

Abstract
Study Objectives:
We examine the association between self-reported sleep duration and diabetes incidence in a national sample of American Indians/ Alaska Natives (AI/ANs) with prediabetes.
Methods:
Data were derived from the Special Diabetes Program for Indians Diabetes Prevention demonstration project. This longitudinal analysis included 1,899 participants with prediabetes recruited between January 1, 2006 and July 31, 2009 who reported sleep duration and completed all 16 classes of the lifestyle intervention consisting of diet, exercise, and behavior modification sessions to promote weight loss. Three years of follow-up data were included to fit Cox regression models to compute hazard ratios (HRs) for diabetes incidence across sleep duration categories.
Results:
The crude diabetes incidence rate was 4.6 per 100 person-years among short sleepers (≤ 6 h per night) compared to 3.2 among those sleeping 7 h and 3.3 among those sleeping 8 h or more. After adjustment for age and sex, short sleep (≤ 6 h vs. others) was associated with increased diabetes risk (HR 1.55 [95% confidence interval 1.11–2.17]); risk remained significantly elevated after controlling for socioeconomic characteristics, health behaviors, and health status. When adjusting for body mass index and percent weight loss, the short sleep-diabetes relationship was attenuated (HR 1.32 [95% confidence interval 0.92–1.89]). No significant long sleep-diabetes association was found. Further, short sleepers lost significantly less weight than others (3.7% vs. 4.3%, P = 0.003).
Conclusions:
Short sleep duration, but not long duration, was significantly associated with increased diabetes risk and less weight loss among AI/ANs in a lifestyle intervention. Further exploration of the complex factors underlying short sleep duration is warranted.
Citation:
Nuyujukian DS, Beals J, Huang H, Johnson A, Bullock A, Manson SM, Jiang L, Special Diabetes Program for Indians Diabetes Prevention Demonstration Project. Sleep duration and diabetes risk in American Indian and Alaska native participants of a lifestyle intervention project. SLEEP 2016;39(11):1919–1926.
Keywords: sleep, diabetes, epidemiology, American Indian/Alaska native, disparities
Significance.
Epidemiologic studies suggest a role for short and long sleep duration in diabetes risk, but racial/ethnic variation in this association has not been studied extensively. To our knowledge, this is the first study to examine the role of sleep in diabetes among AI/ANs, and does so in a large lifestyle intervention cohort to promote weight loss among AI/ANs with prediabetes. In this cohort, we found an increased risk for diabetes with short sleep duration but not with long sleep duration. In addition, short sleepers lost less weight than normal sleepers, thus benefitting less from the lifestyle intervention. This work provides evidence for the importance of emphasizing consistent, adequate sleep in lifestyle intervention to prevent diabetes.
INTRODUCTION
Adequate daily sleep is vital to human health. Yet with the evolvement of multiple social, cultural, behavioral and environmental factors, sleep deficiency in both quality and quantity is common in modern society.1 More than 30% of American adults report sleeping less than 6 hours per night.2 Lack of sleep, both short and long term, is associated with changes in physiologic, cardiovascular, and endocrine system functioning. Habitual long sleep duration is also linked to adverse health effects.2 In a review and meta-analysis, when compared to those sleeping the usual 7 to 8 hours per night, short sleep duration (generally < 7 h) has been associated with a 12% higher risk of death and long sleep duration (commonly > 8 or 9 h) with a 30% higher risk of death.1 Epidemiologic studies show that duration and quality of sleep are related to a spectrum of chronic health conditions including cardiovascular disease,3 hypertension,4 and obesity.5
Sleep duration is related to type 2 diabetes,6 a striking public health challenge which poses enormous economic burden.7 Recent meta-analyses reveal that both short and long duration of sleep are significantly associated with increased risk of type 2 diabetes; the lowest risk occurs at 7 to 8 h of sleep daily.8,9 Substantial racial/ethnic disparities are evident with respect to both sleep duration10 and type 2 diabetes.11 Thus this relationship has been studied in poor, racially and ethnically underserved populations. Analyses of 2004–2011 data drawn from the US National Health Interview Survey describe a U-shaped association between sleep duration and diabetes prevalence among both black and white adults.12 Another analysis focusing on just the 2005 data from this same source shows that the U-shaped association is even more pronounced among blacks.13 A much smaller study of a US multiethnic cohort reports an increased risk of diabetes with short sleep duration among Hispanics.14 In a recent investigation focusing on women, short and long sleep duration is found to be associated with diabetes prevalence among Filipinas, but not their white or black counterparts.15 Clearly, despite some inconsistencies in these findings, potential racial/ethnic variation in this association warrants continued attention.
The prevalence of type 2 diabetes is alarmingly high among American Indians and Alaska Natives (AI/AN); at 15.9%, it is more than twice that of non-Hispanic whites.11 Based on a recent cross-sectional analysis, AI/ANs also exhibit a higher prevalence of frequent insufficient sleep than their non-Hispanic white counterparts.16 However, research on sleep in this population is limited and, to the best of our knowledge, the relationship between sleep and diabetes incidence has never been previously examined among AI/ANs. In this article, we examine the relationship between sleep duration and diabetes incidence among a national sample of AI/ANs with prediabetes who participated in a lifestyle intervention that focused on weight loss promotion.17 Furthermore, we evaluate the relationship of sleep duration with clinical and behavioral outcomes of lifestyle intervention, such as weight loss, diet, blood pressure, and dyslipidemia.
