

Abstract
Background
Cultural adaptation of mental health care interventions is key, particularly when there is little or no therapist interaction. There is little published information on the methods of adaptation of bibliotherapy and e-mental health interventions.
Objective
To systematically search for evidence of the effectiveness of minimally guided interventions for the treatment of common mental disorders among culturally diverse people with common mental disorders; to analyze the extent and effects of cultural adaptation of minimally guided interventions for the treatment of common mental disorders.
Methods
We searched Embase, PubMed, the Cochrane Library, and PsycINFO for randomized controlled trials that tested the efficacy of minimally guided or self-help interventions for depression or anxiety among culturally diverse populations. We calculated pooled standardized mean differences using a random-effects model. In addition, we administered a questionnaire to the authors of primary studies to assess the cultural adaptation methods used in the included primary studies. We entered this information into a meta-regression to investigate effects of the extent of adaptation on intervention efficacy.
Results
We included eight randomized controlled trials (RCTs) out of the 4911 potentially eligible records identified by the search: four on e-mental health and four on bibliotherapy. The extent of cultural adaptation varied across the studies, with language translation and use of metaphors being the most frequently applied elements of adaptation. The pooled standardized mean difference for primary outcome measures of depression and anxiety was -0.81 (95% CI -0.10 to -0.62). Higher cultural adaptation scores were significantly associated with greater effect sizes (P=.04).
Conclusions
Our results support the results of previous systematic reviews on the cultural adaptation of face-to-face interventions: the extent of cultural adaptation has an effect on intervention efficacy. More research is warranted to explore how cultural adaptation may contribute to improve the acceptability and effectiveness of minimally guided psychological interventions for common mental disorders.
Keywords: cultural adaptation, depression, anxiety, self-help, minimally guided intervention, e-mental health, bibliotherapy
Introduction
Globalization of Minimally Guided Interventions
There is an alarming mismatch between the prevalence of mental disorders and the availability of services to meet mental health needs, particularly in low- and middle-income countries (LMICs) [1]. The Movement for Global Mental Health [2] emphasizes increasing the coverage of treatments for mental disorders worldwide, particularly in countries where the treatment gap is greatest (ie, in low- and middle-income countries) [3]. There is a growing interest in how to deliver psychological interventions to diverse populations, and various innovative solutions may expand their reach and accessibility in low- and high-income countries alike.
Evidence shows that minimally guided interventions (ie, self-help and guided self-help) may be as efficacious as face-to-face interventions for the treatment of a broad range of common mental disorders [4], including in routine care [5], with guided self-help being slightly superior to complete self-help [6]. Indeed, the World Health Organization (WHO) has updated recommendations on the treatment of depression in low-resource settings to include both face-to-face (eg, high therapist investment) and self-help interventions [7].
Bibliotherapy (ie, therapeutic books) and e-mental health are established means of providing minimally guided psychological interventions requiring one hour or less of face-to-face support time or up to 90 minutes total telephone or email support [8]. They may also appeal to people who are concerned about stigma associated with accessing mental health services. However, evidence on their efficacy is currently limited to high-income countries (HICs) and in culturally homogenous groups [9,10]. A recent systematic review found only three studies on e-mental health interventions in LMICs [11]. Nevertheless, these types of interventions may be viable solutions to narrow the mental health treatment gap in LMICs [12,13], where two-thirds of the 3.2 billion people using the Internet live [14], and where literacy rates are rapidly rising—currently estimated at 85% of the world population [15]. An important consideration is that in areas with restricted resources and as a means of increasing coverage of minimally guided interventions, the guidance may be given by a trained layperson, such as a family carer [16] or a community volunteer.
Cultural Adaptation
Intervention developers and care providers should ensure that treatments are suited to the culture of the intended users, both for moral reasons and for technical, efficacy-related reasons [16]. Cultural adaptation is defined as “the systematic modification of an evidence-based treatment or intervention protocol to consider language, culture, and context in such a way that it is compatible with the client’s cultural patterns, meanings, and values” [17]. Cultural adaptation to the needs and expectations of intended users is likely very important for minimally guided interventions because there is little or no therapist interaction to carry the dimension of culture into the intervention.
The Bernal and Sáez-Santiago framework was proposed in 1995 as a framework for planning and conducting interventions with culturally and linguistically diverse (CALD) clients [18,19]. It has eight elements of adaptation: (1) language, (2) person (client) attributes, (3) metaphors, (4) content, (5) concepts, (6) goals, (7) methods, and (8) context of the intervention or services [19].
Evidence suggests that culturally adapted interventions may be more efficacious than interventions that have not been adapted [20], and that effectiveness increases with the number of implemented adaptation elements, according to the Bernal and Sáez-Santiago framework [21,22]. Evidence from systematic reviews show that the extent to which face-to-face interventions are culturally adapted varies considerably [23,24]. However, little is known about the methods and potential benefits of cultural adaptation of minimally guided interventions designed to improve the mental health and well-being of CALD populations.
The aim of this paper was to understand the extent and effects of cultural adaptation of minimally guided interventions for the treatment of common mental disorders. We conducted a systematic review and meta-analysis of experimental studies of minimally guided interventions for the treatment of common mental disorders—depression, anxiety, and adjustment disorders—conducted with culturally diverse populations. We also tested whether the characteristics and extent of cultural adaptation of the minimally guided interventions under study were associated with the combined effect estimates.
Methods
The methods and procedures used to conduct the systematic review and meta-analysis are reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [25].
Systematic Search
We designed our search strategy by combining relevant acronyms and synonyms that captured the population, intervention, comparator, and outcomes (PICO) elements, and the study design consistent with our study aim. Professional librarians from the University of Geneva and the University of Zurich assisted in testing and refining the search strategy, which was written for PubMed and adapted to Embase, the Cochrane Library, and PsycINFO.
