

Abstract
Adrenal adenomas usually show 18F-FDG activity less than that of the liver parenchyma. However, lipid-poor and hormone-secreting adenomas have been reported to show mild 18F-FDG avidity. We report on a 51-year-old female with clinical symptoms of hypercortisolemia and a large right adrenal mass detected on CT. Post-contrast CT images showed an enhancing focus in the lower pole of the mass, with corresponding markedly increased activity on 18F-FDG PET/CT. Right adrenalectomy was performed and histology revealed a benign adenoma, indicating that functioning benign adenomas can show intensely increased metabolic activity on 18F-FDG mimicking malignancy.
Keywords: 18F-FDG PET/CT, Computed Tomography (CT), Adrenal glands Adenoma(s)
A 51-year-old female was found to have an adrenal mass during the investigation for sudden onset of upper abdominal pain. For 3 years, the patient had been experiencing generalized weakness, worsening headaches, hypertension, weight gain, hot flashes, and generalized hair loss. Subsequent biochemical work-up revealed ACTH-independent hypercortisolemia, while the corresponding ACTH levels were less than 5 pg/ml both times. Further, biochemical work-up including plasma levels of catecholamines, aldosterone, and renin ruled out both pheochromocytoma and primary hyperaldosteronism. The patient underwent CT scan of the adrenals with contrast which showed a 5.2-cm right adrenal mass (Fig. 1a, b yellow crosses; coronal and axial post-contrast CT images). On the post-contrast images, there was an enhancing focus (107 mean H.U.) in the lower pole of the mass raising the suspicion of malignancy (Fig. 1a, b: yellow arrows). The patient underwent PET/CT using 18F-FDG (glucose analogue) in order to evaluate the metabolic activity of the adrenal mass. The main bulk of the tumor showed less uptake (SUVmax: 3.49) compared to the liver (SUVmax: 4.52), whereas the enhancing focus in the lower pole showed increased 18F-FDG activity (SUVmax: 8.6) (Fig. 1c, d: white arrows; coronal and axial fused PET/CT images). Given the size of the adrenal mass and the increased 18F-FDG uptake by its lower part, decision for right adrenalectomy was made in order to rule out adrenocortical carcinoma (ACC).
Fig. 1.
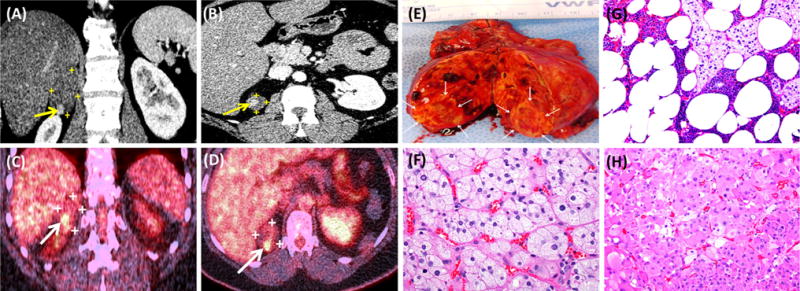
a, b Coronal and axial post-contrast CT images of the adrenal glands. c, d Coronal and axial fused 18F-FDG PET/CT images of the adrenals. e Surgical specimen of the right adrenal gland. f, g Hematoxylin and Eosin (H&E, 400×, 200×respectively) staining of the right adrenal mass outside the smaller nodule. h H&E, 200× staining of the smaller right adrenal nodule
Macroscopic examination of the resected right adrenal gland showed a 5-cm cortical mass (Fig. 1e), while bisection revealed a distinct 0.9 cm nodule (Fig. 1e; arrows). On microscopic examination, the tumor outside the smaller nodule showed uniform cells with foamy cytoplasm and small round nuclei (Fig. 1f; H&E, 400×), while areas of myelolipomatous change were also identified (Fig. 1g; H&E, 200×). Blood lakes, as well as cystic degeneration, hemorrhage, and calcifications were seen, while no necrotic areas were detected. Microscopic examination of the smaller nodule (Fig. 1e; arrows) showed cells with eosinophilic granular cytoplasm and more nuclear pleomorphism than was seen in the rest of the tumor (Fig. 1h; H&E, 200×). However, neither of the two regions of the mass presented changes such as true necrosis, vascular invasion, or high mitotic rate that would suggest malignancy.
Adrenal adenomas typically do not show increased 18F-FDG activity, although lipid-poor and functioning adenomas have been reported to show mild 18F-FDG avidity [1, 2]. Setting a specific SUV threshold in order to differentiate adenomas from malignant adrenal tumors can be misleading. Therefore, comparison to average 18F-FDG uptake by the liver is considered a more efficient approach to assess hypermetabolic adrenal tumors [3]. The presented case indicates that adrenal lesions with 18F-FDG activity markedly higher than the liver uptake should be considered cautiously, since although they are more likely to be malignant, they may prove to be benign adenomas.
Footnotes
Conflict of interest The authors declare that they have no conflict of interest.
References
- 1.Patel D, Gara SK, Ellis RJ, Boufraqech M, Nilubol N, Millo C, Stratakis CA, Kebebew E. FDG PET/CT scan and functional adrenal tumors: a pilot study for lateralization. World J Surg. 2016;40(3):683–689. doi: 10.1007/s00268-015-3242-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Dong A, Cui Y, Wang Y, Zuo C, Bai Y. (18)F-FDG PET/CT of adrenal lesions. Am J Roentgenol. 2014;203(2):245–252. doi: 10.2214/AJR.13.11793. [DOI] [PubMed] [Google Scholar]
- 3.Chong S, Lee KS, Kim HY, Kim YK, Kim BT, Chung MJ, Yi CA, Kwon GY. Integrated PET-CT for the characterization of adrenal gland lesions in cancer patients: diagnostic efficacy and interpretation pitfalls. Radiographics. 2006;26(6):1811–1824. doi: 10.1148/rg.266065057. [DOI] [PubMed] [Google Scholar]