

Abstract
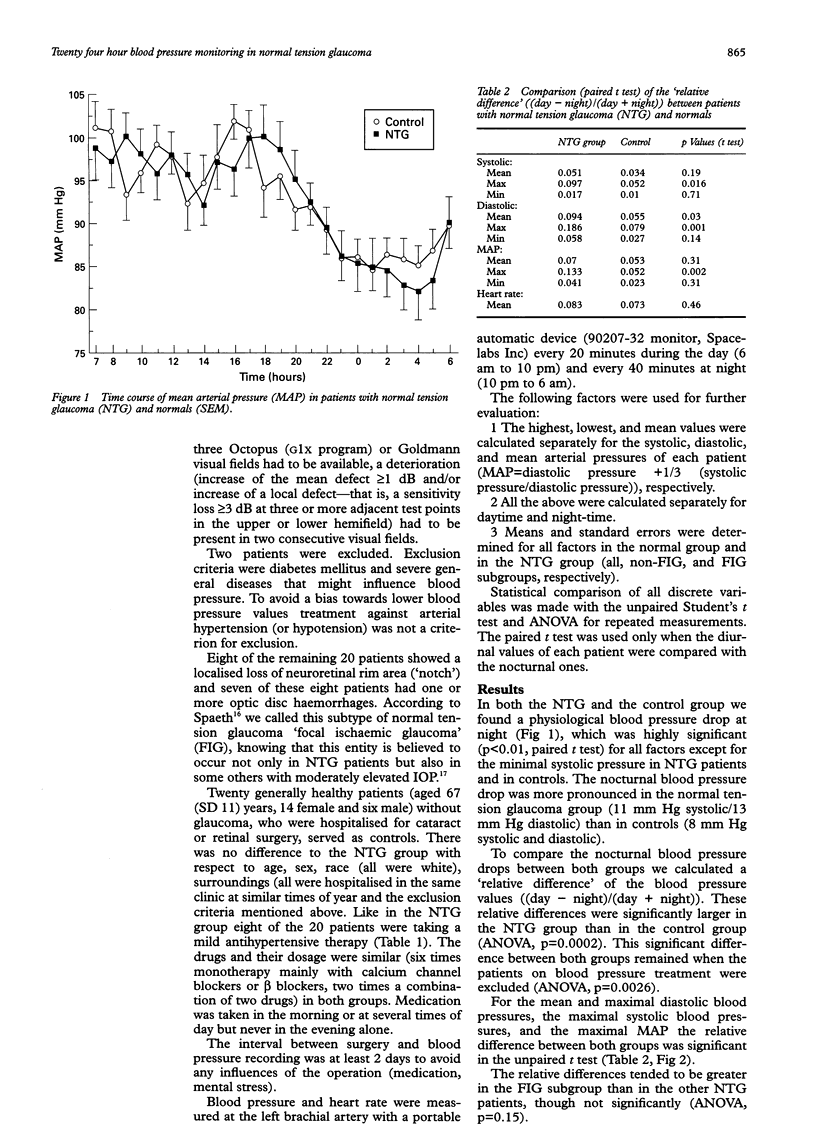
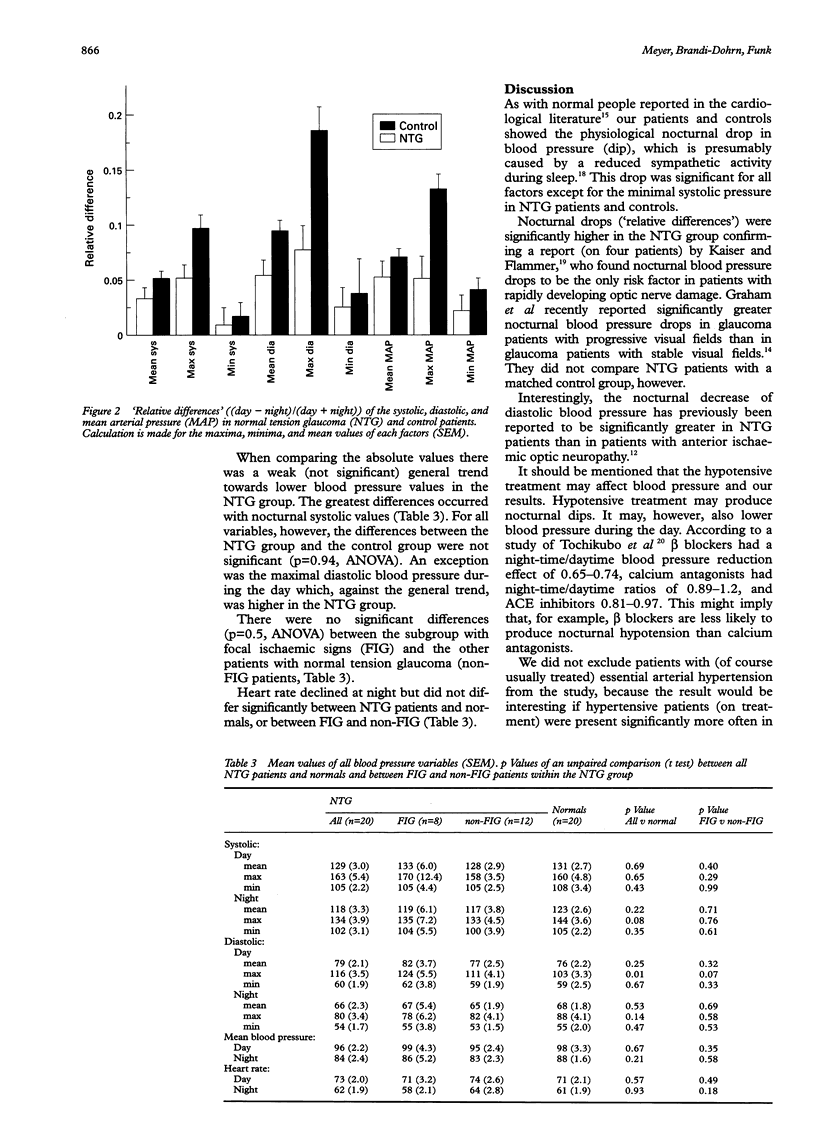
BACKGROUND: The few investigations that used continuous 24 hour blood pressure monitoring to investigate whether blood pressure in patients with normal tension glaucoma is lower than in normal subjects yielded conflicting results. Therefore, a prospective controlled trial was carried out. METHODS: Systemic blood pressure was recorded continuously over a 24 hour period in 20 patients with normal tension glaucoma (IOP < or = 21 mm Hg). Eight of them showed a localised loss of the neuroretinal rim area and, in addition, optic disc haemorrhages-that is, focal ischaemic signs. Twenty healthy patients without glaucoma, who were hospitalised for cataract or retinal surgery, served as controls. Blood pressure was automatically measured every 20 minutes during the day and every 40 minutes at night. RESULTS: Both groups showed a significant (physiological) blood pressure drop at night, which was significantly (p < 0.001, ANOVA) more pronounced in the group with normal tension glaucoma than in the control group. There was a weak trend towards lower blood pressure values in the normal tension glaucoma group. Minima, maxima, and mean values of the systolic, diastolic, and mean arterial pressures did not differ significantly between the group with normal tension glaucoma and the control group. The greatest differences occurred with nocturnal systolic and diurnal diastolic values. There were no significant differences between the subgroup with focal lesions and the other patients with normal tension glaucoma. CONCLUSIONS: Patients with normal tension glaucoma tend to have lower blood pressure values (p > 0.05, ANOVA) than normals; this difference is probably much smaller than formerly assumed. Patients with normal tension glaucoma, however, have significantly greater nocturnal blood pressure drops (p < 0.001, ANOVA) than normal controls. Nocturnal blood pressure drops (relative day-night differences) may play a more important role in the pathogenesis of normal tension glaucoma than the absolute height of the blood pressure.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Béchetoille A., Bresson-Dumont H. Diurnal and nocturnal blood pressure drops in patients with focal ischemic glaucoma. Graefes Arch Clin Exp Ophthalmol. 1994 Nov;232(11):675–679. doi: 10.1007/BF00171383. [DOI] [PubMed] [Google Scholar]