We conducted a database search of Embase, PubMed, Cochrane Library, and PsycINFO. Four search concepts were combined in order to capture relevant literature: mode of delivery (eg, mobile phone, multimedia, and Web based), intervention program (eg, self-help, minimally guided, and Internet cognitive behavioral therapy [iCBT]), common mental disorders (eg, depression, anxiety, stress, and trauma), and cultural diversity. In order to identify culturally diverse populations, we took a proxy of LMICs classified according to the World Bank [26], using their names and population adjectives with additional high-income country and population names that we considered to be culturally divergent from North America, Europe, and Australia (eg, Saudi Arabia).
Searches were limited to experimental reports found in journal articles published between January 1995 and July 2015. Limits for humans were flexibly applied in the electronic searches in PubMed and PsycINFO, though unindexed articles were captured by removing the humans filter from 2013 onwards. Details of the search strategy can be found in Multimedia Appendix 1.
In addition, we hand searched citations of eligible articles, and forward citation of protocol articles found in the search, in order to identify additional relevant published studies. Finally, at the third conference of the European Society for Research on Internet Interventions in Poland in September 2015, where we presented preliminary review results, we asked the audience of experts in e-mental health interventions to inform us if they were aware of any articles that we may have missed. All citations were managed using EndNote X7 (Thomson Reuters) and references and abstracts were exported into Microsoft Excel for easy title and abstract screening.
Study Selection
The inclusion criteria applied to articles to be included in this study are shown in Textbox 1.
Inclusion criteria for articles.
Population:
More than 75% of participants above a clinical cutoff for symptoms of unipolar depression or anxiety including trauma-related disorders, irrespective of the clinical measure used
People culturally and linguistically different to those for which the intervention was originally designed
Intervention:
A minimally-guided or unguided self-help program; one hour or less of face-to-face health worker or trained layperson time or up to 90 minutes total telephone or email support [8], regardless of delivery mode
Structured and active therapeutic modality (ie, the intervention has clear theoretical underpinnings or an evidence base)
Must include methodology used (ie, an observational or controlled study, process report, or a protocol)
Comparator:
Any control condition, including placebo, treatment/care as usual, waitlist control, or active treatment comparison
Outcome:
Postintervention measures of symptoms of mental illness
Study design:
Randomized or nonrandomized experimental studies
The exclusion criteria applied to articles to be excluded from this study are shown in Textbox 2.
Exclusion criteria for articles.
Intervention(s) as an adjunct to traditional face-to-face therapy
Delivered in an inpatient setting
Intervention designed for the culturally and linguistically diverse (CALD) population, therefore not adapted
Training materials for health workers
Prevention programs for mental disorders
Two researchers (EH and MHS) independently screened titles and abstracts according to the inclusion and exclusion criteria, which were then applied to the full texts of the eligible publications. All disagreements were discussed and resolved. Where it did not become clear from the full text, we wrote to investigators to verify the eligibility of the primary study, focusing in particular on whether the intervention was minimally guided and adapted for, not developed for, culturally and linguistically diverse populations.
Data Extraction and Additional Data Collection
Two researchers (EH and MHS) designed and piloted a data extraction tool by considering all study characteristics related to the research question considering the PICO elements.
Consistent with the Cochrane Collaboration approach and the methods used in a recent review of cultural adaptations of traditional psychological interventions [24], we developed a structured checklist to critically appraise the methodological quality of the included studies considering the following four criteria: method of randomization, allocation concealment, blinding of outcome assessment, and attrition bias [24]. Two researchers (EH and MHS) independently applied the checklist to each of the included primary studies and a third researcher (EA) was called upon in cases of discordance of opinion.
In order to find out more about cultural adaptation methods used by researchers, we developed a short online questionnaire based on the framework by Bernal and Sáez-Santiago [19] (see Multimedia Appendix 2) and asked the authors of the included studies to complete it. Based on the information from the full-text articles and the questionnaires received, we assigned each study a score according to the number of Bernal and Sáez-Santiago framework adaptation elements that were applied.
Data Analysis
We retained only the outcome measure designed as the primary endpoint in each study. We entered the number of participants, postintervention means and standard deviations, and the number of adaptation points into Stata 13 (StataCorp LP) [27]. Then we stratified the analyses by the adaptation score and conducted a meta-analysis using a random-effect method to calculate the pooled effect size based on the combination of the standardized mean differences of primary studies, and formally assessed and quantified heterogeneity using Higgins’ I2 [28]. We then examined whether the extent of cultural adaptation explained the heterogeneity across studies using an unadjusted random-effects meta-regression model.
In a sensitivity analysis, we tested the robustness of using primary outcomes data only for our main analysis by rerunning the meta-analysis separating depression and anxiety data, irrespective of whether measures were used as primary or secondary endpoints. We then compared the I2 values and 95% CIs between models to gain insight into the potential contribution of the primary versus secondary outcome to the heterogeneity observed in the stratified analyses.
Results
Systematic Search and Study Selection
We identified 4911 records, and excluded 1125 duplicates and 3585 citations on the basis of their titles and abstracts, which left 101 publications that were taken forward for full-text review. Of these, 11 were conference abstracts only, leaving 90 full texts to screen. Two articles were in Korean, so a Korean-speaking acquaintance of the research team was given guidance as to how to screen the articles, neither of which met inclusion criteria [29,30].
Reasons for exclusion are reported in Figure 1. Briefly, several articles did not meet various inclusion criteria, examples of which follow: they were not interventions designed in the West and adapted for a CALD population, but instead were designed specifically for the population [31-33]; the participants were not considered a CALD population [34-36]; the interventions were not self-help according to our standard definition above [37-39]; and/or no common mental disorder outcome measure was reported [40-42].
Figure 1.
