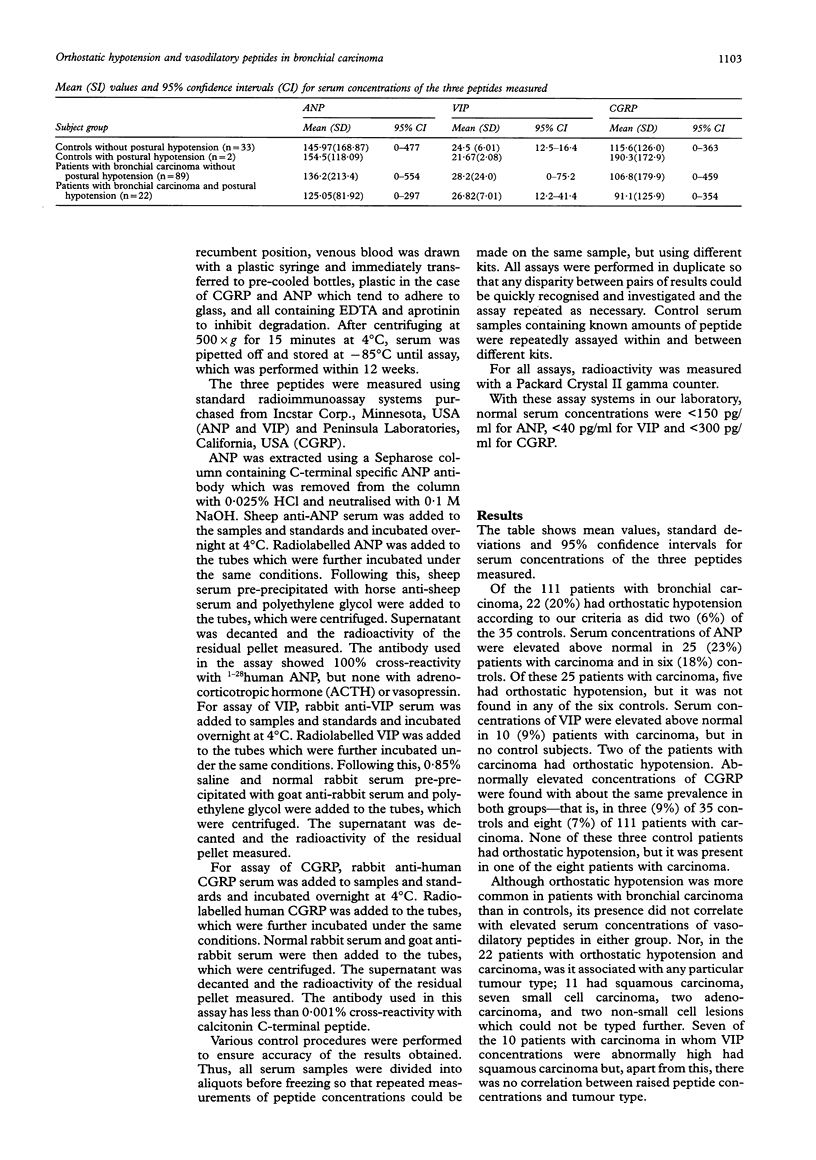
AIM--To determine whether inappropriately secreted vasodilatory peptides have a role in the pathogenesis of orthostatic (postural) hypotension, a recognised paraneoplastic effect of bronchial malignancies usually attributed to immune mediated destruction of autonomic ganglia. METHODS--Serum concentrations of three vasodilatory peptides, atrial natriuretic peptide (ANP), vasoactive intestinal polypeptide (VIP) and calcitonin gene related peptide (CGRP), were measured in 111 patients with bronchial carcinoma and 35 controls prospectively screened for orthostatic hypotension (> 20 mmHg drop in systolic blood pressure on repeated occasions on standing from the supine position) and in whom other causes of this condition were excluded. RESULTS--Twenty two (20%) patients with carcinoma and two (6%) controls had orthostatic hypotension according to the criteria used. Serum concentrations of ANP, VIP and CGRP were elevated above normal in, respectively, 25 (23%), 10 (9%) and eight (7%) patients with carcinoma and in six (18%), zero and three (9%) controls. There was no correlation between orthostatic hypotension and concentrations of any of the vasodilatory peptides. CONCLUSION--Elevated serum concentrations of ANP and CGRP were no more frequent in subjects with bronchial carcinoma than in controls and could not be attributed to the tumour, although there was a possible association for VIP. Orthostatic hypotension was more common in patients with carcinoma, but there was no evidence that the peptides measured played a role in its pathogenesis.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Bliss D. P., Jr, Battey J. F., Linnoila R. I., Birrer M. J., Gazdar A. F., Johnson B. E. Expression of the atrial natriuretic factor gene in small cell lung cancer tumors and tumor cell lines. J Natl Cancer Inst. 1990 Feb 21;82(4):305–310. doi: 10.1093/jnci/82.4.305. [DOI] [PubMed] [Google Scholar]
- Caird F. I., Andrews G. R., Kennedy R. D. Effect of posture on blood pressure in the elderly. Br Heart J. 1973 May;35(5):527–530. doi: 10.1136/hrt.35.5.527. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chinn J. S., Schuffler M. D. Paraneoplastic visceral neuropathy as a cause of severe gastrointestinal motor dysfunction. Gastroenterology. 1988 Nov;95(5):1279–1286. doi: 10.1016/0016-5085(88)90362-9. [DOI] [PubMed] [Google Scholar]
- Craig R. K., Edbrooke M. R., Riley J. H., McVey J. H., Parker D. Differential expression of the human calcitonin--CGRP gene in medullary thyroid carcinoma and lung carcinoma cell lines. Recent Results Cancer Res. 1985;99:71–78. doi: 10.1007/978-3-642-82533-0_8. [DOI] [PubMed] [Google Scholar]