METHODS
Study Population
The data are derived from a lifestyle intervention designed to prevent diabetes among AI/ANs known as the Special Diabetes Program for Indians Diabetes Prevention Demonstration Project (SDPI-DP), which is described in detail elsewhere.17,18 Funded by congressional mandate, the SDPI-DP assessed the feasibility of translating a lifestyle intervention to prevent diabetes among diverse AI/AN communities. Thirty-six health care programs serving 80 tribes in 18 states and 11 Indian Health Service (IHS) administrative areas participated in the SDPI-DP. These programs included seven urban Indian health programs located within non-profit Native organizations that receive IHS funding for health services in urban areas. These programs implemented the 16-session Lifestyle Balance Curriculum adopted from the Diabetes Prevention Program19 and evaluated its effectiveness over a 3-y period. After a baseline assessment, enrollees participated in the lifestyle curriculum consisting of diet, exercise, and behavior modification sessions to reach and maintain a weight reduction of at least 7% of initial body weight. Participants were encouraged to follow a lowfat, low-calorie diet and to increase moderate physical activity to at least 150 min weekly. Cultural adaptation, such as talking circles or indigenous foods, was permitted as long as the basic information of the curriculum was maintained. The curriculum was provided in group settings within 16 to 24 weeks after baseline and typically was taught by a local program dietitian and/or health educator.
Eligible participants had to be AI/AN (eligible to receive IHS services), at least 18 y of age, without a previous diabetes diagnosis, and have either impaired fasting glucose (IFG) (fasting blood glucose [FBG] level of 100–125 mg/dL and an oral glucose tolerance test [OGTT 2-h glucose] result < 200 mg/dL) or impaired glucose tolerance (IGT) (an OGTT 2-h glucose result of 140–199 mg/dL 2 h after a 75-g oral glucose load and an FBG level < 126 mg/dL). Enrollment started in January 2006; by July 31, 2009, 3,312 participants who met the eligibility criteria were recruited and began the intervention. Participants who completed all 16 classes of the lifestyle curriculum, had at least one follow-up assessment for diabetes status, and reported sleep duration at baseline were included in the primary analyses (n = 1,899). We limited the study cohort to those who completed all intervention sessions in order to obtain a homogenous group of participants in terms of intervention exposure. Moreover, among those who did not complete all 16 classes, loss to follow-up rates were significantly higher which, if analyzed separately, would have resulted in analyses that were underpowered.
The SDPI-DP protocol was approved by the institutional review board of the University of Colorado Anschutz Medical Center and the National Indian Health Service institutional review board. When required, grantees obtained approval from other entities charged with overseeing research in their programs (e.g., tribal review boards). All participants provided written informed consent and Health Insurance Portability and Accountability Act authorization.
Measures
Diabetes Incidence
At baseline, within 1 mo of completing the last Diabetes Prevention Program (DPP) class (usually 4 to 6 mo after baseline, hereafter called the postcurriculum assessment), and annually after baseline for up to 3 y, participants underwent a comprehensive clinical assessment to evaluate diabetes risk and incidence. The primary outcome, incident diabetes, was diagnosed by an annual OGTT or a semiannual FBG test conducted in local or regional laboratories. The diagnosis was made according to the 2004 American Diabetes Association criteria: an FBG ≥ 126 mg/dL or a 2-h test result ≥ 200 mg/dL after a 75-g oral glucose load. In addition to the semiannual measurements, FBG was measured if symptoms suggestive of diabetes developed. The diagnosis was usually confirmed by a second test, generally within 6 weeks of the first test, or was confirmed by a provider based on clinical judgment.
Sleep Duration
Sleep duration was obtained by self-report in the baseline participant questionnaire. Participants answered the question: “How many hours a night do you sleep, on average?” with one of the following 10 options: ≤ 3, 4, 5, 6, 7, 8, 9, 10, 11, or ≥ 12 h. The sleep duration of each participant was categorized as 6 or fewer hours (labeled “short sleepers”), 7 and ≥ 8 h (“long sleepers”). We chose a reference group of 7 hours to be consistent with relevant literature8,9 and because it was the category associated with the lowest diabetes incidence among all 10 categories of our original sleep variable.
Sociodemographic Characteristics and Health Behaviors
The questionnaire also encompassed sociodemographic characteristics and health-related behavior.18 Sociodemographic measures included age, sex, educational attainment, marital status, annual household income, and employment status.
Health behaviors, assessed at baseline and in subsequent follow-up questionnaires, included smoking status, alcohol use, physical activity, and diet information. Smoking history and current smoking status were obtained using items from a previous epidemiologic study among AI/ANs.20 Alcohol use was measured with the Alcohol Use Disorders Identification Test (AUDIT).21 Weekly physical activity was recorded via the Rapid Assessment of Physical Activity (RAPA1).22 The RAPA1 is a seven-item instrument covering a range of weekly aerobic physical activity levels. The response indicating the highest activity level was used to categorize participants into one of five levels of physical activity. Diet information was acquired using a set of culturally adapted questions for self-reported frequency of eating a variety of foods,23 with responses for each question ranging from 1 (less than once a month) to 6 (more than once a day). The healthy diet score was the average frequency of consuming six kinds of relatively healthy foods (e.g., whole grain bread, vegetables), whereas the unhealthy diet score was the mean of 12 questions about relatively unhealthy foods (e.g., bacon or sausage, regular soft drinks/soda, fast food).
Clinical Characteristics
At each clinical assessment, a grantee staff member measured the participant's weight, height (shoeless, in light clothing), and blood pressure. Laboratory assays of FBG, OGTT 2-h glucose, high-density lipoprotein cholesterol, low-density lipo-protein cholesterol, and triglycerides were conducted in local or regional laboratories after 9 to 12 h of fasting following standardized protocols. A self-administered comorbidity questionnaire24 assessed the following conditions: prediabetes, heart disease, high blood pressure, lung disease, ulcer or stomach disease, kidney disease, liver disease, anemia or other blood disease, history of cancer, depression, osteoarthritis, back pain, and rheumatoid arthritis. Finally, the general health status item from the Medical Outcomes Study Short Form-12 (SF-12)25 indexed the general health of each participant. Based on the distribution of the data, some categories were combined and treated as a three-category variable: poor or fair, good, very good or excellent.