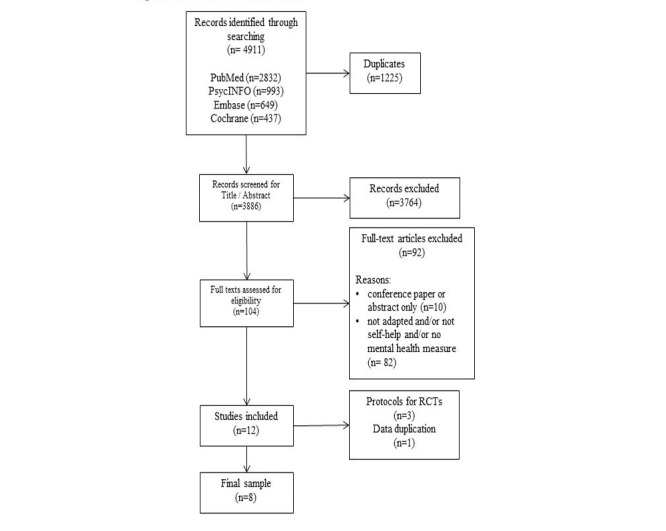
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) diagram with systematic search and selection process. RCT: randomized controlled trial.
A total of 12 articles were retrieved (see PRISMA diagram in Figure 1); eight were randomized controlled trials (RCTs), two were protocols for included RCTs [43,44], and one was a protocol for an RCT whose results have not yet been published [45]. One additional article [46] utilized one of the datasets already included [47] (ie, urban sample). One of the included RCTs [47] had two different study sites—urban and rural—with different methodologies; therefore, we treated these as two different datasets. Four studies investigated the effect of bibliotherapy [47-50], and the remaining four were of e-mental health interventions [51-54].
One additional unpublished dataset was identified from key informants at the European Society for Research on Internet Interventions (ESRII) conference, but this was excluded. Upon contacting the author, there was insufficient information to determine whether the intervention was designed for the CALD population and, therefore, whether the study met our inclusion criteria. Characteristics of the studies are presented in Table 1.
Table 1.
Characteristics of RCTa studies retrieved.
| Study | Randomized, n (analyzed, n) |
CALDb
group |
Delivery | Therapy approach |
Length (weeks) |
Guidance | Adapt.c
points |
Primary outcome measure |
| Choi et al 2012 [48] |
63 (51) | Chinese | e-MHd | CBTe | 8 | MGf | 7 | (C)BDI IIg depression |
| Liu et al 2009 [51] |
52 (40) | Chinese | Biblio.h | CBT | 4 | MG | 0 | (C)BDI II depression |
| Moldovan et al 2013 [52] | 96 (84) | Romanian | Biblio. | CBT | 4.5 | MG | 0 | BDI IIi depression |
| Muto et al 2011 [53] |
70 (42) | Japanese | Biblio. | ACTj | 8 | SHk | 5 | GHQl depression |
| Naeem et al 2014 [54] | 192 (183) | Pakistani | Biblio. | CBT | 12 | MG | 5 | HADS-Dm depression |
| Tulbure et al 2015 [50] | 76 (68) | Romanian | e-MH | CBT | 9 | MG | 5 | LSASSRn anxiety |
| Ünlü Ince et al 2013 [49] | 96 (56) | Turkish | e-MH | PSo | 5 | MG | 5 | CES-Dp depression |
| Wang et al 2013 [47] (urban) |
103 (61) | Chinese | e-MH | SCTq | 4.5 | SH | 3 | PDSr anxiety |
| Wang et al 2013 [47] (rural) |
94 (90) | Chinese | e-MH | SCT | 4.5 | SH | 3 | PDS anxiety |
aRCT: randomized controlled trial.
bCALD: culturally and linguistically diverse.
cadapt: adaptation.
de-MH: e-mental health.
eCBT: cognitive behavioral therapy.
fMG: minimally guided.
g(C)BDI II: (Chinese) Beck Depression Inventory II.
hbiblio.: bibliotherapy.
iBDI II: Beck Depression Inventory II.
jACT: acceptance and commitment therapy.
kSH: self-help.
lGHQ: General Health Questionnaire.
mHADS-D: Hospital Anxiety and Depression Scale.
nLSASSR: Liebowitz Social Anxiety Scale Self Report.
oPS: problem solving.
pCES-D: Center for Epidemiological Studies Depression Scale.
qSCT: social cognitive theory.
rPDS: Patient Distress Scale.
There were eight RCTs, including nine datasets for analysis. The cultural backgrounds of the participants included in the studies were Chinese, Romanian, Pakistani, Japanese, and Turkish. Most of the interventions had a cognitive behavioral approach [48,50-52]; however, one study used a problem solving approach [44], one study with two datasets used a social cognitive theory approach [47], and one study used acceptance and commitment therapy [53]. The duration of interventions ranged from 4 to 12 weeks and only two out of eight interventions were completely self-help (ie, no guidance from a health worker) [53]. The number of Bernal and Sáez-Santiago framework adaptation points carried out ranged from 0 to 7, out of a possible 8. Two interventions, across three datasets, focused primarily on anxiety symptoms, and six on depressive symptomatology, with a range of outcome measures to quantify effects.
Data Extraction and Additional Data Collection
We determined the overall risk of bias of the included studies to be moderate. The main issue that introduced potential bias into studies was the outcome measures being subjective self-report measures, coupled with the fact that participants could not be blinded. Details on risk of bias assessment are reported in Multimedia Appendix 3.
The cultural adaptation methods used were only minimally reported in the primary publications. Six researchers responded to the questionnaire that we sent. Using questionnaire responses, where provided, and the full texts of the RCTs plus any protocols or related previously published studies, we assigned each RCT an adaptation score according to the number of Bernal and Sáez-Santiago framework adaptation elements that we deemed were applied (see Figure 2). In some cases, researchers had considered an element of adaptation but chosen not to carry out that adaptation having not identified a need for it. These were coded as affirmative responses; examples of affirmative questionnaire responses can be found in Multimedia Appendix 4.
Figure 2.

Adaptation score assigned to the selected studies.
All but two researchers indicated that they had translated their interventions into the language of the target group. Seven researchers—five in e-mental health interventions—reported the use of adapted metaphors, using symbols, concepts, idioms, and sayings from the target culture. Local values and traditions in order to carry the content of the intervention were considered by five researchers—four in e-mental health interventions. Theoretical concepts and constructs were considered by four e-mental health researchers and one bibliotherapy researcher. No researcher reported having considered treatment goals in the adaptation of their intervention. The delivery method of the intervention (eg, making particular allowances or breaking strategies into smaller tasks) was mentioned in the questionnaire response of three researchers—two e-mental health interventions. The socioeconomic and political context of the intervention was considered by five researchers—two e-mental health interventions—yet most researchers who responded to the qualitative element of this question mentioned that e-mental health or bibliotherapy in itself was used in response to the socioeconomic and cultural environment (eg, stigma and access to services).