- Carter C. J., Brooks D. E., Doyle D. L., Drance S. M. Investigations into a vascular etiology for low-tension glaucoma. Ophthalmology. 1990 Jan;97(1):49–55. doi: 10.1016/s0161-6420(90)32627-1. [DOI] [PubMed] [Google Scholar]
- Cartwright M. J., Grajewski A. L., Friedberg M. L., Anderson D. R., Richards D. W. Immune-related disease and normal-tension glaucoma. A case-control study. Arch Ophthalmol. 1992 Apr;110(4):500–502. doi: 10.1001/archopht.1992.01080160078035. [DOI] [PubMed] [Google Scholar]
- Corbett J. J., Phelps C. D., Eslinger P., Montague P. R. The neurologic evaluation of patients with low-tension glaucoma. Invest Ophthalmol Vis Sci. 1985 Aug;26(8):1101–1104. [PubMed] [Google Scholar]
- Demailly P., Cambien F., Plouin P. F., Baron P., Chevallier B. Do patients with low tension glaucoma have particular cardiovascular characteristics? Ophthalmologica. 1984;188(2):65–75. doi: 10.1159/000309344. [DOI] [PubMed] [Google Scholar]
- Gasser P., Flammer J. Blood-cell velocity in the nailfold capillaries of patients with normal-tension and high-tension glaucoma. Am J Ophthalmol. 1991 May 15;111(5):585–588. doi: 10.1016/s0002-9394(14)73703-1. [DOI] [PubMed] [Google Scholar]
- Goldberg I., Hollows F. C., Kass M. A., Becker B. Systemic factors in patients with low-tension glaucoma. Br J Ophthalmol. 1981 Jan;65(1):56–62. doi: 10.1136/bjo.65.1.56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Graham S. L., Drance S. M., Wijsman K., Douglas G. R., Mikelberg F. S. Ambulatory blood pressure monitoring in glaucoma. The nocturnal dip. Ophthalmology. 1995 Jan;102(1):61–69. doi: 10.1016/s0161-6420(95)31053-6. [DOI] [PubMed] [Google Scholar]
- Hayreh S. S., Zimmerman M. B., Podhajsky P., Alward W. L. Nocturnal arterial hypotension and its role in optic nerve head and ocular ischemic disorders. Am J Ophthalmol. 1994 May 15;117(5):603–624. doi: 10.1016/s0002-9394(14)70067-4. [DOI] [PubMed] [Google Scholar]