Statistical Analysis
Baseline characteristics were compared among different categories of sleep duration using χ2 tests for categorical variables and analysis of variance tests for continuous variables. To determine the association between sleep duration and diabetes risk in SDPI-DP participants, hazard ratios (HR) and 95% confidence intervals (CI) were calculated using Cox proportional hazards regression models. We began with a model including only sleep duration (model 0), and then purposefully entered groups of covariates: age and sex were added to model 1; socioeconomic characteristics to model 2; behavioral characteristics to model 3; self-reported health status (comorbidi-ties and general health status) to model 4; body mass index (BMI) to model 5; and percent weight loss at postcurriculum assessment to model 6. The proportional hazards assumptions were checked by including an interaction term between each covariate and log of follow-up time. None of those interaction terms were statistically significant, indicating no violation of the assumption.
Missing data were uncommon for most of the independent variables included in these analyses (≤ 5%) except income and marital status (20% and 16%, respectively). Fewer than 3% of participants (n = 55) had missing data for sleep duration and were excluded from the main analysis. Yet, in final multivariate regression models without imputation, about one-third of the observations were excluded due to missing data on other covariates. To avoid potential bias caused by excluding incomplete cases and to maximize the power of the analysis, a multiple imputation method was used to address missing data in the baseline independent variables (income, education, marital status, RAPA1, unhealthy diet, AUDIT, smoking, self-administered comorbidity index, general health status, BMI). The multiple imputations were performed using IVEware software developed by the University of Michigan Survey Methodology Center.26 The results were then combined using the SAS MIANALYZE procedure to obtain the proper estimate for the standard error for each parameter of interest.
Various sensitivity analyses evaluated the robustness of our conclusions with respect to missing data and other assumptions. First, the analyses were repeated with complete cases only (i.e., excluding the participants with missing data on any of the covariates). A sensitivity analysis was subsequently performed using 6 to 8 h of sleep as the reference group, to allow for comparison with previous studies that defined the reference group in this manner.6 Finally, the analyses were repeated using data from all participants without consideration for the number of DPP classes attended. All data analyses were conducted using SAS 9.3 (SAS Institute Inc., Cary, NC).
RESULTS
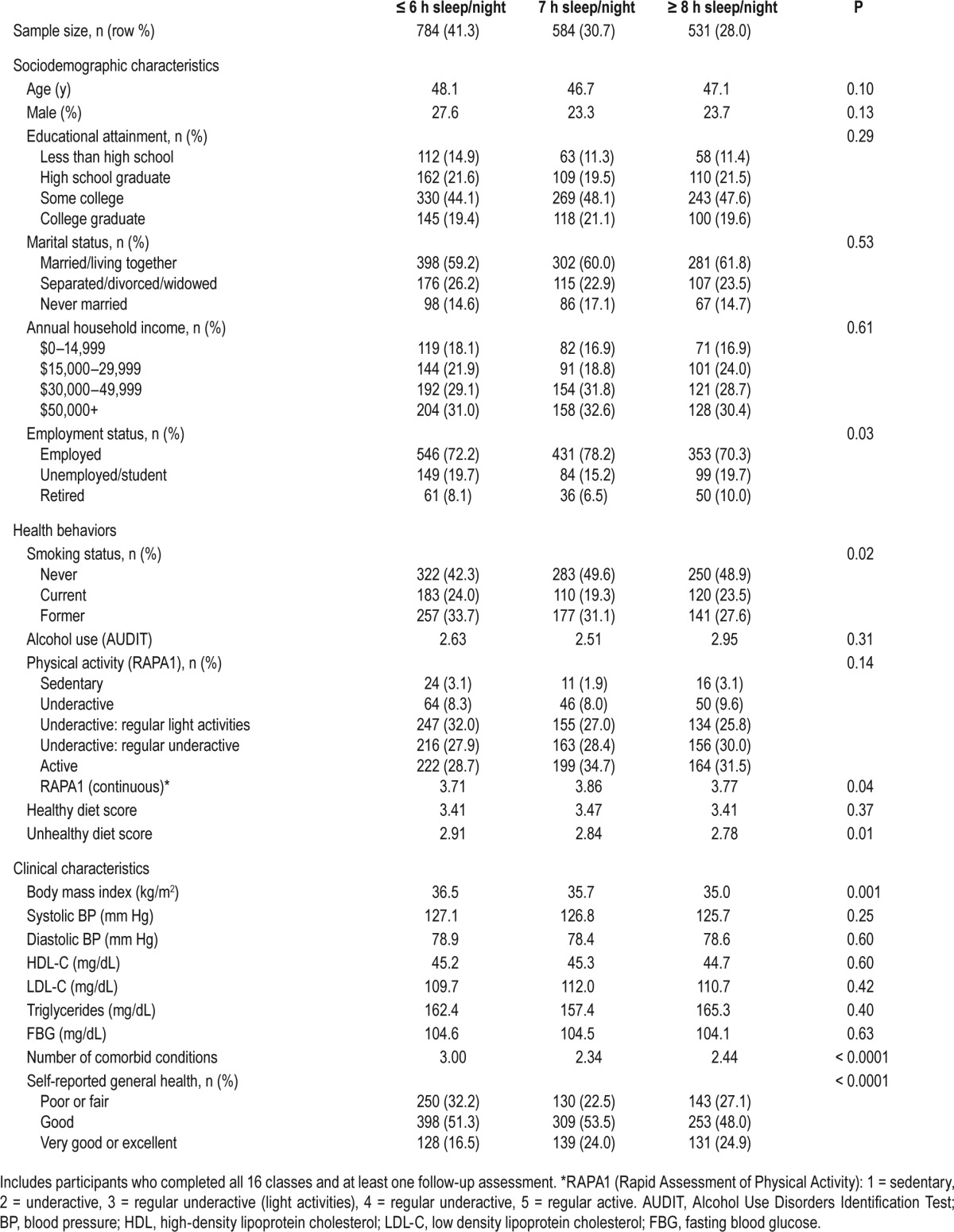
Table 1 presents the baseline sociodemographic, health behavioral, and clinical characteristics of SDPI-DP participants who completed all 16 classes and who had at least one follow-up assessment, stratified by reported baseline sleep duration. Short sleepers reported lower rates of having never smoked than those who reported 7 h or more of sleep per night (42.3% vs. 49.6% and 48.9% respectively, P = 0.02). Lower levels of physical activity, based on the continuous rapid assessment of physical activity (RAPA1), were linked to short and long sleep (P = 0.04). Unhealthy diet consumption (P = 0.01) and higher BMI (P = 0.001) were associated with short sleep duration. In addition, short sleepers reported a higher number of comorbidities than either the reference group or long sleepers (3.00 vs. 2.34 and 2.44 respectively, P < 0.0001). Short sleepers were also significantly less likely to report very good or excellent health status (P < 0.0001).