Data Analysis
The random-effects meta-analysis (see Figure 3) on the primary outcome measures included nine datasets with a total of 684 participants. We stratified the data by descending assigned cultural adaptation points.
Figure 3.
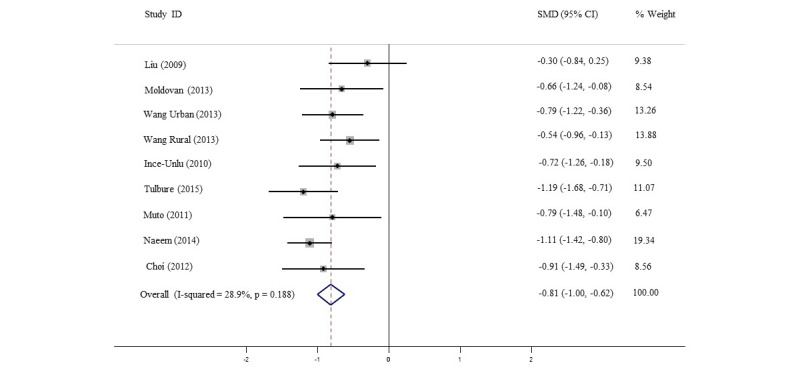
Random-effects meta-analysis of primary outcome measures in order of the study adaptation score. SMD: standardized mean difference.
Overall, the minimally guided and self-help interventions significantly improved depression and anxiety symptomatology; the pooled standardized mean difference (SMD) from primary outcome measures was -0.81 (95% CI -0.10 to -0.62), with low-to-moderate between-studies heterogeneity (I2=28.9%).
The meta-regression (see Figure 4) showed that the adaptation scores significantly explained the pooled SMD. Specifically, a 1-point increase in the adaptation score was significantly associated with an increase in effect size of 0.117 (P=.04), or a 14% rise in pooled efficacy.
Figure 4.
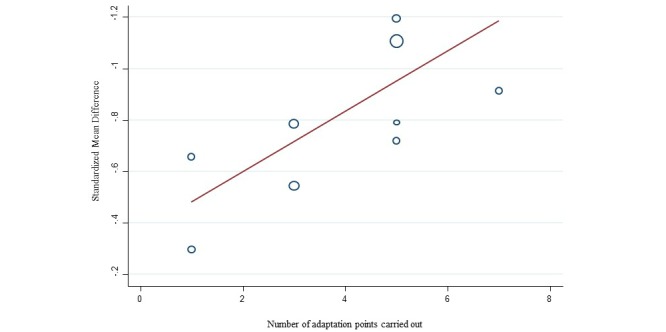
Meta-regression of the standardized mean difference and adaptation score.
To test the robustness of our main model, which focused on the primary outcome measures, we carried out two separate meta-analyses for each outcome (ie, depressive or anxiety symptoms), irrespective of what the intervention was primarily designed for. Our results were largely unchanged, but the heterogeneity across the studies was greater (SMD=-0.65 [95% CI -0.92 to -0.38], I2=62.2% for anxiety and SMD=-0.58 [95% CI -0.93 to -0.24], I2=75.4% for depression), thus confirming our use of primary measures only in the analysis.
Discussion
Principal Findings
Culturally adapted self-help or minimally guided bibliotherapy and e-mental health interventions moderately, but significantly, reduced depressive and anxious symptomatology in populations culturally and linguistically distinct from those for which the interventions had been originally designed. More extensive cultural adaptation of the interventions under study was significantly associated with larger effect sizes; however, details of the cultural adaptation methodologies applied were largely underreported.
Researchers should be encouraged to report in detail their adaptation methods to enable readers to appraise both internal and external validity of the study findings, and to inform the implementation of minimally guided interventions and their scalability beyond the research context.
Our results have both public health and clinical relevance, particularly to program managers and health workers who aim to use minimally guided interventions among CALD clients. Decision makers should consider the implications of cultural adaptation on the expected efficacy of interventions before use and, if feasible, plan the required resources and time investments accordingly. A 14% rise in efficacy per adaptation point increase should be weighed against the costs of adapting intervention content, considering the anticipated coverage of the intervention. Adaptation could also positively affect attrition rates, which can be high in self-help interventions.
Our results suggest that the effect of minimally guided interventions used in CALD populations was significantly influenced by cultural adaptation. We were unable to review the specifics of qualitative methodologies involved, but depending on resources, adaptation could resemble a single focus group of community members, or a costly and extensive multi-stakeholder consultation program. Precise information on the methods used is important to allow, on the one hand, a comprehensive adaptation to other settings and contexts and, on the other hand, the preservation of the original intervention’s core therapeutic techniques and components to maximize the fidelity to the original intervention.
The Bernal and Sáez-Santiago framework was extremely useful but difficult to operationalize. Further research is needed to develop, pilot, and test an adaptation protocol for minimally guided interventions that would favor the utility and efficiency of the original framework’s use in cross-cultural psychology and psychiatry. Such an adaptation protocol should strive to include the target community in qualitative research and discussions on adaptation of materials.
Limitations
Our study has limitations. First, we focused on selected countries that we arbitrarily considered to be culturally distinct. However, this choice was extensively discussed to include geographically diverse LMICs and high-income countries culturally diverse from North America, Australia, and Western Europe, where the majority of minimally guided interventions are developed and tested. We did not consider potential cultural differences between Western countries (eg, an intervention designed in the United States and used in Norway), and we did not focus on indigenous populations as culturally diverse, and underserved, groups.