- Fine W. Some common factors in the causation of postural hypotension. Gerontol Clin (Basel) 1969;11(4):206–215. doi: 10.1159/000245235. [DOI] [PubMed] [Google Scholar]
- Gould G. A., Ashworth M., Lewis G. T. Are cardiovascular reflexes more commonly impaired in patients with bronchial carcinoma? Thorax. 1986 May;41(5):372–375. doi: 10.1136/thx.41.5.372. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Manoogian C., Pandian M., Ehrlich L., Fisher D., Horton R. Plasma atrial natriuretic hormone levels in patients with the syndrome of inappropriate antidiuretic hormone secretion. J Clin Endocrinol Metab. 1988 Sep;67(3):571–575. doi: 10.1210/jcem-67-3-571. [DOI] [PubMed] [Google Scholar]
- Park D. M., Johnson R. H., Crean G. P., Robinson J. F. Orthostatic hypotension in bronchial carcinoma. Br Med J. 1972 Aug 26;3(5825):510–511. doi: 10.1136/bmj.3.5825.510. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Riley J. H., Edbrooke M. R., Craig R. K. Ectopic synthesis of high-Mr calcitonin by the BEN lung carcinoma cell line reflects aberrant proteolytic processing. FEBS Lett. 1986 Mar 17;198(1):71–79. doi: 10.1016/0014-5793(86)81187-5. [DOI] [PubMed] [Google Scholar]
- SIEMSEN J. K., MEISTER L. Bronchogenic carcinoma associated with severe orthostatic hypotension. Ann Intern Med. 1963 Apr;58:669–676. doi: 10.7326/0003-4819-58-4-669. [DOI] [PubMed] [Google Scholar]
- Said S. I., Faloona G. R. Elevated plasma and tissue levels of vasoactive intestinal polypeptide in the watery-diarrhea syndrome due to pancreatic, bronchogenic and other tumors. N Engl J Med. 1975 Jul 24;293(4):155–160. doi: 10.1056/NEJM197507242930401. [DOI] [PubMed] [Google Scholar]
- Schuffler M. D., Baird H. W., Fleming C. R., Bell C. E., Bouldin T. W., Malagelada J. R., McGill D. B., LeBauer S. M., Abrams M., Love J. Intestinal pseudo-obstruction as the presenting manifestation of small-cell carcinoma of the lung. A paraneoplastic neuropathy of the gastrointestinal tract. Ann Intern Med. 1983 Feb;98(2):129–134. doi: 10.7326/0003-4819-98-2-129. [DOI] [PubMed] [Google Scholar]
- Shimizu K., Nakano S., Nakano Y., Ando M., Seki K., Kameda N. Ectopic atrial natriuretic peptide production in small cell lung cancer with the syndrome of inappropriate antidiuretic hormone secretion. Cancer. 1991 Nov 15;68(10):2284–2288. doi: 10.1002/1097-0142(19911115)68:10<2284::aid-cncr2820681030>3.0.co;2-z. [DOI] [PubMed] [Google Scholar]