Table 1.
Baseline sociodemographic, health behavioral, and clinical characteristics by baseline self-reported sleep duration in the Special Diabetes Program for Indians Diabetes Prevention Demonstration Project.
On average, participants were followed for about 2 y (range: 6 mo to 3 y); baseline short sleepers had the lowest completion rates for the first two annual assessments and the shortest average follow-up duration. After completing the DPP curriculum, mean sleep duration increased about 30 min among short sleepers and decreased about 30 min among long sleepers. However, the average change in sleep duration was less than 10 min among those who reported 7 h of sleep per night at baseline (Table 2).
Table 2.
Follow-up completion rates and change in sleep duration in the Special Diabetes Program for Indians Diabetes Prevention Demonstration Project.
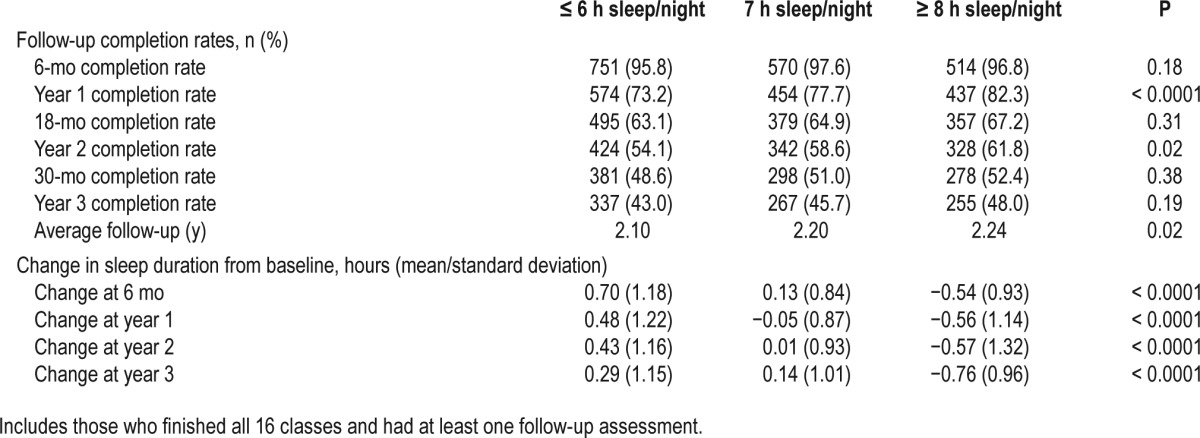
Table 3 presents diabetes incidence and HRs for diabetes by baseline sleep duration, obtained through the Cox models. The analyses initially were based on the three-category sleep variable (short, 7 h, and long); however, as seen on the right side of Table 3, because no differences were found between the 7-h and the ≥ 8 h sleep groups, we created a two-category sleep variable (≤ 6 h vs. ≥ 7 h) for the analysis (left side of Table 3). Among those with 6 h or fewer of sleep per night, 91 participants reported diabetes and the crude diabetes rate was 4.6 per 100 person-years (95% CI 3.7–5.7). Among those with 7 h or more of sleep per night, the crude diabetes rate was 3.2 per 100 person-years (95% CI 2.6–3.9) (93 incident diabetes cases). After adjusting for age and sex, compared to those with 7 h or more of sleep per night, the short sleepers were significantly more likely to have a diabetes diagnosis (HR 1.55 [95% CI 1.11–2.17]). The association remained statistically significant after adjustment for socioeconomic characteristics, health behaviors, and health status. In model 5, which included BMI at baseline, the relationship was attenuated and was no longer statistically significant (HR 1.39 [95% CI 0.99–1.96]). In model 6, which added percent weight loss at the postcurriculum assessment, the relationship was further attenuated (HR 1.32 [95% CI 0.92–1.89]).
Table 3.
Diabetes cases and hazard ratios with 95% confidence interval, by baseline self-reported sleep duration, in the Special Diabetes Program for Indians Diabetes Prevention Demonstration Project.