Second, and briefly mentioned above, although the meta-analysis showed low heterogeneity across the studies, the meta-regression used to formally explore this further was based on only nine datasets for a total of 684 participants. The Cochrane handbook suggests a minimum of 10 studies to run a meta-regression [55], so these findings should be considered with caution. Further, because half of the studies (n=5) included completers only in their analyses, the reported effect sizes might have been inflated, and an overestimation of the true effect in our meta-analysis cannot be excluded [56]. In addition, the marked differences in intervention duration and in follow-up times between studies may further limit comparability. In the meta-regression, we focused only on the number of Bernal adaptation elements. This was coherent with our main scope and was statistically appropriate (see above). However, other study design characteristics could also explain the between-studies heterogeneity and, at least to some extent, they might even confound or modify the observed effect of cultural adaptation.
Third, using the Bernal and Sáez-Santiago framework carries its own limitations. It was developed over 20 years ago in North America in relation to transcultural issues of working with Latino communities. In addition, it was informed by a theory-driven and anecdotal approach, as opposed to being informed by community-based explorative and qualitative data. We used the Bernal and Sáez-Santiago framework because it had been used to categorize adaptations made in previous systematic reviews [22-24]. The number of elements of the Bernal and Sáez-Santiago framework carried out in each study was based on a subjective assessment of the information from full texts and the qualitative information provided in the questionnaires. Though authors agreed that they had carried out most adaptation elements, the review researchers independently tended to assign lower completion rates. This coding remained subjective on both the authors’ and the primary study researchers’ part, mainly because Bernal concepts are rather abstract and can sometimes overlap. Also, if researchers stated that they had considered an element but chosen not to carry it out, we coded this as an affirmative answer. A further limitation of the adaptation coding stemmed from the fact that the Bernal and Sáez-Santiago framework was developed for face-to-face treatments. We chose to use the framework in its original state. Some of the categories (ie, treatment goals or therapeutic relationship) are likely less or modestly relevant for minimally guided interventions.
Comparison With Prior Work
Our results are consistent with evidence from previous systematic reviews on the cultural adaptation of face-to-face interventions for common mental disorders [21-24], particularly that completing more elements of adaptation is associated with a higher effect size [22]. Indeed, the effect size of the most comprehensively adapted, Chinese version of the Sadness intervention [48] was similar, if not slightly higher, compared to its original Australian version [57]—within-groups Cohen’s d for reduction in Beck Depression Inventory score was 1.41 in the Chinese adapted intervention and 1.27 in the original Australian version.
Further comparisons with previous findings are less straightforward. Statistical power was limited by the total number of studies included (see below), which were not sufficient to conduct advanced, multivariable, meta-regression models to test which, if any, of the Bernal adaptation elements might have contributed the most to the observed between-studies heterogeneity. Similarly, we were not able to consider other plausibly relevant covariates in our models, such as therapeutic modality, level of health worker support, length of delivery, and level of engagement or medium. Evidence on the impact of cultural adaptation is scant, but previous studies found that therapeutic goals, metaphors and symbols [22], and conceptualizations (ie, explanatory models) [21] may significantly account for variance in effect sizes of the interventions under study. These previous findings seem plausible because, although little is known about specific components that determine the effectiveness of a self-help program [9], providing users with an explanatory model of their distress using meaningful terms and symbols may constitute a critical prerequisite of minimally guided interventions.
Conclusions
In conclusion, our results support the careful application of cultural adaptation of minimally guided and self-help interventions, whether provided via bibliotherapy or the Internet, before their use in diverse settings and populations. This largely applies to the globalization of mental health services and psychological interventions, for which cultural adaptation is key. Further, there is also a moral case to test and demonstrate the appropriateness, acceptability, and harmlessness of interventions up front. Cultural adaptation is explicitly intended to render interventions meaningful and helpful to groups that are culturally diverse from those for which the intervention was designed. Therefore, these findings may be particularly relevant to program managers and treatment providers in non-Western settings.
Acknowledgments
We thank Dr Kieren Egan and Professor Matthias Egger for their advice on statistical analysis of the data.
Abbreviations
- ACT
acceptance and commitment therapy
- adapt.
adaptation
- BDI II
Beck Depression Inventory II
- biblio.
bibliotherapy
- CALD
culturally and linguistically diverse
- (C)BDI II
(Chinese) Beck Depression Inventory II
- CBT
cognitive behavioral therapy
- CES-D
Center for Epidemiological Studies Depression Scale
- e-MH
e-mental health
- ESRII
European Society for Research on Internet Interventions
- GHQ
General Health Questionnaire
- HADS-D
Hospital Anxiety and Depression Scale
- HIC
high-income country
- iCBT
Internet cognitive behavioral therapy
- LMICs
low- and middle-income countries
- LSASSR
Liebowitz Social Anxiety Scale Self Report
- MG
minimally guided
- PDS
Patient Distress Scale
- PICO
population, intervention, comparator, and outcomes
- PRISMA
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- PS
problem solving
- RCT
randomized controlled trial
- SCT
social cognitive theory
- SH
self-help
- SMD
standardized mean difference
- WHO
World Health Organization
Search strategy.
Questionnaire for researchers.
Risk of bias analysis.
Example responses from researchers.
Footnotes
Conflicts of Interest: None declared.