- Hoyng P. F., de Jong N., Oosting H., Stilma J. Platelet aggregation, disc haemorrhage and progressive loss of visual fields in glaucoma. A seven year follow-up study on glaucoma. Int Ophthalmol. 1992 Mar;16(2):65–73. doi: 10.1007/BF00918934. [DOI] [PubMed] [Google Scholar]
- Kaiser H. J., Flammer J., Graf T., Stümpfig D. Systemic blood pressure in glaucoma patients. Graefes Arch Clin Exp Ophthalmol. 1993 Dec;231(12):677–680. doi: 10.1007/BF00919280. [DOI] [PubMed] [Google Scholar]
- Kaiser H. J., Flammer J. Systemic hypotension: a risk factor for glaucomatous damage? Ophthalmologica. 1991;203(3):105–108. doi: 10.1159/000310234. [DOI] [PubMed] [Google Scholar]
- Klaver J. H., Greve E. L., Goslinga H., Geijssen H. C., Heuvelmans J. H. Blood and plasma viscosity measurements in patients with glaucoma. Br J Ophthalmol. 1985 Oct;69(10):765–770. doi: 10.1136/bjo.69.10.765. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leighton D. A., Phillips C. I. Systemic blood pressure in open-angle glaucoma, low tension glaucoma, and the normal eye. Br J Ophthalmol. 1972 Jun;56(6):447–453. doi: 10.1136/bjo.56.6.447. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maynard C., Litwin P. E., Martin J. S., Cerqueira M., Kudenchuk P. J., Ho M. T., Kennedy J. W., Cobb L. A., Schaeffer S. M., Hallstrom A. P. Characteristics of black patients admitted to coronary care units in metropolitan Seattle: results from the Myocardial Infarction Triage and Intervention Registry (MITI). Am J Cardiol. 1991 Jan 1;67(1):18–23. doi: 10.1016/0002-9149(91)90092-y. [DOI] [PubMed] [Google Scholar]
- O'Brien E., Murphy J., Tyndall A., Atkins N., Mee F., McCarthy G., Staessen J., Cox J., O'Malley K. Twenty-four-hour ambulatory blood pressure in men and women aged 17 to 80 years: the Allied Irish Bank Study. J Hypertens. 1991 Apr;9(4):355–360. doi: 10.1097/00004872-199104000-00007. [DOI] [PubMed] [Google Scholar]
- Richards A. M., Nicholls M. G., Espiner E. A., Ikram H., Cullens M., Hinton D. Diurnal patterns of blood pressure, heart rate and vasoactive hormones in normal man. Clin Exp Hypertens A. 1986;8(2):153–166. doi: 10.3109/10641968609074769. [DOI] [PubMed] [Google Scholar]
- Spaeth G. L. A new classification of glaucoma including focal glaucoma. Surv Ophthalmol. 1994 May;38 (Suppl):S9–17. doi: 10.1016/0039-6257(94)90042-6. [DOI] [PubMed] [Google Scholar]