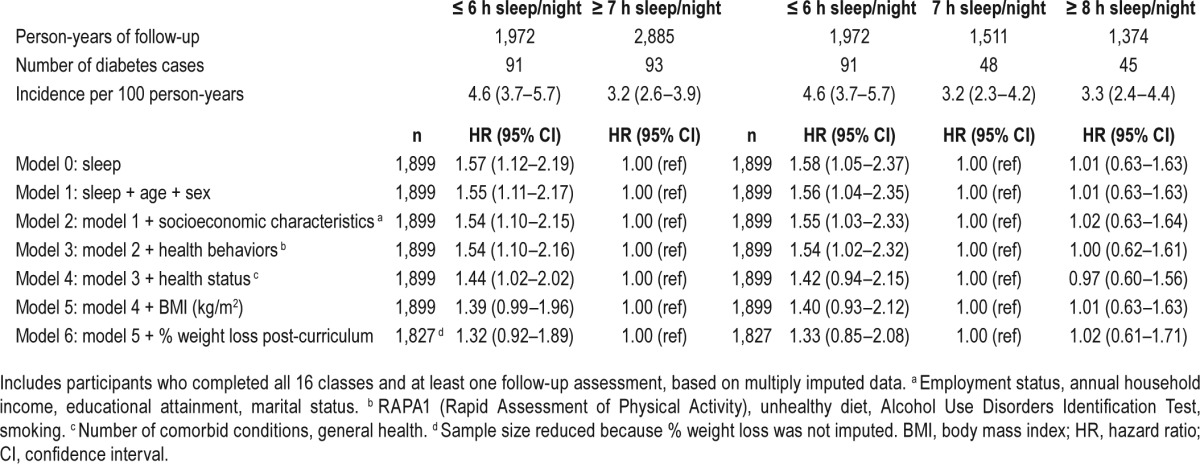
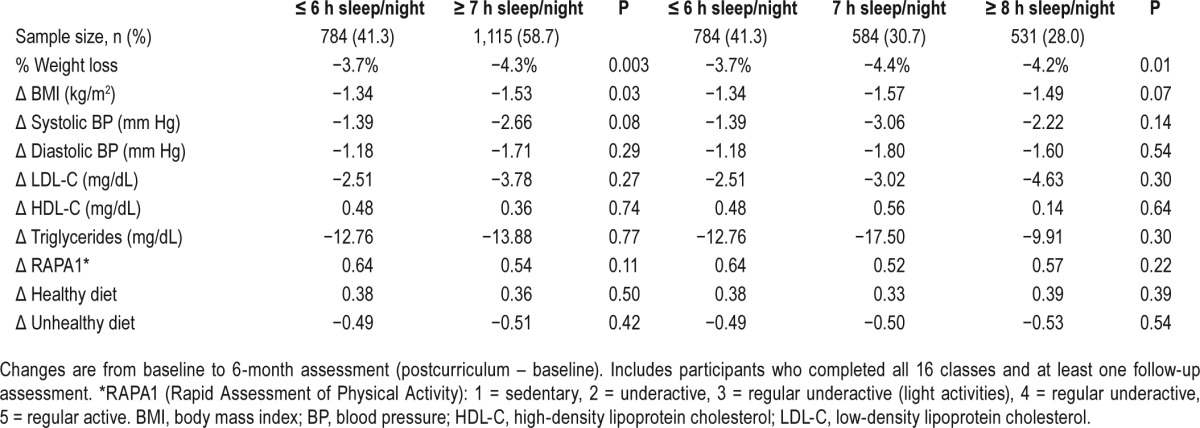
Table 4 presents postcurriculum changes in other clinical and behavioral outcomes of the lifestyle intervention by baseline sleep duration. Participants with 7 h or more of sleep lost significantly more weight (−4.3% vs. −3.7%, P = 0.003) and experienced greater reduction in BMI (−1.53 vs. −1.34, P = 0.03) than short sleepers. Those with adequate sleep had marginally significant greater reductions in systolic blood pressure compared to short sleepers (−2.66 vs. −1.39 mm Hg, P = 0.08). Long sleep, in general, was not significantly associated with changes in clinical or behavioral outcomes; no significant differences in changes of diet or physical activity levels were observed among the groups.
Table 4.
Changes in intervention outcome variables, by baseline self-reported sleep duration, in the Special Diabetes Program for Indians Diabetes Prevention Demonstration Project.
Examining complete cases only, the sensitivity analysis revealed that the association between short sleep duration and diabetes was even stronger after adding sociodemographic characteristics into the model (HR 1.86 [95% CI 1.21–2.83]; Table S1 in the supplemental material). The results of analyses using 6 to 8 h of sleep as the reference group were very similar to those in our main analysis: the HRs for short sleep were slightly reduced with somewhat wider CIs, likely due to reduced sample size of the short sleeper group and the fact that diabetes risk for those with 6 h of sleep was also elevated (Table S2 in the supplemental material). Finally, when repeating the analyses using data from all SDPI-DP participants (n = 3,312), the HR estimates were slightly reduced but all the major conclusions remained the same (data not shown).
DISCUSSION
Among the AI/AN participants in this lifestyle intervention program, short sleep duration was associated with a significantly increased risk of diabetes incidence. This result is consistent with most findings specific to other race/ethnicity groups in previous studies.6,8,9,12–14 However, no significant association was observed between long sleep duration and incident diabetes. Participation in the lifestyle intervention may partially explain this lack of association. In the context of lifestyle intervention, our findings are consistent with those from the intervention arm of a Finnish lifestyle intervention trial.27 In that study, the increased hazard found among long sleepers in the control group was not present in the intervention group (adjusted HR = 2.74 and 0.73 for the control and lifestyle intervention group, respectively), while a nonsignificant increased risk for diabetes was observed among short sleepers in both groups (adjusted HR = 1.68 and 1.44 for the control and lifestyle intervention group, respectively). The authors speculated that the lack of significance in the association between short sleep and incident diabetes might have been due to limited statistical power, with a total sample size of 522. Conversely, lifestyle intervention might mitigate the potential effect of long sleep duration on diabetes risk, indicated by a much smaller hazard ratio of long sleep duration with respect to incident diabetes in the intervention group. It is also worth noting that the mean sleep duration decreased among SDPI-DP long sleepers and increased in the short sleepers following the intervention. These observations are also similar to those in the intervention group of the Finnish Diabetes Prevention Study,27 which were in contrast to the directions of changes in sleep duration among their controls.