References
- 1.Kessler R, Angermeyer M, Anthony J, Demyttenaere K, Gasquet I, Gluzman S, Gureje O, Haro JM, Kawakami N, Karam A, Levinson D, Medina Mora ME, Oakley Browne MA, Posada-Villa J, Stein DJ, Adley Tsang CH, Aguilar-Gaxiola S, Alonso J, Lee S, Heeringa S, Pennell BE, Berglund P, Gruber MJ, Petukhova M, Chatterji S, Ustün TB. Lifetime prevalence and age-of-onset distributions of mental disorders in the World Health Organization's World Mental Health Survey Initiative. World Psychiatry. 2007 Oct;6(3):168–176. http://onlinelibrary.wiley.com/resolve/openurl?genre=article&sid=nlm:pubmed&issn=1723-8617&date=2007&volume=6&issue=3&spage=168 . [PMC free article] [PubMed] [Google Scholar]
- 2.Patel V, Prince M. Global mental health: A new global health field comes of age. JAMA. 2010 May 19;303(19):1976–1977. doi: 10.1001/jama.2010.616. http://europepmc.org/abstract/MED/20483977 .303/19/1976 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Saxena S, Thornicroft G, Knapp M, Whiteford H. Resources for mental health: Scarcity, inequity, and inefficiency. Lancet. 2007 Sep 8;370(9590):878–889. doi: 10.1016/S0140-6736(07)61239-2.S0140-6736(07)61239-2 [DOI] [PubMed] [Google Scholar]
- 4.Andersson G, Cuijpers P, Carlbring P, Riper H, Hedman E. Guided Internet-based vs face-to-face cognitive behavior therapy for psychiatric and somatic disorders: A systematic review and meta-analysis. World Psychiatry. 2014 Oct;13(3):288–295. doi: 10.1002/wps.20151. doi: 10.1002/wps.20151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Andersson G, Titov N. Advantages and limitations of Internet-based interventions for common mental disorders. World Psychiatry. 2014 Feb;13(1):4–11. doi: 10.1002/wps.20083. doi: 10.1002/wps.20083. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Berger T, Hämmerli K, Gubser N, Andersson G, Caspar F. Internet-based treatment of depression: A randomized controlled trial comparing guided with unguided self-help. Cogn Behav Ther. 2011;40(4):251–266. doi: 10.1080/16506073.2011.616531. [DOI] [PubMed] [Google Scholar]
- 7.World Health Organization. Geneva, Switzerland: World Health Organization; 2015. [2016-08-21]. Comparative effectiveness of different formats of psychological treatments for depressive disorder http://www.who.int/mental_health/mhgap/evidence/depression/q8/en/ [Google Scholar]
- 8.Anderson L, Lewis G, Araya R, Elgie R, Harrison G, Proudfoot J, Schmidt U, Sharp D, Weightman A, Williams C. Self-help books for depression: How can practitioners and patients make the right choice? Br J Gen Pract. 2005 May;55(514):387–392. http://bjgp.org/cgi/pmidlookup?view=long&pmid=15904559 . [PMC free article] [PubMed] [Google Scholar]
- 9.Lewis C, Pearce J, Bisson JI. Efficacy, cost-effectiveness and acceptability of self-help interventions for anxiety disorders: Systematic review. Br J Psychiatry. 2012 Jan;200(1):15–21. doi: 10.1192/bjp.bp.110.084756. http://bjp.rcpsych.org/cgi/pmidlookup?view=long&pmid=22215865 .200/1/15 [DOI] [PubMed] [Google Scholar]
- 10.Van't Hof E, Cuijpers P, Stein D. Self-help and Internet-guided interventions in depression and anxiety disorders: A systematic review of meta-analyses. CNS Spectr. 2009 Feb;14(2 Suppl 3):34–40. doi: 10.1017/s1092852900027279. [DOI] [PubMed] [Google Scholar]
- 11.Arjadi R, Nauta M, Chowdhary N, Bockting C. A systematic review of online interventions for mental health in low and middle income countries: A neglected field. Glob Ment Health (Camb) 2015 Jul 14;2:1–6. doi: 10.1017/gmh.2015.10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Muñoz RF. Using evidence-based Internet interventions to reduce health disparities worldwide. J Med Internet Res. 2010;12(5):e60. doi: 10.2196/jmir.1463. http://www.jmir.org/2010/5/e60/ v12i5e60 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Watts S, Andrews G. Internet access is NOT restricted globally to high income countries: So why are evidenced based prevention and treatment programs for mental disorders so rare? Asian J Psychiatr. 2014 Aug;10:71–74. doi: 10.1016/j.ajp.2014.06.007.S1876-2018(14)00140-3 [DOI] [PubMed] [Google Scholar]
- 14.ICT Facts and Figures. Geneva, Switzerland: International Telecommunication Union; 2015. May, [2015-11-27]. The world in 2015 http://www.itu.int/en/ITU-D/Statistics/Documents/facts/ICTFactsFigures2015.pdf . [Google Scholar]
- 15.UIS Fact Sheet No. 32: Adult and Youth Literacy. Montreal, QC: UNESCO Institute for Statistics; 2015. Sep, [2015-11-27]. http://www.uis.unesco.org/literacy/Documents/fs32-2015-literacy.pdf . [Google Scholar]
- 16.Naeem F, Xiang S, Munshi T, Kingdon D, Farooq S. Self-help and guided self-help interventions for schizophrenia and related disorders. Cochrane Database Syst Rev. 2015 May 26;5:1–14. doi: 10.1002/14651858.CD011698. [DOI] [Google Scholar]
- 17.Castro F, Barrera M, Holleran Steiker LK. Issues and challenges in the design of culturally adapted evidence-based interventions. Annu Rev Clin Psychol. 2010;6:213–239. doi: 10.1146/annurev-clinpsy-033109-132032. http://europepmc.org/abstract/MED/20192800 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Bernal G, Jiménez-Chafey M, Domenech RM. Cultural adaptation of treatments: A resource for considering culture in evidence-based practice. Prof Psychol Res Pr. 2009 Aug;40(4):361–368. [Google Scholar]
- 19.Bernal G, Bonilla J, Bellido C. Ecological validity and cultural sensitivity for outcome research: Issues for the cultural adaptation and development of psychosocial treatments with Hispanics. J Abnorm Child Psychol. 1995 Feb;23(1):67–82. doi: 10.1007/BF01447045. [DOI] [PubMed] [Google Scholar]
- 20.Bernal G, Sáez-Santiago E. Culturally centered psychosocial interventions. J Community Psychol. 2006 Mar;34(2):121–132. doi: 10.1002/jcop.20096. [DOI] [Google Scholar]
- 21.Benish S, Quintana S, Wampold B. Culturally adapted psychotherapy and the legitimacy of myth: A direct-comparison meta-analysis. J Couns Psychol. 2011 Jul;58(3):279–289. doi: 10.1037/a0023626.2011-10381-001 [DOI] [PubMed] [Google Scholar]
- 22.Smith TB, Rodríguez MD, Bernal G. Culture. J Clin Psychol. 2011 Feb;67(2):166–175. doi: 10.1002/jclp.20757. [DOI] [PubMed] [Google Scholar]
- 23.Griner D, Smith T. Culturally adapted mental health intervention: A meta-analytic review. Psychotherapy (Chic) 2006;43(4):531–548. doi: 10.1037/0033-3204.43.4.531.2006-23019-014 [DOI] [PubMed] [Google Scholar]
- 24.Chowdhary N, Jotheeswaran A, Nadkarni A, Hollon S, King M, Jordans MJ, Rahman A, Verdeli H, Araya R, Patel V. The methods and outcomes of cultural adaptations of psychological treatments for depressive disorders: A systematic review. Psychol Med. 2014 Apr;44(6):1131–1146. doi: 10.1017/S0033291713001785. http://journals.cambridge.org/abstract_S0033291713001785 .S0033291713001785 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Moher D, Liberati A, Tetzlaff J, Altman D. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int J Surg. 2010;8(5):336–341. doi: 10.1016/j.ijsu.2010.02.007. http://linkinghub.elsevier.com/retrieve/pii/S1743-9191(10)00040-3 .S1743-9191(10)00040-3 [DOI] [PubMed] [Google Scholar]
- 26.The World Bank. [2015-11-27]. World Bank country and lending groups http://data.worldbank.org/about/country-and-lending-groups .
- 27.StataCorp . Stata. College Station, TX: StataCorp LP; 2013. [2016-08-29]. Stata Statistical Software: Release 13 http://www.stata.com/products/ [Google Scholar]
- 28.Higgins JP, Thompson S. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002 Jun 15;21(11):1539–1558. doi: 10.1002/sim.1186. [DOI] [PubMed] [Google Scholar]
- 29.Bae J. [Development and application of a Web-based expert system using artificial intelligence for management of mental health by Korean emigrants] J Korean Acad Nurs. 2013 Apr;43(2):203–214. doi: 10.4040/jkan.2013.43.2.203. doi: 10.4040/jkan.2013.43.2.203.201304203 [DOI] [PubMed] [Google Scholar]
- 30.Bae J. [Development of a user centered Web site for mental health management in adolescents] Taehan Kanho Hakhoe Chi. 2007 Feb;37(1):14–25. doi: 10.4040/jkan.2007.37.1.14.200702014 [DOI] [PubMed] [Google Scholar]
- 31.Mak WW, Chan AT, Cheung EY, Lin CL, Ngai KC. Enhancing Web-based mindfulness training for mental health promotion with the health action process approach: Randomized controlled trial. J Med Internet Res. 2015;17(1):e8. doi: 10.2196/jmir.3746. http://www.jmir.org/2015/1/e8/ v17i1e8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Tsai S. Audio-visual relaxation training for anxiety, sleep, and relaxation among Chinese adults with cardiac disease. Res Nurs Health. 2004 Dec;27(6):458–468. doi: 10.1002/nur.20039. [DOI] [PubMed] [Google Scholar]
- 33.Yuan Q, Liu S, Tang S, Zhang D. Happy@Work: Protocol for a Web-based randomized controlled trial to improve mental well-being among an Asian working population. BMC Public Health. 2014;14:685. doi: 10.1186/1471-2458-14-685. http://bmcpublichealth.biomedcentral.com/articles/10.1186/1471-2458-14-685 .1471-2458-14-685 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Macdonald J, Vallance D, McGrath M. An evaluation of a collaborative bibliotherapy scheme delivered via a library service. J Psychiatr Ment Health Nurs. 2013 Dec;20(10):857–865. doi: 10.1111/j.1365-2850.2012.01962.x. [DOI] [PubMed] [Google Scholar]
- 35.Pinto M, Greenblatt A, Hickman R, Rice H, Thomas T, Clochesy J. Assessing the critical parameters of eSMART-MH: A promising avatar-based digital therapeutic intervention to reduce depressive symptoms. Perspect Psychiatr Care. 2016 Jul;52(3):157–168. doi: 10.1111/ppc.12112. [DOI] [PubMed] [Google Scholar]
- 36.van Spijker BA, Calear AL, Batterham PJ, Mackinnon AL, Gosling JA, Kerkhof AJ, Solomon D, Christensen H. Reducing suicidal thoughts in the Australian general population through Web-based self-help: Study protocol for a randomized controlled trial. Trials. 2015;16:62. doi: 10.1186/s13063-015-0589-1. http://trialsjournal.biomedcentral.com/articles/10.1186/s13063-015-0589-1 .10.1186/s13063-015-0589-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Nasiri S, Kordi M, Gharavi M. A comparative study of the effects of problem-solving skills training and relaxation on the score of self-esteem in women with postpartum depression. Iran J Nurs Midwifery Res. 2015;20(1):105–112. http://europepmc.org/abstract/MED/25709699 . [PMC free article] [PubMed] [Google Scholar]
- 38.Rowe H, Sperlich M, Cameron H, Seng J. A Quasi-experimental outcomes analysis of a psychoeducation intervention for pregnant women with abuse-related posttraumatic stress. J Obstet Gynecol Neonatal Nurs. 2014;43(3):282–293. doi: 10.1111/1552-6909.12312. http://europepmc.org/abstract/MED/24754455 .S0884-2175(15)31545-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Songprakun W, McCann T. Evaluation of a bibliotherapy manual for reducing psychological distress in people with depression: A randomized controlled trial. J Adv Nurs. 2012 Dec;68(12):2674–2684. doi: 10.1111/j.1365-2648.2012.05966.x. [DOI] [PubMed] [Google Scholar]
- 40.Chavira D, Bustos C, Garcia M, Ng B, Camacho A. Delivering CBT to rural Latino children with anxiety disorders: A qualitative study. Community Ment Health J. 2015 Jun 29; doi: 10.1007/s10597-015-9903-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Primm A, Cabot D, Pettis J, Vu H, Cooper L. The acceptability of a culturally-tailored depression education videotape to African Americans. J Natl Med Assoc. 2002 Nov;94(11):1007–1016. [PMC free article] [PubMed] [Google Scholar]