Several important conclusions can be drawn from the baseline association between sleep duration and participant characteristics of this study. First, more than 40% of SDPIDP participants reported ≤ 6 h of sleep per night, providing evidence that insufficient sleep may be a prevalent issue within the AI/AN population with prediabetes. Our site staff suggests that difficulty with work-life balance and struggles to handle multiple jobs might be reasons for the high prevalence of shortened sleep duration. Second, as well documented elsewhere,28,29 short sleepers were found to have lower rates of never smoking and higher BMI. A significant lower level of daytime physical activity has been previously linked to sleep restriction,30 which was also observed based on RAPA1 levels in the present analyses. Moreover, extensive epidemiologic evidence supports the view that diet and sleep are intertwined. Consistent with our baseline data, previous cross-sectional studies have shown that individuals who slept less were less likely to eat fruits and vegetables, snacked more often, ate a higher proportion of carbohydrate-rich or fatty foods, and had more irregular meal patterns.31
Short sleep duration is believed to influence diabetes through hormonal and glycemic factors.9 For example, reduced sleep duration has been associated with decreased leptin and elevated ghrelin levels, thereby altering appetite regulation and increasing hunger.32 In addition, circadian misalignment and sleep apnea, which unfortunately were not measured in SDPI-DP, have been related to low insulin sensitivity or insulin resistance and increased diabetes risk.33,34 Had we been able to adjust for it in our models, we expect that sleep apnea would have further attenuated the short sleep-diabetes relationship we report. Recently, the Look AHEAD study reported signifi-cant weight loss and, correspondingly, substantial improvements in the apnea-hypopnea index maintained through 4 y among diabetes patients participating in a lifestyle intervention.35 The importance of weight loss in diabetes prevention has already been established.36 Attenuation of the sleep/diabetes relationship when percent weight loss was included in our analyses further accentuates the critical role of weight loss in diabetes prevention.
Associations between long sleep duration and diabetes are still not well understood. However, unlike the biologic mechanisms that appear to underlie the association between short sleep and diabetes, the long sleep association may be at least partially explained by depression, psychiatric disorder, or other psychosocial factors.37 In our lifestyle intervention, stress management may play a role in reducing the effect of long sleep on diabetes. As the association between long sleep duration and diabetes risk is still speculative and potentially confounded by other psychosocial factors, the lack of a relationship between long sleep duration and incident diabetes in our study suggests that the mechanisms driving the previously observed associations warrant additional inquiry.
This study is unique for several reasons. It is the first study that revealed high prevalence of short sleep duration in a large sample of AI/ANs at high risk for type 2 diabetes. Further, to our knowledge, the role of sleep duration in diabetes risk among AI/ANs has not been previously explored. In addition, many previous studies of sleep duration and diabetes were conducted using observational longitudinal cohorts or cross-sectional studies. The context of this study allowed us to examine the effects of sleep duration on lifestyle intervention outcomes. That short sleepers lost significantly less weight in SDPI-DP highlights the potential importance of adequate sleep for at-risk individuals to benefit fully from a lifestyle intervention to prevent diabetes. Adding a session focusing on the need for good sleep habits in the Lifestyle Balance Curriculum is likely to enhance the curriculum and benefit this population greatly.
It should be noted, however, that although short sleep duration appears to be a causal factor for increased diabetes risk,9 it could also be a marker for other underlying health conditions and/or life stressors. Chronic conditions, including chronic pain, have been shown to affect sleep duration and/or quality.38 Meanwhile, various stressors including shift work,39 multiple jobs, and disadvantaged neighborhood environment40 may also contribute to sleep problems. Therefore, while encouraging better sleep habits is a logical addition to lifestyle intervention, it might be equally important to identify the causes of shortened sleep and address them individually while implementing the intervention.
Limitations of this study need to be acknowledged. First, only a small number of incident diabetes cases were identified in this sample during the relatively short follow-up period (maximum 3 y). Second, the data specific to sleep duration were obtained via self-report and are subject to measurement error; additionally, no data were available regarding sleep quality, which has also been independently associated with increased diabetes risk.9 Third, the lack of a control group in SDPI-DP, which, while typical for translational projects of this nature, precluded comparison to a group of AI/ANs not undergoing intervention. Last, though missing data were addressed using multiple imputations, this strategy required us to assume that the data in question were missing at random. In the current study, we found attrition to be more common among short sleepers (Table 2), implying that the missing at random assumption may not be completely valid. However, shorter follow-up duration among short sleepers also means that we might have observed more incident diabetes cases in this group had we followed them longer, which suggests our estimate for the association between short sleep and diabetes may be conservative.
In summary, short sleep duration—but not long sleep duration—was associated with increased risk of diabetes among the SDPI-DP participants. These findings add to the growing body of evidence that points to the role of sleep duration in diabetes risk and suggest that future preventive interventions may need to include a component to emphasize consistent, adequate sleep. Further work along these lines may clarify the role of sleep duration in diabetes risk, elucidate the underlying mechanisms of this association, and advance our understanding of possible racial/ethnic variation in this regard.
DISCLOSURE STATEMENT
This was not an industry-supported study. Funding for the SDPI-DP project was provided by the Indian Health Service (HHSI242200400049C, S.M. Manson). Manuscript preparation was supported in part by the American Diabetes Association (ADA #7-12-CT-36, L. Jiang), and the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK; 1P30DK092923, S.M. Manson). The authors have indicated no financial conflicts of interest. There is no use of off-label or investigational agents in this study.
ACKNOWLEDGMENTS
Grant programs participating in the Special Diabetes Program for Indians Diabetes Prevention Program: Confederated Tribes of the Chehalis Reservation, Cherokee Nation, Cheyenne River Sioux Tribe, the Chickasaw Nation, Coeur d'Alene Tribe, Colorado River Indian Tribes, Colville Confederated Tribes, Cow Creek Band of Umpqua Tribe, Fond du Lac Reservation, Gila River Health Care, Haskell Health Center, Ho-Chunk Nation, Indian Health Board of Minneapolis, Urban Native Diabetes Prevention Consortium, Kenaitze Indian Tribe IRA, Lawton IHS Service Unit, Menominee Indian Tribe of Wisconsin, Mississippi Band of Choctaw Indians, Norton Sound Health Corporation, Pine Ridge IHS Service Unit, Pueblo of San Felipe, Quinault Indian Nation, Rapid City IHS Diabetes Program, Red Lake Comprehensive Health Services, Rocky Boy Health Board, Seneca Nation of Indians, Sonoma County Indian Health Project, South East Alaska Regional Health Consortium, Southcentral Foundation, Trenton Indian Service Area, Tuba City Regional Health Care Corporation, United American Indian Involvement, Inc., United Indian Health Services, Inc., Warm Springs Health & Wellness Center, Winnebago Tribe of Nebraska, Zuni Pueblo.