- 42.Songprakun W, McCann T. Effectiveness of a self-help manual on the promotion of resilience in individuals with depression in Thailand: A randomised controlled trial. BMC Psychiatry. 2012;12:12. doi: 10.1186/1471-244X-12-12. http://bmcpsychiatry.biomedcentral.com/articles/10.1186/1471-244X-12-12 .1471-244X-12-12 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Tulbure BT, Månsson KN, Andersson G. Internet treatment for social anxiety disorder in Romania: Study protocol for a randomized controlled trial. Trials. 2012;13:202. doi: 10.1186/1745-6215-13-202. http://trialsjournal.biomedcentral.com/articles/10.1186/1745-6215-13-202 .1745-6215-13-202 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Unlü B, Riper H, van Straten A, Cuijpers P. Guided self-help on the Internet for Turkish migrants with depression: The design of a randomized controlled trial. Trials. 2010;11:101. doi: 10.1186/1745-6215-11-101. http://trialsjournal.biomedcentral.com/articles/10.1186/1745-6215-11-101 .1745-6215-11-101 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Eylem O, van Straten A, Bhui K, Kerkhof AJ. Protocol: Reducing suicidal ideation among Turkish migrants in the Netherlands and in the UK: Effectiveness of an online intervention. Int Rev Psychiatry. 2015 Feb;27(1):72–81. doi: 10.3109/09540261.2014.996121. [DOI] [PubMed] [Google Scholar]
- 46.Xu W, Wang J, Wang Z, Li Y, Yu W, Xie Q, He Li, Maercker A. Web-based intervention improves social acknowledgement and disclosure of trauma, leading to a reduction in posttraumatic stress disorder symptoms. J Health Psychol. 2015 May 1; doi: 10.1177/1359105315583371.1359105315583371 [DOI] [PubMed] [Google Scholar]
- 47.Wang Z, Wang J, Maercker A. Chinese My Trauma Recovery, a Web-based intervention for traumatized persons in two parallel samples: Randomized controlled trial. J Med Internet Res. 2013;15(9):e213. doi: 10.2196/jmir.2690. http://www.jmir.org/2013/9/e213/ v15i9e213 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Choi I, Zou J, Titov N, Dear BF, Li S, Johnston L, Andrews G, Hunt C. Culturally attuned Internet treatment for depression amongst Chinese Australians: A randomised controlled trial. J Affect Disord. 2012 Feb;136(3):459–468. doi: 10.1016/j.jad.2011.11.003.S0165-0327(11)00716-6 [DOI] [PubMed] [Google Scholar]
- 49.Ünlü Ince B, Cuijpers P, van 't Hof E, van Ballegooijen W, Christensen H, Riper H. Internet-based, culturally sensitive, problem-solving therapy for Turkish migrants with depression: Randomized controlled trial. J Med Internet Res. 2013;15(10):e227. doi: 10.2196/jmir.2853. http://www.jmir.org/2013/10/e227/ v15i10e227 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Tulbure BT, Szentagotai A, David O, Ștefan S, Månsson KN, David D, Andersson G. Internet-delivered cognitive-behavioral therapy for social anxiety disorder in Romania: A randomized controlled trial. PLoS One. 2015;10(5):e0123997. doi: 10.1371/journal.pone.0123997. http://dx.plos.org/10.1371/journal.pone.0123997 .PONE-D-14-39593 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Liu E, Chen W, Li Y, Wang C, Mok T, Huang H. Exploring the efficacy of cognitive bibliotherapy and a potential mechanism of change in the treatment of depressive symptoms among the Chinese: A randomized controlled trial. Cognit Ther Res. 2009 Oct;33(5):449–461. doi: 10.1007/s10608-008-9228-4. [DOI] [Google Scholar]
- 52.Moldovan R, Cobeanu O, David D. Cognitive bibliotherapy for mild depressive symptomatology: Randomized clinical trial of efficacy and mechanisms of change. Clin Psychol Psychother. 2013;20(6):482–493. doi: 10.1002/cpp.1814. [DOI] [PubMed] [Google Scholar]
- 53.Muto T, Hayes S, Jeffcoat T. The effectiveness of acceptance and commitment therapy bibliotherapy for enhancing the psychological health of Japanese college students living abroad. Behav Ther. 2011 Jun;42(2):323–335. doi: 10.1016/j.beth.2010.08.009.S0005-7894(11)00018-9 [DOI] [PubMed] [Google Scholar]
- 54.Naeem F, Sarhandi I, Gul M, Khalid M, Aslam M, Anbrin A, Saeed S, Noor M, Fatima G, Minhas F, Husain N, Ayub M. A multicentre randomised controlled trial of a carer supervised culturally adapted CBT (CaCBT) based self-help for depression in Pakistan. J Affect Disord. 2014 Mar;156:224–227. doi: 10.1016/j.jad.2013.10.051.S0165-0327(13)00793-3 [DOI] [PubMed] [Google Scholar]
- 55.Higgins JPT, Green S. Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0. London, UK: The Cochrane Collaboration; 2011. Mar, [2016-08-28]. Chapter 9: Analysing data and undertaking meta-analyses http://handbook.cochrane.org/ [Google Scholar]
- 56.Hollis S, Campbell F. What is meant by intention to treat analysis? Survey of published randomised controlled trials. BMJ. 1999 Sep 11;319(7211):670–674. doi: 10.1136/bmj.319.7211.670. http://europepmc.org/abstract/MED/10480822 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Titov N, Andrews G, Davies M, McIntyre K, Robinson E, Solley K. Internet treatment for depression: A randomized controlled trial comparing clinician vs technician assistance. PLoS One. 2010;5(6):e10939. doi: 10.1371/journal.pone.0010939. http://dx.plos.org/10.1371/journal.pone.0010939 . [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Search strategy.
Questionnaire for researchers.
Risk of bias analysis.
Example responses from researchers.