The authors express our gratitude to the Indian Health Service as well as tribal and urban Indian health programs and participants involved in the Special Diabetes Program for Indians Diabetes Prevention Program.
Author contributions: Daniel S. Nuyujukian researched the data, wrote, reviewed, and edited the manuscript. Janette Beals participated in the design of the SDPI-DP project, contributed to the discussion, reviewed and edited the manuscript. Haixiao Huang researched the data, performed data analysis, reviewed and edited the manuscript. Ann Johnson and Ann Bullock contributed to the discussion, reviewed and edited the manuscript. Spero M. Manson conceptualized and designed the SDPI-DP project, contributed to the discussion, reviewed and edited the manuscript. Luohua Jiang designed the study, researched the data, contributed to the discussion, reviewed and edited the manuscript. Luohua Jiang is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
REFERENCES
- 1.Cappuccio FP, D'Elia L, Strazzullo P, Miller MA. Sleep duration and all-cause mortality: a systematic review and meta-analysis of prospective studies. Sleep. 2010;33:585–92. doi: 10.1093/sleep/33.5.585. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Alvarez GG, Ayas NT. The impact of daily sleep duration on health: a review of the literature. Prog Cardiovasc Nurs. 2004;19:56–9. doi: 10.1111/j.0889-7204.2004.02422.x. [DOI] [PubMed] [Google Scholar]
- 3.Meisinger C, Heier M, Löwel H, Schneider A, Döring A. Sleep duration and sleep complaints and risk of myocardial infarction in middle-aged men and women from the general population: the MONICA/KORA Augsburg Cohort Study. Sleep. 2007;30:1121–7. doi: 10.1093/sleep/30.9.1121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Gottlieb DJ, Redline S, Nieto FJ, et al. Association of usual sleep duration with hypertension: the Sleep Heart Health Study. Sleep. 2006;29:1009–14. doi: 10.1093/sleep/29.8.1009. [DOI] [PubMed] [Google Scholar]
- 5.Marshall NS, Glozier N, Grunstein RR. Is sleep duration related to obesity? A critical review of the epidemiological evidence. Sleep Med Rev. 2008;12:289–98. doi: 10.1016/j.smrv.2008.03.001. [DOI] [PubMed] [Google Scholar]
- 6.Ayas NT, White DP, Al-Delaimy WK, et al. A prospective study of sleep duration and incident diabetes in women. Diabetes Care. 2003;26:380–4. doi: 10.2337/diacare.26.2.380. [DOI] [PubMed] [Google Scholar]
- 7.Arredondo A. Diabetes: a global challenge with high economic burden for public health systems and society. Am J Public Health. 2013;103:e1–e2. doi: 10.2105/AJPH.2012.301106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Shan Z, Ma H, Xie M, et al. Sleep duration and risk of type 2 diabetes: a meta-analysis of prospective studies. Diabetes Care. 2015;38:529–37. doi: 10.2337/dc14-2073. [DOI] [PubMed] [Google Scholar]
- 9.Cappuccio FL, D'Elia L, Strazzullo P, Miller MA. Quantity and quality of sleep and incidence of type 2 diabetes: a systematic review and meta-analysis. Diabetes Care. 2010;33:414–20. doi: 10.2337/dc09-1124. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Grandner MA, Williams N, Knutson KL, Roberts D, Jean-Louis G. Sleep disparity, race/ethnicity, and socioeconomic position. Sleep Med. 2016;18:7–18. doi: 10.1016/j.sleep.2015.01.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Centers for Disease Control and Prevention. 2014 National Diabetes Statistics Report, 2014. [Accessed January 20, 2015]. Available from http://www.cdc.gov/diabetes/pubs/statsreport14/national-diabetes-report-web.pdf.
- 12.Jackson CL, Redline S, Kawachi I, Hu FB. Association between sleep duration and diabetes in black and white adults. Diabetes Care. 2013;36:3557–65. doi: 10.2337/dc13-0777. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Zizi F, Pandey A, Murray-Bachmann R, et al. Race/ethnicity, sleep duration, and diabetes mellitus: analysis of the National Health Interview Survey. Am J Med. 2012;125:162–7. doi: 10.1016/j.amjmed.2011.08.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Beihl DA, Liese AD, Haffner SM. Sleep duration as a risk factor for incident type 2 diabetes in a multiethnic cohort. Ann Epidemiol. 2009;19:351–7. doi: 10.1016/j.annepidem.2008.12.001. [DOI] [PubMed] [Google Scholar]
- 15.Shadyab AH, Kritz-Silverstein D, Laughlin GA, Wooten WJ, Barrett-Connor E, Araneta MRG. Ethnic-specific associations of sleep duration and daytime napping with prevalent type 2 diabetes in postmenopausal women. Sleep Med. 2015;16:243–9. doi: 10.1016/j.sleep.2014.11.010. [DOI] [PubMed] [Google Scholar]
- 16.Chapman DP, Croft JB, Liu Y, Perry GS, Presley-Cantrell LR, Ford ES. Excess frequent insufficient sleep in American Indians/Alaska Natives. J Environ Public Health. 2013:259645. doi: 10.1155/2013/259645. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Jiang L, Manson SM, Beals J, et al. Translating the Diabetes Prevention Program into American Indian and Alaska Native Communities: results from the Special Diabetes Program for Indian Diabetes Prevention demonstration project. Diabetes Care. 2013;36:2027–34. doi: 10.2337/dc12-1250. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Jiang L, Manson SM, Dill EJ, et al. Participant and site characteristics related to participant retention in a diabetes prevention translational project. Prev Sci. 2015;16:41–52. doi: 10.1007/s11121-013-0451-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Knowler WC, Barrett-Connor E, Fowler SE, et al. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med. 2002;346:393–403. doi: 10.1056/NEJMoa012512. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Henderson PN, Jacobsen C, Beals J the AI-SUPERPFP Team. Correlates of cigarette smoking among selected Southwest and Northern Plains tribal groups: the AI-SUPERPFP study. Am J Public Health. 2005;95:867–72. doi: 10.2105/AJPH.2004.050096. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Reinert DF, Allen JP. The alcohol use disorders identification test (AUDIT): a review of recent research. Alcohol Clin Exp Res. 2002;26:272–9. [PubMed] [Google Scholar]
- 22.Topolski TD, LoGerfo J, Patrick DL, Williams B, Walwick J, Patrick MB. The rapid assessment of physical activity (RAPA) among older adults. Prev Chronic Dis. 2006;3:A118. [PMC free article] [PubMed] [Google Scholar]
- 23.Teufel-Shone NI, Jiang L, Beals J, et al. Demographic characteristics and food choices of participants in the Special Diabetes Program for American Indians Diabetes Prevention Demonstration Project. Ethnic Health. 2015;20:327–40. doi: 10.1080/13557858.2014.921890. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Sangha O, Stucki G, Liang MH, Fossel AH, Katz JN. The self-administered comorbidity questionnaire: a new method to assess comorbidity for clinical and health services research. Arthritis Rheum. 2003;49:156–63. doi: 10.1002/art.10993. [DOI] [PubMed] [Google Scholar]
- 25.Ware JE, Kosinski M, Keller SD. A 12-item short-form health survey: construction of scales and preliminary tests of reliability and validity. Medical Care. 1996;34:220–33. doi: 10.1097/00005650-199603000-00003. [DOI] [PubMed] [Google Scholar]
- 26.Raghunathan TE, Solenberger PW, Hoewyk JV. IVEware: Imputation and Variance Estimation Software. [Accessed February 17, 2012]. Available from: http://www.isr.umich.edu/src/smp/ive/
- 27.Tuomilehto H, Peltonen M, Partinen M, et al. Sleep duration, lifestyle intervention, and incidence of type 2 diabetes in impaired glucose tolerance: the Finnish Diabetes Prevention Study. Diabetes Care. 2009;32:1965–71. doi: 10.2337/dc08-1980. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Schoenborn CA, Adams PF. Sleep duration as a correlate of smoking, alcohol use, leisure-time physical inactivity, and obesity among adults: United States, 2004-2006. Centers for Disease Control and Prevention NCHS Health E-stat, 2010. [Accessed April 23, 2015]. Available from http://www.cdc.gov/nchs/data/hestat/sleep04-06/sleep04-06.htm.
- 29.Moraes W, Poyares D, Zalcman I, et al. Association between body mass index and sleep duration assessed by objective methods in a representative sample of the adult population. Sleep Med. 2013;14:312–8. doi: 10.1016/j.sleep.2012.11.010. [DOI] [PubMed] [Google Scholar]
- 30.Schmid SM, Hallschmid M, Jauch-Chara K, et al. Short-term sleep loss decreases physical activity under free-living conditions but does not increase food intake under time-deprived laboratory conditions in healthy men. Am J Clin Nutr. 2009;90:1476–82. doi: 10.3945/ajcn.2009.27984. [DOI] [PubMed] [Google Scholar]
- 31.Peuhkuri K, Sihvola N, Korpela R. Diet promotes sleep duration and quality. Nutr Res. 2012;32:309–19. doi: 10.1016/j.nutres.2012.03.009. [DOI] [PubMed] [Google Scholar]
- 32.Spiegel K, Tasali E, Penev P, Van Cauter E. Brief communication: sleep curtailment in healthy young men is associated with decreased leptin levels, elevated ghrelin levels, and increased hunger and appetite. Ann Intern Med. 2004;141:846–50. doi: 10.7326/0003-4819-141-11-200412070-00008. [DOI] [PubMed] [Google Scholar]
- 33.Eckel RH, Depner CM, Perreault L, et al. Morning circadian misalignment during short sleep duration impacts insulin sensitivity. Curr Biol. 2015;25:3004–10. doi: 10.1016/j.cub.2015.10.011. [DOI] [PubMed] [Google Scholar]
- 34.Zizi F, Jean-Louis G, Brown CD, Ogedegbe G, Boutin-Foster C, McFarlane SI. Sleep duration and risk of diabetes mellitus: epidemiologic evidence and pathophysiologic insights. Curr Diab Rep. 2010;10:43–7. doi: 10.1007/s11892-009-0082-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Kuna ST, Reboussin DM, Borradaile KE, et al. Long-term effect of weight loss on obstructive sleep apnea severity in obese patients with type 2 diabetes. Sleep. 2013;36:641–9. doi: 10.5665/sleep.2618. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Hamman RF, Wing RR, Edelstein SL, et al. Effect of weight loss with lifestyle intervention on risk of diabetes. Diabetes Care. 2006;29:2102–7. doi: 10.2337/dc06-0560. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Buxton OM, Marcelli E. Short and long sleep are positively associated with obesity, diabetes, hypertension, and cardiovascular disease among adults in the United States. Soc Sci Med. 2010;71:1027–36. doi: 10.1016/j.socscimed.2010.05.041. [DOI] [PubMed] [Google Scholar]
- 38.McCracken LM, Iverson GL. Disrupted sleep patterns and daily functioning in patients with chronic pain. Pain Res Manag. 2002;7:75–9. doi: 10.1155/2002/579425. [DOI] [PubMed] [Google Scholar]
- 39.Åkerstedt T, Wright KP. Sleep loss and fatigue in shift work and shift work disorder. Sleep Med Clin. 2009;4:257–71. doi: 10.1016/j.jsmc.2009.03.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Hill TD, Burdette AM, Hale L. Neighborhood disorder, sleep quality, and psychological distress: testing a model of structural amplification. Health Place. 2009;15:1006–13. doi: 10.1016/j.healthplace.2009.04.001. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.